


Abstract
This study was performed to compare 18F-FDG PET with CT for the evaluation of primary tumors and lymph node metastases in gastric cancer.
Methods: Eighty-one patients (28 women and 53 men; mean age, 56.6 y; age range; 32–82 y) who had undergone radical (n = 74) or palliative (n = 7) gastrectomy and lymph node dissection for the management of gastric cancer were included. Preoperative 18F-FDG PET and CT were reviewed retrospectively for primary tumors of the stomach and lymph node metastases. Any increased 18F-FDG uptake exceeding that of the adjacent normal gastric wall was considered positive for the primary tumor. Lymph nodes were classified into 3 groups based on their anatomic sites. Because perigastric lymph nodes (N1) were often not clearly differentiated from primary tumors, N1 lymph node metastases were determined when possible. Lymph nodes were considered positive or negative on the basis of the group as a whole. Final conclusions for primary tumors and lymph node metastases were based on histopathologic specimens in all patients.
Results: There were 17 patients with early gastric cancer (EGC) and 64 patients with advanced gastric cancer (AGC). For primary tumors, both PET and CT showed a sensitivity of 47% (8/17) for EGC and 98% (63/64) for AGC. The sensitivity of CT for N1 disease was significantly higher than that of PET. 18F-FDG PET had a sensitivity, specificity, and accuracy of 34% (11/32), 96% (47/49), and 72% (58/81), respectively, for N2 metastases, whereas the corresponding CT values were 44% (14/32), 86% (42/49), and 69% (56/81). For N3 metastases, PET and CT had the same sensitivity, specificity, and accuracy: 50% (3/6), 99% (74/75), and 95% (77/81), respectively. Overall, the sensitivity, specificity, and accuracy of 18F-FDG PET were not significantly different from those of CT for primary tumors or for N2 and N3 metastases.
Conclusion: 18F-FDG PET is as accurate as CT for the detection of primary tumors of either EGC or AGC. The low sensitivities of PET and CT were insufficient to allow decision making on the extent of lymphadenectomy. In contrast, the high specificity of PET for N disease appeared valuable, and the presence of N disease on PET may have a clinically significant impact on the choice of initial therapy.
At staging, one of the major contributions of 18F-FDG PET is in the detection of unsuspected metastases, leading to changes in therapeutic plans for patients with various malignancies. T staging of primary tumors typically requires a high-resolution anatomic imaging modality because exquisite anatomic details are mandatory in deciding on the surgical resectability of the primary tumors. Unlike anatomic imaging, 18F-FDG PET may have a role in predicting patient prognosis on the basis of the metabolic activity of primary tumors (1). The role of 18F-FDG PET in N staging, unlike T or M staging, seems to be difficult to elucidate because not every lymph node can accurately be confirmed histopathologically, and the evaluation of lymph nodes by individual location or number may not always be possible on 18F-FDG PET. Nevertheless, the superior accuracy of 18F-FDG PET, compared with conventional CT, has been well established in the evaluation of mediastinal lymph nodes in patients with non–small cell lung cancer (2). In patients with squamous cell carcinoma of the esophagus, 18F-FDG PET has proven more sensitive but less specific than CT for detecting lymph node metastases (3). The results of 18F-FDG PET for the axillary staging of breast cancer have been controversial, and sentinel lymph node sampling has been reported to have the lowest number of false-negative results (4). The value of 18F-FDG PET for detecting lymph node involvement is rather limited in patients with osteosarcoma, because metastases to the lymph nodes are rare in osteosarcoma tumors (5). The diagnostic performance of 18F-FDG PET for lymph node staging seems dependent on many factors, such as the avidity of primary tumors for 18F-FDG, the frequency of lymph node metastases, the size of metastatic lymph nodes, and the prevalence of chronic inflammatory diseases in certain areas. Thus, the value of 18F-FDG PET in evaluating lymph node metastases needs to be elucidated according to each type of malignant tumor.
Accurate staging is essential for selecting preoperative surgical strategies for gastric cancer. Adjacent organ involvement, peritoneal carcinomatosis, and distant metastases are important factors for determining the surgical resectability of disease. Although effective for detecting nonskeletal distant metastasis, 18F-FDG PET may not be the most useful imaging modality for evaluating adjacent organ invasion and peritoneal carcinomatosis (6). Unless paraaortic lymph node metastasis is clearly evident, other extragastric lymph node metastases may not affect the surgical resectability of gastric cancer. However, lymph node staging is extremely important for planning the optimal extent of lymphadenectomy. Although CT has been the modality of choice, its accuracy is based solely on the size of lymph nodes—a criterion that is insufficient to guide therapeutic plans. Likewise, lymph node staging by other conventional imaging modalities such as endoscopic ultrasonography and MRI is considered insufficiently accurate for deciding on the extent of lymphadenectomy. This retrospective study was performed to compare the diagnostic performance of 18F-FDG PET with that of CT, mainly for detection of lymph node metastases in patients with gastric cancer.
MATERIALS AND METHODS
Patients
Eighty-one patients (28 women and 53 men; mean age, 56.6 y; age range; 32–82 y) who had undergone radical (n = 74) or palliative (n = 7) gastrectomy and D2 (n = 68), D3 (n = 7), or D4 (n = 6) lymph node dissection for the management of gastric cancer were included in this study. D2 procedures were used for dissection of lymph nodes at the N1 and N2 levels; D3 procedures, for the N3 level; and D4 procedures, for the N4 level, in accordance with the Japanese nodal staging system (7). Within 2 wk of each other, preoperative 18F-FDG PET and CT were performed on all patients, and the images were reviewed retrospectively for evidence of primary tumors of the stomach and for lymph node metastases. The primary tumors were categorized as early gastric cancer (EGC), limited to the mucosa or mucosa and submucosa (T1), or advanced gastric cancer (AGC), including T2, T3, or T4 tumors. No patient had undergone preoperative chemotherapy or radiotherapy.
Imaging Procedures
For PET, patients fasted at least 4 h before the intravenous injection of 18F-FDG, and scanning began 60 min afterward. Images from the neck to the proximal thigh were obtained either on an Advance PET scanner (GE Healthcare), with a spatial resolution of 5 mm in the center of the field of view, or on an Allegro PET scanner (Philips-ADAC Medical Systems), with a spatial resolution of 5.3 mm in the center of the field of view. For the Advance, approximately 370 MBq of 18F-FDG were intravenously injected, and the emission scan was acquired for 5 min per bed position in 2-dimensional mode. The Allegro acquired data in 3-dimensional mode after administration of 5.18 MBq (0.14 mCi)/kg of 18F-FDG. Transmission scans (3 min per bed position) to correct for nonuniform attenuation were obtained using 68Ge for the Advance or 137Cs point sources for the Allegro. Transmission scans were interleaved between the multiple emission scans for the Allegro. The images were reconstructed using an iterative reconstruction algorithm, that is, either the ordered-subset expectation maximization for the Advance or the low-action maximal-likelihood algorithm for the Allegro.
CT of the abdomen and pelvis was performed on 1 of 3 scanners (LightSpeed Plus or HiSpeed CT/I; GE Healthcare, or Sensation 16; Siemens) using reconstruction thicknesses of 3.75, 5, and 3 mm, respectively. Enhanced CT scans were obtained after a bolus intravenous injection of a 60% w/v contrast medium (approximately 90% higher-osmolarity agents and 10% lower-osmolarity agents) at 2–4 mL/s from a volume of 2 mL/kg up to a maximum volume of 150 mL.
Data Analysis
Two experienced nuclear medicine physicians who were unaware of other clinical or imaging information read the 18F-FDG PET images on a high-resolution computer screen. The readers reached a consensus in cases of discrepancy. For primary tumors of the stomach, any increased 18F-FDG uptake exceeding that of the adjacent normal gastric wall was considered positive for malignancy. On the other hand, any mucosal irregularity, mass, or focal or diffuse enhancement on CT was considered a primary tumor. In addition, a region of interest was drawn over the site of the most intense 18F-FDG uptake in the primary tumor, and the average standardized uptake value (SUV) corrected for total body weight was taken for semiquantitative analysis of PET. A minimum region-of-interest diameter of 6 pixels was used in 2 patients with EGC tumors measuring less than 1 cm. In patients with AGC, histologic and macroscopic types of primary tumors were compared using SUVs.
Abdominal lymph nodes were classified into 3 groups based on anatomic location. The N1 group included perigastric lymph nodes attached to the stomach; the N2 group included lymph nodes along the left gastric artery, common hepatic artery, celiac artery, or splenic artery or at the splenic hilum; and the N3 group included lymph nodes in the hepatoduodenal ligament, retropancreatic artery, mesenteric artery, mid colic artery, or paraaortic regions. According to the guidelines of the Japanese Research Society for Gastric Cancer, lymph nodes along the mid colic artery and paraaortic regions are classified as N4 (7). However, we combined N3 and N4 groups into N3 for statistical purposes because there were only a few lymph nodes in these groups. A lymph node with 18F-FDG uptake similar to or higher than that of the liver was considered positive for metastasis. Because perigastric lymph nodes (N1) were often not clearly differentiated from the primary tumors, N1 metastasis was determined whenever possible. Any lymph node of 8 mm or larger was considered metastatic on CT. Lymph nodes were considered positive or negative on the basis of the group as a whole, that is, positive if one or more lymph node metastases were discernible in the group and negative if none was discernible.
Final conclusions on the presence of lymph node metastases were based on the results of histopathologic examination of specimens. The absence of N3 disease could not be histopathologically confirmed in this study because only 13 of the 81 patients underwent D3 or D4 lymph node dissection. The following criteria were used to verify the absence of N3 disease: no N3 lymph node found on preoperative PET and CT, no lymph node enlargement found during the operation, and no lymph node enlargement found on follow-up CT.
Statistical Analysis
The sensitivity, specificity, accuracy, negative predictive value (NPV), and positive predictive value (PPV) of each modality were calculated for detection of primary tumors and lymph nodes according to the groups. The χ2 test was performed to determine differences in diagnostic performance between the 2 imaging modalities. Statistical significance was assumed when a P value was less than 0.05.
In patients with AGC, histologic and macroscopic types of primary tumors were compared with SUVs using the Student t test and 1-way ANOVA, respectively. P values of less than 0.05 were considered significant.
RESULTS
Primary Tumors
The patient characteristics and pathologic data are summarized in Table 1. There were 17 patients with EGC and 64 patients with AGC. Both PET and CT detected 47% (8/17) of EGC and 98% (63/64) of AGC (Fig. 1). Of the 63 AGC tumors detected on PET, 5 showed only mildly increased 18F-FDG uptake compared with that of the adjacent gastric wall. The mean SUVs of the primary tumors were 2.8 ± 1.6 (range, 1.6–3.3) for EGC and 7.9 ± 8.0 (range, 1.9–55) for AGC.

EGC, Bormann type I. PET images demonstrate focus of increased 18F-FDG uptake on sagittal (A) and axial (B) views, and CT shows protruding mass (arrow) (C) in posterior wall of antrum of stomach.
Patient Characteristics
Of the 64 patients with AGC, 36 had poorly differentiated tubular adenocarcinoma (mean SUV, 6.8 ± 5.5), 22 had moderately differentiated tubular adenocarcinoma (mean SUV, 10.5 ± 11.3), 4 had signet ring carcinoma (mean SUV, 4.1 ± 0.9), 1 had well-differentiated tubular adenocarcinoma (SUV, 5.6), and 1 had lymphoepitheliomalike carcinoma (SUV, 5.4). Statistical analysis was performed only between moderately differentiated and poorly differentiated tubular adenocarcinomas because the numbers of cases for the rest of the histologic types seemed insufficient. Although the mean SUV of moderately differentiated tubular adenocarcinoma appeared to be higher than that of poorly differentiated tumors, the difference was not statistically significant.
AGC tumors were categorized according to macroscopic types of primary tumors. There were 9 polypoid tumors (type I; n = 9; mean SUV, 18.6 ± 15.9), 21 ulcerofungating tumors (type II; n = 21; mean SUV, 7 ± 3.9), 22 ulceroinfiltrative tumors (type III; n = 22; mean SUV, 6.2 ± 4.2), and 12 diffusely infiltrative tumors (type IV; n = 12; mean SUV, 4.3 ± 2.1). When the SUVs of the primary tumors were compared with macroscopic types, a statistically significant difference in mean SUV was found between type I and the rest of the 3 macroscopic tumor types (P < 0.0001).
Lymph Node Staging
Using histopathology as a gold standard for lymph node metastasis, N1 disease was present in 53 (65%), N2 in 32 (40%), and N3 in 6 (7%) of 81 patients. 18F-FDG PET had a sensitivity, specificity, accuracy, PPV, and NPV of 34% (18/53), 96% (27/28), 56% (45/81), 95% (18/19), and 44% (27/62), respectively, for N1 disease and 34% (11/32), 96% (47/49), 72% (58/81), 85% (11/13), and 69% (47/68), respectively, for N2 disease (Table 2). The corresponding values for CT were 58% (31/53), 89% (25/28), 69% (56/81), 91% (31/34), and 53% (25/47), respectively, for N1 and 44% (14/32), 86% (42/49), 69% (56/81), 67% (14/21), and 70% (42/60), respectively, for N2 (Figs. 2 and 3). For N3 lymph node metastases, PET and CT had the same sensitivity, specificity, accuracy, PPV, and NPV: 50% (3/6), 99% (74/75), 95% (77/81), 75% (3/4), and 96% (74/77), respectively (Fig. 4).

Patient with AGC and pathologically proven N1 metastasis. (A) 18F-FDG PET shows mass with increased 18F-FDG uptake in body of stomach without perigastric lymph node metastasis. (B) Perigastric lymph node (arrow) is noted on CT. Sensitivity of CT is significantly higher than that of PET for N1 disease.

N2 metastasis (arrow) in region of common hepatic artery on 18F-FDG PET sagittal (A) and axial (B) views and on CT (C). For N2 disease, CT appears to be more sensitive than PET, whereas PET appears more specific than CT.

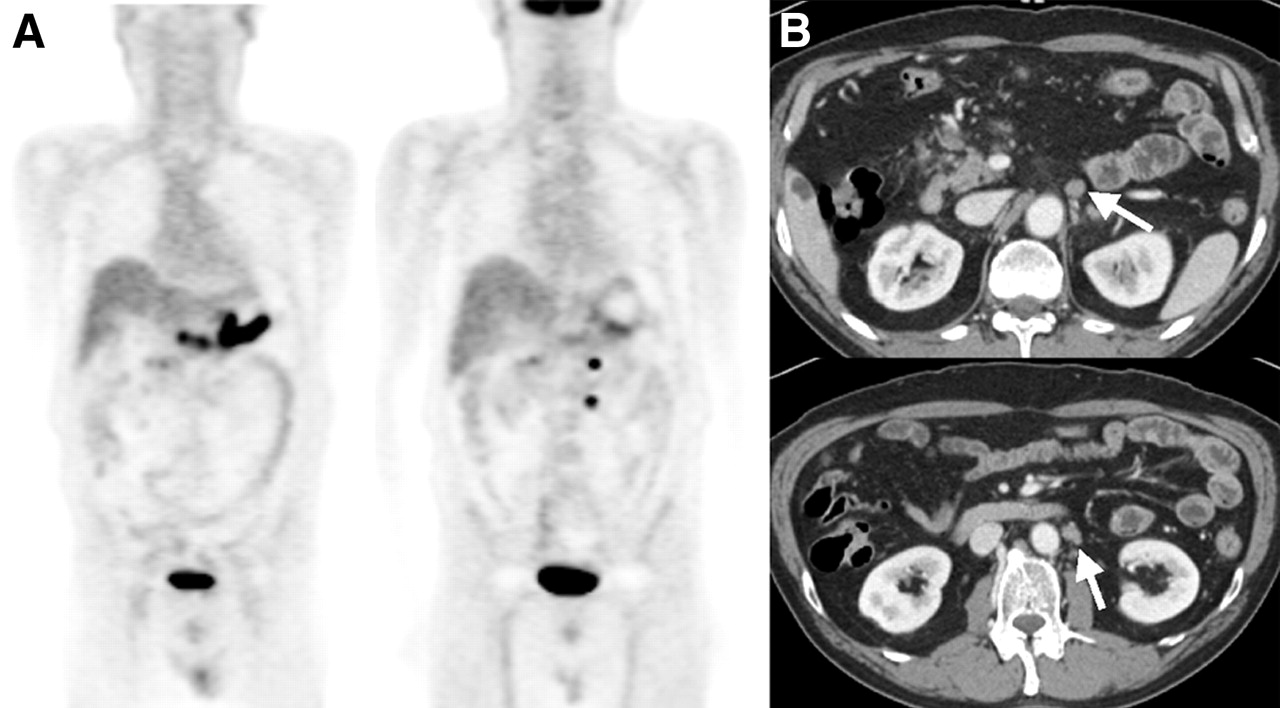
Two N3 metastases (arrows) in left paraaortic space on 18F-FDG PET (A) and CT (B). Both PET and CT are insensitive but highly specific for N3 disease.
Performance of 18F-FDG PET and CT for Lymph Node Staging
Although PET and CT showed sensitivities insufficient for N staging, the sensitivity of CT was significantly higher than that of PET for N1 disease. CT appeared to be more sensitive than PET for N2 disease, but the difference was not statistically significant. The N2 lymph nodes seen only on CT numbered 6 and were between 8 and 10 mm in size. The poorer sensitivity of PET for N2 disease could have been due to a partial-volume averaging effect. Regardless of the poor sensitivities for N1 and N2 disease, PET correctly detected 3 of 22 false-negative N1 nodes and 3 of 18 false-negative N2 nodes on CT. This finding, by suggesting that PET has value in identifying the additional patients with lymph node metastases not seen on CT, seems important. CT and PET had the same low sensitivity of 50% for detecting N3 disease. On the other hand, PET and CT had better specificities than sensitivities for N staging. The specificities of PET for N staging were not significantly different from those of CT, although PET seemed to be slightly more specific for N2 disease.
Both PET and CT had PPVs of more than 90% for N1 disease and the same highest NPV of 96% for N3 disease, which was clearly affected by the prevalence of lymph node disease in each group. For N2 disease, the PPV of PET was higher than that of CT, but without statistical significance.
When the performance of 18F-FDG PET and CT for lymph node staging was evaluated separately for EGC and AGC, no difference in results was noted between both tumors. In cases of EGC, it was difficult to assess the significance of the low sensitivities for both PET and CT because of the limited number of metastatic lymph nodes seen in this subgroup. However, both PET and CT showed the same high specificity of 100%.
Other Findings
Two patients had metastases that were missed on PET and CT but identified at surgery. One of these patients had peritoneal seeding nodules, and the other had a mediastinal lymph node metastasis.
DISCUSSION
Mass screening programs based on barium studies or endoscopy have contributed to the detection of gastric cancer at earlier stages and, consequently, have improved long-term survival rates (8). After detection, surgical resection for localized disease is considered to be the only treatment option with curative potential. Although endoscopic ultrasonography is excellent for locoregional staging, patient discomfort and tumor stenosis limit its use (9). Other than endoscopic ultrasonography, CT has been widely used as the first-line imaging modality to determine the resectability of gastric cancer. It evaluates a fat plane between the primary tumor and an adjacent organ such as liver or pancreas to help the surgeon decide whether the tumor is resectable. CT also plays an important role in assessing the presence of peritoneal carcinomatosis, which is one of the most common causes of futile laparotomies. However, the limited accuracy of CT is well known and prevents differentiation between metastatic and enlarged benign lymph nodes (10,11).
The presence of lymph node metastases is considered to be one of the most important prognostic factors in gastric cancer. Other than the prognostic information, accurate staging of lymph node disease is necessary in planning the extent of lymph node dissection for the management of patients with resectable disease. However, whether a curative resection should include an extended (D2) instead of a limited (D1) lymph node dissection is unclear (12–16). Bonenkamp et al. reported that patients with D2 lymph node resection have a higher operative mortality rate, more complications, and a longer postoperative hospital stay (17). Those authors proposed that D2 lymph node dissection not be used routinely in patients with gastric cancer. However, a 5-y survival rate of 20%–39.2% was reported in a review of the survival data of patients who had undergone D2 dissection for the curative resection of N2 disease (13). The benefit from D2 dissection was found to be substantial, offering long-term survival in patients with N2 disease (18). Moreover, because no adjuvant therapy after D1 dissection has been shown to be more effective than D2 dissection alone, it was recommended as the only treatment modality to achieve curative results for N2 disease. So far, we lack a method capable of staging N disease accurately enough to enable decision making on the extent of lymph node dissection.
In this study, we compared the diagnostic performance of 18F-FDG PET with that of CT for the evaluation of lymph node metastases using histopathology as a gold standard. Despite its high specificity, PET was less sensitive than CT for the detection of N1 disease, probably because the spatial resolution of PET was too low to discriminate perigastric lymph nodes from primary tumors. Actually, the presence or absence of N1 disease may not make a difference in patients with AGC because all will undergo at least D1 dissection. What appears to be of clinical importance is the determination of N2 or N3 disease status, because the presence of N2 disease may change the extent of lymph node dissection from D1 to D2 or more, and the curative potential of surgery may be decreased given evidence of N3 disease. Our results showed that both modalities have low sensitivities for assessing N2 and N3 disease. The absence of lymph node metastases in N2 or N3 groups on CT or PET appears to be insufficient for determining the extent of lymph node dissection. On the other hand, PET and CT showed high specificities for N2 disease. The specificity of PET was higher than that of CT, but without statistical significance. Given the high specificity of 18F-FDG PET for N2 disease, at least D2 lymph node dissection is needed to achieve curative resection when N2 disease is evident on PET. The same holds true for the presence of N3 disease on both 18F-FDG PET and CT. The high specificity, 99%, for PET and CT may play an important role in extending the degree of lymphadenectomy or reducing futile laparotomies in cases of paraaortic lymph node metastasis. In contrast to the results in N1 and N2 diseases, PET and CT showed the same performance for N3 disease. It seems that the low prevalence (6%) of N3 metastasis in this study may be inadequate to accurately compare the diagnostic performance of 2 modalities.
Because of mass screening programs, EGC accounts for a significant portion of gastric cancers—up to 20%. The prognosis of EGC is excellent with radical gastrectomy, and the reported cumulative 5-y survival rate exceeds 95% regardless of the status of lymph node metastases (19). This success in survival has introduced the concept of minimally invasive treatment with no or limited lymph node dissection in the management of EGC. Endoscopic mucosal resection, laparoscopic surgery, or limited resection by open surgery for gastric cancer has been proposed as the initial treatment of choice in some patients with EGC (20–22). However, the application of minimally invasive surgery is limited in lymphadenectomy and may result in tumor recurrence. Therefore, the preoperative staging of lymph node status is particularly important in selecting patients who would benefit from minimally invasive surgery. N2 disease needs invasive surgery with extended lymph node dissection rather than minimally invasive surgery with limited lymph node dissection. The presence of N1 disease is important when deciding on the type of minimally invasive surgery for EGC, unlike AGC. Endoscopic mucosal resection is indicated for EGC tumors without lymph node involvement, and laparoscopic or open gastrectomy with limited lymph node dissection would be sufficient for mucosal cancer with lymph node metastases (23). On the basis of our results, the low sensitivities of both PET and CT appear to be problematic in terms of detecting N1 disease. In contrast, PET showed a very high specificity for N1 disease, and limited lymph node dissection rather than endoscopic mucosal resection should be encouraged for patients with N1 disease on PET.
It is well known that 18F-FDG uptake is low in some histologic types of gastric cancer, such as signet ring cell and mucinous carcinomas, because of an extracellular or intracellular mucin component (24). Our data also appeared to show relatively lower 18F-FDG uptake in signet ring cell carcinoma than in moderately or poorly differentiated tubular adenocarcinoma. However, the number of cases with signet ring histology was too small for statistical significance to be drawn. In addition to our sensitive reading for the detection of primary tumors on PET, we believe that the small number of patients with signet ring cell carcinoma could be reason for the high detection rate, 98%, for AGC in this study. Low 18F-FDG uptake was also reported in poorly differentiated types of primary lesions and was attributed to the low concentration of cancer cells (6). In this study, the mean SUV of poorly differentiated tubular adenocarcinomas appeared to be lower than that of moderately differentiated tumors, but the difference was not statistically significant. We also found that poorly differentiated tubular adenocarcinomas showed an especially wide spectrum of 18F-FDG uptake, from low to intense. Other factors besides histologic grade seemed to affect the degree of 18F-FDG uptake in poorly differentiated tubular adenocarcinomas. Further studies are needed, including studies of the effect of detailed histologic features on 18F-FDG uptake in these tumors. Of the macroscopic types of primary tumors, type I showed significantly greater 18F-FDG uptake than did the other 3 types. The mass-forming growth of type I may have been associated with the high 18F-FDG uptake observed in this macroscopic type.
CONCLUSION
18F-FDG PET is as accurate as CT for detecting primary tumors of the stomach in either EGC or AGC. Until now, no imaging modality had been available to enable decision making on the extent of lymphadenectomy in patients with gastric cancer. Our study showed that the low sensitivities of PET and CT are insufficient to resolve this issue although PET can detect some additional lymph node metastases not seen on CT. Nevertheless, PET and CT show high specificities for N disease, and the specificities of PET are the same as or higher than those of CT. Evidence of N1 disease on PET may change endoscopic mucosal resection to a more aggressive surgical approach in patients with EGC. The high specificity of 18F-FDG PET for N2 disease may play an important role in avoiding limited lymph node dissection for advanced disease. Finally, N3 disease on PET may indicate the need for further aggressive lymphadenectomy or reduce the number of futile laparotomies in cases of paraaortic lymph node metastasis.
Acknowledgments
We thank Sungsook Yeon for her assistance with data preparation.
Footnotes
Received Mar. 4, 2005; revision accepted Jul. 7, 2005.
For correspondence or reprints contact: Sung Hoon Noh, MD, Department of Surgery, Yonsei University, College of Medicine, 134 Shinchon-dong, Seodaemoon-ku, Seoul, Korea, 120-752.
E-mail: tsangel{at}yumc.yonsei.ac.kr
REFERENCES
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Surgical Resection First for Localized Gastric Adenocarcinoma: Are There Adjuvant Options?
- Relationship Between 18F-FDG Uptake on PET and Recurrence Patterns After Curative Surgical Resection in Patients with Advanced Gastric Cancer
- Improving Patient Selection for 18F-FDG PET Scanning in the Staging of Gastric Cancer
- NCCN Task Force: Clinical Utility of PET in a Variety of Tumor Types
- Modern Surgical Considerations for Gastric Cancer
- Imaging Gastric Cancer with PET and the Radiotracers 18F-FLT and 18F-FDG: A Comparative Analysis