


Abstract
68Ga-DOTATOC and 68Ga-DOTATATE are 2 radiolabeled somatostatin analogs for in vivo diagnosis of neuroendocrine tumors with PET. The aim of the present work was to measure their comparative biodistribution and radiation dosimetry. Methods: Ten patients diagnosed with neuroendocrine tumors were included. Each patient underwent a 45-min dynamic and 3 whole-body PET/CT scans at 1, 2, and 3 h after injection of each tracer on consecutive days. Absorbed doses were calculated using OLINDA/EXM 1.1. Results: Data from 9 patients could be included in the analysis. Of the major organs, the highest uptake at 1, 2, and 3 h after injection was observed in the spleen, followed by kidneys and liver. For both tracers, the highest absorbed organ doses were seen in the spleen and urinary bladder wall, followed by kidney, adrenals, and liver. The absorbed doses to the liver and gallbladder wall were slightly but significantly higher for 68Ga-DOTATATE. The total effective dose was 0.021 ± 0.003 mSv/MBq for both tracers. Conclusion: The effective dose for a typical 100-MBq administration of 68Ga-DOTATATE and 68Ga-DOTATOC is 2.1 mSv for both tracers. Therefore, from a radiation dosimetry point of view, there is no preference for either tracer for PET/CT evaluation of somatostatin receptor–expressing tumors.
Neuroendocrine tumors can be diagnosed in vivo using PET with the radiolabeled somatostatin analogs 68Ga-DOTATOC and 68Ga-DOTATATE (1,2). Although the dosimetry of both tracers has been described separately (3,4) and has shown comparable effective doses, a comparative study using an identical, standardized methodology in a single group of patients has not been published and is of interest for tracer selection from a radiation dosimetry point of view. An earlier study did compare the biodistribution and radiation dosimetry of 111In-labeled DOTATOC and DOTATATE (5) as estimated using whole-body scintigraphy. In that study, the main focus was to compare the 2 peptides with reference to their use in targeted peptide radiotherapy, mainly using 111In as an analog for the therapeutic peptides 177Lu-DOTATATE and 90Y-DOTATOC. Similarly, DOTATOC labeled with the positron-emitting isotope 86Y has been suggested as an analog of 90Y-DOTATOC (6), but the complex decay scheme of 86Y (7) makes it unfavorable as a diagnostic tracer. In contrast, the 68Ga-labeled peptides will likely be used mainly for diagnosis and assessment of eligibility for somatostatin analog therapy. The diagnostic yield of the 2 tracers has been compared in 40 patients who underwent PET with both (2). In that study, tumor uptake of 68Ga-DOTATOC was higher than that of 68Ga-DOTATATE. Tumor detection was similar for the 2 tracers in a region-based analysis, but overall, significantly more lesions were found by 68Ga-DOTATOC PET/CT. The aim of the present work was to use dynamic and serial whole-body PET/CT to measure the biodistribution and estimate the radiation dosimetry of 68Ga-DOTATOC and 68Ga-DOTATATE in a single group of patients.
MATERIALS AND METHODS
Patients
Ten patients (mean age, 62 y; range, 44–75 y; 6 men and 4 women) diagnosed with disseminated neuroendocrine tumors as confirmed by histopathology were included. Three of the patients had pancreatic neuroendocrine tumors, 5 had small-intestinal neuroendocrine tumors, and 2 had lung carcinoids. All patients signed a written informed consent form before inclusion, and the study was approved by the Regional Medical Ethics Board.
Tracer Production and Quality Control
Sodium acetate buffer (pH 4.6), sodium hydroxide (10 M), and doubly distilled hydrochloric acid (Riedel de Haën) were obtained from Sigma-Aldrich Sweden. Trifluoroacetic acid was obtained from Merck. The purchased chemicals were used without further purification. Commercially available DOTATOC and DOTATATE (Eurogentec S.A.) were dissolved in sterile water to give a 1 mM solution. 68Ga (half-life, 68 min; β+ decay, 89%; electron capture, 11%) was eluted with 0.6 M HCl from a 68Ge/68Ga-generator (1,850 MBq; IDB Holland BV), where 68Ge (half-life, 270.8 d) was attached to a column of an inorganic matrix based on tin dioxide. Production and quality control of the tracers were compliant with good manufacturing practices and were accomplished within 1 h. The fractionation method was used for the labeling (8). The first 1.0-mL fraction was sent to the waste, and the next 1.0 mL, containing over 65% of the total radioactivity, was collected and buffered with 200 μL of acetate buffer and 60 μL of sodium hydroxide to provide a pH of 4.6 ± 0.4. Radioactivity was measured, and 200–300 MBq were taken for the labeling synthesis. Thirty nanomoles of either DOTATOC or DOTATATE were added, and the reaction mixture was heated at 90°C–95°C for 10 min. The crude 68Ga-DOTATOC and 68Ga-DOTATATE were purified using a C8 (Sep-Pak Light; Waters) reversed solid-phase extraction cartridge. The product was eluted with 0.5 mL of 90% ethanol and formulated with sterile phosphate buffer (pH 7.4), and the resulting solution was passed through a 0.22-μm filter into a sterile injection vial. A sample was taken for determination of identity, radiochemical purity, chemical purity, and pH; for estimation of the peptide content, and for control of sterility and endotoxins.
PET Protocol
PET data were acquired using a Discovery ST (GE Healthcare) PET/CT scanner with an axial field of view of 15.7 cm. After a low-dose CT scan for patient positioning and attenuation correction, a 45-min dynamic PET scan (6 × 10, 4 × 60, 5 × 180, 5 × 300 s) over the abdominal region, including the liver, spleen, adrenals, and kidneys, was started simultaneously with the injection of either 91.4 ± 18.7 MBq (range, 72–120 MBq) of 68Ga-DOTATATE or 86.9 ± 16.4 MBq (range, 62–112 MBq) of 68Ga-DOTATOC. Three whole-body scans followed (proximal femur to base of skull), starting at 1, 2, and 3 h after injection, with scan durations of 3, 4, and 5 min per bed position, respectively, each preceded by a low-dose CT examination. Images were reconstructed using normalization and attenuation-weighted ordered-subsets expectation maximization (2 iterations, 21 subsets), including corrections for dead time, random coincidences as estimated by singles counting rates, model-based scatter correction (9), attenuation based on a bilinear conversion of Hounsfield units to 511-keV attenuation coefficients, and decay. A 5.4-mm gaussian postprocessing filter was applied. Venous blood samples were drawn after each whole-body scan for measurement of whole-blood radioactivity concentrations. Patients were allowed to urinate between the dynamic scan and each consecutive whole-body examination. Urine was collected and weighed, and radioactivity concentration was measured. Accurate cross-calibration between the PET/CT scanner, the dose calibrator, and the well counters that were used to measure blood and urine activity was verified monthly and was always within 3%. The scan was repeated on the next day with the other tracer. The patients were randomized regarding the order of tracer used on the 2 consecutive examination days.
Volumes of Interest (VOIs)
VOIs were drawn at the same locations on the whole-body images and on the last time frame of the dynamic image series over clearly tumor-free subsets of all clearly identifiable source organs: liver, kidneys, spleen, lungs, small intestine, and adrenal glands. VOIs drawn on the last frame of the dynamic scans were transferred to all earlier time frames. Activity concentration and standardized uptake value (SUV) normalized to body mass and injected amount of radioactivity were determined using the mean activity concentration in VOIs. For adrenal glands, SUV was based on maximum pixel values because of their small volume and corresponding limited recovery.
For measurement of blood radioactivity concentrations during the dynamic scan, 1-cm-diameter circular regions of interest were drawn on 10 consecutive image planes over the descending aorta in the time frame where the first pass of the activity was best visualized and were combined to a single VOI. This VOI was then transferred to all other time frames in the dynamic scan and combined with blood samples collected at later time points to obtain a whole-blood time–activity curve.
Absorbed Dose Calculations
Red marrow radioactivity concentration was assumed to be equal to blood radioactivity concentration (10). Total organ activity was calculated by multiplying the radioactivity concentrations by the organ weights of the adult reference male or female phantom (11). Time-integrated activity in each organ was calculated by trapezoidal integration of the first 45 min of the organ’s time–activity curve, followed by a single-exponential fit to the remaining data points (based on the 3 whole-body images) extrapolated to infinity, all based on non–decay-corrected data. For estimation of urinary bladder contents, all urine measurements were decay-corrected to the time of injection. Then, the bladder content at intermediate time points was estimated assuming linear filling of the bladder until each complete voiding. After the last scan, a 4-h voiding interval with filling rates equivalent to those before the last measured urine sample was assumed. This urinary bladder content time–activity curve was then uncorrected for decay, and time-integrated activity was calculated as the area under this time–activity curve. Residence times were obtained by dividing the time-integrated activity by the injected amount of activity. Small intestine, upper large intestine, and lower large intestine residence times were estimated using the ICRP 30 gastrointestinal tract model (12). Remainder-of-body activity was calculated as the injected activity minus the sum of the activity in all source organs and the activity excreted to urine up to each measurement point. Absorbed doses were calculated using OLINDA/EXM 1.1 (13).
Statistical Analysis
Differences between residence times and absorbed doses for both tracers were assessed using a Wilcoxon matched-pairs signed rank test. Differences between absorbed doses in male and female subjects were assessed using a Mann–Whitney test. A P value below 0.05 was considered significant. No multiple-comparisons correction was applied.
RESULTS
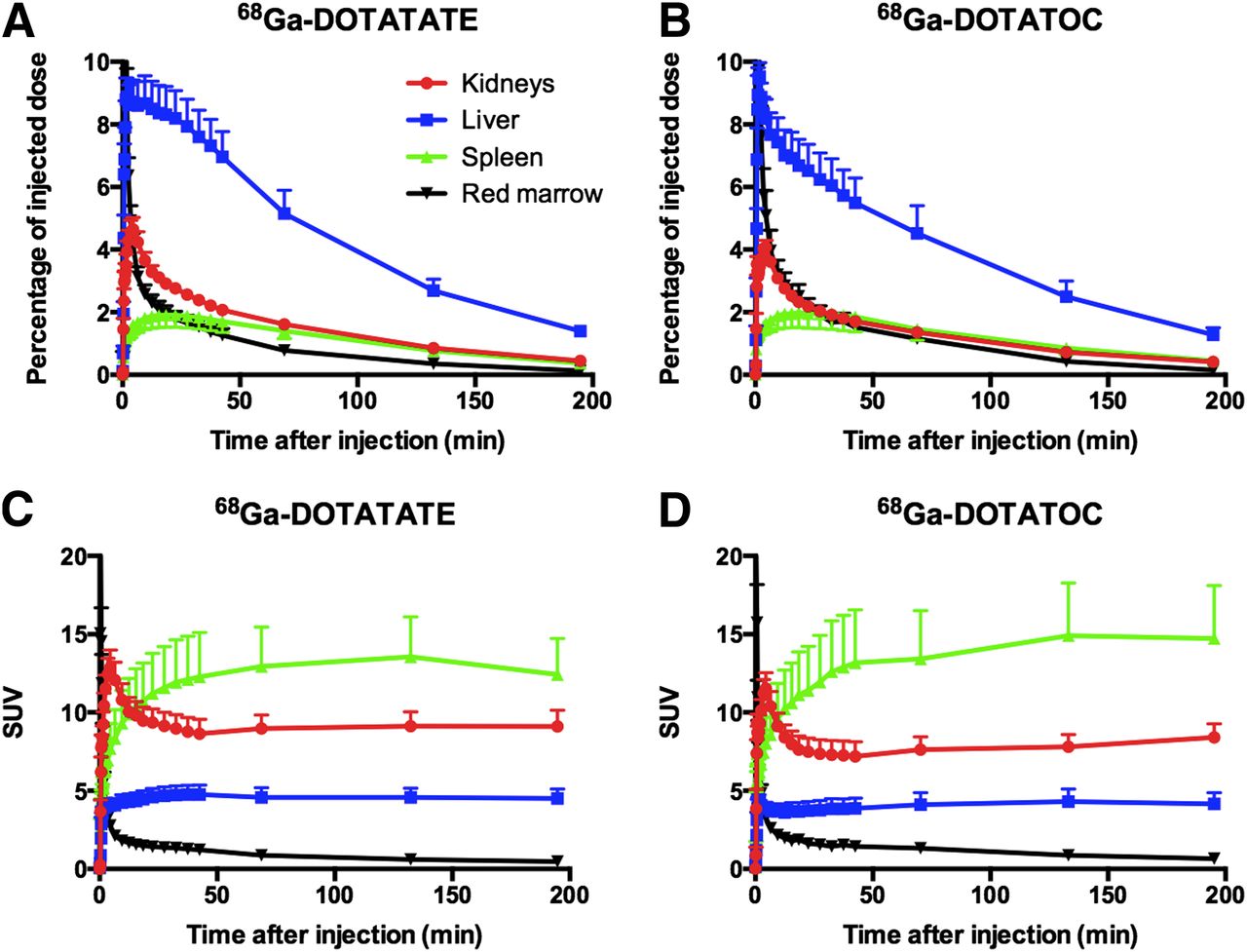
One patient (female) had to be excluded from analysis because of atypical biodistribution caused by a horseshoe kidney. Figure 1 shows typical whole-body images for both tracers. Figure 2 shows the biodistribution, in terms of SUV and percentage injected activity per organ, for 68Ga-DOTATOC and 68Ga-DOTATATE. Of the major organs, the highest SUV at 60–180 min after injection was observed in the spleen, followed by kidneys and liver. Clearance from the liver and kidney was slightly faster for 68Ga-DOTATOC, resulting in a lower residence time in the liver (P < 0.05), whereas blood clearance was faster for 68Ga-DOTATATE. Residence times, as shown in Table 1, were highest for the liver, followed by kidney, spleen, and urinary bladder contents.
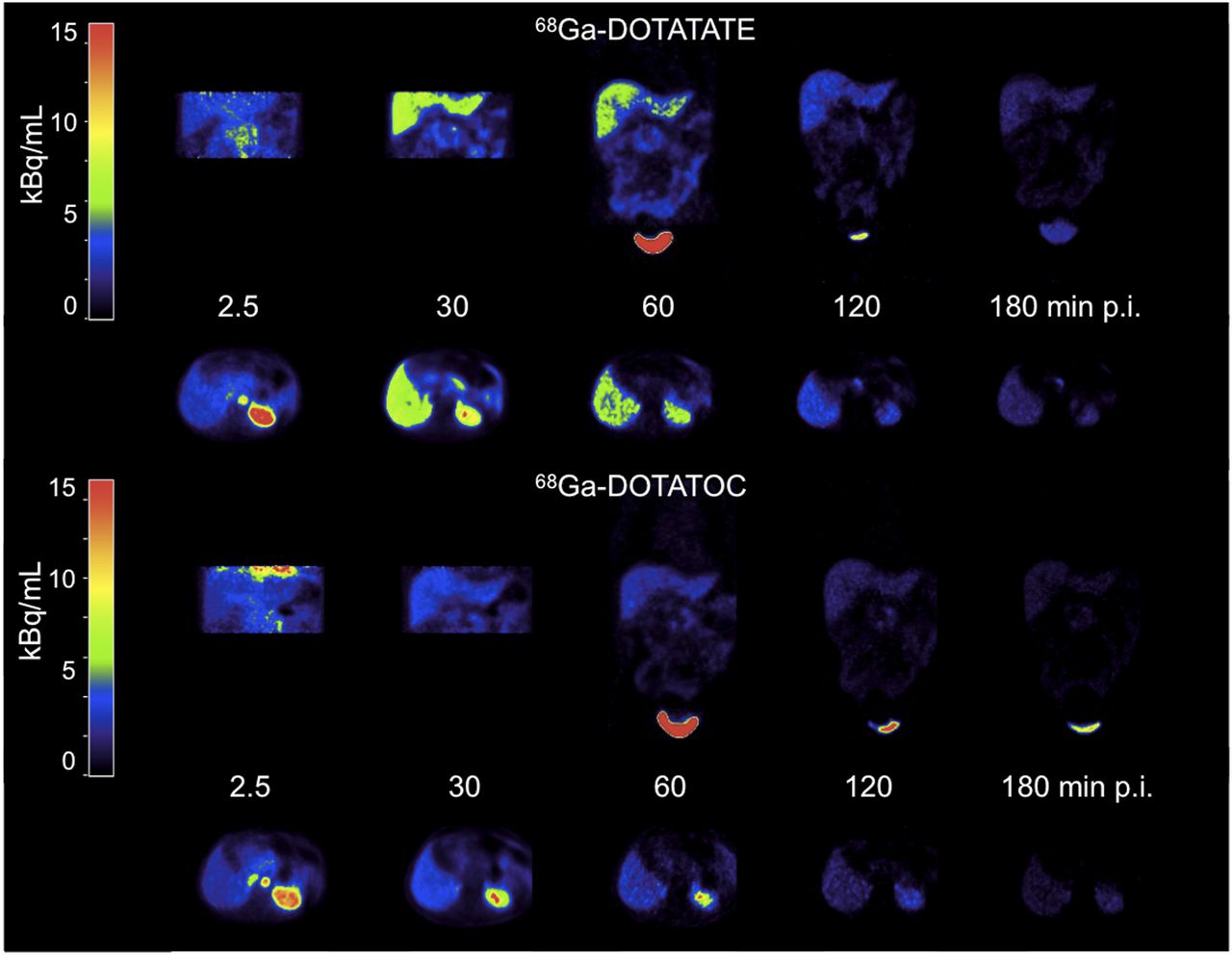
Representative images (not decay-corrected) at 0–5, 30, 60, 120, and 180 min after injection of 103 MBq of 68Ga-DOTATATE and 100 MBq of 68Ga-DOTATOC in same patient (patient with highest 68Ga-DOTATATE liver residence time in Fig. 4) on 2 consecutive days. For both tracers, upper row is coronal slices and lower row is transversal slices.
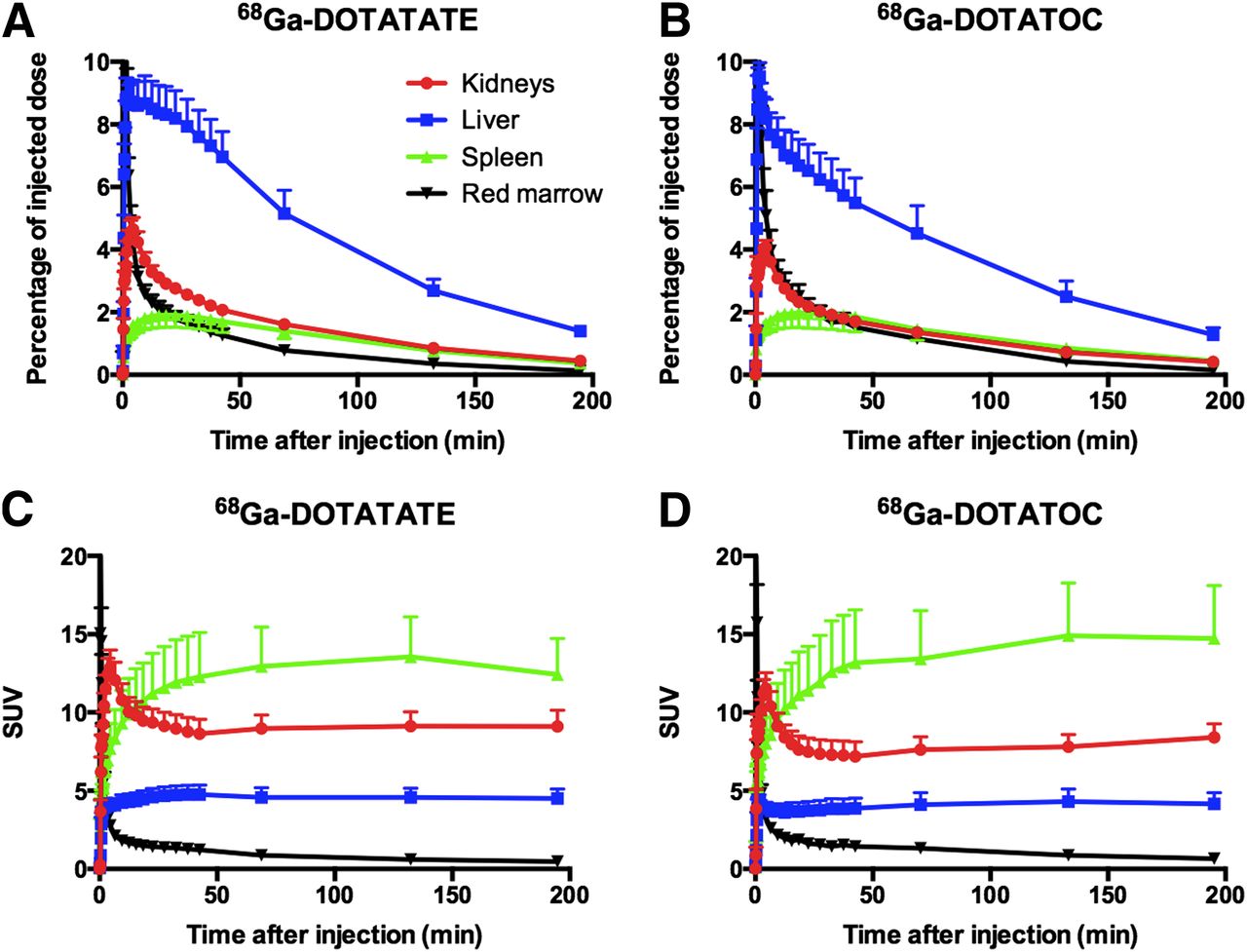
Percentage of injected activity (A and B) and SUV (C and D) as function of time after injection in kidneys, liver, spleen, and red marrow for 68Ga-DOTATATE (A and C) and 68Ga-DOTATOC (B and D). Error bars indicate SEs. SUV data were corrected for radioactive decay; percentage of injected dose data were not. Red marrow SUV is identical to whole-blood SUV.
Residence Times (h) (n = 9)
During the first 4 h after injection, 15.6% (SD, 9.2) and 11.9% (SD, 4.1) of injected activity were excreted to urine for 68Ga-DOTATOC and 68Ga-DOTATATE, respectively. These percentages are in agreement with the slightly faster kidney clearance seen for 68Ga-DOTATOC. However, there was no significant difference between excreted fractions.
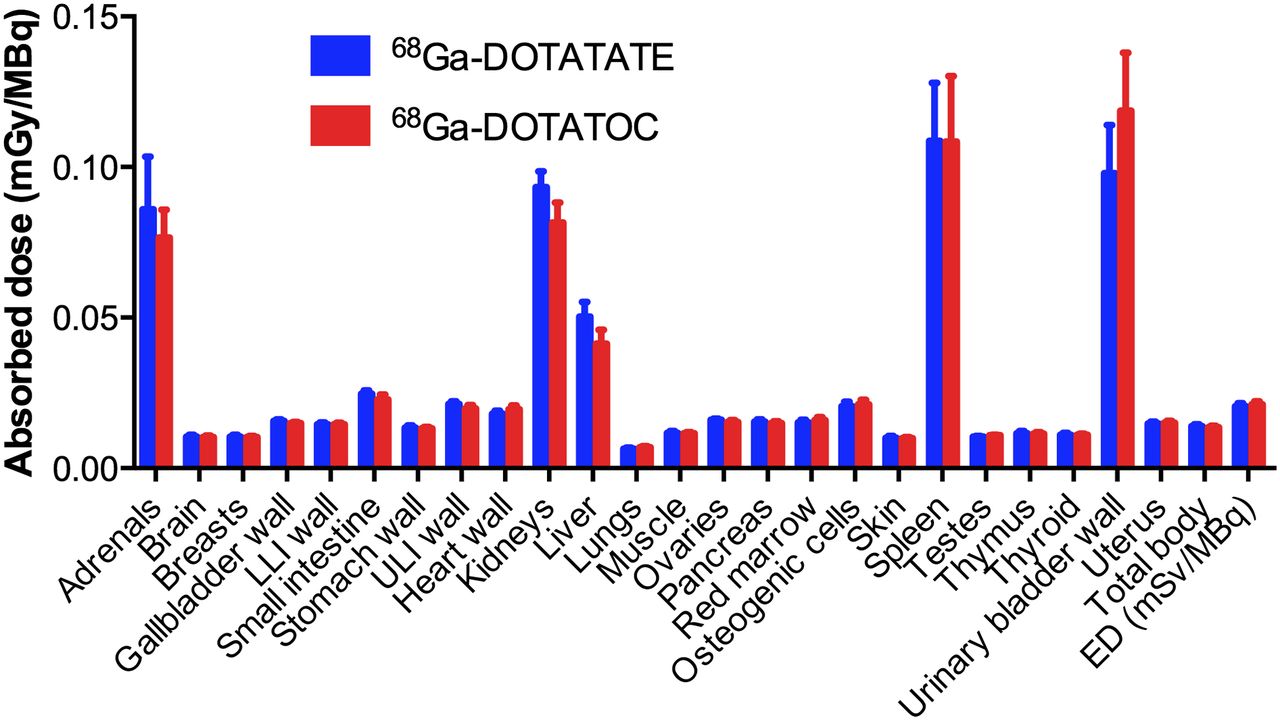
Absorbed dose estimates are shown in Figure 3 and, for selected organs, in Table 2. The highest absorbed organ doses were seen in the spleen and urinary bladder wall, followed by the kidney, adrenals, and liver, for both tracers. Figure 4 compares residence times and absorbed doses in kidney and liver, as well as effective dose, for each individual patient. The total effective dose was 0.021 mSv/MBq for both tracers. When men and women were analyzed separately, effective doses of 68Ga-DOTATATE and 68Ga-DOTATOC were 0.020 and 0.020 mSv/MBq, respectively, for men and 0.022 and 0.023 mSv/MBq, respectively, for women (P = 0.30 and P = 0.26 for 68Ga-DOTATATE and 68Ga-DOTATOC, respectively). These values would result in an effective dose of 2.1 mSv for the typical 100-MBq amount administered in the present work. Absorbed doses to the liver, gallbladder wall, and total body were significantly higher for 68Ga-DOTATATE (Wilcoxon matched-pairs signed rank test, P < 0.05, with higher absorbed doses for 68Ga-DOTATATE in 7 of 9 and 8 of 9 patients, respectively), although absolute differences were small for the gallbladder wall (3%) and total body (1%).

Absorbed doses in all organs included in OLINDA/EXM 1.1. Error bars indicate SEs. LLI = lower large intestine; ULI = upper large intestine; ED = effective dose.
Absorbed Doses (mGy/MBq) in Selected Organs (n = 9)

(A and B) Residence times (A) and absorbed doses (B) in kidney and liver. (C) Effective dose for 68Ga-DOTATATE and 68Ga-DOTATOC. Solid line in each panel is line of identity.
DISCUSSION
To our knowledge, the present work is the first comparative study of the radiation dosimetry of 68Ga-DOTATOC and 68Ga-DOTATATE in a single group of patients. Radiation-absorbed doses were estimated using a protocol combining dynamic PET and serial whole-body PET scans in 9 patients. For both tracers, an effective dose of 2.1 mSv for a typical 100-MBq administration was found, with the only significant, although minor, difference in organ doses being seen for the liver and gallbladder wall. Residence times and absorbed doses in the kidney and liver were higher for 68Ga-DOTATATE in 7 of 9 patients. The opposite was observed for effective dose, although differences in the effective dose of both tracers were minor even within individual patients (Fig. 4). The organ receiving the highest absorbed dose was the spleen for 68Ga-DOTATATE and the urinary bladder wall for 68Ga-DOTATOC. In both cases, the mean absorbed dose to these organs was about 20% of the maximum allowed dose of 50 mGy to a single organ in an adult research subject (14).
As can be seen in Figures 2 and 3, SUVs in the liver, kidney, and spleen are approximately constant starting at about 1 h after injection. Exponential fits to the last 3 measured data points resulted in effective half-lives slightly longer than the physical half-life of 68Ga (∼70 min and 75 min in liver and kidney for 68Ga-DOTATATE and 68Ga-DOTATOC, respectively). Since the scan protocol covered the major part of the radioactive decay of 68Ga, the remaining decays after the last scan amount to at most a small percentage of the total number of disintegrations in each organ. Therefore, uncertainty in extrapolation after the 3-h whole-body scan only has minor effects on the total estimate of the time-integrated activity.
The patients included in the present work all had disseminated neuroendocrine tumor disease, mainly in the liver, mesenterically and retroperitoneally. Although we selected patients with limited tumor burden, that is, without bulky disease, uptake in tumors may have resulted in somewhat decreased availability of tracer for uptake into normal tissues. Tumor tissue is not explicitly accounted for when OLINDA/EXM 1.1 is used to assess radiation dosimetry, but activity in tumor tissue is included in the analysis as part of the remainder of the body.
Forrer et al. (5) compared the radiation dosimetry of 111In-labeled DOTATOC and DOTATATE in a single patient group using planar whole-body scintigraphy and found results comparable to those in the present work, with higher kidney and liver doses for 111In-DOTATATE and higher urinary excretion for 111In-DOTATOC. Hartmann et al. (3) studied the radiation dosimetry of 68Ga-DOTATOC in 14 patients and found a slightly higher effective dose of 0.023 mSv/MBq, with the spleen and kidney receiving much higher absorbed doses than in the present work (0.24 and 0.22 mGy/MBq in the study of Hartmann et al., compared with 0.11 and 0.08 mGy/MBq in our work), using a scanning protocol with sparser sampling requiring extrapolation over a larger fraction of the total decay of the tracer. The higher absorbed doses in the spleen and kidney correspond to proportionally higher SUVs in those organs in their work than in the present work. Walker et al. (4) evaluated the radiation dosimetry of 68Ga-DOTATATE in merely 3 patients, using only whole-body scans at 30, 60, and 90 min after injection, and although the relative distribution of residence times and absorbed doses across organs was similar to the present study, they reported overall slightly higher organ doses and a higher effective dose (0.025 mSv/MBq) than in the present work. This difference may be caused by the extrapolation required for the first 30 min after injection and the shorter duration of their protocol compared with ours, necessitating extrapolation over a larger fraction of the total decay of the tracer as well. For comparison, Pettinato et al. found a somewhat lower effective dose of 0.017 mSv/MBq for 68Ga-DOTANOC (15), a third somatostatin analog that has been suggested because of its highest combined affinity to different somatostatin receptor subtypes (1).
CONCLUSION
The effective dose for a typical 100-MBq administration of 68Ga-DOTATATE and 68Ga-DOTATOC is 2.1 mSv for both tracers, with only minor differences in doses to individual organs. Therefore, there is no preference for either tracer in the diagnoses and pretreatment evaluation of somatostatin receptor–expressing tumors in terms of radiation doses.
DISCLOSURE
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734. Financial support was provided by Uppsala University Hospital and by the Swedish Cancer Society (grant CAN2011/580). No other potential conflict of interest relevant to this article was reported.
Acknowledgments
We thank Mimmi Lidholm, Annie Bjurebäck, Maj Wiberg, Lars Lindsjö, and Marie Åhlman for their technical assistance in performing the scans.
Footnotes
Published online Aug. 8, 2013.
- © 2013 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication January 28, 2013.
- Accepted for publication May 2, 2013.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Safety, Biodistribution, and Radiation Dosimetry of the 68Ga-Labeled Minigastrin Analog DOTA-MGS5 in Patients with Advanced Medullary Thyroid Cancer and Other Neuroendocrine Tumors
- Biodistribution, Dosimetry, and Pharmacokinetics of 68Ga-CBP8: A Type I Collagen-Targeted PET Probe
- Prospective Phase II Trial of [68Ga]Ga-NODAGA-E[c(RGDyK)]2 PET/CT Imaging of Integrin {alpha}v{beta}3 for Prognostication in Patients with Neuroendocrine Neoplasms
- FAPI-74 PET/CT Using Either 18F-AlF or Cold-Kit 68Ga Labeling: Biodistribution, Radiation Dosimetry, and Tumor Delineation in Lung Cancer Patients
- Radiation Dosimetry and Biodistribution of 68Ga-FAPI-46 PET Imaging in Cancer Patients
- Improving Contrast and Detectability: Imaging with [55Co]Co-DOTATATE in Comparison with [64Cu]Cu-DOTATATE and [68Ga]Ga-DOTATATE
- PET-Based Human Dosimetry of 68Ga-NODAGA-Exendin-4, a Tracer for {beta}-Cell Imaging
- 68Ga-FAPI PET/CT: Biodistribution and Preliminary Dosimetry Estimate of 2 DOTA-Containing FAP-Targeting Agents in Patients with Various Cancers
- Comparative Dosimetry for 68Ga-DOTATATE: Impact of Using Updated ICRP Phantoms, S Values, and Tissue-Weighting Factors
- Safety, Biodistribution, and Radiation Dosimetry of 68Ga-OPS202 in Patients with Gastroenteropancreatic Neuroendocrine Tumors: A Prospective Phase I Imaging Study
- Current Concepts in 68Ga-DOTATATE Imaging of Neuroendocrine Neoplasms: Interpretation, Biodistribution, Dosimetry, and Molecular Strategies
- Parametric Net Influx Rate Images of 68Ga-DOTATOC and 68Ga-DOTATATE: Quantitative Accuracy and Improved Image Contrast
- Safety, Dosimetry, and Tumor Detection Ability of 68Ga-NOTA-AE105: First-in-Human Study of a Novel Radioligand for uPAR PET Imaging
- Molecular Imaging of Gastroenteropancreatic Neuroendocrine Tumors: Current Status and Future Directions
- Phase I Study of 68Ga-HER2-Nanobody for PET/CT Assessment of HER2 Expression in Breast Carcinoma
- Radiation Dosimetry of the Fibrin-Binding Probe 64Cu-FBP8 and Its Feasibility for PET Imaging of Deep Vein Thrombosis and Pulmonary Embolism in Rats
- Biodistribution and Radiation Dosimetry for a Probe Targeting Prostate-Specific Membrane Antigen for Imaging and Therapy
- 64Cu-DOTATATE PET for Neuroendocrine Tumors: A Prospective Head-to-Head Comparison with 111In-DTPA-Octreotide in 112 Patients
- Biodistribution and Radiation Dosimetry for the Chemokine Receptor CXCR4-Targeting Probe 68Ga-Pentixafor
- Quantitative and Qualitative Intrapatient Comparison of 68Ga-DOTATOC and 68Ga-DOTATATE: Net Uptake Rate for Accurate Quantification