


Abstract
The aim of this study was to compare FDG PET with a new monoclonal antibody–based imaging agent that comprises an anti–carcinoembryonic antigen (CEA) monoclonal antibody Fab′ fragment directly labeled with 99mTc. Methods: Twenty-eight patients who were previously treated for colorectal carcinoma and in whom recurrence was suspected were examined with FDG PET and immunoscintigraphy. The most common indications were an elevation of serum CEA (13 patients), suggestive lesions documented by CT (9 patients), sonography (4 patients), and severe constipation (2 patients). Planar imaging and SPECT were performed 4–6 h after intravenous injection of the new imaging agent. Whole-body PET was performed 45–60 min after intravenous injection of FDG. The findings were confirmed by conventional diagnostic modalities, surgery, and histology. Results: Histology confirmed local tumor recurrence in 9 of 28 patients. Clinical follow-up or CT confirmed the presence of liver metastases in 9 patients and lymph node involvement, lung metastases, and bone metastases in 2 patients each. The new agent correctly detected 8 of 9 local recurrences, whereas FDG PET was able to detect all 9 cases and in 1 case was false-positive. Liver metastases were confirmed in 9 patients by FDG PET but in only 1 patient by the new agent. Two cases with lymph node metastases and 2 cases with lung metastases were correctly identified by FDG PET, but none were detected by the new agent. Finally, bone metastases were identified in 1 patient by FDG PET but not with the new agent, whereas bone marrow infiltration (n = 1) was diagnosed by both imaging modalities. Conclusion: These results indicate that FDG PET and 99mTc-labeled anti-CEA Fab′ are suitable for the diagnosis of local recurrence of colorectal carcinoma but that FDG PET is clearly superior in the detection of distant metastases (liver, bone, and lung) and lymph node involvement.
Colorectal cancer, the second leading cause of cancer mortality in the United States (1), has an incidence of approximately 12%–13% and a mortality rate of 10%–11%. At the time of first diagnosis, the disease is localized in only 36% of patients; regional lymph node metastases are present in 39%, and distant metastases are present in 19%. The overall 5-y survival rate after resection is 55%–75%. After primary surgery, 30%–40% of patients with resectable tumors experience disease relapse within 3 y.
Because early detection and management of recurrent disease is associated with improved survival, early detection of potentially resectable metastases or tumor recurrence leads to improved prognosis (2). Serum levels of carcinoembryonic antigen (CEA) may be used to monitor the presence of recurrences with a sensitivity of 59% and a specificity of 84% but not to localize recurrent lesions (1).
Multiple imaging methods (sonography, CT, MRI) are thus used in routine follow-up to detect tumor recurrence, but they have only limited diagnostic accuracy (3–6). Identification of a presacral mass by conventional imaging does not allow accurate differentiation between scar tissue, fibrotic tissue, or tumor recurrence. Therefore, complementary methods are warranted. FDG PET and immunoscintigraphy with 99mTc-labeled anti-CEA antigen-binding fragments as topofunctional imaging modalities have both been found suitable, and several groups have shown that FDG uptake increases in colon and rectal carcinomas (4–13).
Because FDG uptake can be observed in malignant and inflammatory lesions (14), the use of more specific tracers such as antibodies seems desirable. Many studies have used monoclonal antibodies to detect colorectal cancer (15–35). Recently, an (Fab′) antibody fragment specific to CEA that can be labeled with 99mTc (CEA-Scan; Immunomedics, Inc., Morris Plains, NJ) has become commercially available. Thus, specific images with good contrast between tumors and normal tissue can be expected (12,29,35). Our aim was to compare the efficacy of FDG PET with that of a 99mTc-labeled anti-CEA monoclonal antibody for the detection of tumor recurrence and systemic spread of colorectal carcinoma.
MATERIALS AND METHODS
Patients
Twenty-eight patients with suspected recurrence of colorectal carcinoma were enrolled and followed up for 6–19 mo. All were informed about the nature of the study and had given written informed consent before the start of immunoscintigraphy or PET.
Immunoscintigraphy
CEA-Scan from a commercially available kit was labeled with 99mTc according to the manufacturer's guidelines. Images were obtained with a double-head camera (Prism 2000; Picker International, Cleveland, OH) 4–6 h after intravenous injection of 740 MBq 99mTc anti-CEA antibodies. The study consisted of planar images (500,000 counts) of the chest, abdomen, and pelvis in anterior and posterior views after bladder voiding. Additionally, SPECT of the pelvis was performed (3 degrees, 30 s per step, step-and-shoot mode, 180° field of view); in 15 patients, SPECT of the liver was also performed. The data were processed with Butterworth-filtered backprojection.
FDG PET
FDG was commercially obtained (Forschungszentrum Karlsruhe, Karlsruhe, Germany). Whole-body studies were performed using a dedicated PET scanner (ECAT EXACT; Siemens/CTI, Knoxville, TN). Patients fasted overnight to reduce serum insulin levels. Approximately 250–370 MBq FDG were injected intravenously and flushed with 20 mL saline solution. Patients were rested at the time of injection and during the waiting period and were asked to drink 1 L water to promote diuresis. The bladder was voided before the examination to reduce artifacts. Scanning was initiated from the inguinal region to minimize bladder activity. Emission scans were obtained 45–60 min after the injection. For attenuation correction, measured transmission scans (7 min per bed position) were used. Tomograms were reconstructed by filtered backprojection with a Hanning filter (cutoff frequency, 0.4/cycle; decay correction; no scatter correction). Qualitative assessment of image quality comparing hot (patient not moved) and cold (patient moved between transmission and emission scans) transmission scans did not reveal significant differences.
Image Assessment
Primary image assessment was by 2 experienced nuclear medicine physicians unaware of the results of the other imaging studies. CEA-Scan findings were considered positive (tumor present) if the observers saw focal enhanced antibody uptake that could not be associated with physiologic accumulation (liver, kidneys, or bladder). FDG PET findings were classified as “malignancy—typical” when antibody uptake was markedly higher than liver uptake. Antibody uptake comparable to liver or mediastinum uptake was classified as “malignancy—suspect or inflammatory.” Antibody uptake lower than liver uptake but higher than background activity was classified as “unspecific.” Absence of uptake in documented morphologic lesions was classified as “no evidence of disease.” After the primary assessment, all results were compared with the results of conventional imaging modalities.
RESULTS
We investigated 28 patients (15 men, 13 women; median age, 62 y) with suspected recurrence who underwent resection of colorectal cancer 6–52 mo previously (Table 1). The indications of recurrence were an increase in serum CEA (13 patients), CT-documented lesions (9 patients), constipation (2 patients), and sonographically documented lesions (4 patients). All patients underwent both imaging techniques within 6 d. The findings was corroborated surgically for 14 patients. The final institutional diagnosis, based on histology and clinical or radiologic follow-up, was used as the gold standard.
Results for All Patients
Overall, recurrence of colorectal carcinoma was finally confirmed in 9 patients. Malignancy could be ruled out by clinical follow-up in 7 patients. Only local recurrence was detected in 7 patients; only metastases were found in 7 patients; and both recurrence and metastases were detected in 1 patient. Liver metastases were confirmed in 9 patients, and bone metastases, lung metastases, and lymph node metastases were confirmed in 2 patients each. Table 2 shows an analysis by tumor site.
Number of Lesions Detected
Local Recurrence
CEA-Scan was able to correctly detect 8 of 9 cases of local recurrence. In 1 patient, the findings were false-negative. FDG PET showed intense uptake in 9 patients (Fig. 1). One patient showed moderate uptake, which was identified as false-positive. Direct comparison with CEA-Scan showed no uptake of monoclonal antibody (true-negative) in this FDG-positive lesion.

(A) FDG PET image (sagittal view) shows large area (arrow) with intense FDG accumulation behind bladder. (B) CEA-Scan (Immunomedics) image of same patient shows increased tracer accumulation in same area (arrow). Histologically, this area represented local recurrence.
Liver Metastases
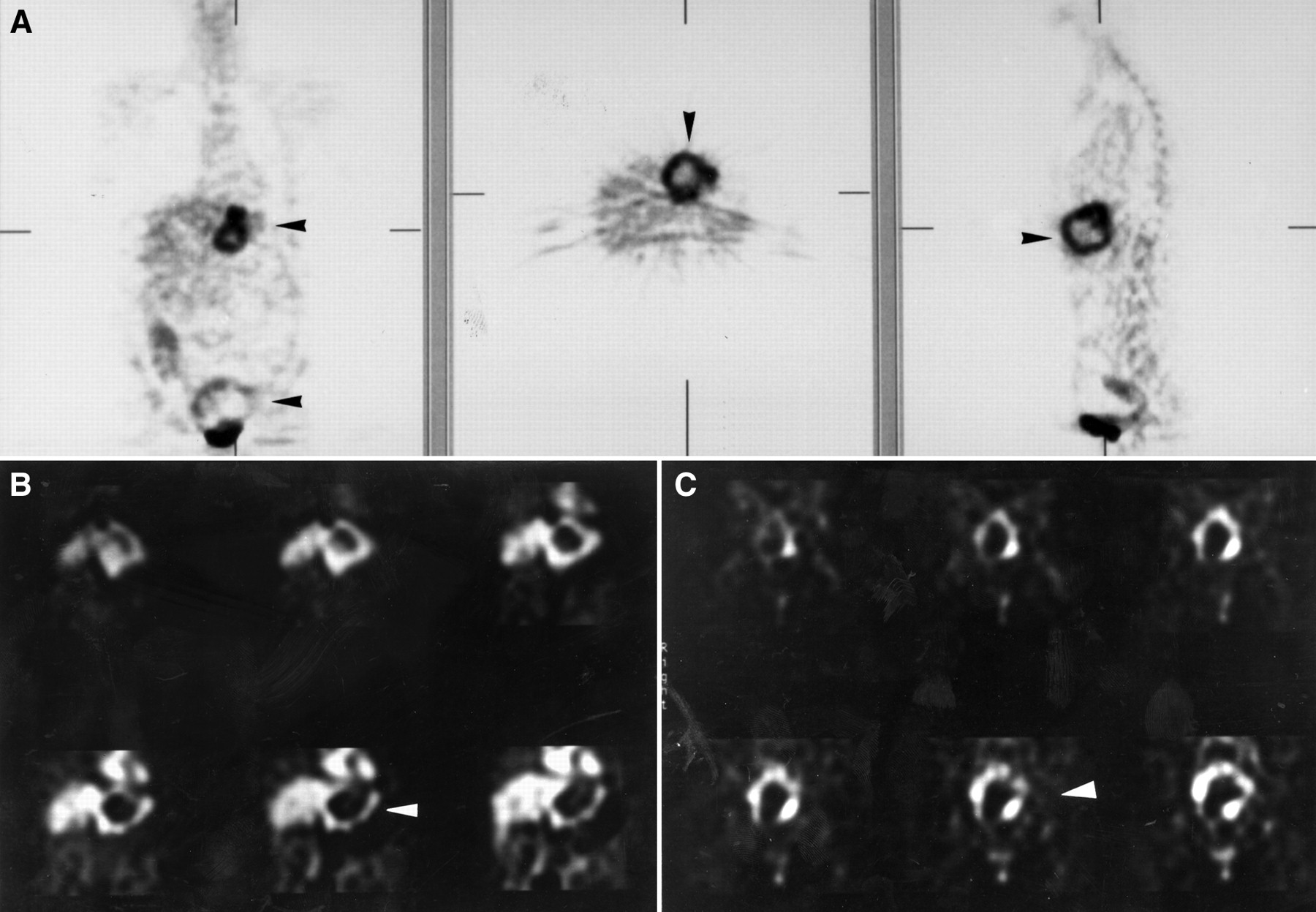
All liver metastases were correctly confirmed by FDG PET (n = 9), but in only 1 patient were liver metastases correctly confirmed by CEA-Scan (Fig. 2). In CEA-Scan images, large metastases appeared either scintigraphically isointense in comparison with normal liver tissue or, in 1 patient, as a cold lesion.

(A) In upper abdomen, FDG PET images (coronal, transversal, and sagittal views) show focally enhanced glucose metabolism with central defect. In lower abdomen directly above bladder, coronal view shows circular lesion with enhanced glucose metabolism in outer rim and central defect. Arrowheads point to local recurrence of liver metastases. (B) Liver SPECT study (CEA-Scan; Immunomedics) reveals similar result, with tracer uptake in viable tumor mass (arrowhead). High uptake is also seen in normal liver and myocardium. (C) High uptake is seen in abdomen, similar to FDG PET. Arrowhead points to local recurrence.
Other Distant Metastases
Two lymph node metastases and 2 cases of lung metastases were correctly identified by FDG PET but were not detected by CEA-Scan. Bone metastases were identified in 1 of 2 patients by both imaging modalities and in 1 patient by only FDG PET.
Overall, with respect to local recurrence, CEA-Scan showed a sensitivity, specificity, and accuracy of 89%, 100%, and 96%, respectively. The sensitivity of FDG PET with regard to local recurrence was 100%, the specificity was 95%, and the accuracy was 96% (Table 3).
Local Recurrence
DISCUSSION
We assessed the usefulness of CEA-Scan versus FDG PET in the detection of recurrent colorectal carcinoma. Our data show that local recurrence of colorectal carcinoma can be detected by both imaging modalities with high sensitivity and specificity.
An initial report on the value of FDG PET in patients with suspected recurrent colorectal cancer by Schlag et al. (4) showed intense FDG uptake in 11 of 12 patients with confirmed recurrence. Ito et al. (9) and Schiepers et al. (13) confirmed these results and observed a higher sensitivity and specificity for PET than for MRI. FDG PET was able to differentiate scar tissue from tumor recurrence. Ogunbiyi et al. (36) investigated 58 patients with CT and FDG PET and found a specificity of 91% and a sensitivity of 100% for FDG PET. Our results confirm their observation of increased uptake of FDG in recurrent rectal cancer. In only 1 patient (patient 2) were the findings misclassified as positive. Problems with interpretation can occur because FDG is excreted by renal elimination and because some artifacts in image reconstruction can be seen next to the kidney and urinary bladder, obscuring lesions or causing false-positive findings. Because of this activity in the bladder, the dorsal pelvic region could not be fully analyzed. The study was repeated with a bladder catheter and showed 1 hot spot, which was classified as tumor recurrence, in the dorsal part of the pelvic area. The patient was followed up by several CT examinations over 9 mo, with no sign of morphologic changes. Thus, we assume that the retained activity was caused by persisting urinary activity, an observation that Miraldi et al. (37) reported.
Major objections to FDG PET have been based mainly on the assumption that FDG may be too unspecific a tracer, because false-positive findings may occur in inflammatory disease (14,38). Because FDG PET is commonly expensive, its use is limited and other techniques are warranted. Therefore, we compared our results with the findings for CEA-Scan, which is a new 99mTc-labeled antibody (Fab′) fragment specific to CEA. Eight of 9 cases were confirmed correctly by CEA-Scan. Because other investigators have observed similar results using CEA-Scan (22,24,25,27–29,35), this agent seems to be useful for establishing local tumor recurrence. Our data show that CEA-Scan is helpful in detecting disease recurrence after surgical resection of primary colorectal cancer. In accordance with studies by Behr et al. (31), our study also showed that CEA-Scan can disclose serum CEA-negative tumor recurrence and high circulating CEA titers.
Nevertheless, the evaluation of such malignancies is complicated, as shown by our patient with false-negative findings. Physiologic excretion of monoclonal antibody is seen in the urinary tract, gallbladder, and gastrointestinal tract, especially in delayed images, and can lead to misdiagnoses. Bowel preparation with an iso-osmotic solution and intravenous application of furosemide are possible methods for overcoming this disadvantage. In our patient with false-negative findings, pathologic monoclonal antibody accumulation was missed, probably because of small tumor size (<2 cm).
If the results of FDG PET are compared with those of CEA-Scan, we find that both imaging modalities are sensitive in detecting local recurrence. Although image quality (resolution and contrast between tumor and normal tissue) was clearly better for FDG PET than for CEA-Scan, the actual benefit was only marginal.
A second goal was to evaluate the possibility of restaging with both methods. Some authors report that FDG PET is more sensitive than CT in the clinical assessment of patients with metastatic colorectal cancer. Lai et al. (39) reported that FDG PET showed better results in detecting extrahepatic lesions than did conventional imaging. Ogunbiyi et al. (36) reported that FDG PET was 95%–100% sensitive for detecting liver metastases. These values were superior to those for CT, which had a sensitivity of 74% and a specificity of 85%. Another group (40) found a sensitivity of 100% and a specificity of 67% for restaging colorectal carcinoma. Our data show that tumor spread with lymph node, liver, and lung metastases was accurately detected by FDG PET. However, with 1 exception, CEA-Scan failed to reveal these tumor sites because of insufficient monoclonal antibody accumulation in these patients. Behr et al. (29) observed a similar result using an intact anti-CEA immunoglobulin G. They also described diminished tumor-to-liver ratios in large liver metastases when fragments were used. Fragments have been shown to exert higher tumor-to-background ratios, rather because of significant enhanced background clearance than because of enhanced absolute uptake. In addition, the imaging characteristics of 99mTc-labeled antibodies are preferential (higher application dose, better detection sensitivities, use of SPECT). In our study, tumor uptake usually did not exceed uptake by normal liver tissue. Reports (16–18) show that liver metastases have been detected in only a few cases (21%–50%) using intact antibodies or 111In-labeled antibodies or fragments. In contrast, Behr et al. (29) observed a higher sensitivity—87%—using fragments. Moffat et al. (35) showed a sensitivity in detecting liver metastases—63%—that was comparable to that of conventional imaging. These data were not confirmed by our results, possibly because we did not always include the liver (Table 4).
Scintigraphic Results for Liver Metastases
Overall, sensitivity in detecting liver metastases seems to be lower for CEA-Scan than for FDG PET. In our study, all confirmed tumor lesions showed intense uptake of FDG. This finding agrees with published results (6,13,40) for this tumor type. Other studies comparing FDG PET with conventional imaging underscore a significant improvement in the detection of liver metastases (39). This improvement may be caused by a significantly higher resolution and improved image contrast from an active trapping mechanism with FDG PET. At the same time, missed lymph node and lung metastases were probably caused by small tumor size (<2 cm), emphasizing the benefit of FDG PET. Thus, if correct tumor staging is required, FDG PET should be preferred.
CONCLUSION
The results indicate that both FDG PET and CEA-Scan are suitable for diagnosing local recurrence of colorectal carcinoma. In differential diagnoses, CEA-Scan shows a high sensitivity for scarring or relapse of CT-proven lesions. Because of a higher sensitivity in detecting lymph node and distant metastases, PET should be used for tumor staging.
Acknowledgments
This study was presented in part at the annual meeting of the Society of Nuclear Medicine, June 1998, Toronto, Ontario, Canada, and at World Federation of Nuclear Medicine and Biology, August 1998, Berlin, Germany.
Footnotes
Received Sep. 27, 1999; revision accepted Mar. 8, 2000.
For correspondence or reprints contact: Petra Willkomm, MD, Department of Nuclear Medicine, Sigmund-Freud-Str. 25, D-53127 Bonn, Germany.




{kind=link}
{kind=link}