


Abstract
A reliable prediction of a pathologic complete response (pathCR) to chemoradiotherapy before surgery for esophageal cancer would enable investigators to study the feasibility and outcome of an organ-preserving strategy after chemoradiotherapy. So far no clinical parameters or diagnostic studies are able to accurately predict which patients will achieve a pathCR. The aim of this study was to determine whether subjective and quantitative assessment of baseline and postchemoradiation 18F-FDG PET can improve the accuracy of predicting pathCR to preoperative chemoradiotherapy in esophageal cancer beyond clinical predictors. Methods: This retrospective study was approved by the institutional review board, and the need for written informed consent was waived. Clinical parameters along with subjective and quantitative parameters from baseline and postchemoradiation 18F-FDG PET were derived from 217 esophageal adenocarcinoma patients who underwent chemoradiotherapy followed by surgery. The associations between these parameters and pathCR were studied in univariable and multivariable logistic regression analysis. Four prediction models were constructed and internally validated using bootstrapping to study the incremental predictive values of subjective assessment of 18F-FDG PET, conventional quantitative metabolic features, and comprehensive 18F-FDG PET texture/geometry features, respectively. The clinical benefit of 18F-FDG PET was determined using decision-curve analysis. Results: A pathCR was found in 59 (27%) patients. A clinical prediction model (corrected c-index, 0.67) was improved by adding 18F-FDG PET–based subjective assessment of response (corrected c-index, 0.72). This latter model was slightly improved by the addition of 1 conventional quantitative metabolic feature only (i.e., postchemoradiation total lesion glycolysis; corrected c-index, 0.73), and even more by subsequently adding 4 comprehensive 18F-FDG PET texture/geometry features (corrected c-index, 0.77). However, at a decision threshold of 0.9 or higher, representing a clinically relevant predictive value for pathCR at which one may be willing to omit surgery, there was no clear incremental value. Conclusion: Subjective and quantitative assessment of 18F-FDG PET provides statistical incremental value for predicting pathCR after preoperative chemoradiotherapy in esophageal cancer. However, the discriminatory improvement beyond clinical predictors does not translate into a clinically relevant benefit that could change decision making.
Preoperative chemoradiotherapy followed by surgery is increasingly applied as standard treatment with curative intent for patients with resectable nonmetastatic esophageal cancer (1). A pathologic complete response (pathCR) to chemoradiotherapy is observed in approximately 25%–30% of esophageal cancer patients (1–4). Many studies have reported that pathCR is associated with favorable overall survival rates (2–4). Whether or not surgery can be safely omitted in patients who achieve a pathCR is an important focus of research, but determining pathCR is difficult without performing surgery (5). A reliable prediction of pathCR before surgery would enable investigators to study the feasibility and outcome of an organ-preserving strategy after chemoradiotherapy that includes omission of surgery and close clinical follow-up. Unfortunately, so far no clinical parameters or diagnostic studies are able to accurately predict which patients will achieve a pathCR (6–9). Therefore, seeking more powerful predictors for pathCR is of high relevance to modern personalized cancer care for which the aim is to tailor treatment to the individual patient.
18F-FDG PET is a well-established imaging modality for the initial staging of esophageal cancer and restaging after preoperative chemoradiotherapy for the detection of distant (interval) metastases (10–12). The value of 18F-FDG PET to predict response to preoperative chemoradiotherapy in patients with esophageal cancer has been studied extensively with wide varying methodologies and conflicting results (6,10,13). Some investigators examined the value of a (subjective) determination of clinical response by experienced nuclear medicine physicians based on 18F-FDG PET scanning after chemoradiotherapy (11,12,14). Most other 18F-FDG PET studies evaluated the value of quantitative metabolic parameters such as the SUVmean or SUVmax within a tumor for assessment of response (5,6,12,13,15). A few studies evaluated more advanced 18F-FDG PET–based metabolic parameters such as metabolic tumor volume (MTV) and total lesion glycolysis (TLG) for response prediction (16–18). Unfortunately, all these methods have not shown sufficient capability of 18F-FDG PET to predict response and guide clinical decision making.
More recently, 18F-FDG PET image texture analysis has been proposed to characterize heterogeneity of intratumoral 18F-FDG uptake, which may provide a useful representation of underlying biologic tumor characteristics (19). Texture analysis refers to a variety of computational methods that describe the relationships between the intensity of voxels and their position within an image (20). Although 18F-FDG PET texture features are not routinely used in clinical evaluation of 18F-FDG PET images, there is increasing recognition that a potential complementary role may exist for prediction of treatment response and prognosis in several cancers (20). The aim of this diagnostic study was to develop and internally validate multivariable prediction models to determine the incremental value of baseline and postchemoradiation 18F-FDG PET scanning for predicting pathCR after chemoradiotherapy in esophageal cancer beyond clinical predictive factors. In a large cohort, the added predictive values of subjective assessment of 18F-FDG PET scans, conventional quantitative metabolic parameters, and comprehensive quantitative 18F-FDG PET texture/geometry features for pathCR were evaluated, respectively.
MATERIALS AND METHODS
This retrospective study was approved by the Institutional Review Board of the MD Anderson Cancer Center (MDACC), and the need for written informed consent was waived. The study was conducted in accordance with the Health Insurance Portability and Accountability Act, the checklist from the STAndards for the Reporting of Diagnostic accuracy studies statement (http://www.stard-statement.org) (21), and the Transparent Reporting of a multivariable prediction model for Individual Prognosis or Diagnosis statement (http://www.tripod-statement.org) (22).
Study Population
All consecutive patients with a biopsy-proven resectable adenocarcinoma of the esophagus or gastroesophageal junction and no distant metastases who underwent preoperative chemoradiotherapy followed by surgery at MDACC from January 2006 to October 2013 were extracted from a prospective database. Patients were included only if results from baseline 18F-FDG PET, postchemoradiation 18F-FDG PET, and postchemoradiation endoscopic biopsy were available. Exclusion criteria were nonavailability of a baseline 18F-FDG PET scan acquired at MDACC, non–18F-FDG avidity of the tumor at baseline, Siewert type 3 gastroesophageal junction tumors, and an esophageal stent in situ at the time of 18F-FDG PET scanning. In addition, patients with a time interval between completion of chemoradiotherapy and surgery of less than 5 wk or more than 14 wk—indicating urgent and salvage resections, respectively—were excluded. A detailed description of the treatment regimen and 18F-FDG PET image acquisition is provided in Supplemental Appendix A (supplemental materials are available at http://jnm.snmjournals.org).
Histopathologic Assessment
The degree of histopathologic tumor regression in the resected specimen was assigned to 1 of 4 tumor regression grades (TRGs) by experienced pathologists: complete absence of residual cancer (i.e., pathCR), 1%–10% residual carcinoma, 11%–50% residual carcinoma, and greater than 50% residual carcinoma (2). PathCR (i.e., TRG 1) as opposed to any grade of residual carcinoma (i.e., TRGs 2–4) was considered the reference standard. Another commonly made distinction between TRGs 1 and 2 (i.e., 0%–10% residual carcinoma) and TRGs 3 and 4 (i.e., ≥11% residual carcinoma) was not made, because this distinction is rather arbitrary in terms of interpathologist reproducibility and overall survival (2,4,23), and the potential clinical consequences of such a distinction are unclear.
Quantitative Image Analysis
Only the primary esophageal tumors were considered for imaging analysis, as texture analysis cannot be reliably performed on small lesions (such as nodal metastases) because of the small number of voxels (24,25). The primary tumor volume was defined as the volume of interest and delineated using a semiautomatic gradient-based delineation method (26) from commercially available software (MIM Software Inc.), followed by manual editing by 1 interpreter. A rationale for using this method is provided in Supplemental Appendix B. The interpreter was masked to other clinical information and to the reference standard. Contours were extracted, and quantitative 18F-FDG PET analysis was performed using the Imaging Biomarker Explorer software package (27) built in-house with commercial software (Matlab, version 8.4; The MathWorks Inc.).
Test–Retest Analysis
The authors recognized that not all 18F-FDG PET features were sufficiently robust (28,29) and therefore aimed to include only features that had sufficient robustness in the prediction modeling. To fulfill this goal, 18F-FDG PET scans taken outside MDACC (with different types of scanners and scan protocols) were used and compared with diagnostic 18F-FDG PET scans taken within MDACC. A subgroup of 7 patients who underwent this form of double baseline scanning, with an average separation between the 2 scans of 31 d (range, 11–42 d), was identified. A single observer contoured the tumor volumes for the test–retest scans on separate occasions. In this way, both robustness and intraobserver contour variability were incorporated in test–retest analysis. For each image-derived parameter, the intraclass correlation coefficient (ICC) was calculated, using an absolute agreement definition in a 2-way mixed-effects model (30), to quantify the relatedness of the 2 scans per parameter.
Statistical Analysis
Statistical analysis was performed using SPSS 20.0 (IBM Corp.) and R 3.1.2 open-source software (http://www.R-project.org). A P value of less than 0.05 was considered statistically significant.
Model Development
A detailed description on the studied parameters, standardized preselection of variables for multivariable analysis, multivariable model development, and model performance tests and validation is provided in Supplemental Appendix C. The association between clinical parameters and pathCR was studied univariably. A χ2 test or Fisher exact test (in the case of small cell count) was used for categoric variables, and a Student t test or Mann–Whitney U test was used for parametric or nonparametric continuous clinical variables. The predictive value of each 18F-FDG PET–based parameter for pathCR was quantified using univariable logistic regression analysis providing odds ratios with 95% confidence intervals. Various features were logarithmically transformed to improve on the assumption of linearity on the logit scale.
Because many potential predictors were studied in univariable analysis, a standardized preselection of variables for multivariable analysis was performed, taking into account test–retest robustness and multicollinearity between parameters (Supplemental Appendix C). Four multivariable logistic regression models were constructed using stepwise backward elimination to study the value of clinical parameters (model 1), the added value of subjective assessment of 18F-FDG PET (model 2), and the subsequent added value of conventional and comprehensive quantitative 18F-FDG PET parameters (models 3 and 4, respectively), for the prediction of pathCR.
Model Performance and Validation
Model discrimination and calibration results were evaluated for all 4 models using c-indices and visual inspection of model calibration plots, respectively. Internal validation using the bootstrap method with 1,000 repetitions was performed to provide insight into potential overfitting and optimism in model performance. Bootstrapping allowed for calculation of bias-corrected c-indices of the 4 models and provided shrinkage factors that were used to adjust the estimated regression coefficients in the final 4 models for overfitting and miscalibration (31). A sensitivity analysis was performed on a subcohort of tumors with an initial MTV above 10 mL, because a recent study suggested that texture analysis may only provide valuable complementary information in tumors larger than 10 mL (24). In addition, the influence of including cases with 2-dimensional-acquisition 18F-FDG PET scans (besides 3-dimensional-acquisition 18F-FDG PET scans) in the model development set was determined by sensitivity analysis.
Clinical Benefit
Because traditional accuracy metrics—such as the c-index—have limited value for clinical decision making in the individual patient, the incremental clinical value of 18F-FDG PET analysis was determined using decision-curve analysis (32). In this net benefit assessment, the adverse effect of falsely predicting pathCR in non-pathCR patients (e.g., false-positives) is incorporated. In fact, a personal decision threshold can be chosen according to the willingness of risking a false-positive result. In the context of predicting pathCR in esophageal cancer, a false-positive finding could result in omission of surgery in a patient with residual disease, which is potentially hazardous (14,33), and therefore the decision threshold should be high (e.g., ∼0.9). To evaluate the incremental value of a model including 18F-FDG PET information, the net benefit (demonstrated on the y-axis) of the model should be higher than the model without that information. Divergence of a model’s decision curve from another model’s decision curve indicates difference in net benefit, but it depends on the personal decision threshold whether this is of clinical relevance. The decision curves of the 4 models used in the present study are presented together with the net benefit of making the same decision for all patients (i.e., performing surgery in all patients or omitting surgery in all patients). Additional explanation on the decision-curve analysis is provided in Supplemental Appendix C.
RESULTS
From 324 patients with an esophageal adenocarcinoma that met the prespecified inclusion criteria, 107 patients were excluded because of nonavailability of a baseline 18F-FDG PET scan acquired at MDACC (n = 48), non–18F-FDG avidity at baseline (n = 18), a Siewert type 3 gastroesophageal junction tumor (n = 15), an esophageal stent in situ at the time of 18F-FDG PET scanning (n = 1), or a time interval between completion of chemoradiotherapy and surgery of less than 5 wk (n = 1) or more than 14 wk (n = 24). A pathCR was found in 59 (27%) of the 217 eligible patients. Patients in the pathCR group had a mean age of 59 y, and 92% (n = 54) of them were men, whereas patients with residual carcinoma had a mean age of 60 y and 94% of them were men (Table 1).
Clinical Baseline and Treatment-Related Characteristics
Univariable Analysis
Smaller endoscopic ultrasound (EUS)–based tumor length and less advanced depth of tumor infiltration (i.e., clinical stage T2 vs. T3) were significantly associated with a higher chance of pathCR (P = 0.034 and 0.006, respectively). The subgroup of 78 patients (36%) who underwent induction chemotherapy before trimodality therapy showed a significantly higher pathCR rate than the group without induction chemotherapy (36% vs. 22%, respectively; P = 0.031). The postchemoradiation endoscopic biopsy result was significantly associated with pathCR (P = 0.023), although the predictive value of an endoscopic biopsy–based complete response for pathCR was only 30% (55/181).
Univariable analysis of subjective assessment and conventional quantitative features of 18F-FDG PET for predicting pathCR are presented in Table 2. Similar to endoscopic biopsy, subjective assessment of the postchemoradiation 18F-FDG PET scan was significantly associated with pathCR (P < 0.001), but only 27 of 60 patients (45%) with a clinical complete response on 18F-FDG PET had a true pathCR. There was a trend toward a lower baseline SUVmax in pathologic complete responders (P = 0.087). Some of the conventional quantitative features on the postchemoradiation 18F-FDG PET scan were significantly related to a higher chance of pathCR including lower SUVmax (P = 0.015), lower MTV (P < 0.001), and lower TLG (P < 0.001).
Univariable Analysis of Subjective and Conventional Quantitative Assessment of 18F-FDG PET for Predicting pathCR
Test–retest relatedness of the conventional 18F-FDG PET features was good (ICCs of SUVmax, SUVmean, MTV, and TLG were 0.86, 0.87, 0.99, and 0.96, respectively). For each comprehensive 18F-FDG PET feature, the ICCs resulting from test–retest analysis along with univariable analyses for predicting pathCR are presented in Supplemental Tables 1 and 2. In general, test–retest relatedness was excellent for geometry features (median ICC, 0.92); good for first-, second-, and regional higher-order texture features (median ICC, 0.86, 0.83, and 0.85, respectively); and poor for local higher-order texture features (median ICC, 0.69).
Multivariable Analysis
Table 3 shows the finalized multivariable analysis of the 4 prediction models. In the clinical model (model 1), 4 variables remained associated with a higher chance of pathCR (EUS-based tumor length, clinical T stage, induction chemotherapy, and postchemoradiation endoscopic biopsy). Adding the subjective assessment of response on postchemoradiation 18F-FDG PET to the clinical model significantly improved the model (model 2). Although 8 conventional quantitative 18F-FDG PET features showed a P value of 0.25 or less in univariable analysis, only 4 (baseline SUVmax, ∆MTV, postchemoradiation SUVmax, and posttreatment TLG) were preselected for multivariable analysis because of several strong interparameter correlations (i.e., multicollinearity). After stepwise elimination, only posttreatment TLG appeared to provide significant model improvement (model 3).
Finalized Prediction Models for pathCR Using Multivariable Logistic Regression Analysis with Stepwise Backward Elimination
Many geometry and first- and second-order texture features from the postchemoradiation 18F-FDG PET appeared significantly associated with pathCR in univariable analysis (Supplemental Table 1). However, most of these features were highly correlated with postchemoradiation TLG (i.e., did not provide additional information but would increase the risk of multicollinearity) and were not preselected for multivariable analysis. Subsequently, 9 comprehensive 18F-FDG PET features that met the preselection criteria were added to model 3 to construct model 4. Four of these features remained significantly important to the model after stepwise elimination (i.e., baseline cluster shade, ∆run percentage, ∆ICM entropy, and postchemoradiation roundness). Examples of 18F-FDG PET scans before and after chemoradiotherapy in patients with and without a pathCR are provided in Figure 1.
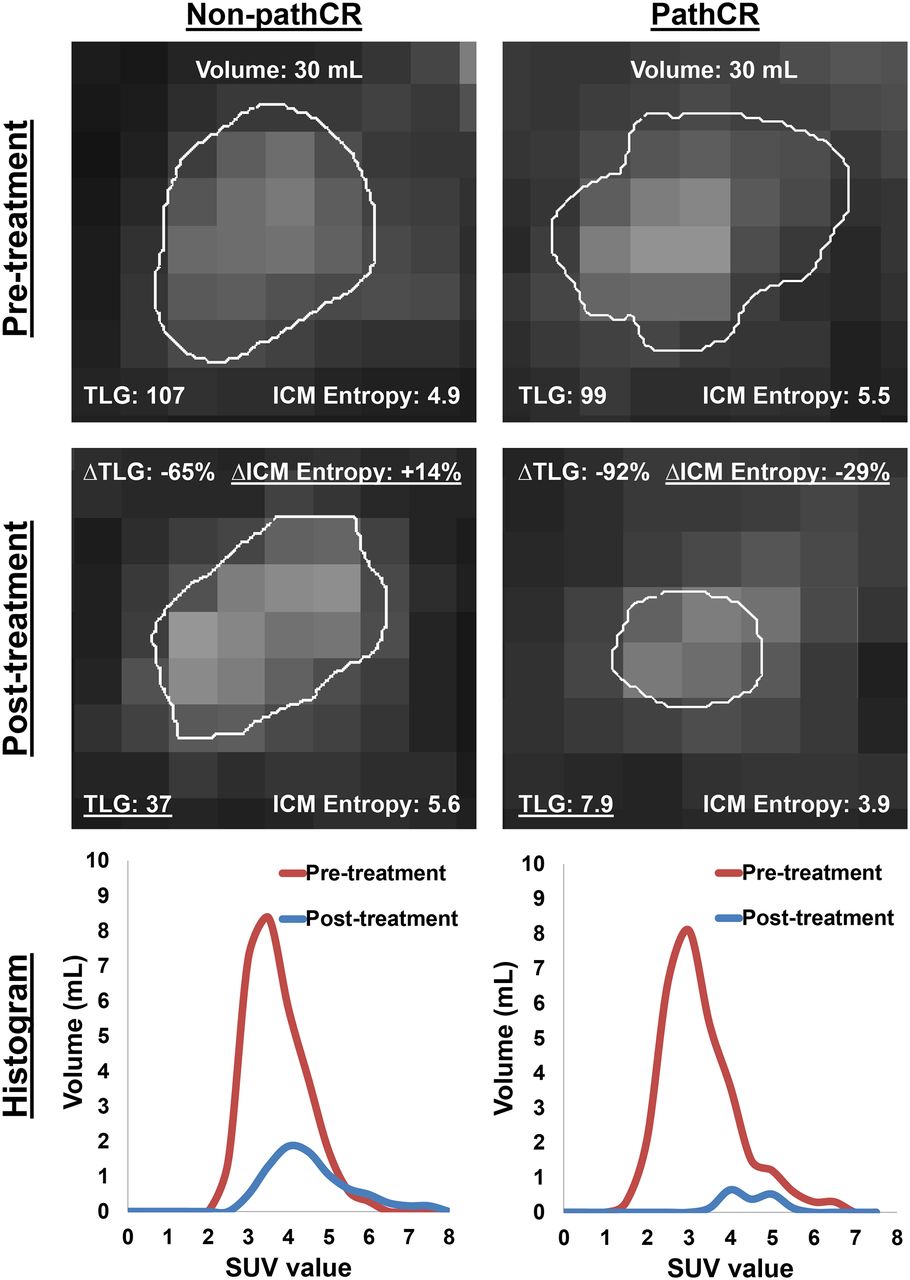
Examples of representative transverse slices of 18F-FDG PET scans before and after chemoradiotherapy in patient with no pathCR (i.e., non-pathCR) and in patient with a pathCR. These patients initially had comparable tumor volume, TLG, and local tumor texture (as expressed by intensity cooccurrence matrix [ICM] entropy metric). However, in the complete responder, ∆ICM entropy metric decreased and posttreatment TLG was markedly lower (underlined), which represent 2 of the important predictors in models 3 and 4. Histograms illustrate 3-dimensional 18F-FDG uptake within volumes of interest.
Model Performance
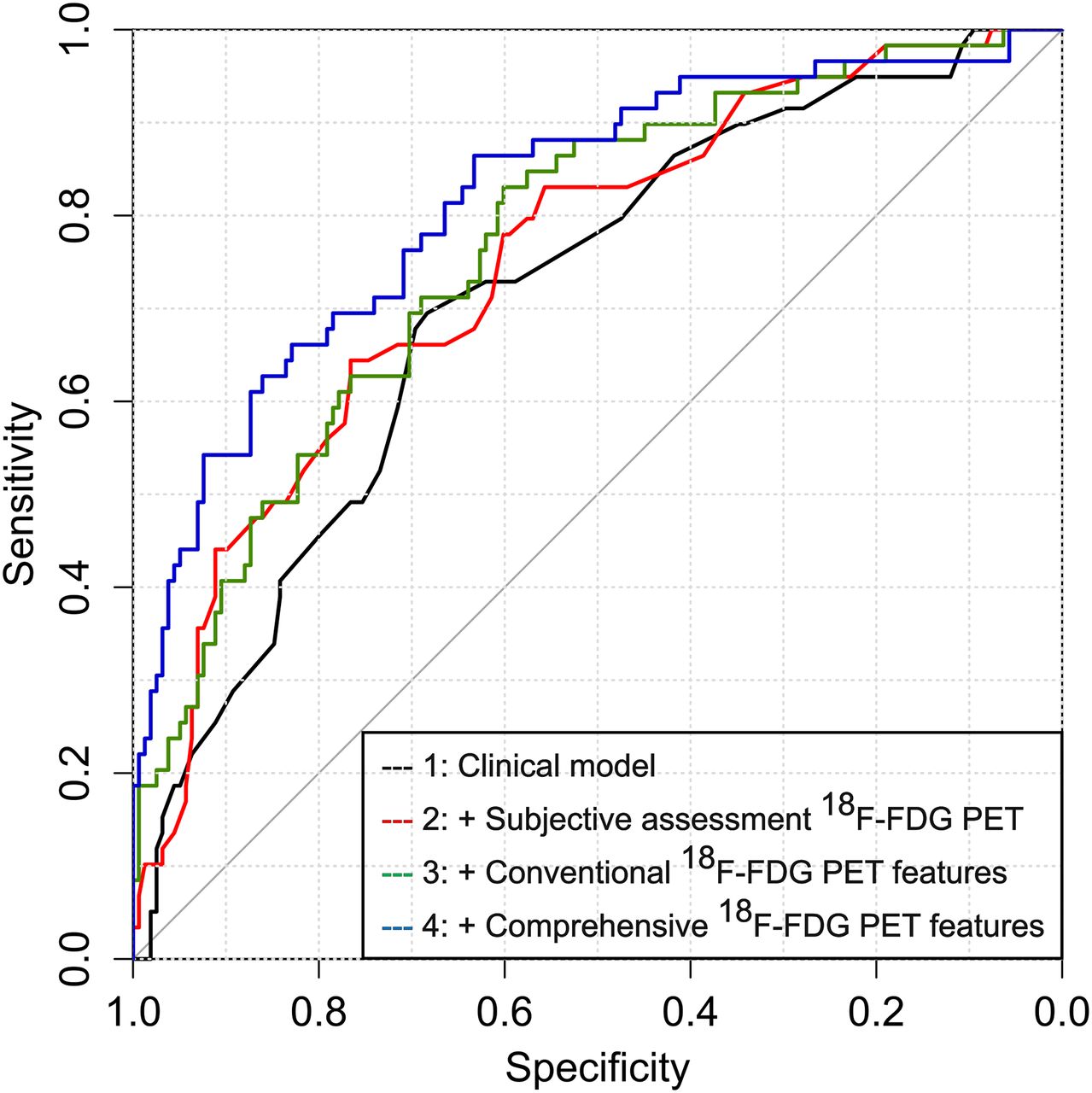
Measures of the performance of each model are presented in Table 4. Discrimination was moderate to good for all 4 models, with c-indices ranging from 0.71 for the clinical model to 0.75, 0.77, and 0.82 for the more complex models including subjective assessment of 18F-FDG PET and conventional and comprehensive quantitative 18F-FDG PET features, respectively (Fig. 2). After internal validation, the corrected c-indices appeared slightly lower (0.67, 0.72, 0.73, and 0.77 for models 1, 2, 3, and 4, respectively), indicating a limited degree of (a combination of) overfitting and bias due to the predictor selection process.
Estimates of Model Performance for 4 Prediction Models

Receiver-operating-characteristic curve analysis of the 4 models indicating their ability to discriminate between pathCR and non-pathCR patients.
Visual inspection of the consecutive model calibration plots showed a good overall fit (Fig. 3). In general, the models tended to slightly overestimate the incidence of pathCR and underestimate the incidence of residual cancer as a result of minimal overfitting (Fig. 3). In Supplemental Table 3, the logistic regression formulas of the 4 models are presented in which the minimal overfitting and miscalibration were considered by applying a shrinkage factor that was obtained by bootstrapping.

(A–D) Calibration plots of the 4 models demonstrating agreement between predicted probability of pathCR by model and observed incidence.
Sensitivity analysis demonstrated no relevant change in discrimination after excluding 45 cases with initial tumor volumes below 10 mL (corrected c-indices, 0.67, 0.70, 0.72, and 0.78 for models 1, 2, 3, and 4, respectively) or after excluding 65 cases with 2-dimensional-acquisition 18F-FDG PET scans (corrected c-indices, 0.69, 0.69, 0.71, and 0.74 for models 1, 2, 3, and 4, respectively).
Clinical Benefit
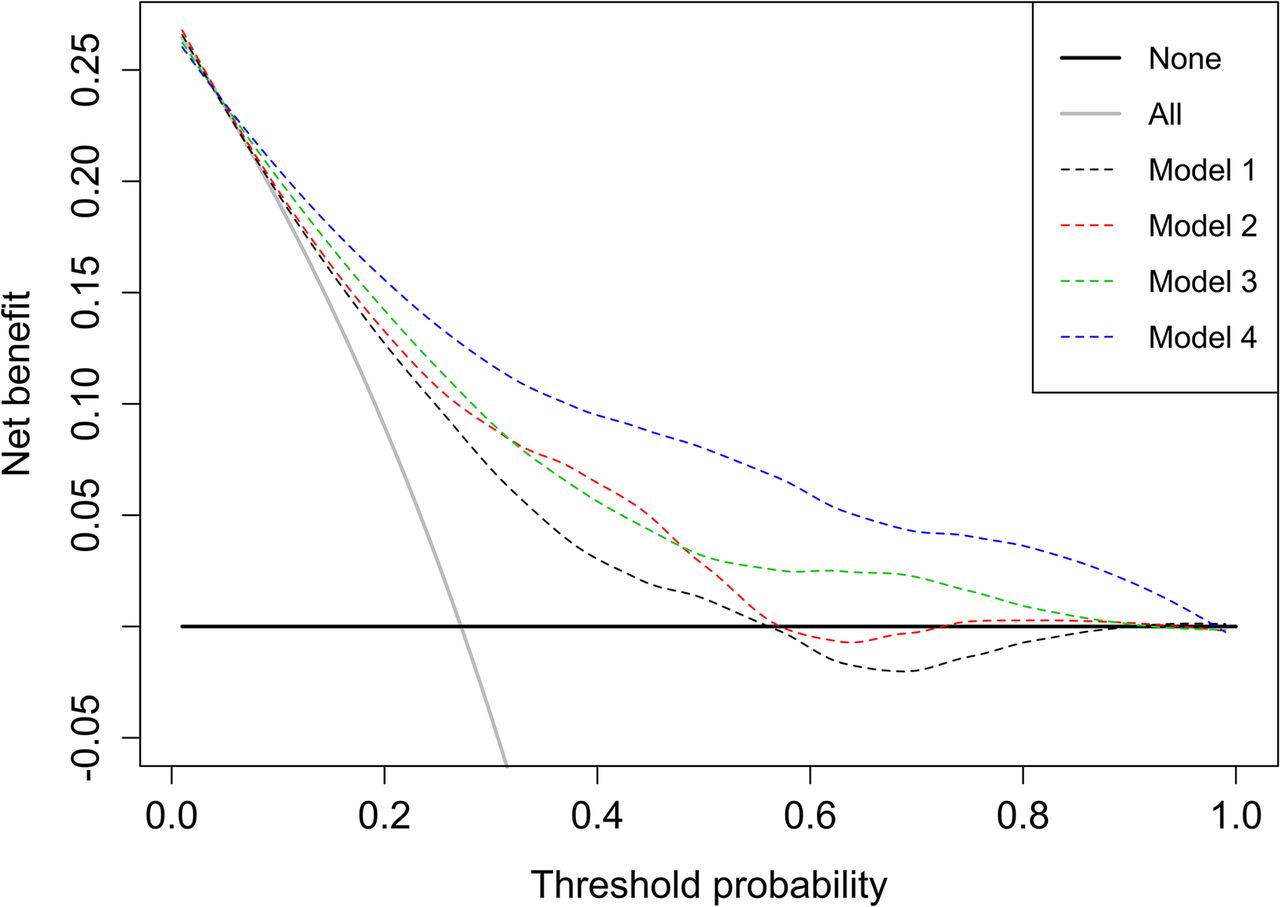
The decision curves of the models for the prediction of pathCR are displayed in Figure 4. At decision thresholds ranging from approximately 0.3 to approximately 0.7, some incremental value of 18F-FDG PET–based analyses (i.e., models 2–4) beyond clinical predictors (i.e., model 1) was suggested by the divergence between the decision curves. However, at a decision threshold of 0.9 or higher—representing a clinically relevant predictive value for pathCR of 90% or more at which one may be willing to omit surgery—there was no clear incremental value of the prediction models (net benefit, 0% for models 1–3, and 1.8% for model 4).

Decision curves graphically representing net benefit (y-axis) for the 4 models at a range of decision thresholds (i.e., minimum probabilities of pathCR at which one would be willing to change clinical decision making; x-axis). The black and gray solid lines represent making same decision in all patients (i.e., omitting surgery in none or in all of the patients, respectively).
DISCUSSION
This study demonstrates incremental value of baseline and postchemoradiation 18F-FDG PET scanning for predicting pathCR after preoperative chemoradiotherapy in esophageal cancer beyond clinical predictive factors in terms of discrimination. A clinical prediction model (corrected c-index, 0.67) was improved by adding the subjective assessment of response by an experienced nuclear medicine physician on a postchemoradiation 18F-FDG PET scan (corrected c-index, 0.72) and even more by subsequently adding comprehensive quantitative 18F-FDG PET feature analysis (corrected c-index, 0.77). In terms of clinical benefit, however, both the clinical and the more complex 18F-FDG PET–based multivariable models were not able to provide reliable predictive values for pathCR of approximately 90% or more, which was supported by the lack of net benefit (0%–1.8%) in decision-curve analysis at this clinically relevant decision threshold. In our opinion, these findings suggest that adding simple or complex 18F-FDG PET analyses to clinical parameters for the prediction of pathCR does not aid the clinician to such a reliable extent that one may be willing to omit surgery in predicted complete responders.
The recent recognition that medical images may contain more useful information than can be perceived with the naked eye led to the field of radiomics, in which comprehensive features can be extracted by computational postprocessing algorithms (20). Evidence is slowly emerging that these comprehensive texture and geometry features may yield additional predictive and prognostic information in several solid tumors (20). Although a single feature is not directly linked to a specific biologic process, investigators assume that a combination of image-derived textural (and geometry) features may be closely related to underlying biologic processes such as vascularization, cell density, tumor aggressiveness, or hypoxia (20,34), which in turn may be related to the degree of chemoradiation resistance. In accordance with what one could reasonably expect, a tumor exhibiting a heterogeneous—compared with a homogeneous—18F-FDG distribution at baseline (i.e., higher cluster shade) was less likely to reach pathCR in our analysis. Similarly, a larger change toward a more homogeneous 18F-FDG uptake and a greater loss in the amount of information (or unpredictability) as a result of chemoradiotherapy—as reflected by ∆run percentage and ∆ICM entropy, respectively—resulted in a higher chance of pathCR. After chemoradiotherapy, more roundly shaped 18F-FDG uptake with higher TLG was more likely to represent residual cancer.
Several investigators have studied the predictive value of baseline or postchemoradiation 18F-FDG uptake for treatment response in esophageal cancer. Large recent studies (n = 88–284) reported that the predictive value of a clinical complete response based on postchemoradiation 18F-FDG PET (either or not combined with endoscopic biopsy) for pathCR was low (range, 20%–64%) (11,12,14), a finding that was confirmed in the current study (45%). In other studies, pathologic response was variably found to be associated with image-derived quantitative parameters such as baseline SUVmax (35) and MTV (17), or postchemoradiation SUVmax (5) and SUVmean (36), or the relative change in SUVmax, MTV, and TLG (16,37). In the current study, a similar trend—although nonsignificant—was observed for baseline SUVmax (P = 0.087), whereas postchemoradiation SUVmax, MTV, and TLG were significantly associated with pathCR (P = 0.015, P < 0.001, and P < 0.001, respectively). Importantly, however, in former studies as well as the current study, these subjective and quantitative 18F-FDG PET parameters did not allow differentiation of pathCR from nonpathCR with high accuracy, a distinction that could be useful for clinical decision making. This emphasizes the difference between a significant association of a parameter with pathologic response and a true predictive value in terms of discrimination or incremental value beyond other predictors. To this regard, we encourage investigators to study new potential diagnostic biomarkers not only for their univariable association with pathologic response, but also for their predictive value and incremental value using a multivariable approach.
In esophageal cancer, 4 recent pilot studies from 2 research groups observed that 18F-FDG PET texture features seemed more informative than conventional metabolic parameters for the prediction of response to chemoradiotherapy (Table 5) (29,34,38,39). However, these studies were generally limited by small sample size (n = 20 to n = 50), heterogeneity of included tumor types and stages, lack of internal validation, and high likeliness of model overfitting and overoptimism of reported results. Also, the used reference standard was suboptimally defined according to RECIST (29,34)—which is known to correlate poorly with pathologic response (8)—or pathCR was mixed together as 1 group with microscopic residual disease (38,39) while these groups are considered different entities associated with different survival rates (2,4). In addition, the studies differed from the current study regarding the used delineation method. All these substantial differences with the current study compromise proper comparison.
Overview of Studies on 18F-FDG PET Texture Analysis in Esophageal Cancer for Treatment Response Assessment
The reported influences of clinical parameters—including pretreatment EUS-based tumor length and T stage and posttreatment endoscopic biopsy—on the probability of pathCR in our study were in accordance with existing literature (5,40,41). The finding that induction chemotherapy before chemoradiotherapy was associated with a significantly higher rate of pathCR in the current series was in line with a recent phase II randomized trial at MDACC that did report a difference in pathCR rate in favor of induction chemotherapy (26% vs. 13%), but this difference was not statistically significant in that trial (P = 0.094) (42). The difference in significance and nonsignificance of the influence of induction chemotherapy on pathCR between the current study and the randomized trial cannot be fully explained. Potential explanations are possible selection bias through selecting operated patients in the current study only or a lack of statistical power (i.e., sample size) in the randomized trial. However, in the current study the significant difference between the 2 groups was considered not negligible, and induction chemotherapy was therefore entered into the multivariable prediction modeling process.
Several limitations apply to this study. First, slight model overfitting occurred despite the large sample size. Therefore, we reported optimism-corrected model performance estimates resulting from internal validation in addition to apparent estimates. In addition, external validation of the prediction models would be necessary to determine the residual overestimation of generalizability caused by the issue of multiple testing that was inherent to the explorative character of this study. Second, pathologic response in the primary tumor alone was examined, whereas a pathCR of the primary tumor may not completely exclude residual lymph node involvement (17), and potentially useful information provided by 18F-FDG PET on lymph node involvement and response could have been missed. Particularly in patients with large lymphadenopathies, texture analysis could potentially provide valuable complementary information (24,25). Third, it should be acknowledged that the MTV threshold of 10 mL used for sensitivity analysis may not have been perfectly chosen, because it was based on a previous study that applied slightly different calculation methods for the texture features (24). Fourth, the MTV on the postchemoradiation scan was small in many cases, which could have compromised the reliability of the texture features analysis of these scans. Finally, inherently to the retrospective character of this study, the authors could not determine whether more modern reconstruction protocols using smaller voxel sizes, smaller postreconstruction filtering methods, and isotropic rather than anisotropic voxels (43) could potentially provide incremental information on tumor heterogeneity. However, our analysis was strengthened by using a prospectively maintained database, including clinical parameters that are practical, restricting analysis to robust features only, studying incremental rather than isolated predictive values, performing internal validation of the developed models, assessing added value in terms of clinical benefit, and providing novel findings.
No comparison with diffusion-weighted MRI (DW-MRI) was performed in this study. However, in a recent prospective explorative study our group found that the treatment-induced change in the median tumor apparent diffusion coefficient during the first 2–3 wk of preoperative chemoradiotherapy as determined on DW-MRI seemed highly predictive of pathCR (44). In future research, a multimodality imaging approach—rather than using 18F-FDG PET alone—might prove to provide sufficient incremental predictive value for pathCR beyond clinical predictors to safely guide treatment decision making. Therefore, in a recently initiated multicenter study (ClinicalTrials.gov, NCT02125448) we aim to evaluate the potential complementary value of DW-MRI in addition to 18F-FDG PET for predicting pathCR by performing both DW-MRI and 18F-FDG PET before, during, and after preoperative chemoradiotherapy in patients with esophageal cancer.
CONCLUSION
This study demonstrates that subjective and quantitative assessment of baseline and postchemoradiation 18F-FDG PET provides statistical—but currently not clinically relevant—incremental value for predicting pathCR after preoperative chemoradiotherapy in esophageal cancer. The statistical discriminatory improvement beyond clinical predictors did not translate into a clinically relevant benefit that could change clinical decision making in terms of safely omitting surgery in predicted complete responders. This particular clinical dilemma demands a high predictive accuracy before clinical decision making can be influenced, warranting improvement, development, and validation of current and new imaging—or biomarkers.
DISCLOSURE
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734. Funding was provided in part by The University of Texas MD Anderson Cancer Center and by the National Cancer Institute Cancer Center support grant CA016672. No other potential conflict of interest relevant to this article was reported.
Footnotes
Published online Jan. 21, 2016.
- © 2016 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication July 13, 2015.
- Accepted for publication December 7, 2015.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- A Meta-Analysis for Using Radiomics to Predict Complete Pathological Response in Esophageal Cancer Patients Receiving Neoadjuvant Chemoradiation
- A Postreconstruction Harmonization Method for Multicenter Radiomic Studies in PET
- Predicting Response to Neoadjuvant Chemoradiotherapy in Esophageal Cancer with Textural Features Derived from Pretreatment 18F-FDG PET/CT Imaging