


Abstract
The overexpression of urokinase-type plasminogen activator receptors (uPARs) represents an established biomarker for aggressiveness in most common malignant diseases, including breast cancer (BC), prostate cancer (PC), and urinary bladder cancer (UBC), and is therefore an important target for new cancer therapeutic and diagnostic strategies. In this study, uPAR PET imaging using a 68Ga-labeled version of the uPAR-targeting peptide (AE105) was investigated in a group of patients with BC, PC, and UBC. The aim of this first-in-human, phase I clinical trial was to investigate the safety and biodistribution in normal tissues and uptake in tumor lesions. Methods: Ten patients (6 PC, 2 BC, and 2 UBC) received a single intravenous dose of 68Ga-NOTA-AE105 (154 ± 59 MBq; range, 48–208 MBq). The biodistribution and radiation dosimetry were assessed by serial whole-body PET/CT scans (10 min, 1 h, and 2 h after injection). Safety assessment included measurements of vital signs with regular intervals during the imaging sessions and laboratory blood screening tests performed before and after injection. In a subgroup of patients, the in vivo stability of 68Ga-NOTA-AE105 was determined in collected blood and urine. PET images were visually analyzed for visible tumor uptake of 68Ga-NOTA-AE105, and SUVs were obtained from tumor lesions by manually drawing volumes of interest in the malignant tissue. Results: No adverse events or clinically detectable pharmacologic effects were found. The radioligand exhibited good in vivo stability and fast clearance from tissue compartments primarily by renal excretion. The effective dose was 0.015 mSv/MBq, leading to a radiation burden of 3 mSv when the clinical target dose of 200 MBq was used. In addition, radioligand accumulation was seen in primary tumor lesions as well as in metastases. Conclusion: This first-in-human, phase I clinical trial demonstrates the safe use and clinical potential of 68Ga-NOTA-AE105 as a new radioligand for uPAR PET imaging in cancer patients.
The urokinase-type plasminogen activator receptor (uPAR) is a cell membrane protein involved in extracellular matrix degradation. Besides regulating proteolysis, uPAR also activates many intracellular signaling pathways that promote cell motility, invasion, and proliferation through cooperation with transmembrane receptors. In normal tissues, uPAR expression is limited. However, in cancer uPAR is frequently overexpressed, for example, in urinary bladder cancer (UBC), uPAR immunoreactivity is detected in 96% of the neoplasias at the invasive front (1), and in more than 500 breast cancer (BC) patients studied only 2% had uPAR levels below the detection limit (2). Importantly, high uPAR expression is associated with cancer invasion and metastases. Accordingly, uPAR represents an established biomarker for aggressive disease and poor prognosis in a variety of human cancers, including the most common malignant diseases, such as BC, colorectal cancer, lung cancer, UBC, and prostate cancer (PC) (1,3–11).
These observations highlight and support that noninvasive imaging of uPAR in cancer tissue could become a clinically relevant diagnostic and prognostic imaging biomarker with the possibility of distinguishing indolent tumors from the invasive phenotype.
Accordingly, we have for several years focused on development of radioligands based on the high-affinity peptide antagonist AE105 for PET imaging of uPAR expression (12–17). We recently published results from a promising first-in-human study with 64Cu-DOTA-AE105 showing high uptake in both primary tumor lesions and lymph node metastases paralleled with high uPAR expression in excised tumor tissue, thereby providing evidence for uPAR PET imaging in cancer patients (4). However, clinical translation of 64Cu-based radioligands is hampered by limited availability and the necessity of a cyclotron facility to produce the PET isotopes. In line with this, the generator-based PET isotope 68Ga has gained special attention because of its independence of an onsite cyclotron and a half-life of 68 min, which matches well with the pharmacokinetics of peptides such as the AE105 (18). The goal of the present phase I study was to investigate the feasibility of 68Ga-NOTA-AE105 for tumor imaging in humans. The primary aim was to evaluate the safety, pharmacokinetics, and internal radiation dosimetry of a single-dose injection of 68Ga-NOTA-AE105 in cancer patients using PET/CT imaging. The secondary objective was to investigate the uptake in primary tumor lesions and potentially in metastases if present.
MATERIALS AND METHODS
Study Design
In this open-label phase I study, 10 patients with histopathologically confirmed PC (6 patients), BC (2 patients), or UBC (2 patients) were enrolled from May 2015 to July 2015 (Table 1). All patients gave written informed consent before inclusion. The study was approved by the Danish Health and Medicine Authority (EudraCT no. 2014-005522-35) and the Ethical Committee of the Capital Region of Denmark (protocol H-15002406). The study was registered at ClinicalTrials.gov (NCT02437539) and was performed in accordance with the recommendation for Good Clinical Practice including independent monitoring by the Good Clinical Practice unit of the Capital Region of Denmark. All patients were injected intravenously with approximately 200 MBq of 68Ga-NOTA-AE105 followed by sequential whole-body PET/CT scanning 10 min, 1 h, and 2 h after injection. The dose was chosen to provide adequate count statistics and based on preclinical data was projected to be well below the maximum acceptable radiation exposure and at the same level as 18F-FDG PET scanning. In a subset of 6 patients (patients 4, 5, 6, 7, 8, and 10), blood was collected approximately 1, 5, 30, and 90 min after injection for pharmacokinetic analysis, including ligand stability. Urine was collected from 3 patients (patients 7, 8, and 10) during the test period. Safety measures included observation and systematic questions of subjective well-being and monitoring of heart rate and blood pressure with regular intervals before, during, and after the last image session (1 min, 10 min, 1 h, and 2 h after injection). Hematologic (hemoglobin, white blood cells, platelets), liver (alanine amino transferase, alkaline phosphatase, lactate dehydrogenase), and renal function (s-creatinine, glomerular filtration rate, sodium, potassium) were measured before radioligand administration, immediately after and on return to the hospital 3–21 d after the study day (Supplemental Fig. 1; supplemental materials are available at http://jnm.snmjournals.org). When available, preoperative biopsies or surgically excised primary tumor tissue and local lymph nodes were collected for target validation, demonstrating immunohistochemical expression of uPAR.
Patient Characteristics
Production of 68Ga-NOTA-AE105
NOTA-AE105 trifluoroacetate was obtained from ABX GmbH. 68Ga (half-life = 68 min; maximum positron energy [Emax, β+] = 1.90 MeV [89%]) labeling of NOTA-AE105 trifluoroacetate was performed using a Modular-Lab Standard module (Eckert & Ziegler). The 68Ge/68Ga generator (IGG100; Eckert & Ziegler) was eluted with 6 mL of 0.1 M HCl. The eluate was concentrated on a Strata-XC cartridge and eluted with 700 μL of 0.82 M HCl/acetone (2:98). NOTA-AE105 (32 nmol), dissolved in 10 μL of dimethyl sulfoxide, was labeled in 500 μL of 0.7 M NaOAc buffer, pH 5.2, and 200 μL of 96% EtOH at room temperature for 12 min. The resulting product, 68Ga-NOTA-AE105, was purified on a SepPak C18 light cartridge (Waters), eluted with 50% ethanol, and formulated with saline to a total volume of 7 mL.
For analysis, a high-performance liquid chromatograph (Ultimate 3000; Dionex) was used with a 2.6-μm, 100-Å, 50 × 4.6 mm C18 column (Kinetex) and with the ultraviolet and radiodetector connected in series. The mobile phases were eluent A, 10% MeCN in H2O with 0.1% trifluoroacetic acid, and eluent B, 10% H2O in MeCN with 0.1% trifluoroacetic acid. For thin-layer chromatography a ScanRam scanner and plates were used. The mobile phase was 77 g of ammonium acetate per liter in water/methanol (1:1). For gas chromatography, a Shimadzu GC2014 was used with a Zebron ZB-WAX 30 m × 0.53 mm × 1.00 μm column.
PET/CT Acquisition
All subjects fasted 6 h before injection of 68Ga-NOTA-AE105. Two peripheral intravenous catheters were placed, 1 for radiotracer injection and 1 in the contralateral arm for withdrawal of blood samples and administration of CT contrast agent.
Data acquisition was performed using a PET/CT system (Biograph mCT; Siemens Medical Solutions) with an axial field of view of 216 mm. Emission scans were acquired 10 min, 1 h, and 2 h after intravenous administration of 68Ga-NOTA-AE105 (≈200 MBq). Whole-body PET scans were obtained in 3-dimensional mode, with an acquisition time of 2 min per bed position. Attenuation- and scatter-corrected PET data were reconstructed iteratively using a 3-dimensional ordinary Poisson ordered-subset expectation-maximization algorithm including point-spread function and time-of-flight information (Siemens Medical Solutions); the settings were 2 iterations, 21 subsets, 2-mm gaussian filter, and a 400 × 400 matrix. Pixel size in the final reconstructed PET image was approximately 2 × 2 mm with a slice thickness of 2 mm. Due to artifacts, the halo effect on 68Ga-NOTA-AE105 PET in the tissue surrounding the urinary bladder caused by the prompt γ of 68Ga at 1,077 keV (brancing ratio of 3.2%) (19), all image data were also reconstructed using prompt γ-correction. A diagnostic CT scan was obtained before the 1-h PET scan, with a 2-mm slice thickness, 120 kV, and a quality reference of 225 mAs modulated by the Care Dose 4D automatic exposure control system (Siemens Medical Solutions). A low-dose CT scan, 2-mm slice thickness, 120 kV, and 40 mAs, was acquired before each of the 10-min and 2-h scans and used for attenuation correction. An automatic injection system was used to administer 75 mL of an iodine-containing contrast agent (Optiray 300; Covidien) with a scan delay of 60 s and flow rate of 1.5 mL/s, followed by an injection of 100 mL of NaCl with a flow rate of 2.5 mL/s. PET images in units of Bq/mL were used for quantitative analysis of tissue radioactivity concentrations for dosimetry purposes and for calculation of SUVs.
Plasma Pharmacokinetics and Urine Metabolite Analysis
The blood and urine samples were analyzed on a Dionex UltiMate 3000 column-switching high-pressure liquid chromatograph system with a Posi-RAM Module 4 as previously described (4). The mobile phase for the extraction step was 0.1% trifluoroacetic acid in H2O, whereas the analytic step was a gradient method with solvent A, 0.1% trifluoroacetic acid in MeCN: H2O 10:90, and solvent B, 0.1% trifluoroacetic acid in MeCN:H2O 90:10, both with a flow of 1.5 mL/min. The gradient was 0–6 min (extraction), 6–7 min 0%–10% B, 7–13 min 10%–65% B, 13–14 min 65%–10% B, 14–15 min 10% B.
Dosimetry
Dosimetry was based on the decay-uncorrected image sets from the 3 time points supplemented with sampled urine data (3 patients) as previously described (4). Briefly, cumulated activity for each patient and organ was determined by integration of time–activity curves based on an average of 3 spheric volumes of interest (VOIs) placed in all major organs defined on CT images using Mirada RTx (Mirada Medical). Individual urine excretion data were fitted to monoexponentials yielding the fraction of injected activity excreted and a biologic half-life of the process. All data were entered into OLINDA/EXM software (Vanderbilt University) to obtain corresponding estimates of organ-absorbed doses and effective dose. OLINDA’s Voiding Bladder Model was used with fraction and half-life from the fitted urine data as input and an assumed bladder-voiding interval of 1 h.
Tumor Uptake by Visual Image Analysis and Activity Quantification
All image data were analyzed by a team consisting of a highly experienced certified specialist in nuclear medicine and a highly experienced certified specialist in radiology for the presence of lesions suggestive of cancer. Semiquantitative analyses of visually detectable tumor lesions were done by drawing spheric VOIs. Because of low counts, the image quality of the last scan (2 h after injection) was suboptimal for assessing tumor uptake, and therefore SUVs were calculated only from the generated VOIs for the first 2 PET scans (10 min and 1 h after injection) and parameterized as SUVmean and SUVmax. In some cases, the standard PET reconstruction showed a reduced signal (halo effect) around the urinary bladder. The halo led to hampered tumor visualization and to underestimation of SUVs of both normal and tumor tissue. Therefore, all PET image data were reconstructed again using prompt γ-correction. The data were subsequently reanalyzed for tumor uptake by the same team of specialists, with more than 3 mo between interpretations, and the SUVs presented here were obtained from prompt γ-corrected images.
Collection of Tissue Samples and Immunohistochemistry of uPAR Expression
Surgical specimens of primary tumors and metastases were obtained from 2 BC patients undergoing surgical treatment subsequently to 68Ga-NOTA-AE105 PET. The time interval between 68Ga-NOTA-AE105 PET and surgery was 5 and 2 d, respectively. Four of the patients with locally advanced PC underwent lymphadenectomy before radiation therapy. None of these patients had lymph node metastases based on CT findings. Prostate tumor specimens were available from the preoperative prostate biopsies only (except from patient 5, for whom the initial biopsy was taken at a regional hospital and therefore not available). The specimens were placed in formalin. Sections were prepared with paraffin sections (2.5 μm thick), and a standard immunohistochemistry technique (avidin–biotin–peroxidase) was performed to visualize the immunostaining intensity and distribution of uPARs as previously described using the monoclonal antibody R2 (4). In addition, hematoxylin and eosin staining was performed. The sections were visually evaluated for visible uPAR-positive staining and scored as either positive or negative.
Statistics
The significance of differences in vital signs and blood tests were evaluated using ANOVA. A P value of less than 0.05 was considered statistically significant.
RESULTS
Radiochemistry
All preparations complied with the specifications. The specifications and results of the 68Ga-NOTA-AE105 preparations are given in Supplemental Table 1.
Patient Safety and Dosimetry
The administered mass of NOTA-AE105 was 13.6 ± 8.7 μg (range, 4.4–34.7 μg). The mean administered activity was 154 ± 59 MBq (range, 48–208 MBq). None of the patients experienced infusion-related reactions or adverse events. There were no clinically detectable pharmacological effects of 68Ga-NOTA-AE105 and no changes in general well-being or vital signs (Supplemental Table 2). No acute or long-term effects on blood parameters or organ (liver and kidney) functions were found using standard biochemical parameters before and after participation in this study (Supplemental Fig. 1). The dose calculations yielded an effective dose of 0.015 mSv/MBq (Table 2). The bladder was the organ with the highest absorbed dose (0.131 mGy/MBq), followed by the kidneys (0.070 mGy/MBq).
uPAR PET Dosimetry
Biodistribution, Pharmacokinetics, and Image Quality
A characteristic imaging series, illustrating biodistribution at 10 min, 1 h, and 2 h after injection, is shown in Figure 1. The excretion route appeared to be mainly through the kidneys with no or little excretion through the hepatobiliary/gastrointestinal tract. Persistently, there was a relatively high but decreasing blood-pool activity, and virtually no activity was found in the brain, lung, bone, and muscle.

Whole-body distribution and SUV in major organs after injection of 68Ga-NOTA-AE105. (A) Maximum-intensity-projection PET images at 10 min, 1 h, and 2 h after injection of 68Ga-NOTA-AE105 (patient 2). Highest accumulation of activity was in kidneys and bladder. (B) Decay-corrected SUVs in blood and major organs plotted individually for n = 10 patients. For each patient, regions of interest were drawn on selected organ of interest at all 3 consecutive PET scans.
Six of 10 patients (patients 4, 5, 6, 7, 8, and 10) in the study were used for investigating the plasma pharmacokinetics of 68Ga-NOTA-AE105. A plasma half-life of 8.5 min was found. Only intact 68Ga-NOTA-AE105 and no major metabolites were detected in plasma or urine (Supplemental Fig. 2).
Tumor Uptake of 68Ga-NOTA-AE105 and Ex Vivo Target Validation
The secondary objective of this study was to investigate the uptake of 68Ga-NOTA-AE105 in malignant tissue in BC, PC, and UBC. Patient-specific clinical information and imaging findings are detailed in Table 3.
Summary of uPAR PET/CT and Immunohistochemistry of uPAR Expression in Available Tumor Tissue
BC
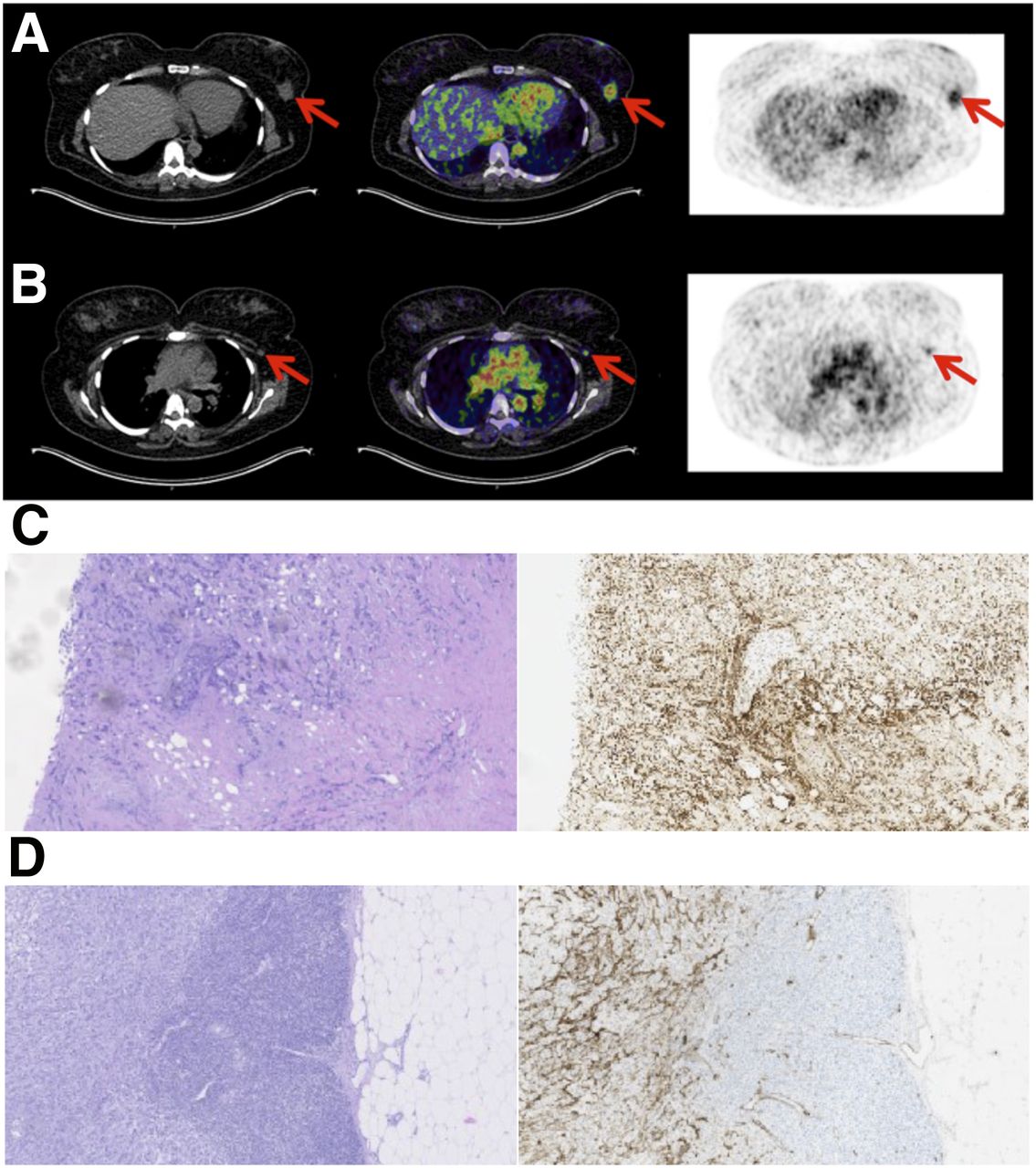
Two BC patients were included before surgical intervention (patients 1 and 6). On qualitative image analysis, primary tumor uptake was clearly visualized already at the first (10 min) and at the 1-h PET scan. In addition, the 68Ga-NOTA-AE105 PET scan clearly visualized metastatic spread to the ipsilateral axillary lymph nodes in both patients. This was confirmed with operative findings and final histopatohologic staging (Fig. 2). One of these patients (patient 6) was positive on the preoperative routine examination with ultrasound and fine-needle biopsies, whereas in the other patient (patient 1) the metastatic spread was found only during sentinel node operation and the following complete axillary lymph node dissection confirmed metastatic spread to 2 of 19 lymph nodes. Positive uPAR immunohistochemistry on surgical specimens of primary tumors and metastatic lymph nodes in both patients confirmed uPAR expression.
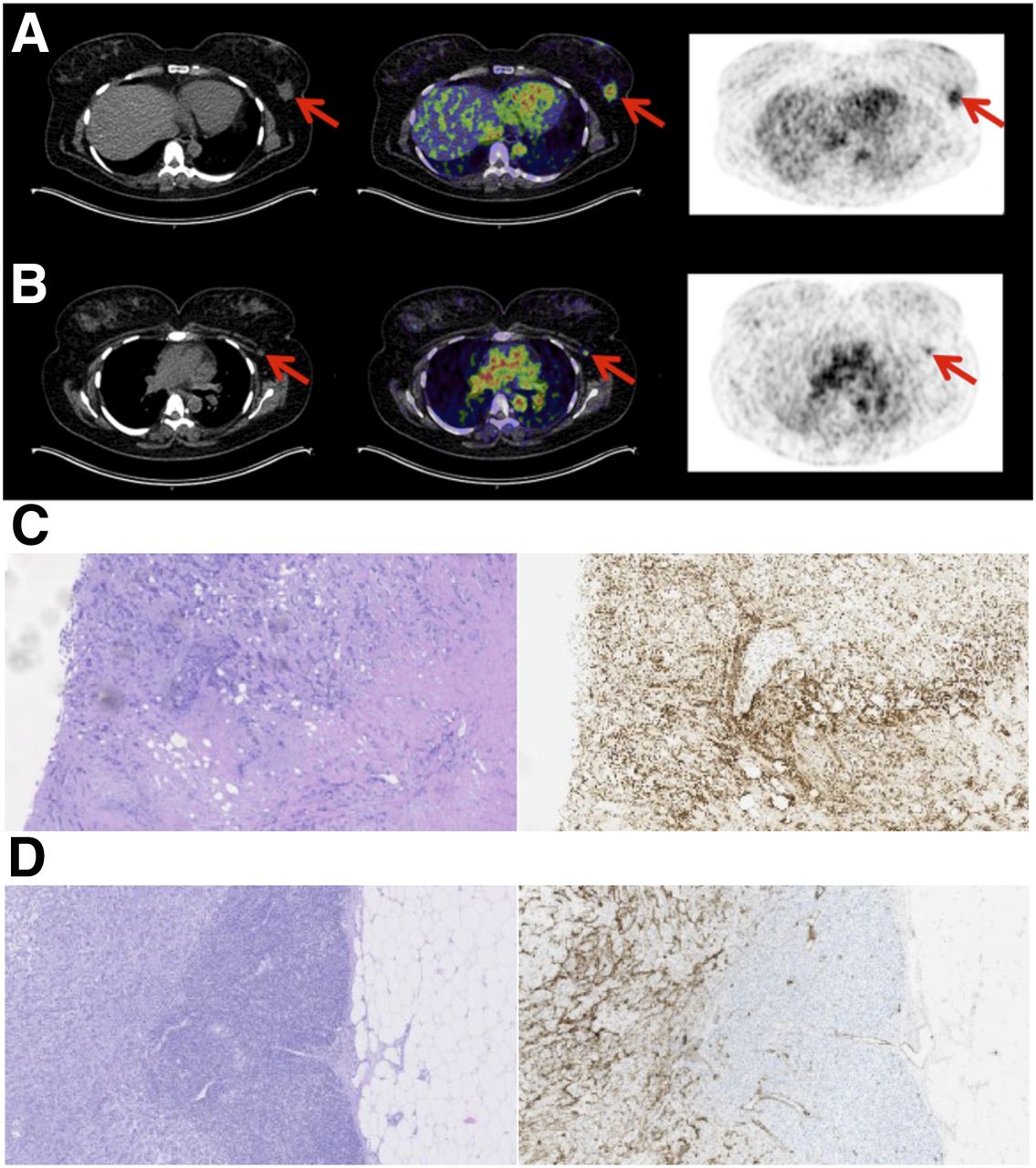
uPAR PET imaging in BC. (A) Representative transverse CT, PET, and coregistered PET/CT images of primary tumor lesion with intense uptake of 68Ga-NOTA-AE105 (patient 1). (B) Images show uPAR-positive axillary lymph node metastasis (red arrow) with significant uptake in same patient. (C) Representative slides with intense uPAR immunohistochemistry staining and corresponding hematoxylin and eosin staining of tumor tissue from patient’s primary tumor. (D) uPAR immunohistochemistry staining and corresponding hematoxylin and eosin staining of lymph node metastases.
PC
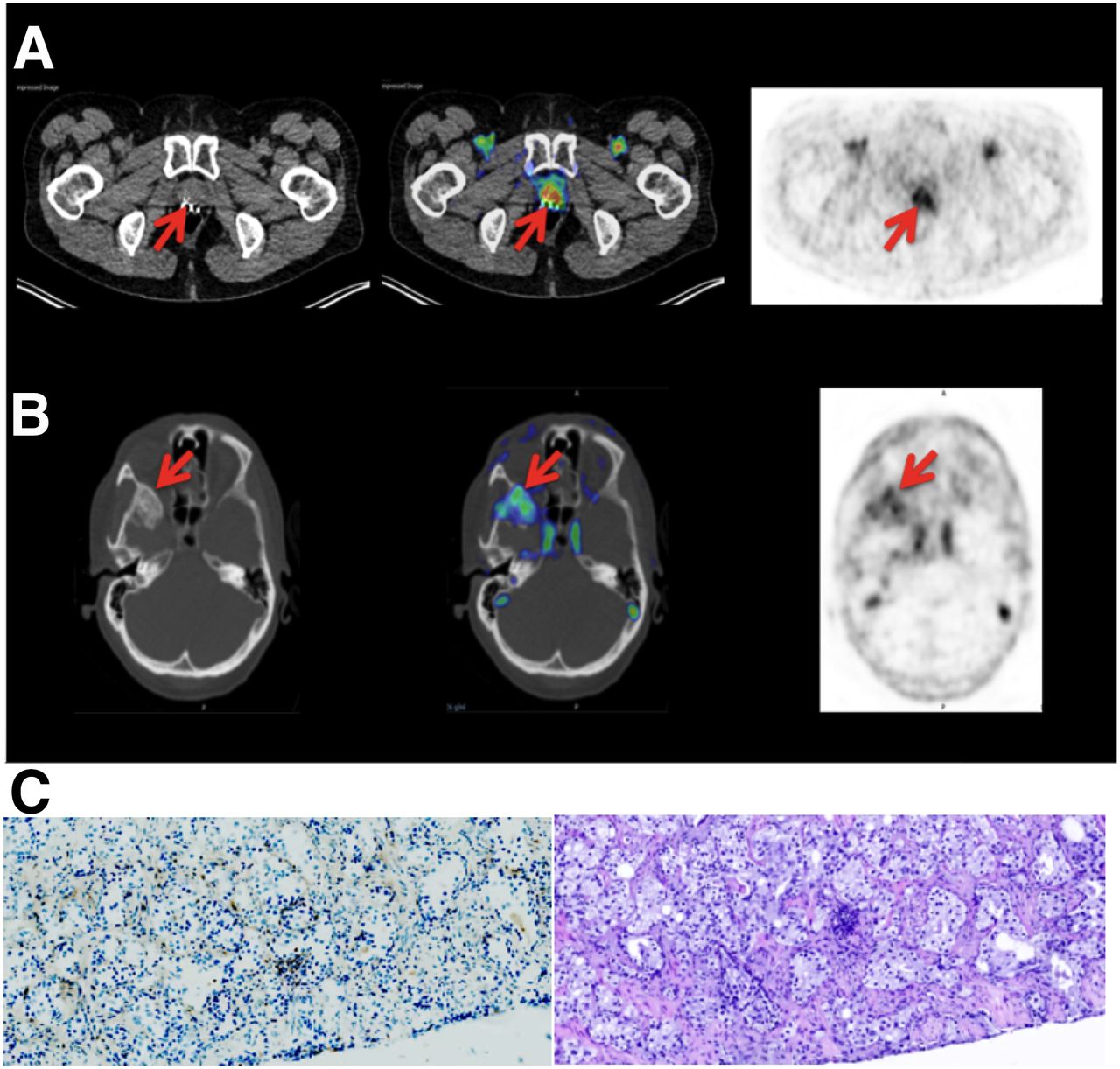
Of the 6 patients with PC, 4 patients with newly diagnosed locally advanced PC (patients 2, 3, 4, and 10) were included in the study before a planned open staging procedure with pelvic lymph node dissection. In these patients a low, heterogeneous intraprostatic distribution of the radioligand was found, with no distinct tumor uptake and no detectable tracer uptake in regional lymph nodes. The latter was in line with the findings at the open staging procedure because pathologic examinations of the removed pelvic lymph nodes showed no lymph node involvement. The remaining 2 patients with PC (patients 7 and 8) had bone metastases and were evaluated before chemotherapy. Both patients had multiple metastases with significant 68Ga-NOTA-AE105 uptake in several malignant lesions concurrent with heterogeneous uptake at the site of the primary tumor within the prostate gland. In the 3 available preoperative prostate biopsies, immunohistochemistry confirmed uPAR expression (Fig. 3).

uPAR PET imaging in PC. (A) Representative transverse CT, PET, and coregistered PET/CT images with uptake of 68Ga-NOTA-AE105 at site of primary tumor (patient 7). (B) Images show uPAR-positive metastasis in sphenoid bone (red arrow) with significant uptake in same patient. (C) Representative slides with weak uPAR immunohistochemistry staining of tumor tissue from preoperative biopsy and corresponding hematoxylin and eosin staining (patient 10).
UBC
Two patients with UBC were included in the study during an ongoing chemotherapy regime with only a small amount of residual disease. Both patients had proven response to chemotherapy, as evaluated by routine CT scans, before inclusion in the present study. In 1 patient (patient 9) there was no visible uptake of 68Ga-NOTA-AE105 in 2 liver metastases, which were identified on the concomitant contrast-enhanced CT. No other lesions could be identified on either 68Ga-NOTA-AE105 or diagnostic CT with intravenous contrast.
DISCUSSION
In this first-in-human study, we present the results of a 68Ga-labeled uPAR PET radioligand, 68Ga-NOTA-AE105. Together with our previous phase I study with the 64Cu-labeled DOTA-AE105, the present study confirms that it is possible to detect uPAR expression in tumor lesions noninvasively with PET/CT.
uPAR PET/CT imaging with 68Ga-NOTA-AE105 was safe, with no adverse events or obvious changes in general well-being or any vital signs. In addition, no significant changes in total blood count or kidney or hepatic function occurred.
As expected, the biodistribution analysis revealed the primary excretion route to be renal, with resulting high activity accumulation of 68Ga-NOTA-AE105 in kidneys and urinary bladder due to the high hydrophilicity and small size of the peptide. In addition, a relatively high blood-pool activity could indicate some protein-bound activity of the intact 68Ga-NOTA-AE105 or free 68Ga bound to transferrin (20). The decreasing blood-pool activity argues against continuous transchelation of 68Ga to transferrin, and the radioligand cleared fast from organs and the blood-pool activity probably reflects plasma protein bound activity. Compared with our 64Cu-DOTA-AE105, we found a lower accumulation of activity in the liver after injection of 68Ga-NOTA-AE105, which is favorable with respect to evaluation of possible liver metastases. Apart from the urinary tract, no other organ or tissues exhibited high nonspecific uptake of 68Ga-NOTA-AE105.
The effective radiation dose was 0.0153 mSv/MBq, equaling 3.1 mSv at an injected activity of approximately 200 MBq, which was applied in the present study. This is lower or comparable to the radiation dose received from a standard 18F-FDG PET scan, for which the effective dose is approximately 0.019 mSv/MBq, equal to 5.7 mSv at a standard dose of 300 MBq (21). The administration of intravenous contrast agent for the 1-h PET/CT scan could potentially result in a modest overestimation of SUVs in background organs. However, this is not expected to have any clinically significant effect on the calculated radiation dose, because based on our results from a previous study the average error in SUVmean was found to be only 1.6% in background organs (22). In addition, it could be argued that a high tumor uptake potentially alters biodistribution. However, because the tumor burden in the current study was relatively small (localized PC, primary BC with no signs of spread, and UBC with minimal residual disease). We therefore believe that tumor uptake had no influence of the biodistribution and the final organ dosimetry.
Importantly, the radiation dose to bone marrow was below the recommended threshold value of 3 mSv (23) Therefore, the radiation burden of uPAR PET with 68Ga-NOTA-AE105 is of no clinical concern, and the effective dose is comparable to that of other clinically applied 68Ga-based PET radioligands, such as 68Ga-labeled prostate-specific membrane antigen (24) and 68Ga-DOTATATE/DOTATOC (25).
Plasma pharmacokinetic and urine metabolite analysis revealed intact 68Ga-NOTA-AE105 in blood and urine and no formation of isotopic labeled metabolites, which is also found in other radioligands (26,27).
As a secondary objective of this phase I study, tumor detection, including SUVs and semiquantitative tumor uptake values, was evaluated. The radioligand performed well in the visual detection of metastatic tumor lesions, especially in BC, for which metastatic disease in ipsilateral axillary lymph nodes was found even in a situation in which the preoperative workup with ultrasound, fine-needle aspiration, and contrast-enhanced CT failed to detect the metastases. This is a clear clinical example of a potential future application of uPAR PET, because this patient could have gone directly to axillary lymph node dissection after uPAR PET and circumvented the other procedures if uPAR PET had been performed preoperatively. The current procedure with preoperative fine-needle biopsy finds only approximately one third of the patients with metastatic spread (28). Therefore, uPAR PET imaging could potentially be a superior technology for this purpose, when focusing on the high and specific radioligand uptake in lymph node metastases found in the present study. However, a sufficiently powered, controlled clinical trial has to be performed to prove this hypothesis.
The failure of 68Ga-NOTA-AE105 PET to detect 2 metastases in the liver in a patient with disseminated UBC (patient 9) might question the application of 68Ga-NOTA-AE105 for disseminated UBC. However, other PET radioligands, for example, 3′-deoxy-3′-18F-fluorothymidine and 18F-galacto-RGD, have also been reported to have lower activity in malignant liver lesions compared with the relatively high physiologic uptake in normal liver tissue (29,30). Another explanation could be downregulation of uPAR expression and tumor inactivation as a result of clinical response to chemotherapy before inclusion in the study. However, future studies to further investigate this hypothesis are warranted.
In PC and BC, tracer uptake in malignant tissue was visible on uPAR PET scans at 10 min and 1 h after injection. The optimal administered dose of 68Ga-NOTA-AE105 and time for PET/CT scan after injection still needs to be established, but it is likely within the first 60 min, which is also the case for other peptide-based radioligands such as 68Ga-prostate-specific membrane antigen (24), 68Ga-DOTATATE/DOTATOC (31), and RGD peptides (32).
Histopathologic examination of the surgical specimens from the primary BC tumors/metastasis and the 3 available preoperative primary PC biopsies demonstrated uPAR expression in all patients, supporting target-specific uptake of 68Ga-NOTA-AE105. Although the preoperative PC biopsies, compared with BC tissue, showed only weak uPAR expression, the limited number of patient samples made it impossible to apply a robust quantitative scoring system and no attempt was made to correlate ex vivo expression of uPAR in the excised surgical specimens with image-derived semiquantitative tracer uptake. It is possible that the general pattern of low, heterogeneous uptake of 68Ga-NOTA-AE105 in prostatic tumors reflects weak tumor uPAR expression in these 6 PC patients who either had localized disease or were treated with radio-/chemotherapy. A significant correlation of uPAR expression based on immunohistochemistry and tumor uptake of the comparable radioligand 64Cu-DOTA-AE105 has previously been demonstrated in murine tumor models (12). However, future prospective studies should ideally include a detailed and complete coregistration between imaging and subsequent cross-section pathology.
The artifact (halo effect) in the form of reduced activity around the urinary bladder with high physiologic activity uptake due to urinary excretion has been described using other 68Ga-based ligands, such as 68Ga-prostate-specific membrane antigen (33) and 68Ga-DOTATOC (34). However, this is of no major concern because it is easily removed by prompt γ-correction, which will be implemented in future standard reconstruction algorithms for 68Ga PET (oral personal communication with Siemens, November 2015).
In addition to BC staging, a promising application of a uPAR-based imaging agent may be in providing an imaging biomarker to determine the aggressiveness of a tumor, thereby giving prognostic information with possible therapeutic implications.
CONCLUSION
This first-in-human clinical study demonstrates the feasibility and potential of using a 68Ga-labeled version of the AE105 peptide for uPAR-targeted PET imaging. The administration of 68Ga-NOTA-AE105 was safe, was well tolerated, and provided satisfactory image contrast and identification of primary tumors and metastases. The most promising results were found in BC, with clear identification of metastatic axillary lymph nodes. Future phase II studies in larger patient populations with this indication will investigate the application and utility of uPAR PET in relevant clinical settings.
DISCLOSURE
This work was supported by the John and Birthe Meyer Foundation, the Danish National Advanced Technology Foundation, the Danish Council for Strategic Research, the Research Foundation of Rigshospitalet, the Capital Region of Denmark, the Novo Nordisk Foundation, the Lundbeck Foundation, the A.P. Moeller Foundation, the Svend Andersen Foundation, the Arvid Nilsson Foundation, Innovation Fund Denmark, and the Danish Council for independent research. Andreas Kjaer (AK), Morten Persson (MP), and Jacob Madsen (JM) are inventors of the composition of matter of uPAR PET with a filed patent application: Positron Emitting Radionuclides Labeled Peptides for Human uPAR PET Imaging (WO 2014086364 A1). AK, MP, and AK are cofounders of Curasight, which has licensed the uPAR PET patent to commercialize the uPAR PET technology (uTRACE®). Dorthe Skovgaard has received funding from Curasight. No other potential conflict of interest relevant to this article was reported.
Acknowledgments
We thank all patients and their families for participating in this study. In addition, we will thank our excellent staff (Bente Dall, Susanne Svalling, Elisabeth Abrahamsson, and Maria Pejtersen) at the department for taking part in the conduction of the study.
Footnotes
↵* Contributed equally to this work.
Published online Sep. 8, 2016.
- © 2017 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication May 31, 2016.
- Accepted for publication August 18, 2016.





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- uPAR Immuno-PET in Pancreatic Cancer, Aging, and Chemotherapy-Induced Senescence
- Prospective Phase II Trial of Prognostication by 68Ga-NOTA-AE105 uPAR PET in Patients with Neuroendocrine Neoplasms: Implications for uPAR-Targeted Therapy
- Prognostic Value of Urokinase-Type Plasminogen Activator Receptor PET/CT in Head and Neck Squamous Cell Carcinomas and Comparison with 18F-FDG PET/CT: A Single-Center Prospective Study
- Urokinase-Type Plasminogen Activator Receptor (uPAR) PET/MRI of Prostate Cancer for Noninvasive Evaluation of Aggressiveness: Comparison with Gleason Score in a Prospective Phase 2 Clinical Trial
- Primary Preclinical and Clinical Evaluation of 68Ga-DOTA-TMVP1 as a Novel VEGFR-3 PET Imaging Radiotracer in Gynecological Cancer
- Plasma levels of intact and cleaved urokinase plasminogen activator receptor (uPAR) in men with clinically localised prostate cancer