


Abstract
This study aimed to evaluate the long-term prognostic usefulness of 18F-FDG PET for patients with metastatic gastroenteropancreatic neuroendocrine tumors (GEPNETs). Methods: Thirty-eight patients with metastatic GEPNETs were prospectively enrolled. Initial check-up comprised CT scan, 111In-pentetreotide scintigraphy (SRS), and 18F-FDG PET. Only 18F-FDG PET–positive lesions with a maximum standardized uptake value (SUVmax) greater than 4.5 or an SUV ratio (SUVmax tumor to SUVmax nontumoral liver tissue, or T/NT ratio) of 2.5 or greater were considered positive for prognosis—that is, indicating a poor prognosis. Progression-free survival (PFS) and overall survival (OS) were estimated using the Kaplan–Meier method. Factors associated with survival were assessed with univariate and multivariate analyses, using the Cox regression model. Results: Median PFS and OS were significantly higher for patients with a negative 18F-FDG PET finding, with an OS of 119.5 mo (95% confidence interval [CI], 72–∞), than for patients with a positive 18F-FDG PET finding (only 15 mo [95% CI, 4–27]) (P < 10−3). Median PFS and OS were significantly higher for the patient group that had a positive SRS than the group with a negative SRS (P = 0.0002). For patients with a positive SRS, PFS and OS were significantly shorter when the 18F-FDG PET finding was positive: 19.5 mo (95% CI, 4–37) for PFS and 119.5 mo (95% CI, 81–∞) for OS (P < 10−3). In the patient group with a low-grade GEPNET and a positive SRS, PFS and OS were also significantly lower for patients with a positive 18F-FDG PET. At 48-mo follow-up, 100% of patients who had a positive 18F-FDG PET for disease progression (of which 47% were also SRS-positive) were deceased, and 87% of patients with a negative 18F-FDG PET were alive (P < 0.0001). The T/NT ratio was the only parameter associated with OS on multivariate analysis. Conclusion: Overall, 18F-FDG PET appears to be of major importance in the prognostic evaluation of metastatic GEPNET. A positive 18F-FDG PET with an SUV ratio (T/NT) of 2.5 or greater was a poor prognostic factor, with a 4-y survival rate of 0%. A positive SRS does not eliminate the need for performing 18F-FDG PET, which is of greater prognostic utility.
Gastroenteropancreatic neuroendocrine tumors (GEPNETs) are rare and form a heterogeneous group of tumors, with different progression profiles (1).
Different histoprognostic classifications (2–4) have been proposed, but determining the prognosis for neuroendocrine tumors (NETs) remains problematic even in the case of metastatic disease. These tumors are characterized by somatostatin receptor expression, which varies quantitatively and qualitatively from one tumor type to another (5).
It is now clearly known that functional imaging based on somatostatin receptor expression (111In- or 68Ga-radiolabeled analogs) has better diagnostic performance than 18F-FDG PET. It is also known that somatostatin receptor expression correlates with well-differentiated NET (6–8) and is a favorable prognostic factor (9–11).
In contrast, a positive 18F-FDG PET finding would correlate with a poorly differentiated NET and be a poor prognostic factor. But so far, only few studies have been performed on this subject (9,11,12). The main objective of our study, with preliminary findings already published (9), was to evaluate on a long-term basis the progression-free survival (PFS) and overall survival (OS) of metastatic GEPNET patients based on 18F-FDG PET and 111In-pentetreotide scintigraphy (SRS) results.
MATERIALS AND METHODS
In this prospective study, 38 patients with a histologically confirmed metastatic NET, mainly gastroenteropancreatic (n = 36), were enrolled from September 2003 to January 2006. The trial was approved by the ethics committee of our university hospital, and written informed consent was obtained from each patient. There were 24 men and 14 women (mean age ± SD, 60 ± 15 y).
The primary tumor site was known for 26 patients (pancreas, 9; midgut, 11; hindgut, 3; lung, 2; and gallbladder, 1). For the other 12 patients, the primary tumor site was unknown, but they had neuroendocrine hepatic metastases.
All of the patients had metastatic disease. The site of metastases was as follows: liver (n = 34 patients), lymph nodes (n = 15), peritoneum (n = 8), bone (n = 3), lungs (n = 1), central (n = 1), and ovaries (n = 1). The Ki67 index was available for 34 patients, established at less than 2% in 13 patients and greater than 15% in 7. Four tumors were classed as high-grade according to the World Health Organization (WHO) classification. Of the 34 low-grade tumors (WHO), 4 were classed grade 3 according to the European Neuroendocrine Tumor Society classification.
The study protocol, histologic diagnosis, and study population were detailed in a previously published article (9).
SRS and 18F-FDG PET were performed in a standard fashion (9). 18F-FDG uptake was quantified with the maximum standardized uptake value (SUVmax) and using the tumor-to-nontumor ratio (T/NT), calculated as the ratio of SUVmax tumor to SUVmax nontumoral liver. Poor prognosis was defined as patients with rapidly progressive disease—that is, with progressive disease at 6 mo (9), given that 6 mo is the typical timeframe used to discriminate rapidly progressive disease (requiring aggressive therapy) from nonrapidly progressive disease (requiring no aggressive therapy).
For prognostic evaluation, 18F-FDG PET was considered as positive (i.e., predictive of a poor prognosis) only for an SUVmax of 4.5 or greater or a T/NT ratio of 2.5 or greater.
Specific antitumor treatments, such as chemotherapy or chemoembolization, were initiated only when tumor progression was identified on a CT scan in accordance with Response Evaluation Criteria In Solid Tumors.
Statistical Analysis
Receiver-operating-characteristic (ROC) analysis was applied to determine the positive threshold for SUV (standardized uptake value) and T/NT ratio with respect to prognostic evaluation.
The factors associated with PFS and OS were analyzed on univariate and multivariate analyses using a forward Cox model (Wald method). The tested parameters consisted of T/NT ratio (<2.5 or ≥2.5), SUV (<4.5 or ≥4.5), SRS, histologic grade, and Ki67 index (<15% or ≥15%). For the multivariate analysis, neither SUV nor histologic grade was analyzed because T/NT ratio and SUV were linked variables, as were histologic grade and Ki67 index.
PFS and OS were estimated using the Kaplan–Meier method, and their comparison was based on log-rank test.
The statistical analyses were conducted using SPSS software (IBM). The significance level was set at 0.05.
RESULTS
The mean follow-up duration was 55.2 ± 37.9 mo, ranging from 1 to 119.2 mo. Only 1 patient was lost to follow-up, at 81 mo of follow-up. During the follow-up period, 27 patients (71%) exhibited disease progression, and 24 (63%) died.
18F-FDG PET and SRS positivity or negativity related to the histologic grade and Ki67 are presented, respectively, in Tables 1 and 2. 18F-FDG PET correlated with the histoprognostic grade (P = 0.01) and Ki67 (P < 10−3) whereas SRS results did not.
Results Using 111In-Octreotide Scintigraphy and 18F-FDG PET Scanning (n = 38 Patients)
Results of 18F-FDG PET and SRS Depending on Ki67 (n = 34 Patients)
The identified thresholds of positivity for prognosis were 4.5 for SUV (area under the ROC curve, 0.897) and 2.5 for T/NT ratio (area under the ROC curve, 0.920), (Fig. 1).
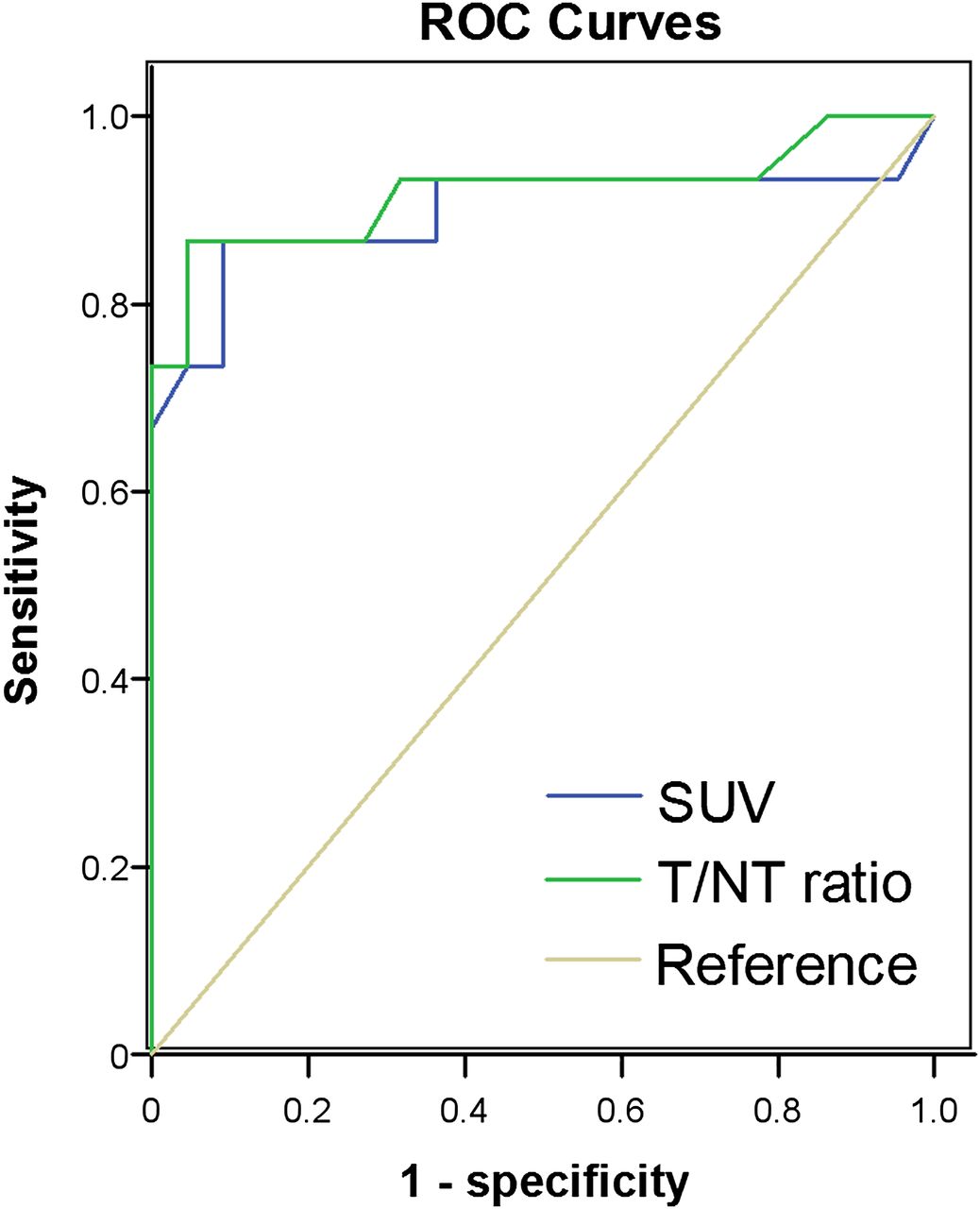
ROC curves for SUV and T/NT ratio for identification of poor prognosis (i.e., rapidly progressive disease).
Using univariate analysis, we found SUV, T/NT ratio, Ki67, and histologic grade to be significantly correlated to PFS and OS (Table 3). Yet at multivariate analysis, T/NT ratios were still found to highly significantly correlate with PFS and only T/NT ratio was still found to significantly (P < 0.0001; relative risk of death: 26.8) correlate with OS (Table 3).
Univariate and Multivariate Analysis (Cox Regression Model) of Factors Associated with PFS and OS
Fifteen patients (39%) had a positive 18F-FDG PET. PFS and OS were highly significantly better in the patient group with a negative 18F-FDG PET than in the patient group that had a positive 18F-FDG PET: respectively, 71 mo (IC 95%, 50 m–∞) versus 3 mo (IC 95%, 3–6 mo), P < 0.0001, for PFS, and 119.5 (IC 95%, 72 mo–∞) versus 15 mo (IC 95%, 4–27 mo) for OS, P < 0.0001 (Fig. 2).
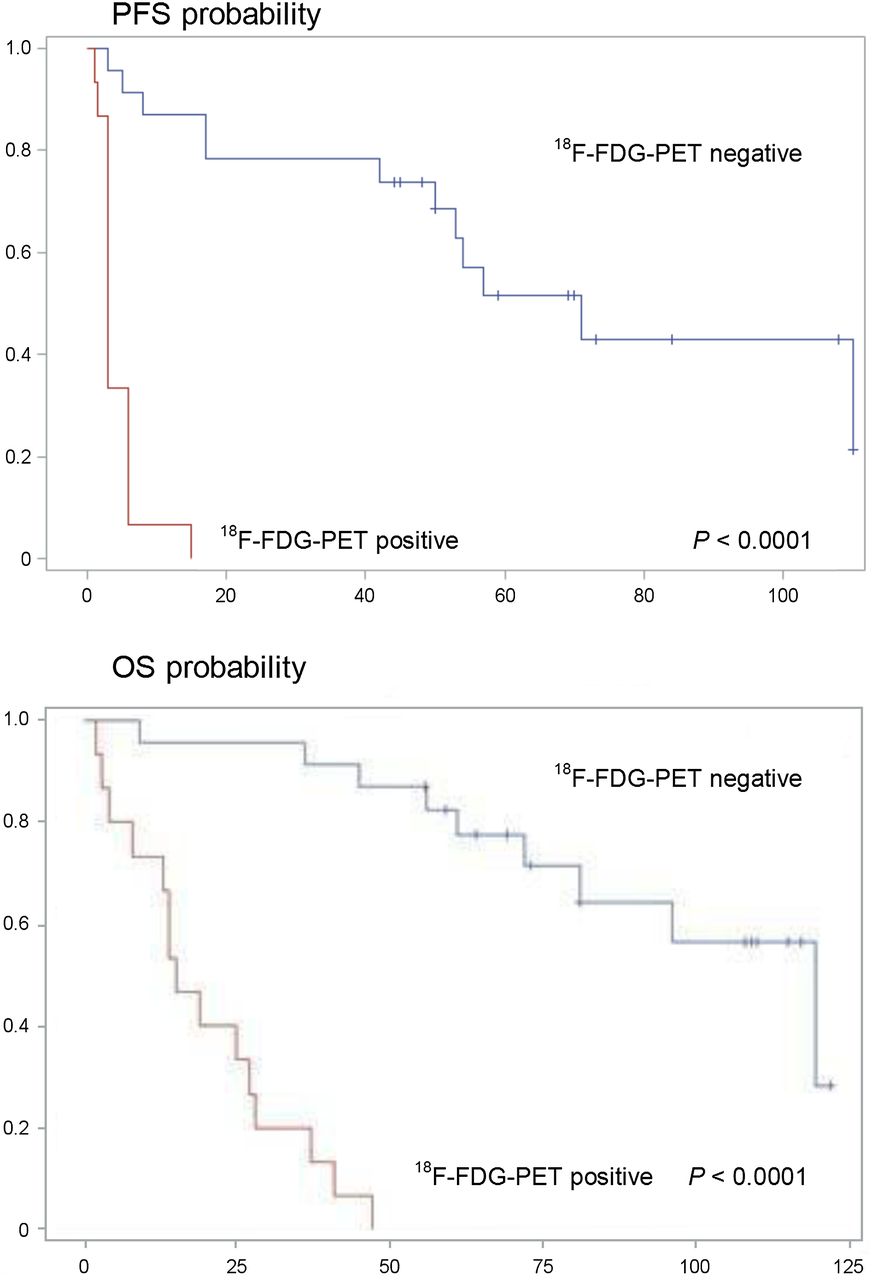
PFS and OS probabilities (time in mo) according to 18F-FDG PET.
We observed that 23 patients (61%) had a positive SRS. PFS and OS were significantly better in the patient group with a positive SRS than in the patient group that had a negative one: respectively, 54 mo (IC 95%, 8–110 mo) versus 3 mo (IC 95%, 1.5–6 mo) for PFS, P = 0.0002, and 96 mo (IC 95%, 47 mo–∞) versus 27 mo (IC 95%, 3–41 mo) for OS, P = 0.0002 (Fig. 3).

PFS and OS probabilities (time in mo) related to SRS.
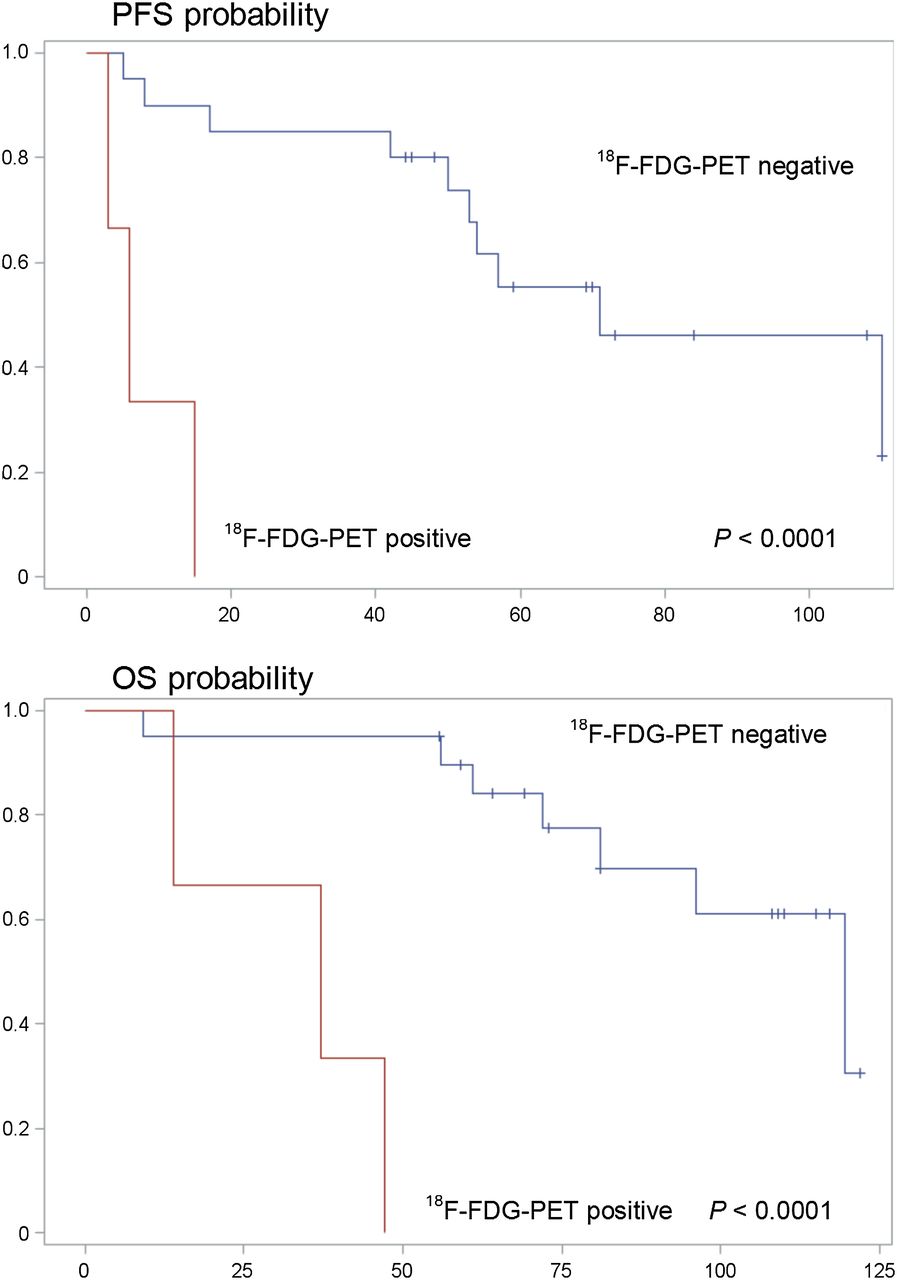
Twenty-nine percent of the patients with a positive SRS also had a positive 18F-FDG PET (i.e., 11 patients). For those patients, PFS and OS were highly significantly better in the patient group with a negative 18F-FDG PET than in the patient group that had a positive 18F-FDG PET: respectively, 71 mo (IC 95%, 50 mo–∞) versus 6 mo (IC 95%, 3–6 mo) for PFS, P < 0.0001, and 119.5 mo (IC 95%, 81 mo–∞) versus 19 m (IC 95%, 4–37 mo) for OS, P < 0.0001 (Fig. 4).

PFS and OS probabilities (time in mo) for SRS-positive patients related to 18F-FDG PET.
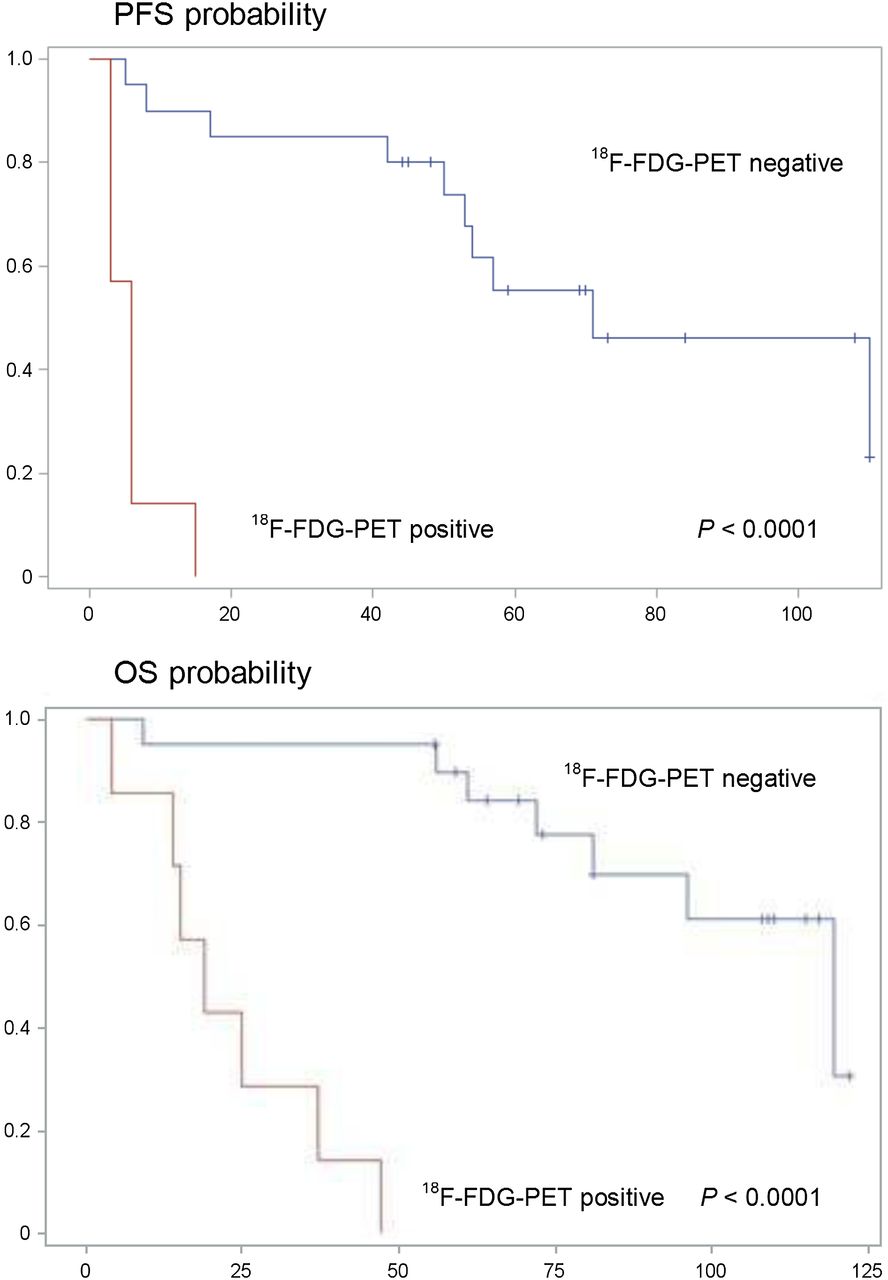
In the patient group with the best assumed prognostic profile—that is, patients with low-grade GEPNET (WHO/ENETS) and positive SRS—PFS and OS were highly significantly better in patients who had a negative 18F-FDG PET (of the patients of this group) than in patients who had a positive 18F-FDG PET (of the patients of this group): respectively, 71 mo (IC 95%, 50 mo–∞) versus 6 mo (IC 95%, 3–15 mo) for PFS, P < 0.0001, and 119.5 mo (IC 95%, 81 mo–∞) versus 37 mo (IC 95%, 14–47 mo) for OS, P < 0.0001 (Fig. 5).
PFS and OS probabilities (time in mo) for the group of patients with both SRS positivity and low grade.
Survival rates regarding 18F-FDG–negative and –positive patients were, respectively, 73% versus 95% (P < 0.0001) at 1 y, 40% versus 95% (P < 0.0001) at 2 y, 20% versus 91% (P < 0.0001) at 3 y, and 0% versus 87% (P < 0.0001) at 4 y.
Survival rates regarding SRS-negative and -positive patients were, respectively, 92% versus 72% (P = 0.0002) at 1 y, 81% versus 54% (P = 0.0002) at 2 y, 77% versus 27% (P = 0.0002) at 3 y, 70% versus 9% (P = 0.0002) at 4 y, and 57% versus 0% (P = 0.0002) at 6 y.
DISCUSSION
In this study, median PFS and OS were highly significantly better (P < 10–3) in the patient group with a negative 18F-FDG PET than in the group with a positive 18F-FDG PET (respectively, 119.5 and only 15 mo), whatever the results of other prognostic tools, including SRS and even Ki67 or histologic classification. To our knowledge, no other prospective study has performed a long-term prognostic evaluation in metastatic GEPNET patients, based on both 18F-FDG PET and SRS.
Indeed, Binderup et al. (12) evaluated survival in NET patients over only a short period (average follow-up, 11.5 mo). Median OS was not reached but the authors also found that a positive 18F-FDG PET with an SUVmax cutoff of 9 strongly correlated with a greater risk of mortality (hazard ratio, 0.8; 95% CI, 2.7–28.7; P < 0.001). In this study, a comparison with the SRS prognostic value was not performed.
A positive SRS has been reported to be factor of good prognosis (9,11,12). In our study, median PFS and OS were significantly better in the patient group that had a positive SRS than in the one exhibiting a negative SRS (P < 10−3), confirming the prognostic value of SRS. However, the prognostic value of SRS has been shown to be lower than that of 18F-FDG PET. We have, in fact, found that SRS was no longer correlated to OS when using multivariate analysis, as opposed to 18F-FDG PET.
For patients with both a positive SRS and a positive 18F-FDG PET, prognosis can be difficult to anticipate (because of the contradictory prognosis information provided by SRS and 18F-FDG PET). In this situation representing 18.2% of the global population and 25% of the positive SRS patients, our study clearly demonstrates for the first time that prognosis is related to the positivity of the 18F-FDG PET (poor prognosis), because median OS is only 17 mo when 18F-FDG PET is positive versus 119.5 mo when it is negative (P < 10−3).
Because SRS sensitivity for tumor detection is far better than 18F-FDG PET (6–8), most recommendations reserve 18F-FDG PET for cases in which SRS is negative, for high-grade tumors with a high proliferation index (Ki67), or for tumors shown to be rapidly progressing based on morphologic examinations (13–15).
However, in our results 25% of the patients with a positive SRS and 21% of the patients who had a tumor with a low proliferation index (Ki67 < 2%) also had a 18F-FDG PET–positive result and a poor prognosis. Binderup et al. (12) reported similar findings, namely 40% of patients who had a NET with a low proliferation index (Ki67 < 2%) had a positive 18F-FDG PET. These results are of great interest, suggesting that 18F-FDG PET is indicated in metastatic NETs, even in cases of low Ki67 index (i.e., <2%).
Elsewhere, the usefulness of SRS in known metastatic NETs remains a matter of debate. Given its lower prognostic impact than 18F-FDG PET, it should be performed solely if surgery or radiolabeled somatostatin analog therapy is proposed, and this is still the case for patients with a high Ki67 index, because 42% of our patients with a Ki67 index of 15% or greater also exhibited a positive SRS.
In the patient group having both a low-grade NET (WHO/ENETS) and a positive SRS (n = 23), 3 patients also had an 18F-FDG PET–positive finding. Here again, median PFS and OS were highly significantly lower when 18F-FDG PET was positive versus when it was negative (P < 10−3).
The coexistence in the same patient, or even in the same tumor, of well-differentiated and poorly or undifferentiated tumor clones (5) may explain why some NETs exhibit uptake of both 111In-pentetreotide and 18F-FDG. This coexistence would also explain the variability of tumor behavior and the sometimes fatal progression of certain patients with a NET who had wrongly been classed as of low risk.
Thus, in the case of metastatic NETs, 18F-FDG PET should be more widely used for prognostic evaluation.
The prognostic impact of 18F-FDG PET is confirmed by the long-term evaluation with an overall 4-y survival rate of 0% in the patient group that had a positive 18F-FDG PET, compared with 87% in the group that had a negative 18F-FDG PET. On the basis of this finding, 18F-FDG PET appears to be of dramatic prognostic value. This point is of major interest because aggressive therapeutic approaches including chemotherapy, radiolabeled somatostatin analog internal radiation therapy (for SRS-positive patients), liver radioembolization (especially for PET-positive and SRS-negative patients), or targeted therapy can be proposed to patients with poor prognosis.
The main drawback of this study is a relatively small number of patients and heterogeneity of the population (NETs of different origin), but these drawbacks are almost always the case in others’ published data on PET and NETs. The interesting result observed in this prospective study—the highly significant dramatic prognostic impact of 18F-FDG PET in metastatic patients—should be validated in a larger multicentric trial. The prognostic value of 18F-FDG PET has also to be evaluated in nonmetastatic patients.
CONCLUSION
Our study results clearly demonstrate the usefulness of 18F-FDG PET for metastatic GEPNET. A positive SRS does not eliminate the need for an 18F-FDG PET, because 18F-FDG PET is of greater prognostic value even when SRS is positive or in some cases of low-grade lesions.
Early prognostic assessment of these tumors could be used for the selection of patients requiring aggressive treatment. The prognostic value of 18F-FDG PET in nonmetastatic patients has also to be evaluated because it was not evaluated in this study.
DISCLOSURE
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734. No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Oct. 6, 2014.
- © 2014 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication June 17, 2014.
- Accepted for publication August 12, 2014.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- [18F]FDG and [68Ga]Ga-FAPI-04-Directed Imaging for Outcome Prediction in Patients with High-Grade Neuroendocrine Neoplasms
- Dual Somatostatin Receptor/18F-FDG PET/CT Imaging in Patients with Well-Differentiated, Grade 2 and 3 Gastroenteropancreatic Neuroendocrine Tumors
- [18F]FDG PET/CT-Avid Discordant Volume as a Biomarker in Patients with Gastroenteropancreatic Neuroendocrine Neoplasms: A Multicenter Study
- High Tumor Uptake on 18F-FDOPA PET/CT Indicates Poor Prognosis in Patients with Metastatic Midgut Neuroendocrine Tumors: A Study from the Groupe detude des Tumeurs Endocrines and ENDOCAN-RENATEN Network
- Somatostatin Receptor Imaging and Theranostics: Current Practice and Future Prospects
- 18F-FDG PET is Superior to WHO Grading as a Prognostic Tool in Neuroendocrine Neoplasms and Useful in Guiding PRRT: A Prospective 10-Year Follow-up Study
- Efficacy of FOLFOX Chemotherapy in Metastatic Enteropancreatic Neuroendocrine Tumors
- Evaluating the Role of Theranostics in Grade 3 Neuroendocrine Neoplasms
- The thymidine dideoxynucleoside analog, alovudine, inhibits the mitochondrial DNA polymerase {gamma}, impairs oxidative phosphorylation and promotes monocytic differentiation in acute myeloid leukemia
- Clinical Usefulness of 18F-Fluorodeoxyglucose Positron Emission Tomography in the Diagnostic Algorithm of Advanced Entero-Pancreatic Neuroendocrine Neoplasms
- Current Concepts in 68Ga-DOTATATE Imaging of Neuroendocrine Neoplasms: Interpretation, Biodistribution, Dosimetry, and Molecular Strategies
- The Antiproliferative Role of Lanreotide in Controlling Growth of Neuroendocrine Tumors: A Systematic Review
- Comparison of the Impact of 68Ga-DOTATATE and 18F-FDG PET/CT on Clinical Management in Patients with Neuroendocrine Tumors
- Molecular Imaging of Gastroenteropancreatic Neuroendocrine Tumors: Current Status and Future Directions
- Prognostic Value of FDG-PET/CT Total Lesion Glycolysis for Patients with Resectable Distal Bile Duct Adenocarcinoma
- Prognostic Value of 68Ga-DOTANOC PET/CT SUVmax in Patients with Neuroendocrine Tumors of the Pancreas
- Modifying the Poor Prognosis Associated with 18F-FDG-Avid NET with Peptide Receptor Chemo-Radionuclide Therapy (PRCRT)
- Reply: Modifying the Poor Prognosis Associated with 18F-FDG-Avid NET with Peptide Receptor Chemo-Radionuclide Therapy (PRCRT)