


Abstract
Fibroblast activation protein (FAP), a membrane-anchored peptidase, is highly expressed in cancer-associated fibroblasts in more than 90% of epithelial tumors and contributes to progression and worse prognosis of different cancers. Therefore, FAP is considered a promising target for radionuclide-based approaches for diagnosis and treatment of tumors and for the diagnosis of nonmalignant diseases associated with a remodeling of the extracellular matrix. Accordingly, a variety of quinolone-based FAP inhibitors (FAPIs) coupled to chelators were developed displaying specific binding to human and murine FAP with a rapid and almost complete internalization. Because of a high tumor uptake and a very low accumulation in normal tissues, as well as a rapid clearance from the circulation, a high contrast is obtained for FAPI PET/CT imaging even at 10 min after tracer administration. Moreover, FAPI PET/CT provides advantages over 18F-FDG PET/CT in several tumor entities for initial staging and detection of tumor recurrence and metastases, including peritonitis carcinomatosa.
Malignant tumors consist of neoplastic cells but also of a variety of nonmalignant cells that create and shape the tumor microenvironment, also called tumor stroma. These include cells of the basement membrane and capillaries, immune cells, and the heterogeneous population of fibroblastlike cells, termed cancer-associated fibroblasts (CAFs) (Fig. 1). Dysregulated interactions and signaling between tumor cells and cellular components of the tumor microenvironment—representing up to 90% of tumor tissue in frequently occurring carcinomas of the breast, colon, and pancreas (1)—significantly determine the malignant phenotype of cancer cells and contribute to tumor evolution and progression. Notably, through the production of various growth factors, chemokines, and cytokines, noncancerous stromal cells promote extracellular matrix remodeling, induction of angiogenesis, cellular migration, drug resistance, and evasion of immunosurveillance, facilitating invasion and the development of metastasis (2).
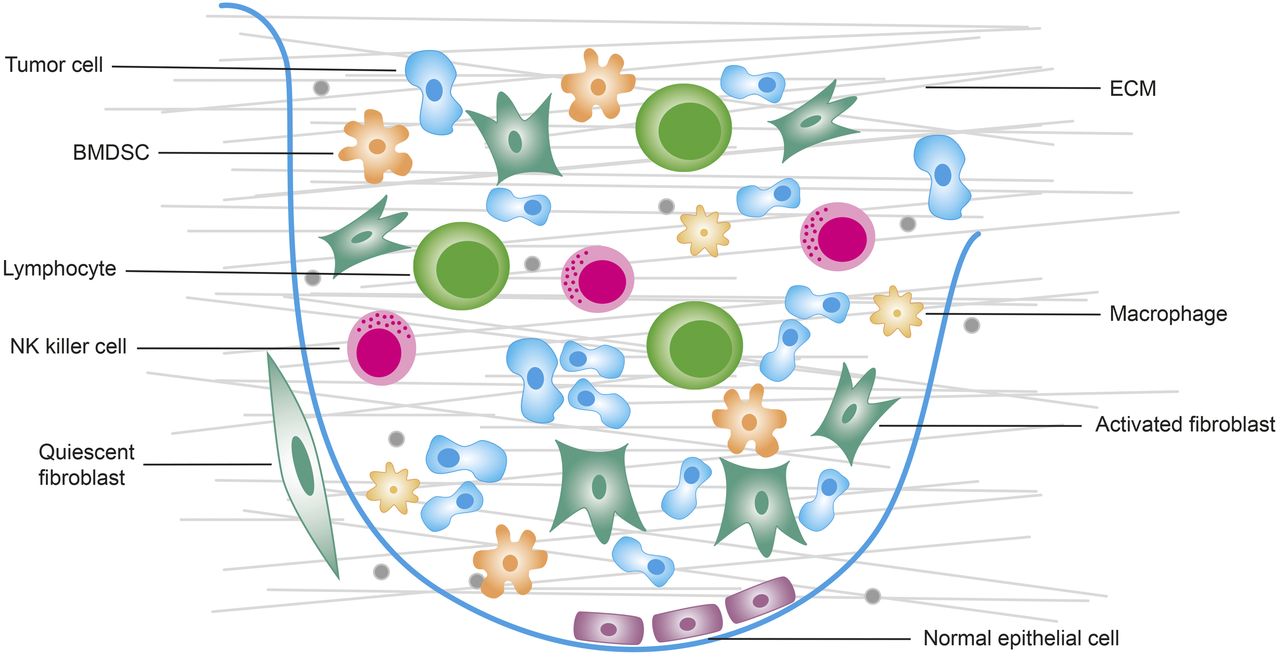
Tumor microenvironment consists of tumor cells and nontumor cells such as bone marrow–derived stem cells (BMDSC), B and T lymphocytes, natural killer (NK) cells, normal epithelial cells, activated fibroblasts (CAFs), and macrophages (T1 and T2). ECM = extracellular matrix. (Modified from (56).)
CAFs
CAFs, which account for most of the tumor stroma, have prominent desmoplastic reactions in colorectal cancer (3) and pancreatic cancer (4) and represent the most prominent modifiers of cancer progression and metastasis. Because of secretion of growth stimulatory, prosurvival, and angiogenic factors, they promote many different aspects of tumor development, including metabolic cooperation, remodeling of the extracellular matrix, induction of epithelial-to-mesenchymal transition, and therapy resistance. Moreover, the interaction of CAFs with cellular components of the immune system mediates immunosuppression and inflammation (5). CAFs are genetically more stable and, therefore, less susceptible to the development of therapy resistance than cancer cells per se.
CAFs originate from local fibroblasts, circulating fibroblasts, vascular endothelial cells via endothelial-to-mesenchymal transition, adipocytes, bone marrow–derived stem cells, or even cancer cells via endothelial-to-mesenchymal transition (5,6). This spectrum of origin at least partially explains the phenotypically different subsets of CAFs that promote heterogeneous properties in individual tumor regions (6).
Irrespective of origin, the development of CAFs in the tumor stroma is accompanied by morphologic and molecular changes leading to spindle-shaped form and the expression of particular surface markers such as the α-smooth muscle actin, the platelet-derived growth factor β, and the fibroblast activation protein (FAP) (6). Whereas many markers are heterogeneously expressed in CAFs in various tumor entities, FAP was shown to be upregulated in the stroma of more than 90% of epithelial carcinomas (7). A recently published metaanalysis involving 15 studies that assessed FAP expression in 11 solid tumors by immunohistochemistry concluded that FAP was detected in 50%–100% of the patients and that FAP expression is associated with increased local tumor invasion, increased risk of lymph node metastasis, and decreased survival (8). The association between FAP expression and poor prognosis was most clearly demonstrated in colorectal cancer and pancreatic cancer but was also shown in patients with hepatocellular cancer (9) and ovarian cancer (10). Therefore, FAP is considered an important target for diagnosis and therapeutic approaches.
FAP
FAP is a type II membrane-bound glycoprotein belonging to the dipeptidyl peptidase 4 family, with dipeptidyl peptidase and endopeptidase activity and sharing a 52% identity at the protein level with dipeptidyl peptidase 4 (11). The protein, which was also given the name seprase, consists of 760 amino acids comprising a short intracellular domain (6 amino acids), a transmembrane domain (20 amino acids), and a large extracellular domain (734 amino acids). Both the postproline dipeptidyl peptidase and the endopeptidase activity of FAP depend on the catalytic triad consisting of serin (S624), aspartate (D702), and histidine (H734) (12) and require homodimerization of the protein (13).
Further to overexpression in CAFs and certain transformed cells of malignant tissues, FAP is also selectively expressed in cells of benign diseases and in normal tissues during remodeling. These include stromal cells and mesenchymal stem cells during embryogenesis, wound healing, fibrotic reactions, and inflammatory conditions such as arthritis, atherosclerotic plaques, and fibrosis (14,15), as well as in ischemic heart tissue after myocardial infarction (16,17). In healthy adult tissues, no or only insignificant levels of the protein are detected in the uterus, cervix, placenta, breast, and skin.
On the basis of enzymatic or nonenzymatic effects, FAP directly enhances proliferation, migration, and invasion of stromal fibroblasts and of additional cell types, including tumor, endothelial, and immune cells, leading to invasiveness, extracellular matrix degradation, tumor vascularization, and escape from immunosurveillance (1,18). Accordingly, in many human malignancies, including colorectal cancer, pancreatic cancer, ovarian cancer, hepatocellular cancer, and non–small-cell lung carcinoma, high FAP expression is reported to correlate with increased local tumor invasion, increased risk of lymph node metastases, and decreased survival of patients (1).
FAP-SPECIFIC TARGETING OF TUMORS
The involvement of FAP in tumor development and progression, as well as the selective expression of the protein in the microenvironment of the most frequent tumors, led to the development of several FAP-based therapeutic approaches. Most of these strategies focused on the development of inhibitors of the enzymatic activity of the protein and, thereby, the contribution to growth and invasiveness of the tumor. The characterization of the dipeptide substrate requirements for FAP enabled the synthesis of a variety of different small molecules inhibiting the specific prolyl peptidase activity of the enzyme. Among these, talabostat, a boronic acid–based inhibitor (Val-proline boronic acid, PT-100), the only FAP inhibitor (FAPI) tested in clinical studies so far, was well tolerated in solid tumor patients but, despite promising preclinical results, failed to induce tumor response in most malignancies in phase II clinical trials (19). A combinatorial treatment of talabostat with either docetaxel in non–small-cell lung carcinoma patients (20) or cisplatin in metastatic malignant melanoma patients (21) also failed to show any clinical benefit and even reduced the survival rate of these patients. Nevertheless, a variety of FAP-specific small molecules has recently been developed, providing the basis for new radiopharmaceuticals (22,23).
Because of the conflicting data regarding the contribution of FAP’s enzymatic activity to tumor progression, several therapeutic strategies have focused on the restricted tumor expression of FAP and the elimination of FAP-expressing cells. The unique proline-specific proteolytic activity of FAP was used to design FAP-activated prodrugs comprising a peptide containing the FAP cleavage site and a cytotoxin that, after systemic administration, circulates throughout the body in an inactive form (24,25). On specific binding to FAP and subsequent proteolytic cleavage of the peptide, the cytotoxin is able to cross the cell membrane and reach its intracellular target in FAP-expressing cells but also nearby FAP-negative cancer cells (bystander effect). Although most of these strategies showed promising results in different xenograft models regarding tumor regression—and toxic side effects were markedly suppressed in comparison with the original drug—clinical application was limited by the toxicity of unprocessed protoxin or partial deposition of the active drug in healthy organs (9).
Clinical studies demonstrated the ability of FAP-specific antibodies to accumulate in tumor tissues after intravenous application. The 131I-labeled FAP-specific murine antibody 19F—originally used to indentify FAP as a tumor-associated antigen—displayed specific accumulation in tumor tissues of colon carcinoma patients. Thereafter, several humanized versions of 19F antibody were prepared and preclinically evaluated for their diagnostic and therapeutic properties in mouse models. Among these, the 131I-labeled anti-FAP antibody sibrotuzumab was applied for the treatment of patients with metastasized FAP-positive carcinomas, including breast cancer, colorectal cancer, and non–small-cell lung carcinoma, and tumor-specific accumulation was observed (26). However, 131I-sibrotuzumab revealed slow elimination from the liver, the spleen, and other normal organs, as was consistent with a slow blood-pool clearance. Although an antitumor activity of nonlabeled FAP antibodies was soon excluded, their excellent tumor stroma–targeting properties were exploited for the design of conjugates with toxins or immunomodulatory cytokines for localized delivery (27). Anti-FAP antibodies and anti-FAP single-chain variable fragments and antibody fragments, respectively, coupled to highly toxic substances significantly improved the antitumor activity of the substance alone and stimulated the antitumor immune response in mouse tumor models (9).
Immune-based therapies targeting FAP also include the application of FAP-derived DNA, protein, and dendritic cell vaccines to elicit CD8+- and CD4+-mediated immune response against FAP-expressing cells (9) and the development of FAP-specific genetically engineered chimeric antigen receptor T cells (28). On the basis of T-cell–mediated release of proinflammatory cytokines and FAP-specific cytotoxicity, both therapeutic strategies led to elimination of FAP-positive cells in vitro and in different mouse cancer models and induced delayed tumor growth and prolonged survival of the respective animals. Moreover, the combination of FAP vaccination and chemotherapy improved the antitumor response in murine CT26 colon carcinoma and D2F2 breast cancer models (29). Nevertheless, the limited therapeutic effect combined with occasionally severe side effects has prevented the clinical transfer of these strategies so far.
SMALL-MOLECULE INHIBITORS FOR IMAGING AND THERAPY
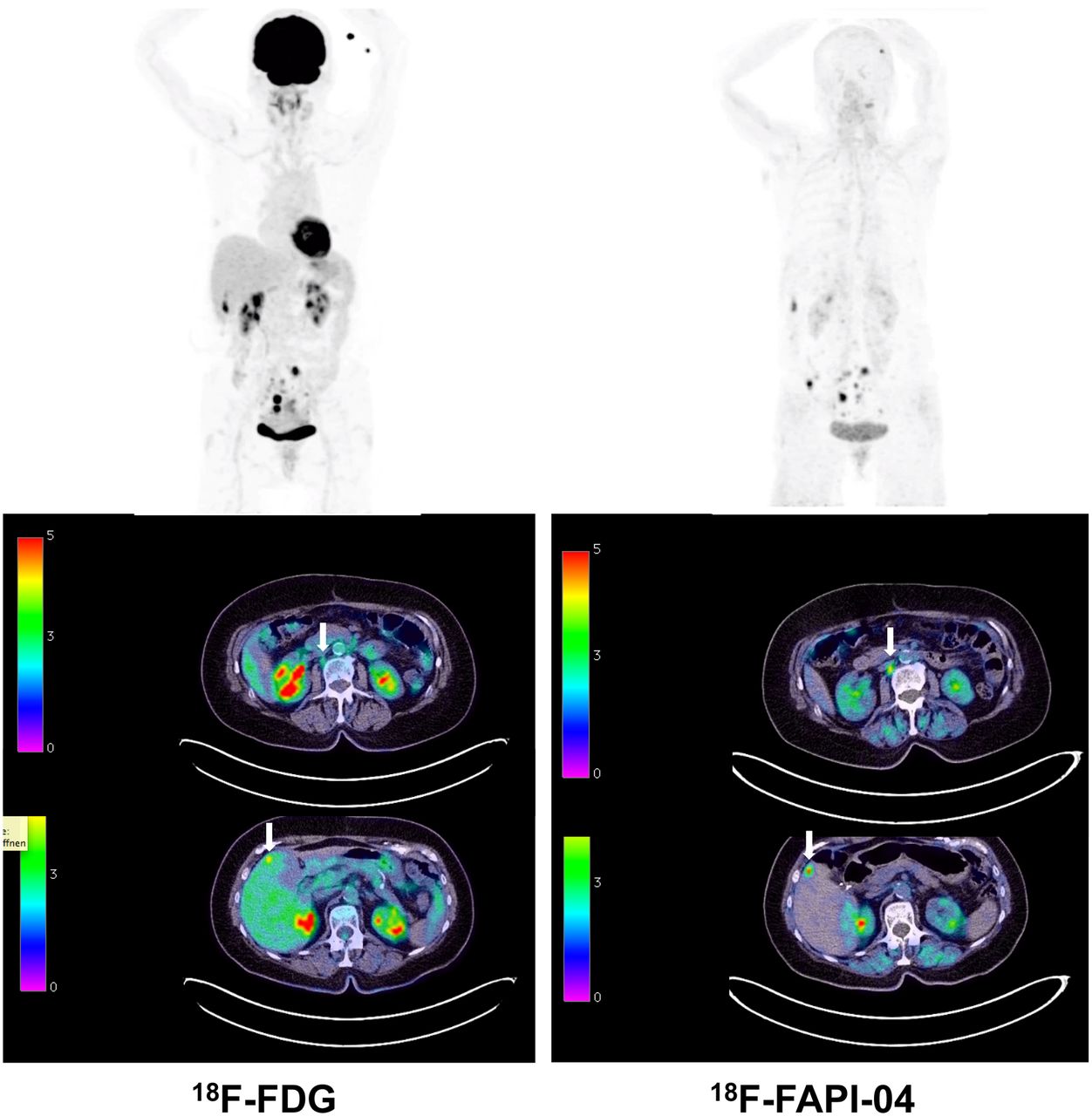
The slow clearance of FAP antibodies leading to a high background signal results in a limited sensitivity for the detection of small lesions. This limited sensitivity can be countered by applying radiolabeled small molecules such as MIP-1232 or other FAPIs (22,23,30). Therefore, a variety of quinoline-based (22) inhibitors were coupled to chelators and showed specific binding to human and murine FAP, with rapid and almost complete internalization (Fig. 2) (31–33). Because of high tumor uptake, a very low accumulation in normal tissues, and rapid clearance from the circulation, a high contrast is obtained for PET imaging even at 10 min after tracer administration (Fig. 3) (34,35). Usually, radioactivity was seen only in the renal pelvis and the bladder, with no accumulation in the renal parenchyma—characteristics that are favorable for a possible therapeutic application. Dose estimates for 68Ga-FAPI-02, 68Ga-FAPI-04, and 68Ga-FAPI-46 ranged from 1.4 to 1.8 mSv/100 MBq (34,36) and, therefore, were comparable to other 68Ga-based tracers such as 68Ga-DOTATOC/DOTATATE or 68Ga-PSMA-11. A first comparison with 18F-FDG in 6 patients with different tumor entities showed that, except for thyroid carcinoma, 68Ga-FAPI PET/CT showed a better contrast and a higher tumor uptake than 18F-FDG. This finding may be especially important in patients with peritonitis carcinomatosa (Fig. 4) (34).

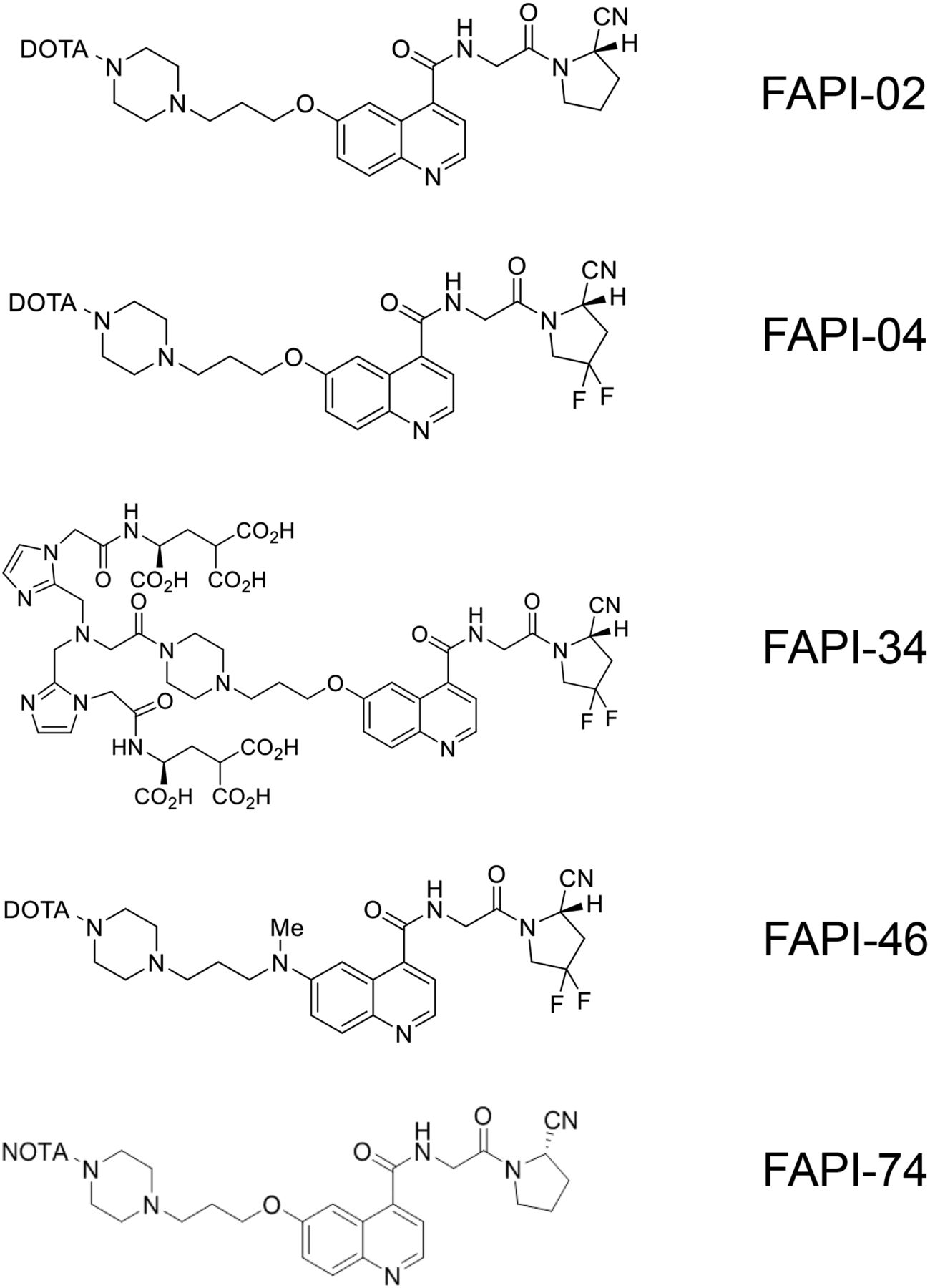
Structures of FAPI tracers used in clinical application.
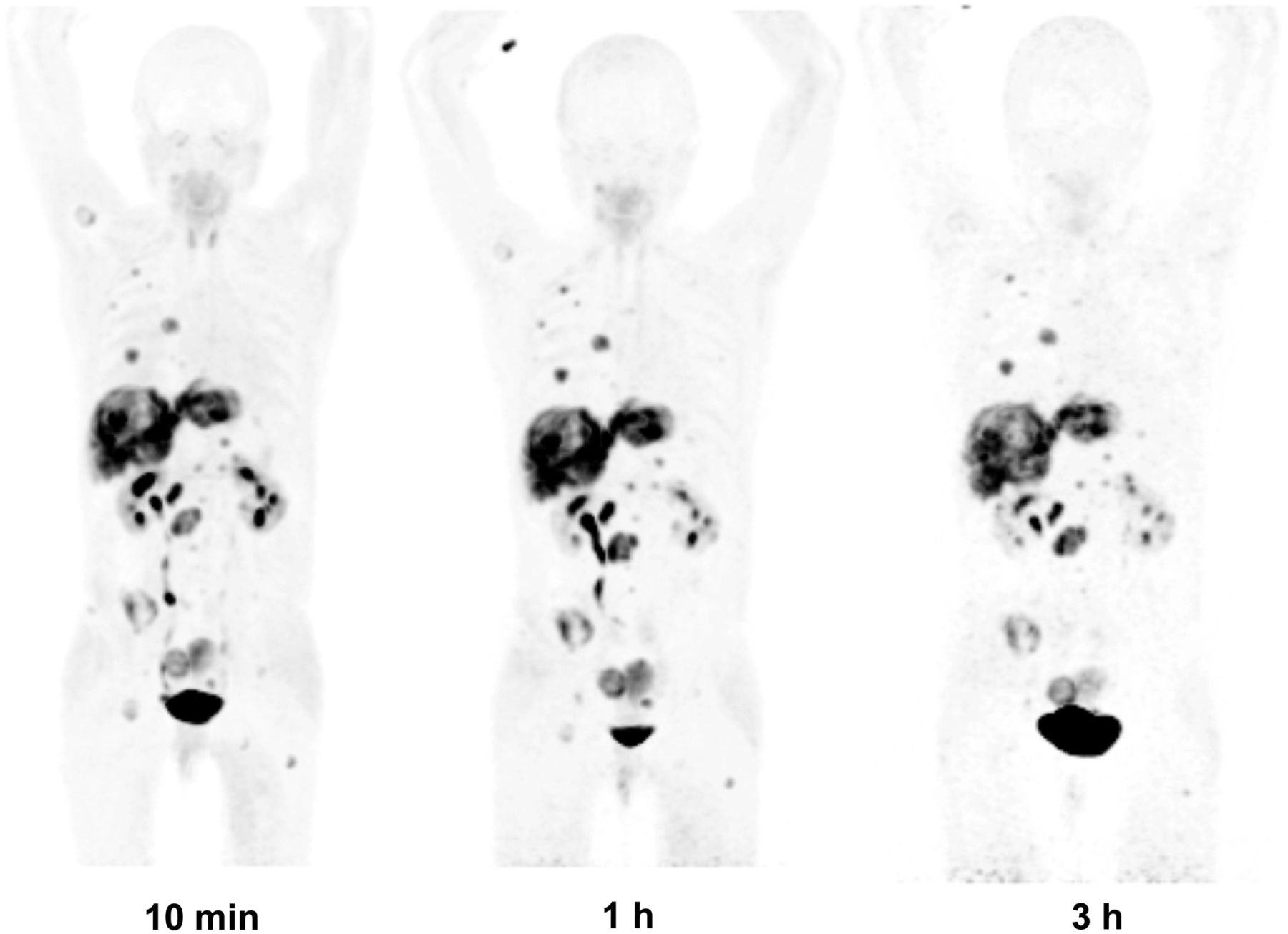
Maximum-intensity projections at 10 min, 1 h, and 3 h after administration of FAPI-46 in patient with metastasized colorectal cancer. Because of rapid tumor uptake and very fast clearance, high-contrast images are possible even at 10 min after injection.

Comparison of 18F-FDG PET/CT and FAPI-46 PET/CT in patient with metastasized ovarian cancer. Shown are maximum-intensity projections and transaxial slices at 1 h after injection. Metastatic lesions in liver and lymph nodes are better seen with FAPI (arrows).
Recently, several new ligands were developed. Moon et al. (37) modified a high-affinity inhibitor with squaric acid containing bifunctional DATA5m and DOTA chelators, which showed high tumor uptake and tissue contrast. Besides, ligands enabling large-scale production for clinical routine application were designed for 18F labeling (38,39). Toms et al. (38) used an 18F-labeled glycosylated FAPI (18F-FGlc‐FAPI). Compared with 68Ga-FAPI‐04 (half-maximal inhibitory concentration, 32 nM), the glycoconjugate, FGlc‐FAPI (half-maximal inhibitory concentration, 167 nM), revealed lower affinity in vitro, higher plasma protein binding, and significant hepatobiliary excretion but higher tumor retention in the U87MG glioma model. Furthermore, 18F-FGlc‐FAPI demonstrated high specific uptake in bones and joints. Giesel et al. (39) reported the use of the NOTA-coupled FAPI-74, which can be labeled with both 18F-AlF and 68Ga, in 10 patients with lung cancer. A high contrast with an SUVmax of more than 10 was seen at 1 h after injection. Dosimetry in these patients revealed effective doses of 1.4 ± 0.2 mSv/100 MBq for 18F-FAPI-74 and 1.6 mSv/100 MBq for 68Ga-FAPI-74—doses that are lower than those obtained with 18F-FDG and other 18F tracers.
Furthermore, new FAPI derivatives were designed for labeling with 99mTc and 188Re, which are available from generators and can be used as a couple for diagnosis and FAP-targeted endoradiotherapy (40). The resulting 99mTc-labeled FAPI tracers showed excellent affinity (half-maximal inhibitory concentration, 6.4–12.7 nM) and binding properties in vitro and significant tumor uptake (≤5.4 percentage injected dose per gram) in biodistribution studies. The lead candidate, 99mTc-FAPI-34, was used for scintigraphy and SPECT in one patient with metastasized ovarian cancer and another patient with pancreatic cancer for follow-up of 90Y-FAPI-46 therapy (40). A comparison to PET/CT imaging with 68Ga-FAPI-46 revealed that 99mTc-FAPI-34 accumulated in the same tumor lesions, with excellent image quality.
In 80 patients who had 28 different tumor entities, with 54 primary tumors and 229 metastases, Kratochwil et al. (35) evaluated 68Ga-FAPI-02 and 68Ga-FAPI-04 uptake and discriminated 3 different groups: the highest average SUVmax (>12) was found in sarcoma, esophageal cancer, breast cancer, cholangiocarcinoma, and lung cancer; an intermediate SUVmax (SUV, 6–12) was seen in hepatocellular, colorectal, head and neck, ovarian, pancreatic, and prostate cancer; and the lowest uptake (average SUVmax < 6) was observed in pheochromocytoma, renal cell cancer, differentiated thyroid cancer, adenoid cystic cancer, and gastric cancer. Nevertheless, high variations in uptake were observed across and within all tumor entities.
In 75 patients with 12 different tumor entities, Chen et al. (41) compared 68Ga-DOTA-FAPI-04 PET/CT with 18F-FDG PET/CT with respect to their performance in initial staging (51 patients) and in detecting tumor recurrence (21 patients). Because of its higher contrast, 68Ga-FAPI-04 PET/CT showed a higher detection rate in all 12 types of malignant tumors than did 18F-FDG PET/CT (98.2% vs. 82.1%, P = 0.021). The sensitivity of 68Ga-FAPI PET/CT was also higher in lymph node metastases (86.4% vs. 45.5%, P = 0.004) and in bone and visceral metastases such as liver metastases, peritoneal carcinomatosis, and brain lesions (83.8% vs. 59.5%, P = 0.004).
The same group evaluated the value of 68Ga-FAPI PET/CT in 68 patients with inconclusive 18F-FDG PET/CT results for the discrimination of mass lesions seen on morphologic imaging (n = 18), for the detection of unknown primary (n = 6), for staging (n = 21), and for suspected recurrence (n = 23). Imaging was followed by histologic analysis as the gold standard. Most tumor lesions had higher uptake for 68Ga-FAPI than for 18F-FDG and higher image contrast, leading to better tumor detection in suspected mass lesions and unknown primaries and better tumor staging and detection of disease recurrence, with an accuracy of 66.7%, 66.7%, 33.3%, and 87.0%, respectively (42).
Furthermore, Shi et al. assessed the value of 68Ga-FAPI-04 PET/CT in 17 patients with suspected hepatic nodules before surgery or biopsy and found high uptake in all tumor nodules, as opposed to only one benign nodule (43).
In patients with brain tumors (5 mutant isocitrate dehydrogenase [IDH] gliomas and 13 wild-type IDH glioblastomas), wild-type IDH glioblastomas and grade III or IV gliomas, but not grade II mutant IDH gliomas, showed elevated tracer uptake. In glioblastomas, spots were found with increased uptake in projection on MRI contrast-enhancing areas. Immunohistochemistry revealed FAP-positive cells with mainly elongated cell bodies and perivascular FAP-positive cells in glioblastomas and an anaplastic mutant IDH astrocytoma. If these data are confirmed in larger patient numbers, it seems possible that 68Ga-FAPI PET/CT may allow noninvasive distinction between low-grade mutant IDH and high-grade gliomas (44).
68Ga-FAPI PET/CT has also been used for radiation therapy planning in patients with glioblastoma, head and neck tumors, and tumors of the lower gastrointestinal tract (45–47). In 13 patients with glioblastoma, the target volume delineation with MRI and 68Ga-FAPI PET/CT showed significant variations resulting in a larger volume when 68Ga-FAPI PET/CT and MRI were used in combination for treatment planning (45).
Since head and neck cancers show a diffuse growth pattern, differentiation between tumor and healthy tissue can be challenging. Therefore, it can be expected that high-contrast images such as those obtained by 68Ga-FAPI PET/CT may improve therapy planning. Syed et al. (46) used 4 different thresholds (3-, 5-, 7- and 10-fold increases in FAPI tumor-to-normal tissue ratio) to calculate 4 different gross tumor volumes, which were compared with gross tumor volumes obtained by contrast-enhanced CT and MRI. The quantitative analysis revealed high uptake in tumors (primary-tumor SUVmax, 14.62 ± 4.44) versus low uptake in healthy tissues such as the salivary glands (SUVmax, 1.76 ± 0.31). Concerning radiation planning, the gross tumor volume obtained with contrast-enhanced CT and MRI was 27.3 cm3, whereas FAPI-derived contours resulted in significantly different gross tumor volumes of 67.7, 22.1, 7.6, and 2.3 cm3 for, respectively, 3-, 5-, 7- and 10-fold increases in FAPI. The combination of the morphologic methods with 68Ga-FAPI PET/CT revealed median volumes that were significantly larger with a 3-fold increase in FAPI (54.7 cm3, 200.5% relative increase, P = 0.0005) and a 5-fold increase (15.0 cm3, 54.9% increase, P = 0.0122).
For tumors of the lower gastrointestinal tract (n = 22), a high tumor-to-background ratio of more than 3 was found in most cases. The TNM classification was changed in 50% of treatment-naïve patients (n = 6), and new lesions were seen in 47% of patients with metastases (n = 15). High, medium, and low changes in therapy were observed in 19%, 33%, and 29% of patients, respectively. Furthermore, in almost all patients, delineation of the target volume improved when the image information from 68Ga-FAPI PET/CT was used (47).
For all 3 tumor entities, future prospective studies are needed to assess the impact of 68Ga-FAPI PET/CT–based radiation therapy on tumor recurrence and survival. If these prospective studies turn out to be positive, the higher contrast between tumor and normal tissues may allow an automatically performed delineation of tumor volume and may thereby improve interphysician variability during therapy planning.
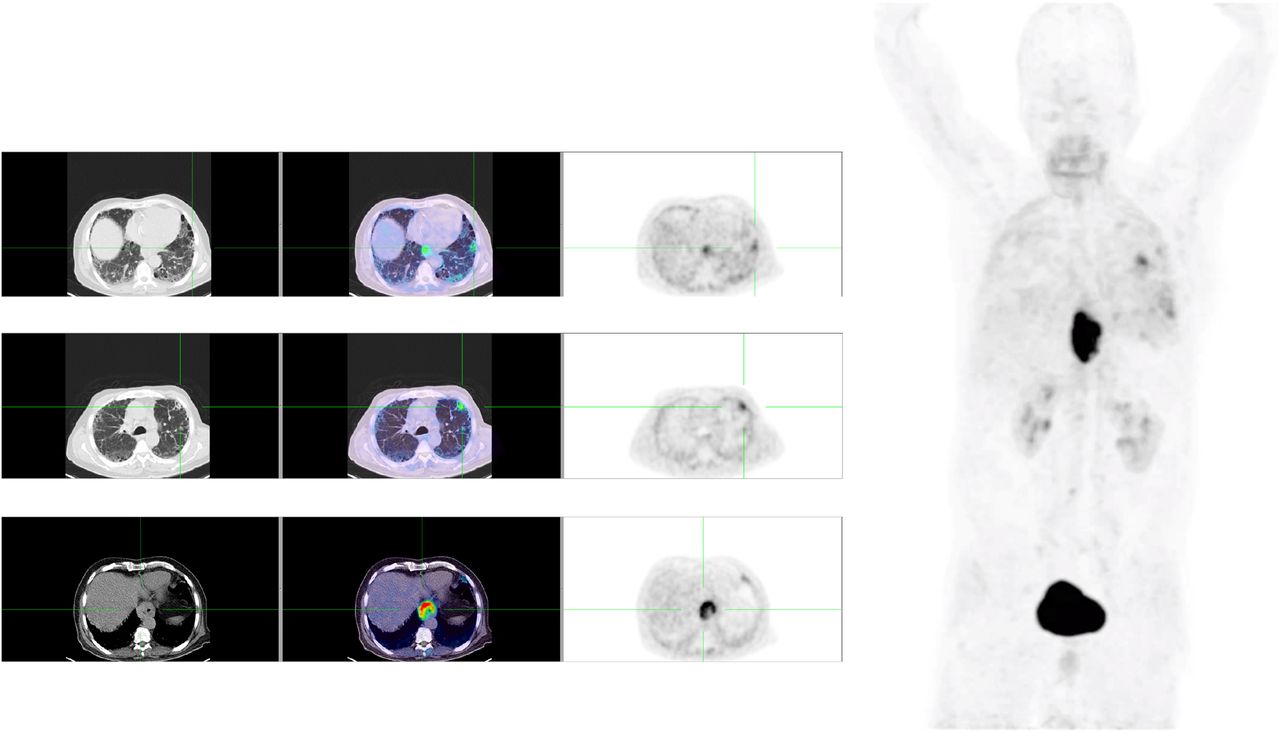
Besides its expression in malignant tumors, FAP expression is upregulated in a variety of benign diseases such as myocardial infarction, fibrosis of several organs, rheumatoid arthritis, and atherosclerotic plaques (14–17); an example of a patient with tumor and fibrosis is shown in Figure 5. For rheumatoid arthritis, murine models imaged with PET and SPECT using radiolabeled anti-FAP antibodies demonstrated high tracer uptake in the inflamed joints and a correlation between tracer accumulation and the severity of the disease (48–50).

FAPI-04 PET/CT of patient with esophageal cancer and lung fibrosis. On left are transaxial slices (CT, fusion image, and PET alone, from left to right); on right is maximum-intensity projection.
In general, autoimmunity-triggered diseases are associated not only with inflammatory reactions but also with fibroblast activation, finally resulting in fibrosis and organ damage. In that respect, IgG4-related disease (IgG4-RD) is characterized by autoimmune inflammation associated with fibrosis predominantly in the pancreas, biliary tree, salivary glands, kidney, aorta, and other organs. Two studies evaluated the performance of 68Ga-FAPI PET/CT as compared with 18F-FDG PET/CT in IgG4-RD (51,52).
Using 68Ga-FAPI PET/CT to examine 26 patients with 136 IgG4-RD–related lesions, Luo et al. (51) additionally detected disease-associated changes in 13% of the organs in 50% of these patients. This led to a higher detection rate of disease manifestation in pancreas, bile duct/liver, and lacrimal glands. In lesions, 68Ga-FAPI uptake was significantly higher than 18F-FDG uptake, a finding that was attributed to the presence of activated fibroblasts. However, in IgG4-related lymphadenopathy, FAPI showed no accumulation, a finding that was explained by a lack of fibrosis.
Using 68Ga-FAPI- and 18F-FDG PET/CT, as well as MRI and histopathologic assessment, Schmidkonz et al. (52) studied 27 patients with inflammatory, fibrotic, and overlapping manifestations of IgG4-related disease. Lesions that were positive on 18F-FDG were found, on histology, to consist of dense infiltrations of IgG4+ cells, whereas FAPI-positive lesions consisted of abundant activated FAP-positive fibroblasts. Therefore, a discrimination between inflammatory and fibrotic activity seems possible. In addition, as compared with inflammatory lesions, fibrotic lesions showed a reduced response to antiinflammatory treatment. The authors see potential for individualization of treatment strategies according to the extent of fibrosis or inflammation. If fibrosis is more extensive than inflammation, specific antifibrotic agents may be preferable to antiinflammatory therapy.
Another area of interest is cardiac disease. In an experimental setup, Varasteh et al. studied remodeling in rats after sham operation and coronary ligation to induce myocardial infarction (53). 68Ga-FAPI uptake in the diseased myocardium peaked at 6 d after coronary ligation, mainly localizing at the border of the infarction as shown by autoradiography and conventional staining. The FAPI-positive area was 18F-FDG–negative but positive for immunofluorescence in myofibroblasts. This finding may have a significant impact on diagnosis and the determination of prognosis, as well as on the clinical management of these patients.
A further possible application is mentioned in a case report of a patient with pancreatic cancer undergoing restaging after therapy with gemcitabine in combination with nab-paclitaxel followed by a modified protocol of folinic acid, fluorouracil, irinotecan, and oxaliplatin (54). Besides 68Ga-FAPI uptake in the primary tumor, in multiple liver metastases, and in peritoneal carcinomatosis, high tracer accumulation was seen in the left ventricular myocardium. The authors speculate that detection of myocardial damage after chemotherapy using 68Ga-FAPI PET/CT may be useful for identification and early management of cardiotoxicity.
Since the FAPI ligands are chelator-based and contain DOTA, these molecules may also be used for therapeutic applications. A first preclinical therapeutic application of 225Ac-FAPI-04 was performed on nude mice bearing human pancreatic PANC-1 cancer cells (55). In this model, high FAP expression was shown by small-animal PET imaging and immunohistochemistry. The therapy—an administration of 34 kBq of 225Ac-FAPI-04—significantly delayed tumor growth, compared with nontreated controls, without significantly changing body weight. Clinically, few data exist for FAPI-04. In a first patient with metastasized final-stage breast cancer, FAPI-04 with 90Y (half-life, 64 h) was chosen to match the physical half-life of the therapeutic radionuclide to the tumor retention time. After a relatively low dose (2.9 GBq) of 90Y-FAPI-04, the metastases could be seen in Bremsstrahlung images even at 24 h after injection (33). Clinically, no therapy-related side effects and, especially, no hematotoxicity were observed, and a significant reduction in opioid dosing for pain was reported.
Because the origin, number, and distribution of FAP-expressing CAFs, as well as the number of FAP molecules per cell, may differ among tumors, we may expect variations in tumor uptake and intratumoral tracer distribution, potentially resulting in different pharmacokinetic profiles in different tumor entities. In a small series of patients with different tumor types, different kinetics from 1 to 3 h after injection was seen (32). If confirmed in a larger number of patients, this observation may have an impact on the indication for FAPI-based endoradiotherapy: tumors with a long retention of the radiopharmaceutical may respond better than tumors that eliminate it quickly. Furthermore, since differences in proteomes can be expected because of differences in the cellular origin of CAFs—with variations existing in the expression of different CAF markers, such as FAP, α-smooth muscle actin, or platelet-derived growth factor β—heterogeneity may be present in tracer uptake or in other FAP-targeting cells or molecules.
CONCLUSION
FAPIs are promising tracers for diagnostic applications in tumors showing a desmoplastic reaction, as well as for nonmalignant diseases associated with tissue remodeling, such as myocardial infarction; sarcoidosis; chronic inflammation; fibrosis of the lung, liver, and kidney; rheumatoid arthritis; and possibly atherosclerosis. For FAPI-based endoradiotherapy, the physical half-life of the radionuclide has to be adjusted to the retention time: radionuclides with shorter half-lives seem preferable to those with longer half-lives. Thus, the use of 188Re, 153Sm, 213Bi, or 212Pb would be favored. Since CAFs are involved in many tumor-supporting processes, such as angiogenesis, chemoresistance, and resistance to immunotherapy, combinations of FAP-targeted endoradiotherapy with radiation therapy, chemotherapy, and immunotherapy may have a synergizing effect and represent an exciting future research area.
DISCLOSURE
There is a patent application (EP 18155420.5) for quinoline-based FAP-targeting agents for imaging and therapy in nuclear medicine (Uwe Haberkorn). Jens Siveke receives research funding from Celgene and BMS; receives personal fees from AstraZeneca, BMS, Celgene, Immunocore, Novartis, and Roche; and holds ownership in FAPI Holding (<3%). Uwe Haberkorn holds ownership in FAPI Holding (<3%). No other potential conflict of interest relevant to this article was reported.
Footnotes
Published online Oct. 30, 2020.
- © 2021 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication September 2, 2020.
- Accepted for publication October 21, 2020.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Macrocyclic phage display for identification of selective protease substrates
- Correlation of FAPI PET Uptake with Immunohistochemistry in Explanted Lungs from Patients with Advanced Interstitial Lung Disease
- 68Ga-Fibroblast Activation Protein Inhibitor PET/CT Improves Detection of Intermediate and Low-Grade Sarcomas and Identifies Candidates for Radiopharmaceutical Therapy
- Immunohistochemical FAP Expression Reflects 68Ga-FAPI PET Imaging Properties of Low- and High-Grade Intraductal Papillary Mucinous Neoplasms and Pancreatic Ductal Adenocarcinoma
- Myocardial Fibrosis: Emerging Target for Cardiac Molecular Imaging and Opportunity for Image-Guided Therapy
- Impact of 68Ga-FAPI PET/CT on Staging and Oncologic Management in a Cohort of 226 Patients with Various Cancers
- Response Prediction Using 18F-FAPI-04 PET/CT in Patients with Esophageal Squamous Cell Carcinoma Treated with Concurrent Chemoradiotherapy
- PET with a 68Ga-Labeled FAPI Dimer: Moving Toward Theranostics
- Detecting Fibroblast Activation Proteins in Lymphoma Using 68Ga-FAPI PET/CT
- The Latest Advances in Imaging Crosstalk Between the Immune System and Fibrosis in Cardiovascular Disease