


Visual Abstract

Abstract
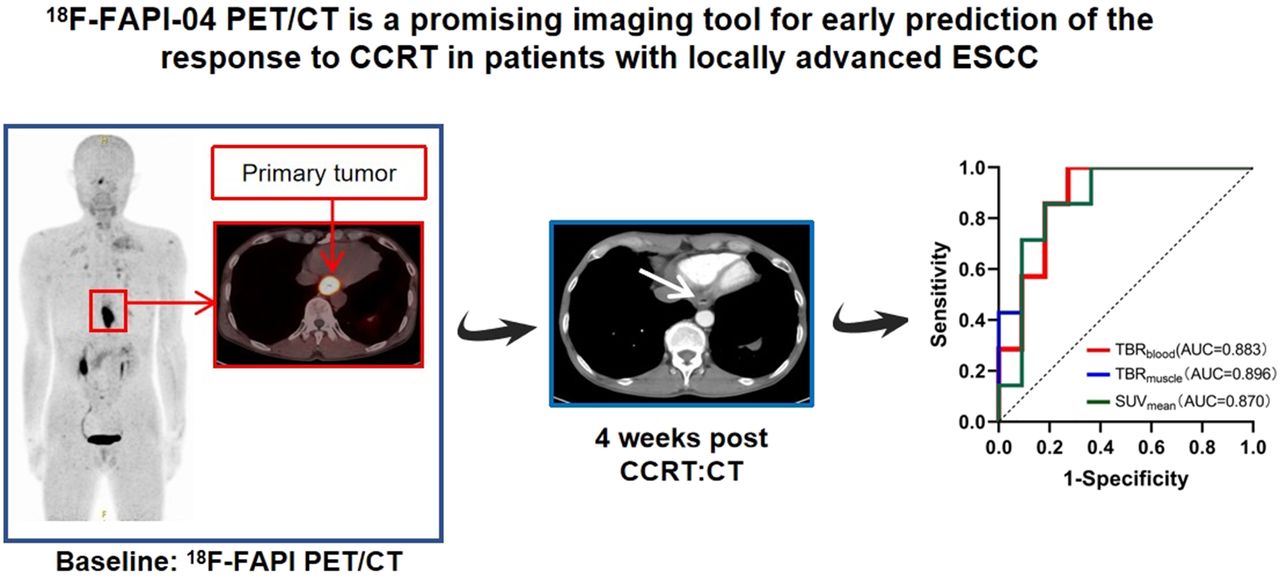
This prospective study examined whether imaging results obtained using the tracer 18F-AlF-NOTA-fibroblast activation protein inhibitor (FAPI)-04 (denoted as 18F-FAPI-04) in PET/CT can predict the short-term outcome in patients with locally advanced esophageal squamous cell carcinoma (LA-ESCC) treated with concurrent chemoradiotherapy (CCRT). Methods: The 18 enrolled LA-ESCC patients underwent 18F-FAPI-04 PET/CT scanning before CCRT. The SUVmax, SUVmean, SUVpeak, metabolic tumor volume, and total lesion fibroblast activation protein expression of the primary tumor were recorded. Additionally, the SUVmax of the primary tumor and SUVmean of normal tissue (muscle and blood) were measured, and their ratios were denoted as target-to-background ratios (TBRmuscle and TBRblood). Patients were classified as responders or nonresponders according to RECIST (version 1.1), and variables were compared between the 2 groups. Results: The TBRblood, TBRmuscle, and SUVmean were significantly higher in nonresponders than in responders (all P < 0.05). Receiver-operating-characteristic curve analysis identified TBRblood (area under the curve [AUC], 0.883; P = 0.008), TBRmuscle (AUC, 0.896; P = 0.006) and SUVmean (AUC, 0.870; P = 0.010) as significant predictors of the response to CCRT, with cutoffs of 10.68, 10.95, and 6.88, respectively. The sensitivity, specificity, positive predictive value, negative predictive value, and accuracy were also determined for TBRblood (100.0%, 72.7%, 66.7%, 88.9%, and 77.8%, respectively), TBRmuscle (100.0%, 72.7%, 66.7%, 88.9%, and 77.8%, respectively), and SUVmean (85.7%, 81.8%, 75.0%, 90.0%, and 83.3%, respectively). On univariate logistic regression analysis, TBRblood (P = 0.026), TBRmuscle (P = 0.036), SUVmean (P = 0.045), and tumor site (P = 0.032) were significantly correlated with the short-term outcome. On multivariable logistic regression analysis, TBRblood (P = 0.046) was an independent prognostic factor for short-term outcome. Conclusion: A higher baseline TBRblood on 18F-FAPI-04 PET/CT scans was associated with a poor response to CCRT in LA-ESCC patients, and thus, TBRblood may be useful for screening LA-ESCC patients before CCRT treatment.
Esophageal cancer is one of the most common malignant tumors of the digestive system in the world, ranking seventh in terms of incidence and sixth in mortality overall in 2020 (1,2). Squamous cell carcinoma is the main histologic type of esophageal cancer in central and southeast Asia (3), and radical concurrent chemoradiotherapy (CCRT) has been recognized by the Radiation Therapy Oncology Group as the first-line treatment for locally advanced esophageal squamous cell carcinoma (LA-ESCC) (4).
Fibroblast activation protein (FAP) is a member of the dipeptidyl peptidase 4 protein family and has both endopeptidase and dipeptidyl peptidase activities. FAP is highly expressed in the stromal fibroblasts of more than 90% of epithelial carcinomas (5–7). Research has shown that high expression of FAP in the stromal fibroblasts of breast cancer, colon cancer, esophageal cancer, and other malignant tumors is related to poor prognosis (8–11). As a means of visualizing FAP expression, a previous study demonstrated that uptake of FAP inhibitor (FAPI) can accurately reflect the biologic distribution of FAP (12). In addition, use of a FAPI-based tracer, 68Ga-DOTA-FAPI-04, in PET/CT was able to clearly identify 12 types of malignant tumors with favorable tumor-to-background contrast (12). We previously performed a pilot clinical study in which 18F-FAPI-04, a novel tracer, was proven to be safe and to offer high specificity for FAP imaging (13). Accordingly, to some extent, parameters on 18F-FAPI-04 PET/CT are expected to predict the outcome of CCRT. However, the efficacy of 68Ga-FAPI/18F-FAPI-04 PET/CT for the prediction of treatment response needed to be verified by prospective studies.
The aim of the present study was to identify imaging parameters that can predict tumor response to CCRT by comparing 18F-FAPI-04 PET/CT parameters between LA-ESCC patients classified as responders and nonresponders. The ability to identify patients with a poor prognosis in advance via imaging will help to realize individualized treatment of tumors.
MATERIALS AND METHODS
Patient Cohort
Potentially eligible LA-ESCC patients were recruited in Shandong Cancer Hospital and Institute from June 2021 to February 2022 (Table 1). All patients volunteered to participate in this prospective study and gave written informed consent. The study was approved by the local ethics committee of Shandong Cancer Hospital and Institute.
Characteristics of Enrolled LA-ESCC Patients (n = 18)
Patients were enrolled according to the following criteria: histopathologically confirmed esophageal squamous cell carcinoma (T3∼4N0∼2M0∼1); an age of at least 18 y; an Eastern Cooperative Oncology Group score of no more than 1; the presence of measurable primary tumors according to RECIST (version 1.1); readiness to undergo CCRT without prior surgery, chemotherapy, or radiotherapy for thoracic tumors; and 18F-FAPI-04 PET/CT scanning performed before CCRT. The exclusion criteria included pregnancy or breastfeeding and unwillingness to participate. A flowchart of the study design is shown in Figure 1.

Research flowchart.
CCRT
Patients were scanned within 1 wk before the start of CCRT. The total radiotherapy dose ranged from 50.4 to 60 Gy, and intensity-modulated radiotherapy was delivered to all patients with megavoltage equipment (6 MV). Radiotherapy was given as the conventionally fractionated regimen, 1.8–2.0 Gy for 5 d per week. The specific chemotherapy regimens that followed are listed in Supplemental Table 1 (supplemental materials are available at http://jnm.snmjournals.org).
18F-FAPI-04 PET/CT Scanning
18F-FAPI-04 was synthesized as described previously (14). Patients were not required to fast or undergo blood glucose measurement before scanning. After receiving an intravenous injection of 18F-FAPI-04 (4.81 MBq/kg), the patients rested for approximately 1 h. Scanning was then performed with an integrated in-line PET/CT system (Gemini TF Big Bore; Philips Healthcare). Whole-body CT scans were obtained using a low-dose protocol (300 mAs, 120 kV, 512 × 512 matrix, rotation time of 1.0 s, and pitch index of 0.688; reconstructed with a soft-tissue kernel to a slice thickness of 2 mm) for attenuation correction. PET data were acquired in 3-dimensional mode using a 200 × 200 matrix with an imaging time of 1 min per bed position. During image acquisition, the patients maintained normal shallow breathing. Subsequently, after attenuation correction (Body-ctac-SB. Lstcln, Biograph 3-dimensional iterative reconstruction software, time-of-flight correction), we reviewed the PET, CT, and PET/CT images.
Imaging Analysis
The attenuation-corrected PET images, CT images, and PET/CT images, displayed as coronal, sagittal, and transaxial slices, were viewed and analyzed on a Nuclear Medicine Information System (Beijing Mozi Healthcare Ltd.). Two experienced nuclear medicine physicians visually assessed the 18F-FAPI-04 PET/CT images and reached consensus on interpretations for primary and metastatic tumors. Regions of interest were drawn around tumor lesions with higher uptake in transaxial sections, and 18F-FAPI-04 PET/CT parameters were generated by an automated 3-dimensional contouring program with a 30% isocontour. The uptake values within regions of interest were normalized to the injected dose per kilogram of patient body weight to derive the SUVs, according to the following formula: [measured activity concentration (Bq/mL) × body weight (g)]/injected activity (Bq). Regions of interest were drawn around the primary tumor lesion, and the obtained parameters, including SUVmax, SUVmean, SUVpeak, metabolic tumor volume (MTV), and total lesion FAP expression, were generated by an automated contouring program provided by the vendor. We also measured the SUVmean of 1-cm3 areas in the pulmonary aortic trunk and erector spinae. Then, the ratio of the SUVmax of the primary tumor to the SUVmean of normal tissue (blood and muscle) was calculated, denoted as tumor-to-background ratio (TBRblood and TBRmuscle). For controversial lesions, discussion among the imaging experts with consideration of the results from other imaging modalities proceeded until a final consensus was reached.
Response Evaluation and Survival Assessments
Two imaging specialists independently reviewed the contrast-enhanced CT images obtained at baseline and at 4 wk of follow-up. The specialists knew that all patients had pathologically confirmed cancer but not the clinical, laboratory, or follow-up results. The reviewers recorded the primary tumor location and size in the axial plane. Short-term outcome was assessed at 4 wk after CCRT according to the revised RECIST using thoracic CT. According to RECIST, patients with an outcome of complete response or partial response were classified as responders, and patients with an outcome of stable disease or progressive disease were classified as nonresponders.
Statistical Analysis
Statistical analysis was performed using SPSS Statistics (version 25.0; IBM) for Microsoft Windows. Quantitative data for SUVmax, SUVmean, SUVpeak, MTV, total lesion FAP expression, TBRblood, and TBRmuscle were expressed as mean ± SD. Mann–Whitney U tests were used to compare the 18F-FAPI-04 PET/CT parameters between responders and nonresponders. Logistic regression analyses were performed to identify the relationships between tumor site, degree of differentiation, and 18F-FAPI-04 PET/CT parameters and short-term outcomes. Receiver-operating-characteristic curve analysis was used to determine the thresholds with the maximum Youden index as well as the predictive accuracy of 18F-FAPI-04 PET/CT parameters for treatment response. Spearman rank correlation coefficients were calculated to assess the relationships between biomarkers. All tests were 2-sided, and a P value of less than 0.05 was considered statistically significant.
RESULTS
Characteristics and Outcomes of Enrolled Patients
From June 2021 to March 2022, 18 patients diagnosed with LA-ESCC on the basis of histologic examinations at Shandong Cancer Hospital and Institute were enrolled in this study. The characteristics of the patients are presented in Table 1. Among all patients, 11 were classified as responders and 7 as nonresponders (Table 1). Figure 2 shows representative 18F-FAPI-04 PET/CT imaging results for a responder and a nonresponder.

18F-FAPI-04 PET/CT and CT images of LA-ESCC patients with outcome classified as partial response (A) and stable disease (B).
Quantitative 18F-FAPI-04 PET/CT Parameters
The quantitative baseline 18F-FAPI-04 PET/CT parameters SUVmax, SUVmean, SUVpeak, MTV, total lesion FAP expression, TBRblood, and TBRmuscle are shown in Table 2 for all patients, responders, and nonresponders. TBRblood, TBRmuscle, and SUVmean were significantly higher in nonresponders than in responders (12.53 ± 1.11 vs. 10.29 ± 1.54, P = 0.008; 12.24 ± 1.08 vs. 9.81 ± 1.62, P = 0.006; and 14.30 ± 8.83 vs. 6.30 ± 4.25, P = 0.010, respectively) (Table 2). None of the other parameters showed a significant difference between responders and nonresponders.
Parameters Calculated from Pretreatment 18F-FAPI-04 PET/CT Scans
Correlations Between 18F-FAPI-04 PET/CT Parameters and Short-Term Outcome
Receiver-operating-characteristic curves were generated to evaluate the predictive accuracy of 18F-FAPI-04 PET/CT parameters for identifying responders and nonresponders (Table 3; Fig. 3). The area under the curve (AUC) for TBRblood (AUC, 0.883) was higher than those for TBRmuscle (AUC, 0.896) and SUVmean (AUC, 0.870) (Table 4), and the AUCs for all 3 parameters were significant (P = 0.008, P = 0.006, and P = 0.010, respectively) (Table 3). The cutoffs for TBRblood, TBRmuscle, and SUVmean, based on the Youden indices, were 10.68, 10.96, and 6.88, respectively (Table 4). The calculated values for the sensitivity, specificity, positive predictive value, negative predictive value, and accuracy of these 3 parameters also are presented in Table 4.
Areas Under Curve for Ability of SUVmax, SUVmean, SUVpeak, MTV, TLF, TBRblood, and TBRmuscle to Predict LA-ESCC Tumor Response to CCRT

Receiver-operating-characteristic curves for ability of 18F-FAPI-04 PET/CT parameters to predict short-term response to CCRT.
Specificity, Sensitivity, PPV, NPV, and Accuracy of SUVmax, SUVmean, SUVpeak, MTV, TLF, TBRblood, and TBRmuscle for Predicting LA-ESCC Tumor Response to CCRT
Correlations Between Biomarkers
The observed correlations between 18F-FAPI-04 PET/CT biomarkers, extracted from tumor lesions and variables of interest, are presented in Figure 4. TBRblood, TBRmuscle, and SUVmean showed significant correlations with each other. However, none of the 18F-FAPI-04 parameters correlated with any clinical variables.

Correlations between 18F-FAPI-04 PET/CT parameters and clinical or biologic variables (Spearman coefficient). Those with P < 0.05 are marked by circles. Blue represents positive correlation between 2 variables, and red represents negative correlation. The stronger the correlation, the darker the color. Those with P > 0.05, indicating no correlation, are recorded as X. As example, SUVmax showed positive correlation with MTV. ECOG = Eastern Cooperative Oncology Group; TLF = total lesion FAP expression (18F-FAPI-04).
Associations Between Baseline 18F-FAPI-04 PET/CT Parameters, Clinical Variables, and Short-Term Treatment Response
According to univariate logistic regression analyses, TBRblood (P = 0.026), TBRmuscle (P = 0.036), SUVmean (P = 0.045), and tumor site (P = 0.032) were independently associated with the short-term treatment response in LA-ESCC patients. Because of the significantly positive correlation among TBRblood, TBRmuscle, and SUVmean, we included only TBRblood and tumor site in the multivariate analysis. Finally, only TBRblood (P = 0.046) remained significant as a prognostic factor for short-term outcome in these patients (Table 5).
Univariate and Multivariate Logistic Regression Analyses of 18F-FAPI-04 PET/CT Parameters and Clinical Factors Able to Predict Short-Term Outcomes in LA-ESCC Patients
DISCUSSION
The results of the present study indicate that certain parameters derived from baseline 18F-FAPI-04 PET/CT scans, specifically the baseline TBRblood, TBRmuscle, and SUVmean, as well as the tumor site, are potentially valuable for predicting the response to CCRT in patients with LA-ESCC. Moreover, TBRblood was an independent predictor of short-term CCRT efficacy in these patients by multivariable logistic regression analysis.
In clinical practice, we observed different outcomes in patients with LA-ESCC treated with CCRT—differences that may be related to the heterogeneity of the tumor microenvironment (15,16). Previous studies reported that FAP is expressed mainly by interstitial cells of the tumor microenvironment, including cancer-associated fibroblasts and tumor-associated macrophages (17,18). It has been confirmed that FAP plays a key role in chemotherapy resistance (19–21), radiotherapy resistance (22), and immune escape (23–25). Furthermore, FAP can promote tumor cell invasion, migration, and tumor angiogenesis (26–28). In a previous report of 2 cases, 1 patient with peritoneal carcinomatosis who experienced disease progression after 4 mo of chemotherapy showed an increase in the average SUVmax compared with before chemotherapy, whereas the other patient, who achieved partial remission after 5 mo of treatment, showed a decrease in the average SUVmax relative to baseline (29). Accordingly, 18F-FAPI-04 uptake within the tumor was considered potentially valuable for predicting the short-term response to CCRT in patients with LA-ESCC.
A series of studies found that in esophageal cancer patients treated with chemoradiotherapy, the metabolic parameters on pretreatment 18F-FDG PET are reliable predictors of prognosis and survival (30–32). However, at present, the value of 18F-FDG PET/CT parameters for predicting tumor prognosis remains controversial. Caresia Aroztegui et al. found that the evidence for the prognostic value of SUVmax in axillary lymph nodes derived from 18F-FDG PET/CT is limited, although higher values have been associated with higher recurrence rates (33). Research also has demonstrated that the application of 18F-FDG PET parameters in breast cancer prognosis is still limited, and the criteria for these parameters have not been established (34). Thus, the urgent need to find a new imaging agent with higher diagnostic and predictive efficiency persists.
Several studies have demonstrated that high tumor MTV and total lesion glycolysis, derived from 18F-FDG PET/CT scans, are independent predictors in patients with esophageal cancer treated with chemoradiotherapy (32) and definitive chemoradiotherapy (31). However, in our cohort, the baseline tumor MTV and total lesion FAP expression from 18F-FAPI-04 PET/CT did not provide significant prognostic information. We consider that this difference between the results for 18F-FAPI-04 PET/CT and 18F-FDG PET/CT may be related to the imaging principle of 18F-FDG PET/CT, which is based on the level of glucose metabolism within tumor cells.
The main limitations of the present study included its single-center design and relatively small sample size. Further large-scale, multicenter clinical studies are needed to confirm our findings before clinical application. Additionally, the fact that this study included a heterogeneous population consisting of patients treated with total radiation doses of 50 and 60 Gy might affect the outcome. However, Xu et al. reported no significant difference in survival endpoints between groups that received 60 and 50 Gy (35), and Minsky et al. reported that higher radiotherapy doses do not lead to better outcomes (36). Additionally, the ARTDECO study found that increasing the radiation dose from 50.4 to 60 Gy did not improve local control in esophageal cancer (37). Overall, further prospective trials are required to confirm the role of 18F-FAPI-04 PET/CT in the treatment of patients with LA-ESCC.
CONCLUSION
The baseline TBRblood on 18F-FAPI-04 PET/CT was associated with the short-term response to CCRT in patients with LA-ESCC. Combined with clinical prognostic factors, including tumor site, pretreatment 18F-FAPI-04 PET/CT can potentially improve the selection of candidates for CCRT and identify patient groups with markedly different prognoses.
DISCLOSURE
This work was funded by the Natural Science Foundation of China (NSFC81872475, NSFC82073345), the Jinan Clinical Medicine Science and Technology Innovation Plan (202019060), the Natural Science Foundation of Shandong Province (ZR2021QH008), and the Bethune Charitable Foundation (flzh202116). No other potential conflict of interest relevant to this article was reported.
KEY POINTS
QUESTION: Can 18F-FAPI-04 PET/CT parameters predict the short-term response to CCRT in patients with LA-ESCC?
PERTINENT FINDINGS: Baseline TBRblood on 18F-FAPI-04 PET/CT was associated with short-term outcome in patients with LA-ESCC treated with CCRT.
IMPLICATIONS FOR PATIENT CARE: On the basis of the encouraging results of this analysis, 18F-FAPI-04 PET/CT may offer a standardized and reproducible technique for identifying LA-ESCC patients most likely to respond to CCRT.
Footnotes
Published online Oct. 13, 2022.
- © 2023 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication July 8, 2022.
- Revision received October 4, 2022.
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- [18F]AlF-NOTA-FAPI-04 PET/CT for Predicting Pathologic Response of Resectable Esophageal Squamous Cell Carcinoma to Neoadjuvant Camrelizumab and Chemotherapy: A Phase II Clinical Trial
- Fibroblast Activation Protein Inhibitor Tracers and Their Preclinical, Translational, and Clinical Status in China
- Value of 68Ga-FAPI-04 and 18F-FDG PET/CT in Early Prediction of Pathologic Response to Neoadjuvant Chemotherapy in Locally Advanced Gastric Cancer