


REPLY: We thank Dr. Nabavizadeh and colleagues for bringing up postoperative ischemia as a possible cause for the flare phenomenon in O-(2-[18F]-fluoroethyl)-L-tyrosine PET after resection of gliomas (1). Indeed, it cannot be excluded that postoperative ischemia has contributed to the observed flare phenomenon. On the other hand, we would like to emphasize that increased amino acid uptake in subacute ischemia is generally mild and in the range of a tumor-to-brain ratio of 2 or less. In contrast, some patients with flare phenomenon in our study (2) had maximum tumor-to-brain ratios of O-(2-[18F]-fluoroethyl)-L-tyrosine (18F-FET) uptake of up to 5 or above, which has not been reported in acute and subacute ischemia. According to the authors’ suggestion to exclude ischemia in areas with flare phenomenon, we identified 1 patient in our database with a flare phenomenon in postoperative 18F-FET PET who simultaneously underwent MR diffusion-weighted imaging (DWI) (patient 36, Fig. 1). However, the typical signs of ischemia, that is, a high signal intensity on DWI associated with low signal intensity on apparent diffusion coefficient maps, could not be identified in the corresponding area showing the flare phenomenon in postoperative 18F-FET PET. Thus, DWI in this patient with a flare phenomenon does not support the “ischemia hypothesis.” Nevertheless, this important aspect should be considered and further investigated in future studies.
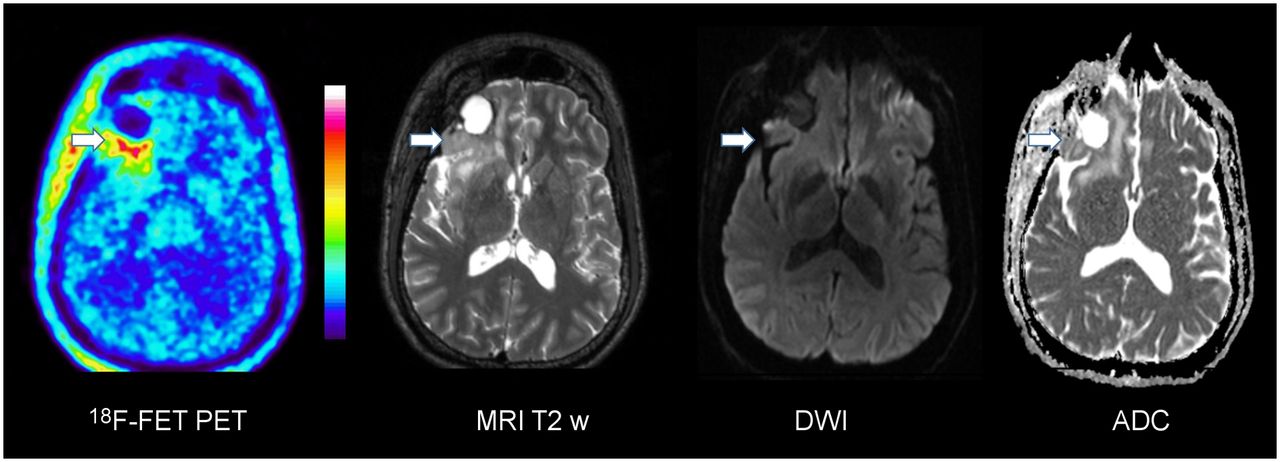
Brain scans of patient 20 d after resection of recurrent, right frontal oligodendroglioma World Health Organization II. 18F-FET PET shows increased uptake at posterior border of resection cavity (white arrow) but no signs of ischemia, that is, a high signal intensity on diffusion-weighted imaging associated with low signal intensity on the apparent diffusion coefficient map.
Footnotes
Published online Aug. 28, 2020.
- © 2020 by the Society of Nuclear Medicine and Molecular Imaging.





{kind=link}