


Abstract
This study evaluated the predictive value of 18F-FDG PET for distant metastasis-free survival and peritoneal recurrence-free survival as well as recurrence-free survival and overall survival after curative surgical resection in patients with advanced gastric cancer (AGC). Methods: Two hundred seventy-nine patients with AGC who underwent preoperative 18F-FDG PET and subsequent curative surgical resection were included. The tumor–to–normal liver uptake ratio (TLR) of cancer lesions was measured, and the prognostic significance of TLR and tumor factors for distant metastasis-free survival, peritoneal recurrence-free survival, recurrence-free survival, and overall survival was assessed. Results: The 5-y recurrence-free survival, peritoneal recurrence-free survival, distant metastasis-free survival, and overall survival rates were 46.9%, 68.5%, 76.0%, and 58.1%, respectively. Depth of tumor invasion, lymph node metastasis, lymphovascular invasion, and TLR were independent prognostic factors for both recurrence-free survival and overall survival (P < 0.05). For distant metastasis-free survival, lymphovascular invasion and TLR were independent risk factors (P < 0.05). In patients with a TLR of 2.0 or less, the 5-y distant metastasis-free survival rate was 95.5%; in patients with a TLR greater than 2.0, the 5-y distant metastasis-free survival rate was 68.8%. For peritoneal recurrence-free survival, TLR showed no statistical significance (P = 0.7) whereas pT stage, lymph node metastasis, Lauren classification, and Bormann type were independent prognostic factors (P < 0.05). Conclusion: 18F-FDG uptake of AGC is an independent prognostic factor for distant metastasis-free survival, recurrence-free survival, and overall survival. The possibility of distant metastasis during follow-up should be considered in patients with high 18F-FDG uptake.
Advanced gastric cancer (AGC) continues to have a poor prognosis and is one of the most common causes of death from malignancy in eastern Asia (1–3). The only curative treatment modality for AGC patients without distant metastasis is radical surgical resection. However, gastric cancer often recurs after curative surgical resection, at a rate of 12%–48%, and death from gastric cancer is mainly due to cancer recurrence (4–6). Although early detection of cancer recurrence is important for improving prognosis, detection is difficult in some of the AGC patients because of varying recurrence patterns such as locoregional recurrence, peritoneal recurrence, and distant metastasis. Moreover, adjuvant treatment such as intraperitoneal chemotherapy focuses on specific sites of potential recurrence (7,8). Hence, understanding the relationship between clinicohistopathologic factors and patterns of cancer recurrence could help in planning adjuvant treatment and selecting diagnostic studies during the follow-up (5,8).
18F-FDG PET has been widely used in patients with gastric cancer. Although 18F-FDG PET has low sensitivity for detecting early gastric cancer and lymph node metastasis, 18F-FDG PET has high detection rates for recurrent cancer lesions and high specificity for N2 or N3 lymph node metastasis (9–12). In addition, 18F-FDG uptake of primary gastric cancer lesions is a significant prognostic factor for predicting cancer recurrence after surgical resection (13–15). Because 18F-FDG uptake of gastric cancer is related to the tumor aggressiveness and histopathology (9,16), patients with high 18F-FDG uptake can have different cancer recurrence patterns than patients with low 18F-FDG uptake. However, no studies have evaluated the relationship between 18F-FDG uptake of the primary gastric cancer and patterns of gastric cancer recurrence.
In the present study, we evaluated the relationship between 18F-FDG uptake of AGC and patterns of cancer recurrence and assessed the significance of 18F-FDG PET for predicting distant metastasis-free survival, peritoneal recurrence-free survival, recurrence-free survival, and overall survival.
MATERIALS AND METHODS
Patients
We retrospectively reviewed the medical records of 4,917 patients who underwent surgical resection for gastric cancer in our hospital between May 2003 and April 2009. Of these patients, 279 with AGC (pT2–T4 stage) who underwent preoperative staging 18F-FDG PET and subsequent curative surgical resection were enrolled in this study. Patients who had a history of another malignancy, received neoadjuvant treatment before surgical resection of the AGC, were lost to follow-up, or underwent palliative surgery were excluded from the study. Patients with early gastric cancer (pT1 stage, irrespective of lymph node metastasis) were also excluded to avoid the partial-volume averaging effect, which would affect the measurement of 18F-FDG uptake of gastric cancer lesions. The Institutional Review Board of our university approved this retrospective study, and the requirement to obtain informed consent was waived.
All patients underwent subtotal or total gastrectomy with at least D2 lymph node dissection (17). In histopathologic evaluation of dissected AGC lesions, the tumors were classified into the 4 Borrmann macroscopic growth types and the 2 microscopic growth types on the basis of the Lauren classification (intestinal and nonintestinal). Diffuse, mixed, and nonclassifiable types in the Lauren classification were included in nonintestinal type (13,18). AGC histopathologic subtypes were categorized into papillary adenocarcinoma, well-differentiated and moderately differentiated tubular adenocarcinoma, poorly differentiated adenocarcinoma, signet-ring cell carcinoma, and mucinous adenocarcinoma according to the Japanese Gastric Cancer Association system (19). Tumor size was measured at the longest diameter of the dissected tumor lesion.
After surgical resection of the AGC, 214 patients underwent postoperative adjuvant treatment (adjuvant chemotherapy, 198 patients, and adjuvant chemotherapy and radiotherapy, 16 patients) on the basis of histopathologic results and the patient’s clinical conditions. In the first 3 y after surgery, gastroduodenoscopy, contrast-enhanced CT, and blood tests were performed every 6–8 mo. Subsequent, follow-up studies were performed every 10–12 mo. Median follow-up was 51.7 mo (range, 3.1–131.7 mo). Patients with cancer recurrence were classified into 3 groups according to the first site of recurrence: locoregional recurrence, peritoneal recurrence, or distant metastasis. Patients with peritoneal seeding nodules, massive ascites, abnormal intestinal wall thickening, increased mesentery density, peribiliary tumor infiltration, or Krukenberg tumors were classified in the peritoneal recurrence group (7). Patients with hematogenous and distant lymph node metastases were classified in the distant metastasis group.
18F-FDG PET
18F-FDG PET scans were obtained using a dedicated PET scanner (Advance [GE Healthcare] or Gemini [Philips-ADAC Medical Systems]) or a dedicated PET/CT scanner (Discovery Ste; GE Healthcare). All patients were instructed to fast for at least 4 h before 18F-FDG administration. PET or PET/CT was performed 60 min after intravenous injection of 370 MBq, 5.18 MBq/kg, and 5.5 MBq/kg of 18F-FDG for the Advance, Gemini, and Discovery Ste scanners, respectively. All PET images were acquired from the neck to the proximal thigh. For PET scans, emission scans were obtained with 5 min per bed position in 2-dimensional mode for the Advance and in 3-dimensional mode for the Gemini scanners. Transmission scans using 68Ge for the Advance or 137Cs point sources for the Gemini were acquired with 3 min per bed position to correct for nonuniform attenuation. Transmission scans were obtained after completing emission scans for the Advance or interleaved between multiple emission scans for the Gemini. In PET/CT, CT scans were initially obtained at 30 mA and 130 kVp without contrast enhancement. Afterward, PET scans were obtained with 3 min per bed position in 3-dimensional mode. PET images were reconstructed using an iterative algorithm, either the ordered-subset expectation maximization for the Advance and Discovery STe or the low-action maximal-likelihood algorithm for the Gemini.
Image Analysis
All 18F-FDG PET images were retrospectively evaluated by 2 nuclear medicine physicians masked to the clinical outcome of the patients. For semiquantitative analysis, the uptake ratio of the maximum standardized uptake value (SUV) of the primary tumor–to–mean SUV of normal liver (TLR) was measured in all patients. SUV was calculated as (decay-corrected activity [kBq] per tissue volume [mL])/(injected 18F-FDG activity [kBq] per body mass [g]). A circular region of interest was drawn over the site of the most intense 18F-FDG uptake in the gastric cancer lesion on transaxial 18F-FDG PET images, and maximum SUV of the gastric cancer was measured. In patients with no visible focally increased 18F-FDG uptake in the stomach, a region of interest was drawn according to the tumor location seen on contrast-enhanced CT images and gastroduodenoscopy. For measuring normal liver 18F-FDG uptake, 3 circular 1-cm-sized regions of interest were drawn, 2 in the right lobe and 1 in the left lobe. The mean value of the mean SUV of the 3 regions of interest was calculated and defined as mean SUV of normal liver, and TLR was calculated. Because different PET and PET/CT scanners were used in the study, only TLR was used as the PET parameter in statistical analysis.
Statistical Analysis
Differences in variables between patient groups were analyzed using the Student t test, Kruskal–Wallis test, and χ2 test. Survival curves were estimated using the Kaplan–Meier method to calculate cumulative recurrence-free survival, distant metastasis-free survival, peritoneal recurrence-free survival, and overall survival rates. Survival time was defined as time from operation to day of the occurrence of an event such as cancer recurrence, distant metastasis, peritoneal recurrence, or death. Data for patients without recurrence or death were censored at date of the last follow-up visit at our medical center. For statistical analyses, all variables for survival analysis were grouped into 2 categories according to specific cutoff values. Optimal cutoff values for continuous variables were determined using receiver-operating-characteristic curve analysis. The significance of the predictive value of each variable was analyzed using the log-rank test for univariate analysis and Cox proportional hazards regression test for multivariate analysis. Statistical analyses were performed using SPSS (version 20.0 for Windows; SPSS Inc.), and a P value of less than 0.05 was considered statistically significant.
RESULTS
Patient Characteristics
Of the 279 patients enrolled, 148 (53.1%) experienced recurrence and 120 (43.2%) died during clinical follow-up. Among 148 patients with documented recurrence, 116 (78.4%) experienced recurrence within the first 2 y. The most frequent site of recurrence was peritoneal recurrence (n = 80, 54.1%), followed by distant metastasis (n = 63, 42.6%) and locoregional recurrence (n = 31, 20.9%; Fig. 1). The most common site of distant metastasis was distant lymph node, followed by the liver, bone, and lung. The 5-y recurrence-free survival was 46.9%, peritoneal recurrence-free survival was 68.5%, distant metastasis-free survival was 76.0%, and overall survival rate was 58.1%. The pT stage, pN stage, tumor size, presence of lymphovascular invasion, Bormann type, adjuvant treatment, and TLR were significantly different between patients with and without recurrence (P < 0.05; Table 1). In the 148 patients with cancer recurrence, the Kruskal–Wallis test showed significant differences in TLR between 63 patients with distant metastasis (median, 2.7; range, 1.4–12.5), 70 patients with peritoneal recurrence without distant metastasis (median, 1.8; range, 0.9–13.7), and 15 patients with locoregional recurrence without peritoneal recurrence or distant metastasis (median, 2.5; range, 2.0–11.2; P < 0.0001). Post hoc analysis revealed that patients who experienced recurrence with distant metastasis and locoregional recurrence had significantly higher TLRs than patients with peritoneal recurrence (P < 0.05).

First sites of recurrence in enrolled 279 patients after curative surgical resection.
Patient Characteristics According to Cancer Recurrence
Prognostic Factors for Recurrence and Overall Survival
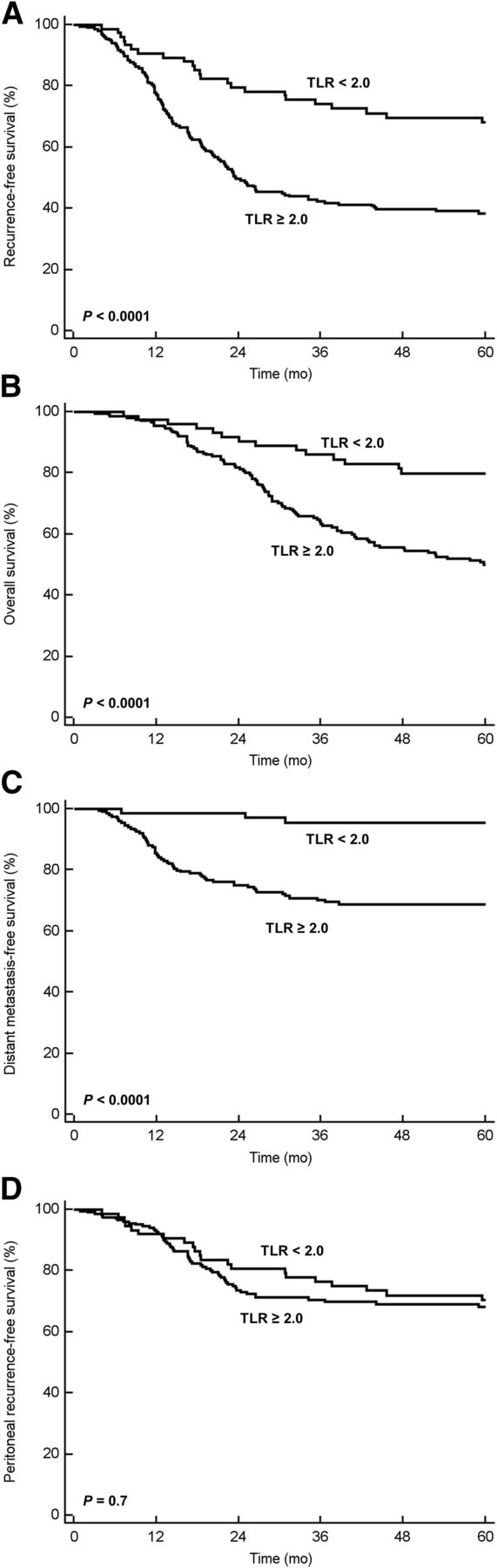
The significance of prognostic factors in univariate and multivariate analyses is shown in Table 2 for recurrence-free survival and Table 3 for overall survival. Optimal cutoff values were 60 y for age, 5.0 cm for tumor size, and 2.0 for TLR, as determined by receiver-operating-characteristic curve analysis. In multivariate analysis, pT stage, lymph node metastasis, lymphovascular invasion, and TLR were significant independent prognostic factors for both recurrence-free survival (Fig. 2A) and overall survival (Fig. 2B; P < 0.05). Bormann type was an independent prognostic factor for recurrence-free survival only (P = 0.02), and tumor size was an independent prognostic factor for overall survival only (P = 0.01).
Prognostic Factors for Recurrence-Free Survival
Prognostic Factors for Overall Survival

Cumulative recurrence-free survival curve (A), cumulative overall survival curve (B), cumulative distant metastasis-free survival curve (C), and cumulative peritoneal recurrence-free survival curve (D) according to TLR in enrolled 279 patients.
In addition to recurrence-free survival and overall survival, the significance of variables for predicting distant metastasis-free survival and peritoneal recurrence-free survival was also assessed (Tables 4 and 5). In multivariate analysis, only lymphovascular invasion and TLR (Fig. 2C) were determined to be independent risk factors for distant metastasis-free survival (P < 0.05). The 5-y distant metastasis-free survival rate was 95.5% for patients with a TLR of 2.0 or less, whereas in patients with a TLR greater than 2.0, the 5-y distant metastasis-free survival rate was only 68.8%. In contrast to distant metastasis-free survival, TLR showed no statistical significance for predicting peritoneal recurrence-free survival (Fig. 2D; P = 0.7). However, pT stage, lymph node metastasis, Lauren classification, and Bormann type were independent prognostic factors for peritoneal recurrence-free survival (P < 0.05).
Prognostic Factors for Distant Metastasis-Free Survival
Prognostic Factors for Peritoneal Recurrence-Free Survival
DISCUSSION
In the present study, 18F-FDG uptake of AGC was significantly related to risk of distant metastasis after curative surgical resection. AGC patients with distant metastasis had significantly higher 18F-FDG uptake than those with peritoneal recurrence. Furthermore, 18F-FDG uptake of AGC was an independent risk factor for distant metastasis-free survival along with recurrence-free survival and overall survival. Patients with low 18F-FDG uptake had a 5-y distant metastasis-free survival rate of 95.5%, whereas patients with high 18F-FDG uptake had a 5-y distant metastasis-free survival rate of 68.8%.
Several studies have evaluated 18F-FDG PET for prognosis of patients with gastric cancer. Although no significant differences in survival rate are seen according to 18F-FDG uptake of gastric cancer in patients who underwent chemotherapy, 18F-FDG uptake of tumor lesions is a significant prognostic factor for gastric cancer patients who undergo curative surgical resection (13,15,20,21). In our study, enrolled patients had a median clinical follow-up of 51.7 mo, which was considerably longer than previous studies (13,15,20). Our study showed that 18F-FDG uptake of gastric cancer remained an independent prognostic factor for recurrence-free survival and overall survival in AGC patients, along with pT stage, lymph node metastasis, and lymphovascular invasion, which were already known to be significant prognostic factors (5,22–24). Different from these prognostic factors, 18F-FDG PET is advantageous in providing prognostic information even before surgery.
Because 18F-FDG uptake of gastric cancer is related to tumor aggressiveness (9,16), we further investigated whether or not it could play a role in predicting recurrence patterns in addition to predicting recurrence-free survival and overall survival. Although previous studies showed no difference in prognosis between peritoneal recurrence and distant metastasis (8,25,26), the evaluation of risk factors for peritoneal recurrence and distant metastasis could improve selection of treatment and follow-up strategies. Depth of tumor invasion, lymph node metastasis, tumor size, Lauren classification diffuse type, undifferentiated cancer, and Bormann classification type 4 are independent risk factors for peritoneal recurrence (5,7,8,25,27,28). Meanwhile, depth of tumor invasion, lymph node metastasis, venous invasion, and Lauren classification intestinal type were determined to be independent risk factors for distant metastasis (5,8,25,28). Similar to the previous studies, we also found that pT stage, lymph node metastasis, Bormann type 4, and Lauren classification nonintestinal type were independent risk factors for peritoneal recurrence, whereas lymphovascular invasion was an independent risk factor for distant metastasis.
In addition to the above-mentioned pathologic risk factors, 18F-FDG uptake of AGC on PET was significantly related to the risk of recurrence with distant metastasis. On multivariate analysis, 18F-FDG uptake was an independent prognostic factor for distant metastasis after curative surgical resection. Patients with distant metastasis showed significantly higher 18F-FDG uptake of tumor than those without distant metastasis. Given the fact that gastric cancers with aggressive features and intestinal type of pathology show high 18F-FDG uptake (13,16,29,30), it is reasonable that 18F-FDG uptake of gastric cancer can reflect a high risk of distant metastasis in this study. Within 5 y of surgical resection, more than 30% of patients with high 18F-FDG uptake experienced recurrence with distant metastasis, whereas only 4.5% of patients with low 18F-FDG uptake had distant metastasis. When recurrence is suspected during the follow-up of patients with high 18F-FDG uptake in their primary gastric cancer, full consideration should be given to the possibility of distant metastasis and whole-body imaging studies such as 18F-FDG PET are highly recommended to detect distant metastases.
In contrast to distant metastasis-free survival, no significant difference was seen in peritoneal recurrence-free survival between patients with high and low 18F-FDG uptake. Risk factors for peritoneal metastasis such as depth of tumor invasion and lymph node metastasis are related to high 18F-FDG uptake (13,16,29). In contrast, tumors with diffuse type of Lauren classification and Bormann classification type 4 that show low 18F-FDG uptake are also risk factors for peritoneal recurrence (5,7,9,13,21,28,31). Further, the high peritoneal recurrence rate in signet-ring cell carcinoma/mucinous adenocarcinoma, which is known to have low 18F-FDG uptake, could have contributed to the results of this study (9,13,21). Therefore, it is unlikely that peritoneal recurrence-free survival differs by the degrees of 18F-FDG uptake.
The present study has several limitations. First, because the patterns of recurrence were based on clinical examination and imaging studies, exact recurrence sites could be underestimated in some of the patients. Second, patients with early gastric cancer were excluded from the study to avoid the partial-volume averaging effect in 18F-FDG uptake measurements. However, because the recurrence rate of early gastric cancer is only 1.1%–2.2% (32,33), performing 18F-FDG PET/CT to predict prognosis and recurrence patterns in these patients might not be necessary. Finally, because this study was a retrospective single-center study, selection bias can be inevitable and further studies are needed to confirm the results of our study.
CONCLUSION
Patterns of recurrence varied with both clinicohistopathologic characteristics of AGC and 18F-FDG uptake of the tumor on PET. 18F-FDG uptake of AGC is an independent significant prognostic factor for recurrence-free survival and overall survival. Especially, patients with low 18F-FDG uptake have significantly better distant metastasis-free survival than those with high 18F-FDG uptake. Systemic evaluation using 18F-FDG PET is highly recommended for AGC patients with high 18F-FDG uptake in the primary tumor for early detection and accurate restaging of unsuspected distant recurrence.
DISCLOSURE
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734. This research was supported by the Basic Science Research Program through the National Research Foundation of Korea (NRF) grants funded by the Ministry of Science, ICT, and Future Planning (MSIP) (2012R1A1A3008042 and no. NRF-2011-0030086). No other potential conflict of interest relevant to this article was reported.
Footnotes
Published online Aug. 6, 2015.
- © 2015 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication May 8, 2015.
- Accepted for publication July 30, 2015.





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.