


Abstract
The aim of this study was to use gastroesophageal and pulmonary scintigraphy to evaluate the prevalence of gastroesophageal reflux and airway involvement among patients with posterior laryngitis. Methods: The study included a total of 201 patients (131 females, 70 males; age range, 15–77 y; mean age ± SD, 49 ± 16 y). All patients had posterior laryngitis documented by laryngoscopy and symptoms such as a dry cough, painful swallowing, and hoarseness. A control population of 20 healthy volunteers (13 females, 7 males; age range, 19–74 y; mean age, 53 ± 13 y) was also evaluated. After a 12-h fast, all subjects underwent gastroesophageal scintigraphy through administration of 300 mL orange juice labeled with 185 MBq 99mTc-sulfur colloid. After 18 h, planar anteroposterior thoracic images were acquired with the subjects supine. Results: Sixty-seven percent of patients (134/201) had scans positive for gastroesophageal reflux; of these, 30 (22%) had distal reflux and 104 (78%) had proximal reflux. In addition, the scans of 31 patients were positive for proximal reflux–associated pulmonary uptake. The frequency, duration, and degree of reflux episodes were significantly greater in patients with proximal reflux than in patients with distal reflux (P < 0.001). The 67 patients in whom reflux was not detected had diseases or reflux-associated cofactors that could account for laryngeal symptoms. No statistically significant difference in symptoms or esophageal motility parameters could be identified among the patient groups, but patients with proximal reflux had significantly prolonged gastric emptying times compared with healthy volunteers. Conclusion: Most patients with posterior laryngitis had detectable proximal gastroesophageal reflux. Exposure of the proximal part of the esophagus to acid, by setting the stage for microaspiration of gastric material into the larynx, remains a major cause of damage to the laryngeal mucosa. Slowed gastric emptying may be a predisposing factor. Moreover, symptoms such as a dry cough, painful swallowing, or hoarseness may not be reliable predictors of the presence of gastroesophageal reflux or of associated airway involvement.
Symptoms such as heartburn, pyrosis, and acid regurgitation as clinical manifestations of gastroesophageal reflux (GER) disease are well described and occur in 50%–65% of patients with this disorder (1–7). Respiratory manifestations are less recognized but appear to occur frequently as a complication of reflux. Posterior laryngitis appears particularly relevant, occurring in 50%–60% of patients with GER (6,8), who present clinically with laryngitis, hoarseness, a cough, difficulty swallowing, and a sensation of a foreign body in the throat.
Reflux extending to the upper esophagus—so-called proximal reflux—appears to be responsible for many such cases (9). Therefore, awareness of nongastroesophageal symptoms of reflux and a high index of suspicion when they are present may allow timely identification and formulation of a treatment strategy. The well-established use of scintigraphy to evaluate GER and motility noninvasively can be effective for screening and following up these patients. This examination is sensitive, dosimetrically favorable, and well tolerated and can define the degree of GER and its level of extension into the esophagus. In addition, the technique can be extended to include a later lung image, which potentially can reveal microaspiration of gastric contents as the cause of airway infection.
The purpose of this study was to evaluate, in a large group of patients with endoscopically documented posterior laryngitis, the correlation between GER and several related variables such as the degree and upper extension of reflux, esophageal and gastric motility, and pulmonary aspiration.
MATERIALS AND METHODS
The study included 201 patients with posterior laryngitis (131 females, 70 males; age range, 15–77 y; mean age ± SD, 49 ± 16 y). Posterior laryngitis was documented endoscopically, and all patients underwent gastroesophageal scintigraphy and lung field scintigraphy. A dry cough, painful swallowing, and hoarseness were present for at least 6 mo. Before scintigraphy, all patients were required to complete a questionnaire in which pertinent symptoms (dry cough, painful swallowing, dryness of the mouth, excessive salivation, hoarseness, acid regurgitation, aerophagia, heartburn, epigastric pain, and postprandial fullness) and their duration were scored from 0 to 3 (0 = symptoms occurring less than once a month; 1 = between once weekly and once monthly; 2 = once weekly; 3 = daily). None of the study patients had a history of gastrointestinal disease or were undergoing treatment with medications potentially interfering with either esophageal or gastric motility or with secretory function.
Twenty healthy volunteers served as a control group (13 females, 7 males; age range, 19–74 y; mean age, 53 ± 13 y). None had a history of gastroesophageal disease, central nervous system disease, peripheral neuropathy, diabetes mellitus, or other systemic diseases commonly associated with gastroesophageal dysfunction. In addition, none had a recent history of drug treatment potentially affecting gastroesophageal function.
Informed consent was obtained from all study participants, and the study was approved by the San Paolo Hospital ethical committee.
Evaluation Techniques
Laryngoscopy was performed by a single operator, using a fiberoptic laryngoscope, who was unaware of the results of the other evaluations. The term “posterior laryngitis” was applied when the operator saw symmetric thickening of the mucosal surfaces of the posterior third of the true vocal cords, particularly in the arytenoid area and posterior commissure (10).
Scintigraphy was performed over 2 d. The first day was dedicated to the identification and quantification of GER (11–16); during the second day, lung field uptake was studied to detect signs of pulmonary aspiration of gastric contents. Sulfur colloid (Hepatate; Nycomed Amersham, Princeton, NJ) radiolabeled with 185 MBq (5 mCi) 99mTcO4 was added to acidified orange juice (150 mL orange juice plus 150 mL 0.1-N hydrochloric acid). The 99mTc labeling efficiency of this suspension was 90% and remained stable for the following 18 h.
A wide-field, low-energy, high-resolution gamma camera (ADAC Laboratories, Milpitas, CA) with a parallel-hole collimator was used. The 20% energy window was centered at 140 keV. A 64 × 64 matrix with 1.4 zoom was used for dynamic acquisitions, and a 256 × 256 matrix without zoom was used for static acquisitions. The dynamic images were corrected to account for decay of 99mTc.
Gastroesophageal scintigraphy was performed after the subjects had fasted for 12 h. They ingested 15-mL boluses of a labeled liquid meal in a single deglutition when indicated by the operator, immediately after the start of image acquisition and recording. All examinations were performed with the subjects standing and with the gamma camera in anterior projection. The fields included the oral cavity and the upper abdominal quadrants. The jugular and xiphoid processes were marked with 57Co. For each dynamic study, 2 images per second were acquired for 30 s so that the transit of the labeled bolus could be followed through the entire esophagus. After the remaining 285 mL labeled orange juice were ingested, the patients were placed supine and a second set of dynamic images was acquired (1 image every 5 s, for a total of 720 images) in anterior projection. Ten minutes before the completion of the examination, a rigid abdominal belt connected to a manometer was positioned, and abdominal compressions of 20, 40, 60, and 100 mm Hg were applied for 30 s each.
The next morning, approximately 18 h after ingestion of the labeled orange juice, a static, 10-min anteroposterior acquisition was obtained to check for aspiration of gastric contents into the lung fields. The subjects were supine, the oral cavity and thorax were included in the acquisition fields, and jugular marking was used as an anatomic reference point.
Image and Data Analysis
For gastroesophageal scintigraphy, regions of interest were placed on the esophageal body (in some instances, the esophagus was divided into 3 segments), on the gastric cavity, and on the right lung (background activity) to obtain time–activity curves with which to evaluate GER, esophageal transit time, esophageal emptying time, and gastric emptying.
The evaluation of GER involved visual confirmation of at least 1 episode of gastroesophageal radioactivity reflux lasting at least 10 s and having an activity at least 2% of the corresponding gastric activity. GER episodes were divided into distal, that is, reflux radioactivity limited to the distal third of the esophagus, and proximal, that is, reflux radioactivity detected throughout the esophageal body. Analysis of esophageal and gastric area-of-interest time–activity curves showed increased esophageal activity peaks and decreased gastric activity peaks in patients with GER, with the height of the peak being proportional to the amount of refluxed gastric content, and the width of the peak reflecting the duration of the reflux episode. Hence, the time–activity curve integral was proportional to the product of the amount of reflux and its duration.
Esophageal transit time (in seconds) was the interval between the entry of 50% of the radioactivity into the proximal esophagus and the elimination of 50% of the bolus from the entire esophagus. Esophageal emptying time (in seconds) was the interval between the entry of 50% of the radioactivity into the proximal esophagus and the clearance of 90% of the bolus from the entire esophagus. Gastric emptying was expressed as the gastric activity half-time (in minutes) obtained by interpolation from the gastric time–activity linear function, after decay correction.
For lung field scintigraphy, pulmonary aspiration of gastric contents was evaluated, including detection of airway activity, definition of its site, and, when feasible, calculation of percentage activity.
Statistical Analysis
The data were expressed as mean ± 1 SD. Statistical analysis was based on Kruskal-Wallis variance analysis and sample comparison by the Mann-Whitney nonparametric test. P < 0.05 was considered statistically significant.
RESULTS
Study Population
Three groups of patients could be identified. The first, representing 33% of enrolled patients, was 67 patients with no spontaneous or induced GER (GER-n) (38 females, 29 males; age range, 15–76 y; mean age, 47 ± 16 y). Of these 67 patients, 21 had known asthma, 3 were heavy smokers (>20 cigarettes per day), 6 had nodular thyroid disease, 9 had chronic lung disease, 5 were taking antibiotics for upper airway infections, and 6 were taking anxiolytic or antihypertensive medications. The second group was 134 patients with pathologic GER (GER-p) (93 females, 41 males; age range, 16–76 y; mean age, 51 ± 15 y). In 98% (131/134) of these patients, reflux was spontaneous, appearing before compression of the abdomen. The third group was a control group of 20 healthy volunteers with no symptoms and no reflux.
Patients with GER-p were divided into 2 subgroups depending on GER extension. The first was 30 patients with reflux limited to the distal third of the esophagus (GER-pd), or so-called distal reflux (20 females, 10 males; age range, 25–71 y; mean age, 53 ± 13 y). The second was 104 patients with reflux extending throughout the esophagus and into the oral cavity (GER-pp), or so-called proximal reflux (73 females, 31 males; age range, 16–76 y; mean age, 50 ± 16 y). Late static thoracic acquisitions revealed a further subgroup of 31 patients with lung radioactivity (pulmonary gastric aspiration, proximal [PGA-p]) (22 females, 9 males; age range, 22–72 y; mean age, 50 ± 16 y). All patient groups and the healthy volunteers were comparable in age and sex distribution, with no statistically significant differences.
Symptoms
None of the study participants reported experiencing epigastric pain, heartburn, acid regurgitation, or aerophagia during the preceding 6 mo. No statistically significant differences in symptom scores were observed between GER-n patients and GER-p patients, as shown in Table 1, nor were differences observed between GER-pp patients and GER-pd patients (see Table 2), even when the analysis was restricted to the most severe reported symptoms (scores 2 and 3). As shown in Tables 1 and 2, PGA-p patients had no difference in symptom scores, either overall or limited to scores 2 and 3, compared with patients having either no reflux or reflux not associated with aspiration.
Symptom Frequency Distribution in Patients with GER-n, GER-p, and PGA-p
Symptom Frequency Distribution in Patients with GER-pd, GER-pp, and PGA-p
Gastroesophageal Scintigraphy
Overall, 67% (134/201) of patients had positive gastroesophageal scintigraphy findings for reflux; 22% (30) of these had GER-pd, and the remaining 78% (104) had GER-pp. As shown in Table 3, statistically significant (P < 0.05) differences were seen between GER-pd and GER-p patients and between GER-pd and PGA-p patients in the frequency of reflux episodes, their maximal duration, and the overall duration and number of episodes recorded during the examination.
Episode Data
As shown in Table 4, no statistically significant differences were detected in esophageal functional parameters (i.e., esophageal transit and emptying times) or gastric motility (i.e., gastric emptying time) among the patient groups. In all patients, both esophageal transit times and emptying times were less than the mean plus 2 SDs obtained from healthy volunteers (Table 4). Gastric half-emptying time, however, was in all patients greater than the mean plus 2 SDs obtained from healthy volunteers (39 min), with the exception of those with distal reflux (35 min).
Esophageal and Gastric Motility Data
Lung Field Scintigraphy
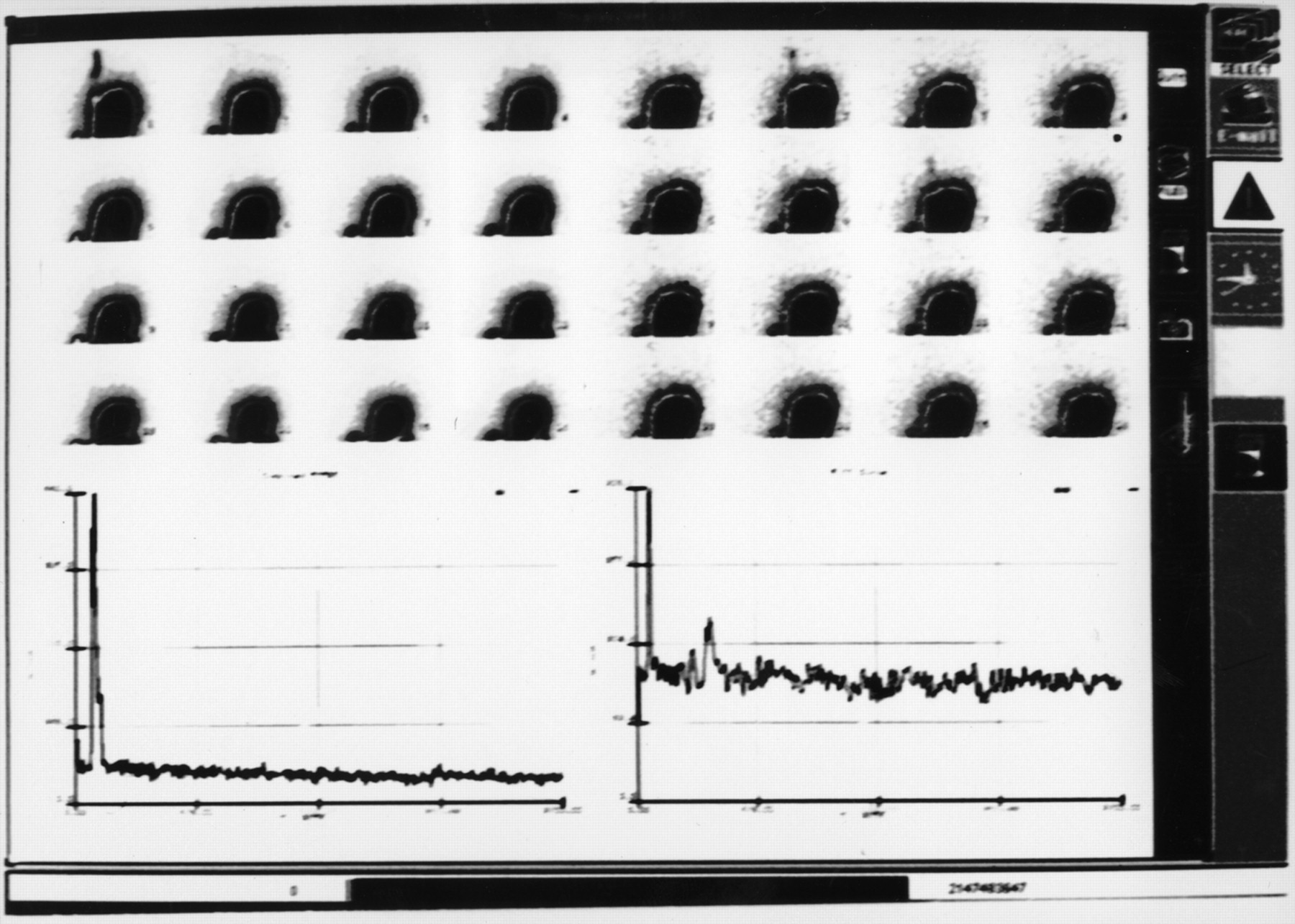
Thirty-one patients had PGA-p on late static acquisitions. These patients represented 30% (31/104) of GER-pp patients and 23% (31/134) of GER-p patients. Non–statistically significant differences in symptoms and esophageal or gastric functional parameters were detected between PGA-p patients and all other groups (Tables 1 and 2). Gastric and esophageal emptying times were significantly (P < 0.01) prolonged compared with those in healthy volunteers (Table 4). As for reflux characteristics (Table 3), a significant difference was detected between PGA-p patients and GER-pd patients (P < 0.001) but not between PGA-p patients and GER-pp patients. No GER-n patients, GER-pd patients, or healthy volunteers had detectable pulmonary activity on late static acquisitions. Figure 1 shows GER-pp (Fig. 1A) and GER-pd (Fig. 1B); Figures 2 and 3 show late pulmonary uptake, anterior and posterior views, respectively.

Dynamic scintigraphic images and time–activity curves from GER-pp patient (A) and GER-pd patient (B).
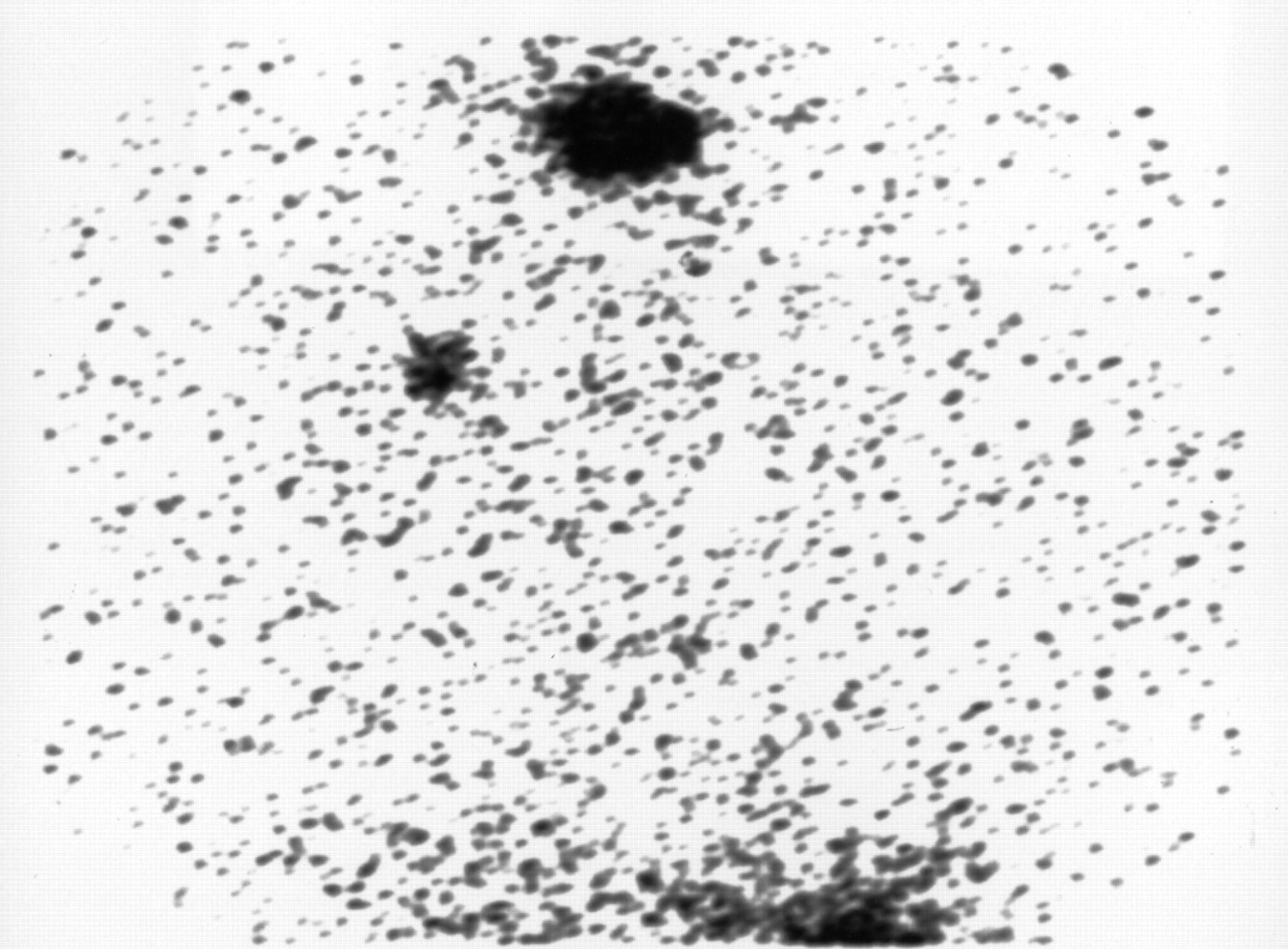
Anterior scintigraphic image from PGA-p patient.

Posterior scintigraphic image from PGA-p patient.
DISCUSSION
Several reports have pointed out an association between upper respiratory tract disturbances and acid reflux (6,8,16). Specifically, some authors have reported that patients with laryngitis have more GER episodes and longer exposure of the proximal esophagus to acid reflux than do healthy volunteers or, most important, patients with reflux but no laryngitis (9,17). A low pharyngeal pH, suggestive of a reflux episode, generally indicates contact of acid with the glottis and tracheobronchial tract, potentially inducing inflammatory changes of the pharyngeal and laryngeal mucosae (6,18–20). Moreover, even small quantities of acid may be responsible for significant damage to the laryngeal mucosa because it lacks the protective buffering effect of saliva (6). Protective mechanisms preventing acid exposure of the larynx include esophagoglottic, pharyngoglottic, and pharyngeal swallowing reflexes (21–23). Upper airway aspiration of gastric contents is generally of low volume and of limited duration; thus, a sensitive technique with prolonged monitoring is required for detection (15).
Our study population consisted of 201 patients with endoscopically documented posterior laryngitis; symptoms such as a dry cough, painful swallowing, or hoarseness; and no history of gastrointestinal tract disorders. Sixty-seven percent of these patients had scintigraphic evidence of pathologic GER, with most cases (78% of positive cases) including reflux up to the pharynx. Most of these patients had spontaneous reflux. This finding further underscores direct contact with gastric contents as the major cause of reflux-associated posterior laryngitis. In fact, the frequency of reflux episodes, their duration, and their percentage volume of gastric contents were significantly higher (P < 0.001) in GER-pp patients than in GER-pd patients, pointing out that what matters in the pathogenesis of reflux-associated posterior laryngitis is probably the duration of esophageal exposure to gastric contents rather than the reflux episode per se.
Among the GER-n patients, the 21 known to have asthma, the 9 with a history of chronic respiratory disorders, and the 5 with a recent upper respiratory infection had a possible alternative explanation for their nonspecific symptoms. In fact, we could not detect a significant association between symptoms and the presence and type of GER. This finding agrees with most reports (9,16,18,19,24). Moreover, in these patients, reflux could occur intermittently.
The esophageal motility of all patients was superimposable on that of healthy volunteers, whereas with the exception of GER-pd patients, every patient had delayed gastric emptying. These observations were independent of the presence of reflux and seem to support the hypothesis that reduced gastric motility may predispose to GER. The manometric studies of lower esophageal sphincter tone in the various groups may have helped elucidate this issue.
Lastly, 30% of patients with reflux had documentable pulmonary activity consistent with aspiration. Interestingly, all these patients had proximal reflux but no significant differences in symptoms, gastroesophageal motility, and number and duration of reflux episodes compared with patients who had proximal reflux and no pulmonary activity. A longer term of follow-up may clarify whether pulmonary aspiration has a negative prognostic value.
CONCLUSION
Gastroesophageal scintigraphy with evaluation of late lung fields is a sensitive, noninvasive way to detect proximal GER and respiratory complications in patients with posterior laryngitis and nonspecific symptoms. Our observation that a high percentage of patients with posterior laryngitis had reflux or gastric motility disturbances and pulmonary aspiration may be useful in the development of management strategies for posterior laryngitis.
Footnotes
Received Oct. 19, 1999; revision accepted Feb. 16, 2000.
For correspondence or reprints contact: Alberto Bestetti, MD, Servizio di Medicina Nucleare, Ospedale S. Paolo, Via Di Rudinì 8, 20142 Milano, Italy.




{kind=link}
{kind=link}
{kind=link}