


Abstract
The aim of this study was to assess the value of 99mTc-hexakis-2-methoxyisobutylisonitrile (MIBI) scintigraphy in patients with clinical and radiologic features of primary or metastatic musculoskeletal tumors. Methods: The scintigraphic findings for 84 patients were compared with the surgical and histologic findings. Each patient underwent three-phase bone scanning with 99mTc-methylene diphosphonate (MDP) and dynamic and static MIBI scintigraphy. The MIBI scans were evaluated by visual and quantitative analysis. The count ratio of the lesion to the adjacent or contralateral normal area (L/N) was calculated from the region of interest drawn on the MIBI scan. The Mann–Whitney test was used to determine the differences between the uptake ratios of malignant and benign lesions. Results: Although increased MDP uptake was not specific for bone malignancy, a significant difference was found between benign tumors (L/N = 1.22 ± 0.43) and malignant tumors (L/N = 2.25 ± 1.03) on MIBI scans. Sensitivity and specificity were 81% and 87%, respectively. Forty-six of 53 proven benign lesions did not show significant MIBI uptake. The negative predictive value was 88%. In all seven sites of pathologic fracture, significant uptake was seen. However, three malignant lesions were not detected by MIBI scintigraphy, whereas seven benign lesions showed false-positive results. Conclusion: The major diagnostic worth of MIBI scintigraphy is its high negative predictive value. Although not capable of replacing tissue biopsy as a definitive diagnostic modality for musculoskeletal neoplasms, MIBI scintigraphy does appear to have a role in better preoperative assessment and in distinguishing between pathologic and simple fractures.
Malignant bone tumors represent 0.2% of all new cancers (1). In the United States, approximately 2,100 new cases of bone cancer occur each year, and the incidence of soft-tissue sarcoma is approximately 6,000 cases (1). During the past two decades, significant advances in neoadjuvant therapy and new surgical techniques permit limb-sparing operations with improved functional results and decreased morbidity. Treatment planning requires precise preoperative evaluation and staging. MRI, with its excellent soft-tissue contrast resolution and multiplanar imaging capability, is the main diagnostic modality for preoperative assessment and staging of musculoskeletal tumors but cannot always differentiate benign from malignant lesions (2,3). Radionuclide methods using specific radiopharmaceuticals permit cost-effective whole-body imaging to assess tumor spread and contribute to the preoperative differential diagnosis of these tumors.
99mTc-hexakis-2-methoxyisobutylisonitrile (MIBI) is a lipophilic cation predominantly stored in subcellular structures in response to electric potentials (4). It was originally developed for myocardial perfusion studies and has recently been used as a tumor-imaging agent for various malignancies (5–9).
This study presents the role of MIBI scintigraphy in the preoperative diagnosis of malignant versus benign musculoskeletal tumors and in the differential diagnosis of pathologic (caused by metastases) versus simple fractures in a large group of patients.
MATERIALS AND METHODS
Between January 1996 and August 1999, 91 patients (47 males, 44 females) were studied prospectively. This group included 15 previously reported patients (10). Seven patients without definitive pathologic diagnoses were excluded, leaving 84 evaluable patients (43 males, 41 females; age range, 10–83 y; mean age, 47 y). Sixty-nine patients with clinical and radiologic features of primary musculoskeletal tumors and 15 patients with suspected bone metastases and pathologic fractures were examined. All patients were examined before biopsy, and none had received radiotherapy or chemotherapy before imaging.
Each patient underwent three-phase bone scanning with 99mTc-methylene diphosphonate (MDP). Three to seven days later, dynamic and static MIBI scans were obtained. SPECT images were obtained if needed for better visualization of spinal and pelvic tumors. All scans were obtained using a single- or dual-head gamma camera with a parallel-hole, high-resolution collimator (Apex SP-4 or Varicam; Elscint, Haifa, Israel).
Bone Scintigraphy
After intravenous injection of 500–925 MBq MDP, three-phase bone scanning of the lesion area was performed. After the flow phase (2-s images for 90 s), static images were taken 5 min and 3 h later. Whole-body bone scans were also obtained for each patient to assess tumor spread.
99mTc-MIBI Study
The patients received intravenous injections of 370–740 MBq 99mTc MIBI. No adverse reactions were noted. Subsequently, radionuclide angiography was performed with the collimator over the lesion area. Data were obtained every 2 s for 60 s. Twenty to 30 min later, whole-body scans were obtained. Spot images were also taken over the pathologic areas on a 256 × 256 matrix for a preset time of 10 min.
Data Analysis
MDP and MIBI images were interpreted by two nuclear medicine physicians who reached a mutual agreement and were unaware of the clinical findings. MDP scans were used as a guide to lesion localization and tumor spread.
MIBI images were evaluated visually and quantitatively. For quantitative analysis, a region of interest was drawn on the lesion and on a contralateral or adjacent normal area. The lesion-to-normal tissue count ratio (L/N) was then calculated. The group was empirically divided into three subgroups according to the intensity of MIBI uptake: group 1 showed no increase in uptake, group 2 showed mildly increased uptake (L/N < 1.5), and group 3 showed significantly increased uptake (L/N > 1.5). The detected lesions were confirmed by histologic findings and clinical outcome.
Statistical Analysis
The values were presented as mean ± SD. The Mann-Whitney test was used to determine differences between the uptake ratios for malignant and benign lesions. P < 0.05 was considered significant.
RESULTS
The individual lesions were classified by histologic findings as benign or malignant, and the results are summarized in Tables 1–3. Fifty-three benign and 31 malignant (19 primary and 12 metastatic) musculoskeletal tumors were evaluated.
Type of Musculoskeletal Lesion
The L/N Distribution of 84 Musculoskeletal Lesions
The Results for 84 Patients Who Underwent MIBI Scintigraphy
Increased MDP blood flow and uptake were seen in 78 of the 84 patients. No increased uptake was seen in one patient with a simple bone cyst, three patients with benign soft-tissue tumors, and two patients with liposarcoma. In four patients with metastatic disease, the bone scan showed multiple foci of uptake.
MIBI Scanning of Benign Lesions
Forty-six of 53 proven benign lesions did not show significant MIBI uptake (Fig. 1). Among these, 34 lesions had no pathologic tracer concentration and 12 lesions had mildly increased uptake. The mean L/N of the entire benign group was 1.22 ± 0.43. Among seven benign lesions with false-positive results were two recurrent giant cell tumors, two cases of myositis ossificans, two nonossifying fibromas, and one osteoid osteoma.
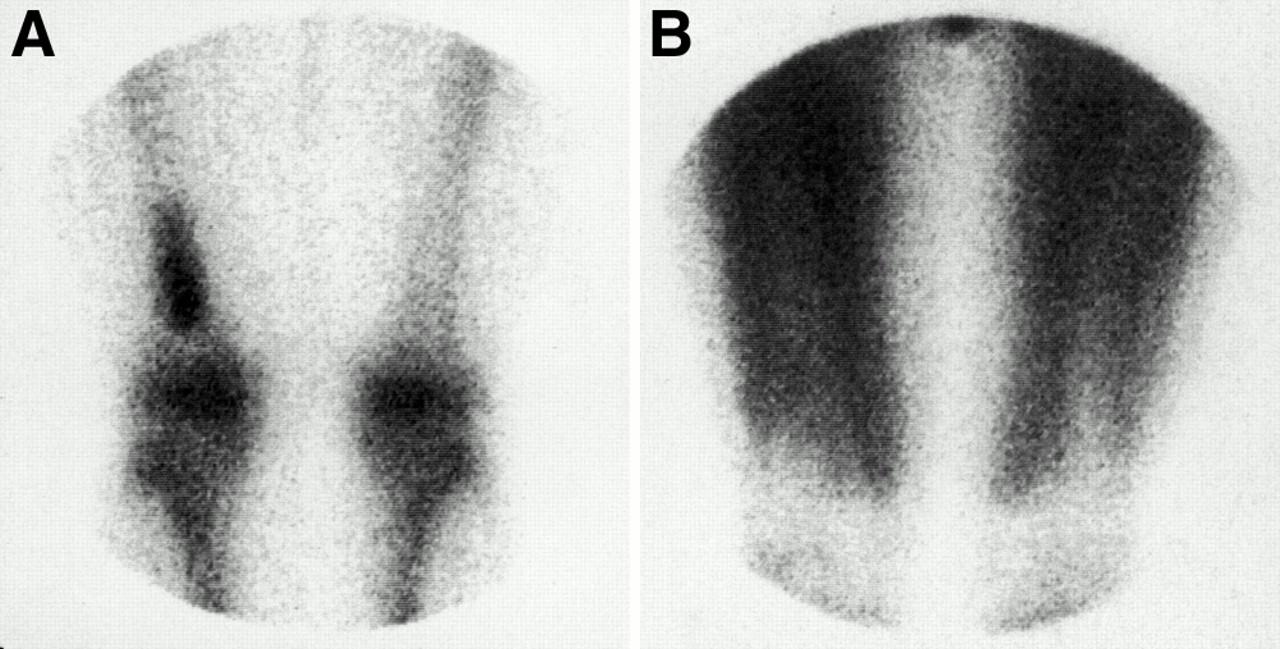
In patient with enchondroma of right femur, MDP scan (A) shows increased tracer uptake, whereas MIBI scan (B) of same area shows no abnormal uptake.
MIBI Scanning of Malignant Tumors
Twenty-five of 31 histologically confirmed malignant tumors showed highly increased MIBI uptake (Fig. 2), and in three additional cases, mildly increased uptake was noted. All true-positive studies showed increased tumor blood flow. No increased MIBI uptake was seen in three malignant tumors, which included a malignant soft-tissue schwannoma, a liposarcoma, and a metastasis of poorly differentiated squamous cell carcinoma. Four of six tumors with no significant MIBI uptake were poorly differentiated histologically. The mean L/N of the malignant tumors was 2.25 ± 1.03.

In patient with osteogenic sarcoma of lumbar spine, both MDP scan (A) and MIBI scan (B) show significantly increased tracer uptake.
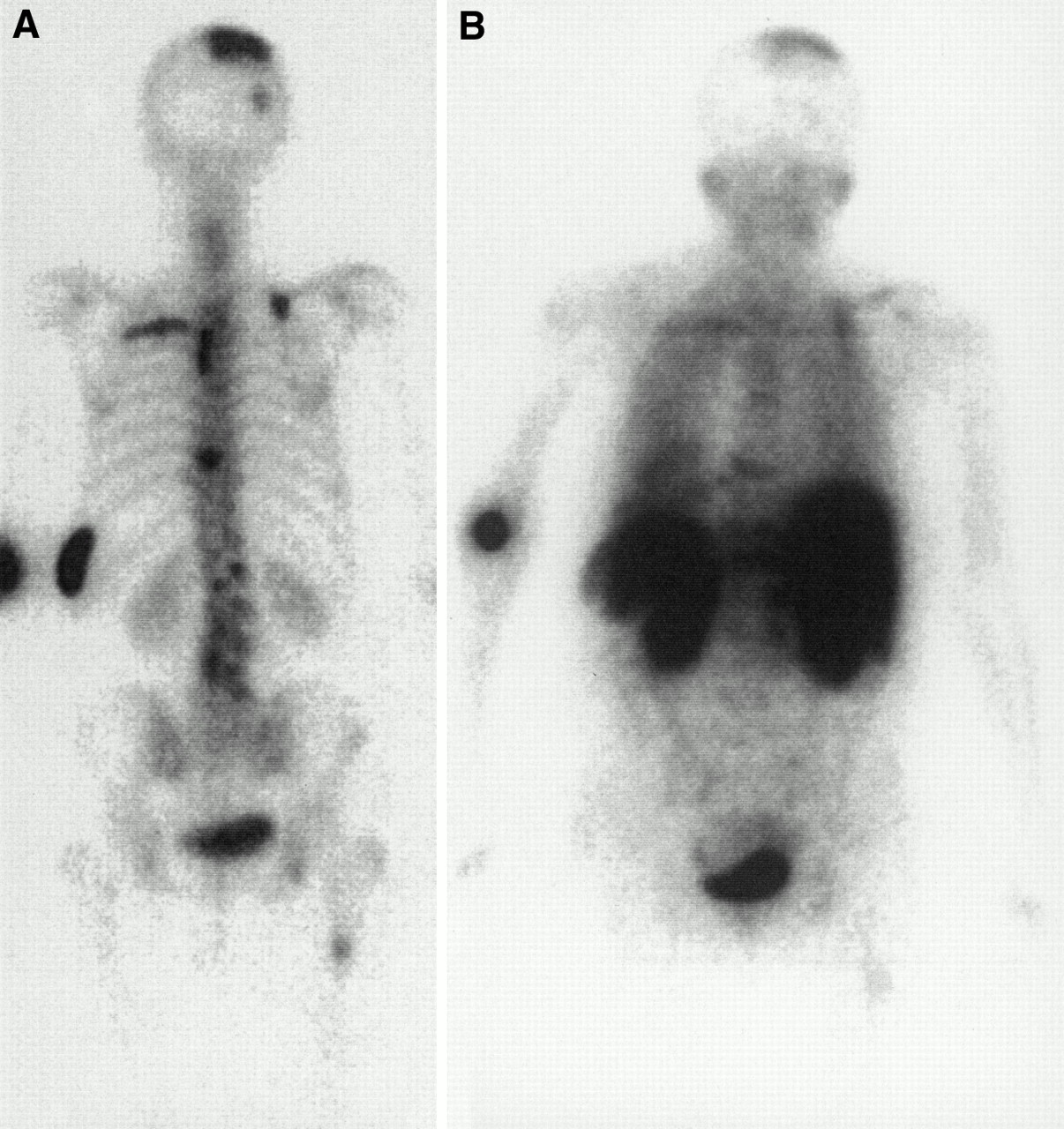
Metastatic lesions were detected in 12 of 15 patients with nonmusculoskeletal primary malignant tumors. In the other patients, assumed to have metastatic lesions, the MIBI scan showed normal findings and simple fractures were found. Three patients had more than one focus of increased uptake (Fig. 3), but the entire number of metastases detected was lower for the MIBI scan than for the MDP scan. The L/N of one metastatic lesion per patient was calculated. This lesion was thought to be a pathologic fracture. Ten of 12 metastatic bone tumors showed significantly increased uptake, and two had mildly increased activity. All seven sites of proven pathologic fracture had significantly increased MIBI uptake (Fig. 4).

MDP (A) and MIBI (B) scans of patient with bone metastatic disease (posterior view). Total foci are fewer for MIBI scan than for bone scintigraphy.

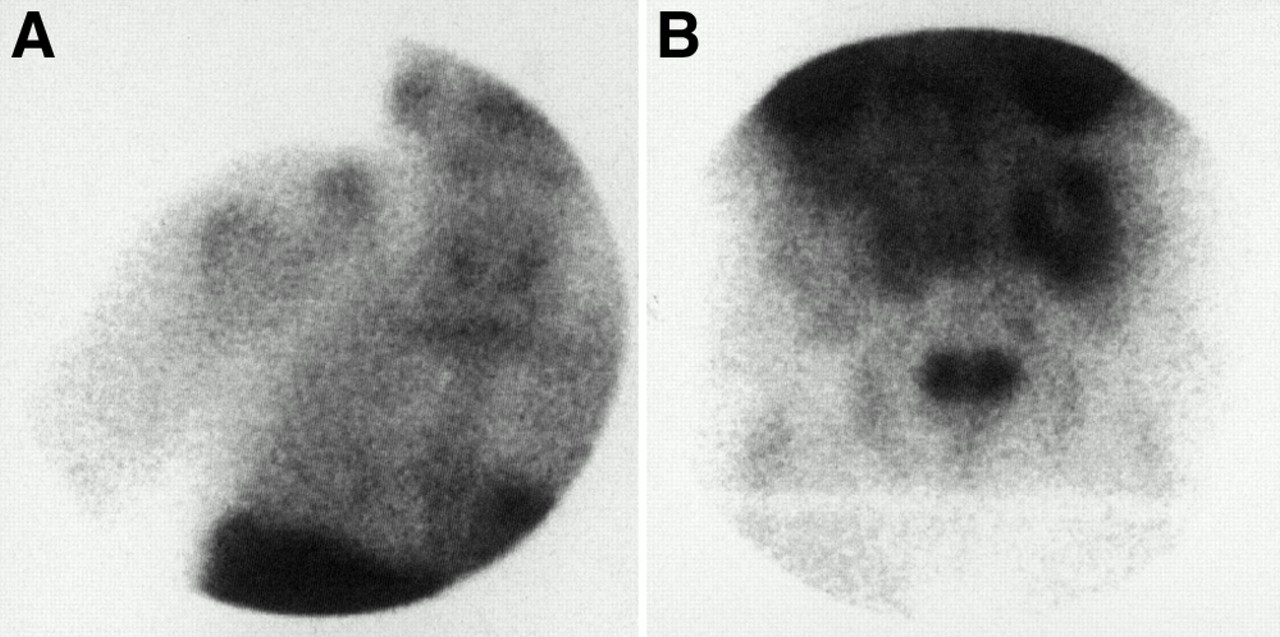
In patient with bone metastasis and pathologic fracture of right shoulder, MIBI scan shows increased lesion uptake (A). Increased concentration is also seen in right posterior pelvic region (B), where metastatic tumor was found.
A highly significant difference was found between the L/N of benign lesions and the L/N of malignant tumors (P < 0.001). The mean uptake ratio of the two groups was 1.59 ± 0.85. Figure 5 provides an overview of the data for both groups. It shows that most uptake ratios for the malignant tumors were greater than the mean value, whereas most uptake ratios for the benign lesions were less than the mean value.
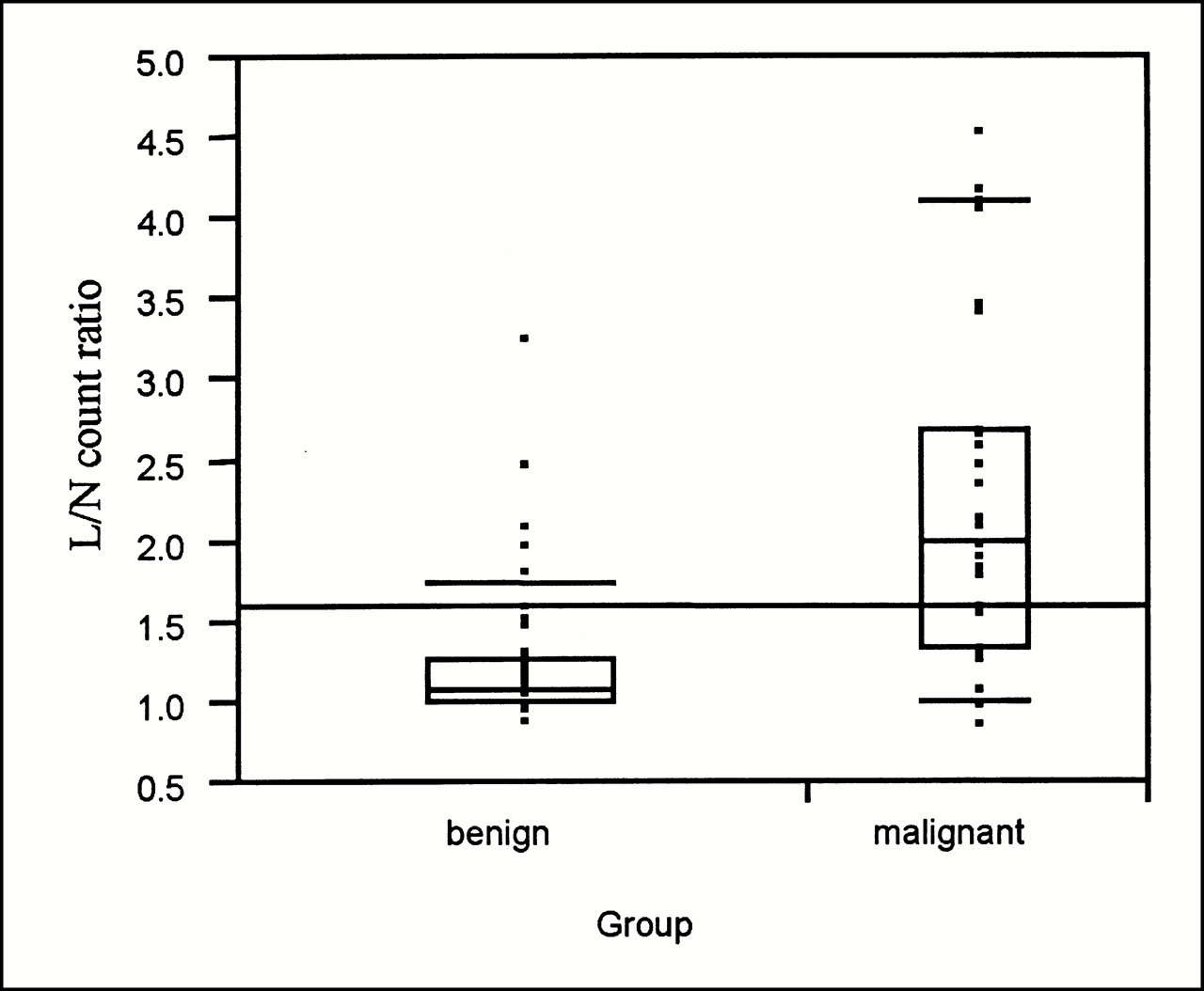
Comparison between MIBI uptake ratio of benign and malignant lesions. Mean uptake ratio of the two groups is 1.59 ± 0.85. Most uptake ratios of malignant tumors are greater than mean, whereas most uptake ratios of benign lesions are less than mean.
The malignant tumors with significantly increased MIBI uptake were considered to be true-positive. Sensitivity and specificity were 81% and 87%, respectively. Accuracy was 84%. The negative predictive value of MIBI was 88%, and taking only true- and false-negative cases (with no MIBI uptake), the negative predictive value was 92%.The positive predictive value was only 78%.
DISCUSSION
Interest among orthopedists in musculoskeletal tumors has increased over the past decade as research of new therapeutic modalities has progressed. Although essential for diagnosis, biopsy is subject to error and consequent complications (11); therefore, prebiopsy localization, accurate diagnosis, and staging are helpful. Plain film radiography is a basic modality in the diagnosis of bone tumors but is limited in detecting early bone destruction and soft-tissue extension (12). Cross-sectional imaging techniques (CT and MRI) permit excellent morphologic characterization and have a major diagnostic role. However, numerous studies using radionuclide methods for preoperative diagnosis of musculoskeletal tumors have shown some advantages over MRI and CT, such as cost-effectiveness, lack of adverse reactions, and the ability to obtain functional whole-body imaging (13–15). MDP bone scanning is highly sensitive but less specific and cannot precisely differentiate between malignant and benign tumors. In all but six musculoskeletal lesions, increased MDP uptake was seen.
FDG PET, although expensive and not yet available in many institutions, appears preferable for tumor imaging. Recently, several studies have confirmed the diagnostic value of MIBI in the evaluation and follow-up of bone sarcomas (16–19). Similar to 201Tl, 99mTc-MIBI accumulation depends on cell viability and metabolic conditions. However, MIBI with 99mTc as a radiolabel is preferred to 201Tl-chloride because the former has better physical characteristics, permits blood flow studies, gives better resolution, and allows higher doses (4,14,15).
Most malignant tumors in this study (25/31) showed significantly increased MIBI uptake, with a mean L/N count ratio of 2.25 ± 1.03. This ratio was significantly higher than the mean L/N count ratio for the group of benign lesions (1.22 ± 0.43, P < 0.001). These results, in comparison with those obtained by Taki et al. (19), showed better differentiation between benign and malignant lesions. In our group, accuracy and specificity were 84% and 87%, respectively. However, in three patients with malignant disease no MIBI uptake was seen, and in three additional malignant lesions only mildly increased uptake was found. Four of these lesions with no significant MIBI uptake were diagnosed as poorly differentiated tumors, one was diagnosed as low-grade fibromyxoid sarcoma, and one was diagnosed as liposarcoma. The varying levels of MIBI concentration in malignant lesions could be caused by heterogeneity and variable differentiation of tumor tissue. We believe that some low MIBI uptake in these tumors can also be explained by high P-glycoprotein expression. MIBI has been validated as a transport substrate for P-glycoprotein in a variety of multidrug-resistant human tumor cells (20,21).
Distinguishing between pathologic and simple bone fractures is important. In such situations, MRI does not always give the answer. MIBI scintigraphy was true-positive in all seven patients with metastatic bone disease at the site of pathologic fracture and was true-negative in three patients with simple fractures, allowing clear differentiation between the two conditions. To the best of our knowledge, no data exist on the use of MIBI in the diagnosis of pathologic fractures. Unfortunately, MIBI scintigraphy cannot reveal all bone metastatic lesions seen on MDP images, especially those in the lower chest and pelvic areas.
Seven of 53 benign musculoskeletal lesions were false-positive, giving a positive predictive value of 78%. Two patients with myositis ossificans showed increased blood flow and MIBI uptake at the lesion sites. Adalet et al. (16) and Taki et al. (19) have shown numerous benign lesions with increased MIBI uptake. No correlation was found between histologic results and MIBI concentration in our group. However, five of seven tumors with increased MIBI uptake showed increased vascularization.
CONCLUSION
The major diagnostic benefit of MIBI scintigraphy is its high negative predictive value. The overlap between benign and malignant tumors decreases the usefulness of MIBI scanning as a single diagnostic tool. However, this method is helpful as an additional modality to differentiate between pathologic and simple fractures. Also, MIBI scanning appears to have a role in improving the preoperative assessment and staging of musculoskeletal tumors.
Footnotes
Received Feb. 16, 2000; revision accepted Jun. 20, 2000.
For correspondence or reprints contact: Tifha Horne, MD, Department of Nuclear Medicine, Assaf Harofeh Medical Center, Zerifin 70300, Israel.
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.