


Abstract
Synthetic somatostatin analogs have been posed as a potential source of error in somatostatin receptor imaging through interference with tumor detection; however, experimental models and clinical studies have shown a complex mechanism of the effect of octreotide on tumors. The aim of this study was to assess whether 68Ga-DOTATATE uptake before treatment with long-acting somatostatin analogs differs from that after treatment. Methods: Thirty patients (15 men; age [mean ± SD], 64.6 ± 13.4 y) who had intermediately differentiated to well-differentiated neuroendocrine tumors and who underwent 68Ga-DOTATATE PET/CT scanning before and after receiving long-acting repeatable octreotide (Sandostatin LAR) were included in the study. The SUVmax and SUVmean of healthy target organs, residual primary tumor, and up to 5 lesions with the highest SUVmax in each organ were compared before and after octreotide treatment. Results: The mean time interval between the 2 68Ga-DOTATATE studies was 9.6 ± 7.2 mo, and the mean time gap between the last Sandostatin LAR injection and the second 68Ga-DOTATATE study was 25.1 ± 14.8 d. The pretreatment mean SUVmax and SUVmean were both significantly higher in the thyroid, liver, and spleen (P < 0.05) than the values measured after the administration of Sandostatin LAR. No significant differences were found among the uptake indices for residual primary tumor or any metastatic lesions in the liver, bone, lung, or lymph nodes before and after Sandostatin LAR administration (P > 0.05). Conclusion: Long-acting octreotide treatment diminished 68Ga-DOTATATE uptake in the liver, spleen, and thyroid but did not compromise tracer uptake in residual primary tumor and metastatic lesions. These findings have a direct impact on the interpretation of 68Ga-DOTATATE PET/CT scans.
PET/CT with 68Ga-DOTATATE plays a pivotal role in neuroendocrine tumor (NET) management (1), providing incremental data compared with 111In-pentetreotide (Octreoscan; Mallinckrodt) and conventional imaging (2) and better sensitivity and specificity than 18F-FDG PET imaging for neuroendocrine neoplasms (3,4).The clinical indications include primary tumor localization (5), metastatic disease detection, and response monitoring (6). In addition, somatostatin receptor (SSTR) imaging has established value in the prediction of response to treatment (7).
Synthetic somatostatin analogs have been shown to have clinical utility in patients with functionally active NETs by prolonging the time to progression (8,9) and controlling symptoms (10). However, somatostatin analogs may confound the interpretation of SSTR imaging data because they interfere with tumor detection (11) by saturating SSTRs in tumors (12). Experimental models and some human studies have shown the upregulation of SSTR expression in tumor cells and alterations in the internalization of subtype 2 SSTRs after the introduction of somatostatin analog treatment (12–15). These observations may result partly from the complex mechanism of the effect of octreotide on tumoral lesions, which may be different from the mechanism of the effect of the compound on normal target tissues (16). Clinical studies in this regard have been limited with respect to the number of patients evaluated and have mainly assessed the impact of octreotide treatment on Octreoscan imaging (17,18). Only 1 study has investigated the effect of octreotide on PET tracer SSTR imaging (19).
The aim of this study was to assess whether 68Ga-DOTATATE uptake in target organs, residual primary NETs, and metastases before treatment with long-acting somatostatin analogs differs from that after treatment.
MATERIALS AND METHODS
All patients who had intermediately differentiated to well-differentiated NETs, who underwent 68Ga-DOTATATE PET/CT scans before and after receiving somatostatin analog treatment, and who were referred to Austin Hospital (Heidelberg, Victoria, Australia) for restaging from December 2013 to July 2016 were included in the study. Thirty patients (15 women and 15 men; age [mean ± SD], 64.6 ± 13.4 y; age range, 32–86 y) were studied. The study was approved by the Austin Health Human Research Ethics Committee, and all subjects signed a written informed consent form.
Demographic data were collected, and all disease-related information—including tumor type, grade, and primary site; any treatment received between the 2 scans; exact somatostatin analog dosing; the time interval from the last treatment to the second study; and the interval between the 2 studies—was recorded. If the patient had more than 1 scan before and more than 1 scan after octreotide administration, the last scan before and the first scan (not the final scan) after treatment were chosen for analysis. This selection minimized the time interval between 2 compared scans. All patients received long-acting repeatable octreotide (Sandostatin LAR; Novartis) at a dose of 30 mg every 4 wk, except for 1 patient, who received a 60-mg dose on the same time line.
68Ga-DOTATATE was synthesized using established techniques (7). 68Ga was eluted from a 68Ge/68Ga generator (ITG), and high-performance liquid chromatography and radio–thin-layer chromatography were used to assess the purity and verify the identity of the final product. The radiochemical purity of the final product was greater than 90%.
Sixty minutes after the injection of 110–185 MBq of 68Ga-DOTATATE, whole-body scans were obtained from the skull vertex to the upper thighs on a Gemini Time-of-Flight PET/CT scanner (Philips). After the transmission scans, 3-dimensional PET acquisition was performed for 2–3 min per bed position. Low-dose CT was performed, and the data were used for attenuation correction and lesion localization. An iterative reconstruction algorithm was applied for image reconstruction.
Images were analyzed using a dedicated software package (version 6.4.5; MIM Software Inc.). The SUVmean and SUVmax of healthy target organs, including the liver, spleen, adrenal glands, thyroid, and pituitary gland, were analyzed in both scans for each patient. If there was evidence of metastasis in an organ, then it was excluded from the analysis, except for the liver. In livers with up to 3 focal sites of metastasis, a region of interest was drawn distal to the lesions at the same location in both 68Ga-DOTATATE studies, and the indices were considered to represent the values of the healthy target organ. SUVmean and SUVmax were also calculated in the primary site of the tumor (if remaining) and in up to 5 lesions that had the highest SUV in each organ and were present in both scans (Fig. 1). To prevent partial-volume effects, we excluded subcentimeter lesions from the analysis.
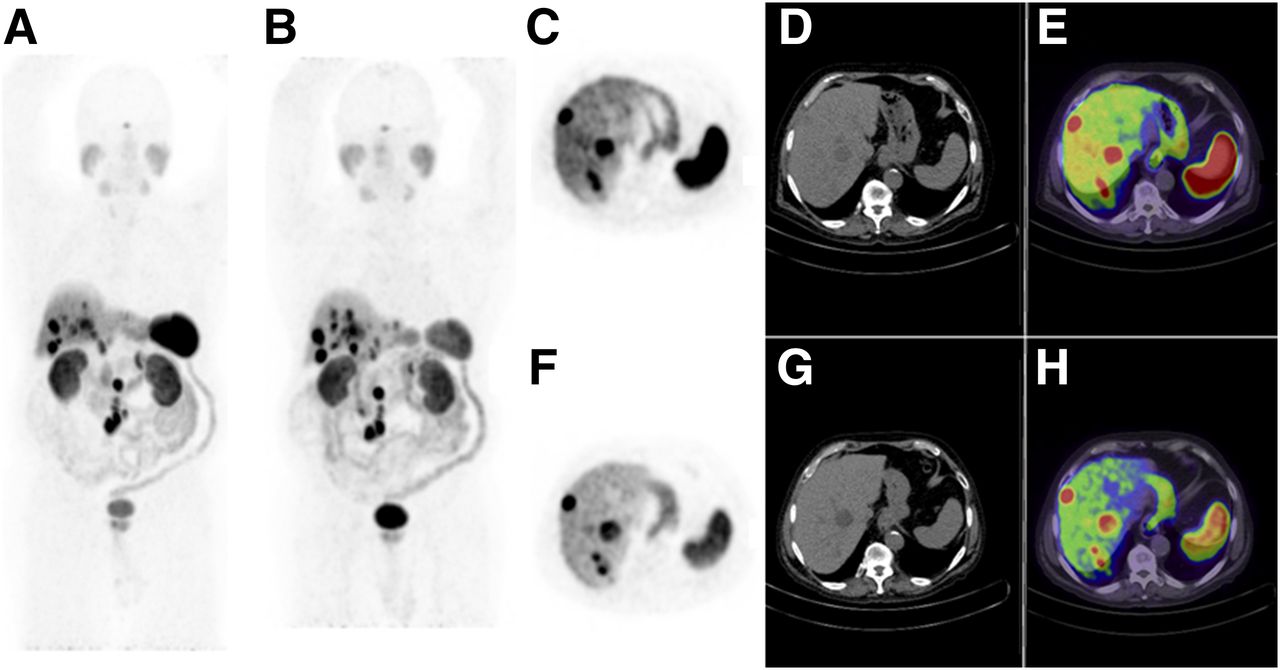
68Ga-DOTATATE PET whole-body maximum-intensity projection images in patient with small-bowel carcinoid tumor before (A) and after (B) 12 mo of treatment with Sandostatin LAR (30 mg/4 wk). The post treatment scan showed reduced uptake of 68Ga-DOTATATE in normal liver, spleen, and thyroid, also seen in transaxial PET, CT, and fused images before (C–E) and after (F–H) treatment. Both primary and metastatic lesions showed similar uptake of 68Ga-DOTATATE, with the SUVmean of the hottest lesion 30.6 in the first study and 31.8 in the second study.
SPSS software (version 16.0; SPSS Inc.) was used for data analysis. Descriptive statistics were used to describe the data. Quantitative variables were compared between 2 groups using paired-sample t tests, and qualitative variables were assessed using the McNemar test. A P value of less than 0.05 was considered significant in all comparisons.
RESULTS
Primary tumor sites are shown in Table 1. Tumor grade and Ki-67 were formally reported in 18 and 14 patients, respectively (Table 1).
Characteristics of Primary Tumor, Metastatic Lesions, and Treatment
The mean time interval between the 2 studies was 9.6 ± 7.2 mo (range, 3–32 mo), and the mean time gap between the last Sandostatin LAR injection and the second study was 25.1 ± 14.8 d (range, 1–59 d). Our analysis of 68Ga-DOTATATE studies in individual patients revealed stable disease in 73.3% (22/30), disease progression in 20.0% (6/30), and a partial response in 6.7% (2/30).
The mean SUVmax and SUVmean in normal organs were compared before and after Sandostatin LAR administration; the results are shown in Table 2. After Sandostatin LAR treatment, the mean SUVmax significantly decreased in the thyroid, liver, and spleen (P < 0.05), whereas no significant differences were noted in the pituitary and adrenal glands (P was not significant). Figure 1 shows 68Ga-DOTATATE PET/CT images from a representative patient before and after Sandostatin LAR treatment.
Comparison of SUVmax and SUVmean in Normal Organs Before and After Sandostatin LAR Treatment
No significant differences in the SUVmax were found in any metastatic lesions in the liver, bone, lung, or lymph nodes before and after Sandostatin LAR administration (P > 0.05). We analyzed the SUVmean of the metastatic lesions before and after Sandostatin LAR treatment. There were no significant differences in the SUVmean before and after Sandostatin LAR treatment (P > 0.05). Table 3 shows the mean pre- and posttreatment SUVmax and SUVmean for the metastatic lesions examined. We compared the SUVmax and SUVmean for the hottest lesion (i.e., with the highest SUVmax) in each scan before and after Sandostatin LAR therapy. The mean SUVmax for the hottest lesion was 26.8 ± 14.7 before Sandostatin LAR therapy and 27.8 ± 13.3 after Sandostatin LAR therapy (P = 0.58), and the mean SUVmean was 19.9 ± 10.2 and 20.3 ± 9.1, respectively (P = 0.79). For the residual primary tumors, the mean SUVmax was 15.3 ± 8.0 before Sandostatin LAR therapy and 13.3 ± 6.9 after Sandostatin LAR therapy (P = 0.087), and the mean SUVmean was 12.4 ± 5.9 and 11.0 ± 4.8, respectively (P = 0.179).
Mean SUVmax and SUVmean in Metastatic Lesions Before and After Sandostatin LAR Treatment
DISCUSSION
In the present study, the effect of long-acting somatostatin analog treatment on 68Ga-DOTATATE uptake in patients with NETs was assessed. To our knowledge, this study is the first to assess 68Ga-DOTATATE uptake in the same subset of patients before and after the administration of a long-acting somatostatin analog.
SSTR imaging guidelines recommend the withdrawal of octreotide therapy before imaging because of the possibility of interference of cold octreotide with tracer uptake in tumor cells, caused by competition for receptor occupancy as well as SSTR blockade (11,20). However, in vitro studies (14,21–23), in vivo animal studies (24), and human studies (25) have all shown that octreotide treatment strongly triggers agonist-induced internalization of subtype 2 SSRT and alters the degree of SSTR expression in NETs.
In the present study, we showed that primary tumor sites and metastatic lesions exhibited similar 68Ga-DOTATATE uptake before and after the administration of a long-acting somatostatin analog; however, 68Ga-DOTATATE uptake was significantly reduced in the liver, spleen, and thyroid after the treatment. Our findings suggest that pretreatment with somatostatin analogs does not affect the detection of metastatic disease and, in fact, reduces background uptake in normal organs; the later effect enhances the tumor-to-background ratio and facilitates tumor detection. Possible explanations for our findings are the difference in the internalization patterns in normal tissues and tumor cells (25) and the potential upregulation of SSTR expression after somatostatin analog therapy. These mechanisms may compensate for each other and, consequently, negate possible decreases in 68Ga-DOTATATE accumulation in metastatic lesions. Previous studies showed that NETs may have heterogeneous SSTR expression (25) and may respond differently to somatostatin analog treatment. To address this potentially confounding issue, we compared 68Ga-DOTATATE uptake in the same lesions in individual patients and used both SUVmean and SUVmax in our analysis.
The finding that there were no differences in adrenal and pituitary gland uptake before and after Sandostatin LAR treatment is interesting and is in agreement with the results of a previous study (18). However, significant differences in uptake were found in other normal organs (liver, spleen, and thyroid). This finding may have been due to physiologic variability in SSTR expression among different organs, as previously reported (26,27).
Two previous studies (17,18) investigated the effect of somatostatin analog treatment on 111In-octreotide uptake and reported increases in tumor-to-background ratios after octreotide administration. However, both studies evaluated small populations (5 and 8 patients), and the tumor-to-background ratios measured in the latter study were quite heterogeneous—ranging from −79% to +0.87%, with an average of 50% (17,18). In the only previously published study on the effect of cold somatostatin analog treatment on the uptake of 68Ga-labeled somatostatin analogs, Haug et al. (19) compared 68Ga-DOTATATE uptake in 2 groups of patients with NETs: 1 group received long-acting octreotide treatment, whereas the other did not. Lower tracer uptake was found in normal liver and spleen tissues in the treated patients, whereas no significant difference in radiotracer uptake was found in the metastatic lesions in the 2 groups (19). Intraindividual assessments of 9 patients also showed that uptake was unaffected after octreotide treatment. The results of the present study agree with the results obtained in the previous studies for both normal organ uptake and residual primary tumor activity.
To reduce the interfering effect of somatostatin analog treatment on SSTR imaging, some guidelines have recommended scheduling the imaging just before the next dose (28-d intervals); however, a previous study showed a steady-state profile for long-acting octreotide (28) with a long maintenance period of greater than 0.01 ng/mL/mg by week 12 or 13. Further studies comparing 68Ga-DOTATATE uptake in patients with less and more than 28-d intervals between the last octreotide injection and imaging may be needed. Although the present study evaluated the effect of initial somatostatin analog treatment on 68Ga-DOTATATE uptake in NETs, in many patients 68Ga-DOTATATE PET studies are performed throughout the course of their treatment and at different times from somatostatin analog administration. The results of the present study provide important information on the potential effect of the time after treatment on initial 68Ga-DOTATATE scans, which may be relevant to repeat imaging in individual patients.
In the present study, all patients were imaged using 68Ga-DOTA-Tyr3-octreotate (68Ga-DOTATATE). Although variable affinity for SSTR subtypes has been reported for somatostatin analogs with different labeling, the imaging characteristics of these radiotracers are similar (29,30). Therefore, our results might be extended to all PET tracer–radiolabeled somatostatin molecules. The slow-growth nature of NETs as well as the potential antiproliferative properties of somatostatin analogs could imply differences in disease status. However, the present study was not designed to assess the therapeutic activity of somatostatin analogs or the ability of 68Ga-DOTATATE to assess or predict a response.
Although the present study has the advantage of a comparison of data within the same subset of patients, because of the retrospective nature, the time interval between the 2 PET/CT imaging studies was quite long (9.6 mo). A prospective study with a shorter imaging interval (e.g., SSTR PET before somatostatin analog treatment and after the first or second administration) would be helpful.
CONCLUSION
Long-acting somatostatin analog treatment decreased 68Ga-DOTATATE uptake in the liver, spleen, and thyroid but did not compromise 68Ga-DOTATATE uptake in residual primary tumor or metastatic lesions. These findings support the sensitivity of SSTR imaging for the detection of metastasis in patients receiving somatostatin analog treatment.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Jul. 20, 2017.
- © 2018 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication February 27, 2017.
- Accepted for publication June 28, 2017.





{kind=link}
Jump to section
Related Articles
Cited By...
- Factors Associated with Myocardial Uptake on Oncologic Somatostatin PET Investigations and Differentiation from Myocardial Uptake of Acute Myocarditis
- SNMMI Procedure Standard/EANM Practice Guideline for SSTR PET: Imaging Neuroendocrine Tumors
- Systemic Radiopharmaceutical Therapy of Pheochromocytoma and Paraganglioma
- Head-to-Head Comparison of 68Ga-DOTA-JR11 and 68Ga-DOTATATE PET/CT in Patients with Metastatic, Well-Differentiated Neuroendocrine Tumors: A Prospective Study
- A Prospective Observational Study to Evaluate the Effects of Long-Acting Somatostatin Analogs on 68Ga-DOTATATE Uptake in Patients with Neuroendocrine Tumors