


Abstract
16α-18F-fluoro-17β-estradiol (18F-FES) is an estrogen receptor (ER)–specific PET tracer with various potential interesting applications. The precise contribution of this technique in current clinical practice, however, has yet to be determined. Therefore, the aim of this study was to evaluate the value of 18F-FES PET in breast cancer patients presenting with a clinical dilemma. Methods: 18F-FES PET examination could be requested by referring physicians for patients with a history of ER-positive breast cancer and the presence of a clinical dilemma despite complete standard work-up. All requests for 18F-FES PET required a positive arbitration by a dedicated medical oncologist and nuclear medicine physician. The referring physician was asked to fill in validated questionnaires before, shortly after, and at more than 3 mo after 18F-FES PET to determine indication, diagnostic value, and therapeutic consequences of 18F-FES PET. To further validate 18F-FES PET findings, 18F-FES PET lesions were quantified and compared with centrally reviewed conventional imaging. Results: Thirty-three patients underwent 18F-FES PET between December 2008 and October 2010. 18F-FES PET was requested to evaluate equivocal lesions on conventional work-up (n = 21), ER status in metastatic patients (n = 10), and the origin of metastases (n = 2). 18F-FES–positive lesions were observed in 22 patients. 18F-FES PET was especially sensitive for bone metastases, detecting 341 bone lesions, compared with 246 by conventional imaging. The sensitivity for liver metastases was poor, and quantification of 18F-FES uptake in liver lesions was hampered by high physiologic background. 18F-FES uptake was highly variable between all metastases (range of standardized uptake value, 1.20–18.81), and 45% of the patients with a positive 18F-FES PET finding had both 18F-FES–positive and 18F-FES–negative metastases. 18F-FES PET improved diagnostic understanding in 88% of the patients and led to therapy change in 48% of the patients. Conclusion: With the exception of liver metastases, whole-body imaging of ER expression with 18F-FES PET can be a valuable additional diagnostic tool when standard work-up is inconclusive. 18F-FES PET supported therapy decisions by improving diagnostic understanding and providing information on ER status of tumor lesions.
Breast cancer is the most common cancer in women in the Western world (1). Approximately 75% of the tumors express the estrogen receptor (ER) at diagnosis (2). Knowledge of the ER status of a patient has important consequences for treatment decision making, because patients with ER-positive tumors are likely to respond to antihormonal therapy (3).
Evaluation of ER status is therefore performed by means of immunohistochemical staining of the primary tumor. This golden standard has some limitations: it predicts tumor response to antihormonal therapy correctly in only 50%–60% of the patients (4,5). The technique is semiquantitative, which can result in interobserver variation, and ER scoring depends on the antibody used and delay-to-fixation time (6,7). The recent systematic review by the American Society of Clinical Oncology and the College of American Pathologists revealed that up to 20% of all immunohistochemical determinations worldwide are inaccurate (8). Absence of ER expression does, however, have a strong negative predictive value for response to antihormonal therapy (9).
Also during metastatic disease, evaluation of ER status is important to determine changes in receptor expression. This evaluation is of relevance because discordant ER expression between primary tumor and metastatic lesions occurs in 18%–55% of the patients (10,11). A recent study in 336 patients with an ER-positive primary tumor revealed loss of ER expression in distant metastases in 36% of these patients, which was a predictor of poor response to antihormonal therapy (12). For this reason, guidelines of the European Society for Medical Oncology and National Comprehensive Cancer Network recommend repeated biopsies (13,14). In addition, biopsies of suspected recurrences are advised to confirm the diagnosis of metastasized breast cancer and to exclude benign lesions or (metastases from) a second cancer.
Despite these clear indications for rebiopsy, this may not always be feasible because of the characteristics of the lesion (such as location) or the patient (such as comorbidity). Additionally, within a single tumor or across lesions within a patient, ER expression can be heterogeneous (15). In these cases, a single biopsy may not be representative of the ER characteristics of the tumor burden as a whole. Furthermore, physicians may be reluctant to perform biopsies given the invasive nature of the procedure. A noninvasive method to quantify ER expression in all metastatic lesions would therefore be valuable.
Whole-body PET with 16α-18F-fluoro-17β-estradiol (18F-FES) provides a unique method to noninvasively obtain molecular information about ER expression (16,17). Several studies have shown that 18F-FES PET can reliably detect ER-positive tumor lesions and that 18F-FES uptake correlates well with immunohistochemical scoring for ER (18–20). Furthermore, low 18F-FES uptake was a strong predictor for failure of antihormonal therapy (21–23). On the basis of these results, 18F-FES PET examinations have been routinely requested in our center since December 2008 for patients with a history of ER-positive breast cancer in whom a clinical dilemma remained despite complete standard work-up (e.g., when imaging procedures were inconclusive and performing a biopsy was not feasible). The aim of this study was to determine the value of 18F-FES PET in breast cancer patients presenting with a clinical dilemma.
MATERIALS AND METHODS
Patients
Patients with a history of histologically proven ER-positive breast cancer were eligible for routine 18F-FES PET examination when, despite complete standard work-up, they presented a clinical dilemma for their treating physician. All requests for 18F-FES PET required a positive arbitration by a dedicated medical oncologist and nuclear medicine physician. A detailed medical history, current complaints, laboratory results (if available), and conventional imaging results were collected from all patients. The informed consent requirements for these retrospectively enrolled patients were waived by the University Medical Center Groningen Institutional Review Board (METc 2010.102).
Standard Work-up
The routine staging protocol for these patients adheres to the Dutch Breast Cancer Guidelines, which are highly comparable with National Comprehensive Cancer Network guidelines (version 2.2011) (13). In short, work-up for disseminated disease includes chest CT or chest imaging, CT of the abdomen or ultrasound of the liver, and bone scanning. During follow-up, examinations are directed by signs and symptoms and include bone scanning or MRI in the case of localized bone pain or elevated alkaline phosphate; chest CT in the case of chest lesions or pulmonary complaints; and abdomen CT in the case of abdominal lesions or abnormal liver tests. The use of 18F-FDG PET is discouraged and limited to patients with equivocal lesions, although tissue biopsy is more likely to provide useful information in these cases. Biopsies of suspected distant recurrences are recommended to confirm the diagnosis of metastatic breast cancer and evaluate receptor status.
18F-FES PET
ER antagonists were discontinued for a minimum of 5 wk before 18F-FES PET to prevent false-negative results. The use of aromatase inhibitors was allowed. 18F-FES was produced as previously described (24). 18F-FES that was ready for injection was obtained in a 32% ± 10% decay-corrected radiochemical yield. Specific activity was 182 ± 101 MBq/nmol, with a radiochemical purity of 99.9% ± 0.3%. Patients received 18F-FES (207 ± 8 MBq) intravenously. Whole-body 18F-FES PET was performed 60 min after tracer injection, using an ECAT Exact HR+ PET camera (Siemens CTI) (spatial resolution, 5 mm; emission time, 5 min; and transmission time, 2 min per bed position) or a 64-slice mCT (PET/CT) camera (Siemens CTI), with 2-mm spatial resolution with an emission time of 3 min per bed position and a transmission CT scan for attenuation correction. All scans and quantifications were obtained according to the guidelines for tumor PET of the European Association of Nuclear Medicine (25). Scans were reconstructed with a gaussian filter of 5 mm in full width at half maximum, and iterative reconstruction methods were used with 3 iterations and 24 subsets. PET images were assessed qualitatively and quantitatively by a nuclear medicine physician. In reference to other 18F-FES PET studies, we used the maximum SUV (SUVmax) to quantify ER expression and a cutoff value of 1.5 or more to dichotomize results into ER-positive and ER-negative (20). When in the field of view, CT data were used to allocate PET-positive lesions to an anatomic substrate.
Analysis of Imaging Results
Imaging analysis was performed retrospectively. Lesions detected by 18F-FES PET were recorded, and 18F-FES uptake was quantified. When a patient had innumerable lesions, an arbitrary maximum of 40 lesions was recorded. Aside from evaluation of the routine radiology and nuclear medicine reports, conventional imaging was centrally reevaluated, with the investigators masked to other imaging results. All lesions were classified into benign, equivocal, and metastatic categories. Thereafter, conventional imaging results were compared with findings on 18F-FES PET. For discordant lesions, a fusion of 18F-FES PET with CT, MRI, or 18F-FDG PET and a one-to-one comparison between 18F-FES PET and bone scanning were performed for final classification of these lesions. Follow-up imaging and clinical data were reviewed, whenever available, to evaluate remaining discordances.
Clinical Value
Validated questionnaires were used to collect the insight of the referring physician before, shortly after, and more than 3 mo after 18F-FES PET (26). Questionnaire 1 served to identify the clinical dilemma and intended therapeutic strategy. Using the reason for 18F-FES PET examination, we retrospectively categorized the patients into 3 different groups. Questionnaire 2 permitted us to evaluate the outcome of 18F-FES PET study and the influence of the exam on treatment decision making. The last questionnaire served to analyze the value of 18F-FES PET on diagnostic understanding and therapy management after a follow-up of at least 3 mo, using a 5-point scale (Table 1). The scoring was performed by the referring physicians. All questionnaires were checked for internal consistency.
Questionnaire
Statistical Analysis
Differences in tracer uptake between different (patients and) organs were analyzed by a 1-way ANOVA. Site-to-site variability in 18F-FES uptake was expressed as coefficient of variability. Scores on diagnostic understanding and therapeutic consequences were calculated for the 3 different reasons for 18F-FES PET examination with a 2-sided nonparametric Kruskal–Wallis test.
RESULTS
Patient Characteristics
Thirty-three patients were referred for 18F-FES PET examination between December 2008 and October 2010. Patients were retrospectively divided into 3 groups that were based on the reason for the 18F-FES PET examination: to differentiate between benign and malignant lesions in the case of equivocal or ambiguous work-up (n = 21), to evaluate the patients’ ER status (n = 10), and to differentiate between metastases originating from different tumor types (n = 2). Patient characteristics are shown in Table 2.
Patient Characteristics
18F-FES PET and Conventional Imaging Results
18F-FES PET was performed in 22 patients and 18F-FES PET/CT in 11. Work-up before 18F-FES PET consisted of CT (n = 24), bone scanning (n = 23 patients), MRI (n = 8), and 18F-FDG PET (n = 3). Ultrasound and radiographic images were not considered in our analysis. Biopsy of suggestive lesions was performed before 18F-FES PET in 4 patients and during follow-up in 2. PET showed 18F-FES–positive metastases in 22 of the 33 patients. No apparent false-positives were noted in a patient-based analysis.
18F-FES PET was negative in 11 patients. In 3 patients, 18F-FES PET showed no tumor lesions despite the presence of metastases, matching the histologic findings (ER-negative) in tumor biopsy in 2 patients. In 1 patient, 3 mo later, biopsy showed an immunohistochemical ER-positive metastasis in the liver. In the remaining 8 patients, the negative 18F-FES PET findings concurred with the absence of metastases during follow-up of 6 mo.
In total, 398 lesions were detected by 18F-FES PET. Lesions were located in bone (n = 341 lesions), lymph nodes (n = 26), lung or pleura (n = 19), liver (n = 8), and soft tissue (n = 4). Although investigators were unaware of the 18F-FES PET results, they detected 242 of these 398 18F-FES–positive lesions (61%) on conventional imaging. After comparison between conventional imaging and 18F-FES PET, an additional 79 lesions with 18F-FES uptake could also be detected using conventional techniques. Of the remaining lesions, 15 were confirmed during follow-up. Therefore, most 18F-FES PET lesions (n = 336, 84%) could eventually be validated by conventional techniques. The remaining 62 lesions were not detected during follow-up. However, nearly all these lesions were additional bone metastases in patients with known bone metastases. It is therefore plausible that these lesions are also true-positives.
Investigators (who were unaware of the 18F-FES PET results) detected a total of 319 metastases on conventional imaging. Of these, 18F-FES PET missed 77 lesions (24%). The detection of liver metastases by 18F-FES PET was poor. None of 7 patients with known liver metastases had increased focal 18F-FES uptake. In 2 patients, however, cold spots were observed at the site of liver metastases, and in 2 others 18F-FES uptake was more heterogeneous than in other patients. Also, relatively few lymph nodes were detected by 18F-FES PET (26/55 lymph nodes, 47%). However, 68% of the undetected nodes had diameters less 15 mm (Response Evaluation Criteria in Solid Tumors, version 1.1, cutoff value for measurable lymph node metastases), indicating that some of these may have been misclassified or were below the detection threshold for PET (27). An overview of the concordance between conventional imaging and 18F-FES PET is shown in Table 3.
Malignant Lesions Detected at Conventional Imaging and 18F-FES PET
Heterogeneity of 18F-FES Uptake
A striking 11-fold difference in tracer uptake was observed between different patients (range of SUVmax, 1.68–18.81), and a 6-fold difference was observed between lesions within the same individual (range of SUVmax, 2.59–15.84). The coefficient of variability for the SUVmax of all 18F-FES PET lesions was high (68% ± 4%, 95% confidence interval). In 45% of the patients, both 18F-FES–positive and 18F-FES–negative metastases were present, suggesting partial discordant ER expression. Only 1 patient had conversion to a complete ER-negative phenotype, indicated by the absence of 18F-FES uptake in all (n = 4) tumor lesions. Quantification of 18F-FES uptake in liver metastases was hampered because of high physiologic uptake in surrounding normal liver tissue. Mean 18F-FES uptake did not differ significantly among metastases in different organs (Fig. 1). Only 1 premenopausal patient underwent 18F-FES PET in this study. She had tracer uptake (SUV range, 1.2–1.65) in tumor lesions far below the 95% confidence interval (5.91 ± 0.38) of the postmenopausal patients. Although it may be theoretically plausible that 18F-FES uptake depends on estrogen background level, this cannot be concluded from these limited data.

Differences in tracer uptake in all 22 patients with positive lesions on 18F-FES PET (A) and tracer uptake at different sites of metastases (n = 398 lesions) (B). No significant differences in average SUVmax were observed; however, bone metastases did show significantly higher coefficient of variance. Bars represent 25–75 percentiles, and whiskers represent minimal to maximum values.
Clinical Value of 18F-FES PET
18F-FES PET in Case of Equivocal or Conflicting Standard Work-up
Twenty-one patients underwent 18F-FES PET to evaluate equivocal or ambiguous findings on standard work-up or for signs and symptoms for which no substrate could be found on conventional imaging. Equivocal lesions were present in bone (n = 13), lung (n = 4), liver (n = 3), and abdomen (n = 1). These patients underwent bone scanning (n = 16), CT (n = 16), MRI (n = 4), 18F-FDG PET (n = 3), or biopsy (n = 3) before 18F-FES PET, which did not establish a final diagnosis. In 9 of these, 18F-FES PET showed elevated uptake at the suspected lesion, confirming the presence of ER-positive metastases. Interestingly, in 3 patients biopsies before 18F-FES PET did not show malignancy, despite suspected distant recurrences on conventional imaging. 18F-FES PET showed multiple 18F-FES–positive lesions in these 3 patients (Fig. 2). The next therapeutic choice was affected by 18F-FES PET in 7 of 9 patients with positive 18F-FES PET findings. Four of them received radiotherapy, and 1 received bisphosphonates, in addition to the intended antihormonal therapy, after 18F-FES PET provided confirmation of bone metastases. In 2 patients, first-line antihormonal therapy for metastatic disease was initiated. In the remaining 12 patients, 18F-FES uptake was absent in the equivocal lesion. Six months of follow-up of the lesions indicated no metastasis in 10 of 12 patients. In 2 patients, given persisting uncertainty about the nature of the lesion, a biopsy was performed. Histology showed ER-negative adenocarcinoma in 1 patient and an ER-positive liver metastasis in the other patient. In 2 patients, 18F-FES PET was negative at the suspected site but revealed unknown metastases at other sites. 18F-FES PET affected therapy management in only 2 patients with 18F-FES–negative findings. In these 2, 18F-FES PET led the physician to refrain from radiotherapy in the absence of 18F-FES uptake at the suspected lesions and confirmed benign disease during follow-up.
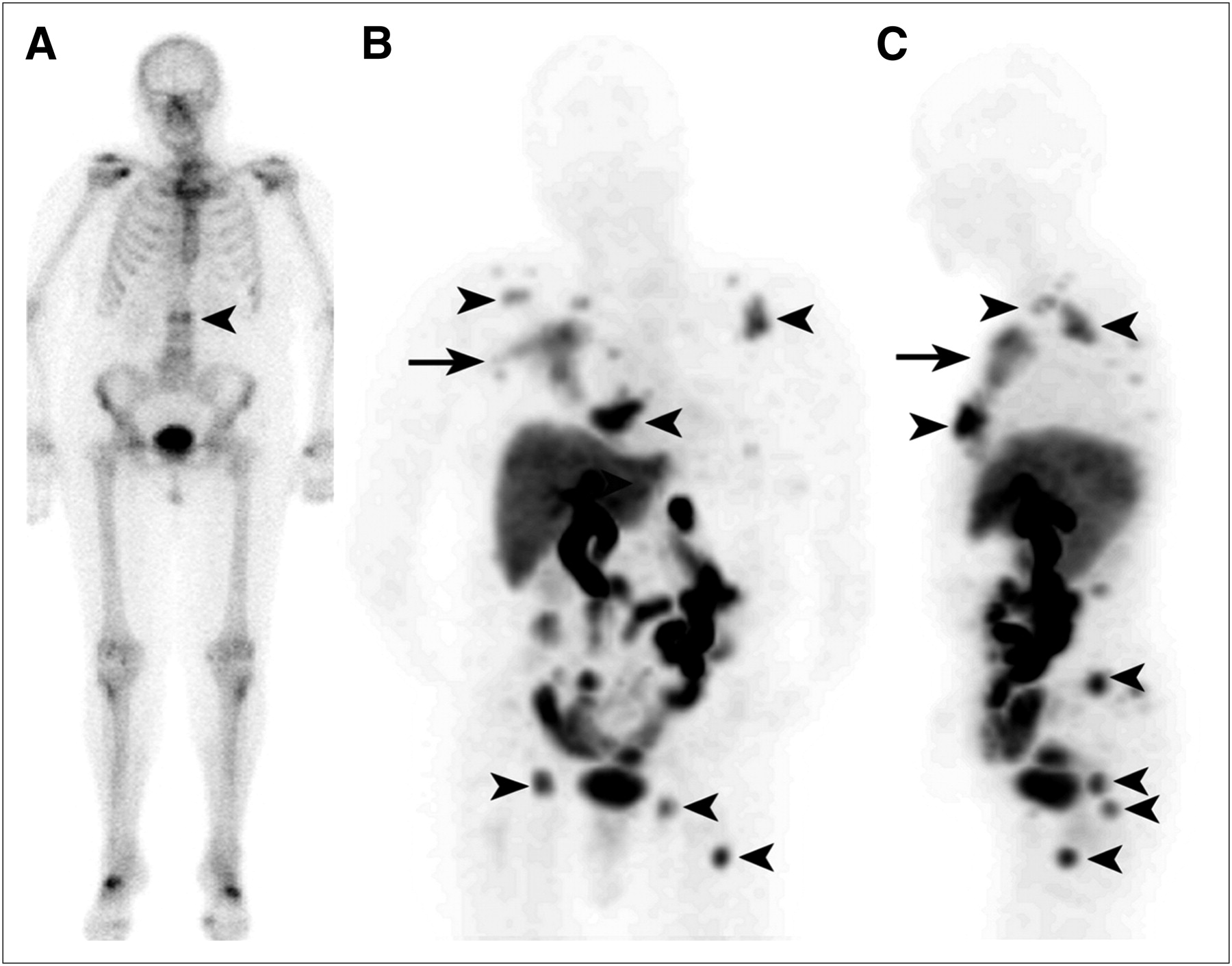
Bone scan (A) of patient showing suggestive lesion at L2 (arrowhead). Biopsy of this lesion did not show malignancy. Coronal (B) and sagittal (C) images of 18F-FES PET showing 18F-FES uptake in vertebra L2 and multiple other bone metastases (arrowheads), as well as large locoregional recurrence in soft tissue (arrow). Only most intense lesions are indicated.
18F-FES PET to Evaluate ER Expression After Progression on Antihormonal Therapy
Ten patients underwent 18F-FES PET to evaluate their ER status after progression on antihormonal therapy. In these patients, there was no consensus on whether to give chemotherapy or antihormonal therapy. 18F-FES PET showed increased 18F-FES uptake in one or more metastatic lesions in all 10 patients. In 6 of these, there was partial discordance, with an absence of 18F-FES uptake in some metastases. In 4 patients, intended chemotherapy was switched to antihormonal therapy based on high 18F-FES uptake. One patient with signs of bone marrow invasion on 18F-FES PET and accompanying thrombocytopenia was switched to chemotherapy (Fig. 3).

Bone scan (A), 18F-FES PET (B), and 18F-FES PET/CT (C and D) images of patient with progressive disease after multiple lines of antihormonal therapy and chemotherapy. Extensive tracer uptake was seen in bone, in lymph nodes, and intracerebrally. Interestingly, 18F-FES uptake seemed to be predominant in bone marrow of this patient, in whom laboratory signs of bone marrow infiltration were present.
18F-FES PET to Differentiate Between Metastases Originating from Different Tumor Types
In 2 patients, definite malignant lesions were detected by conventional imaging. It was uncertain whether these originated from the earlier ER-positive breast tumor or from another tumor type. One patient presented with a radicular syndrome in the region of root C6, 5 y after a primary breast cancer diagnosis. Neurologic examination and MRI indicated pathologic compression at vertebra C6, suspected to be due to a metastasis or plasmacytoma. A biopsy to prove the origin of the metastasis was considered too risky. 18F-FES PET showed uptake in C6 and T4 (Fig. 4). No other tumor lesions were observed. Therefore, this patient received antihormonal therapy for metastatic disease and radiotherapy. A second patient, known to have an ER-negative second tumor, presented with a single metastasis in the humerus. Too little material was obtained by biopsy to differentiate between the ER-positive and ER-negative primary. 18F-FES PET showed no lesional uptake, suggesting an origin from the ER-negative tumor. Therefore, this patient did not receive antihormonal therapy.
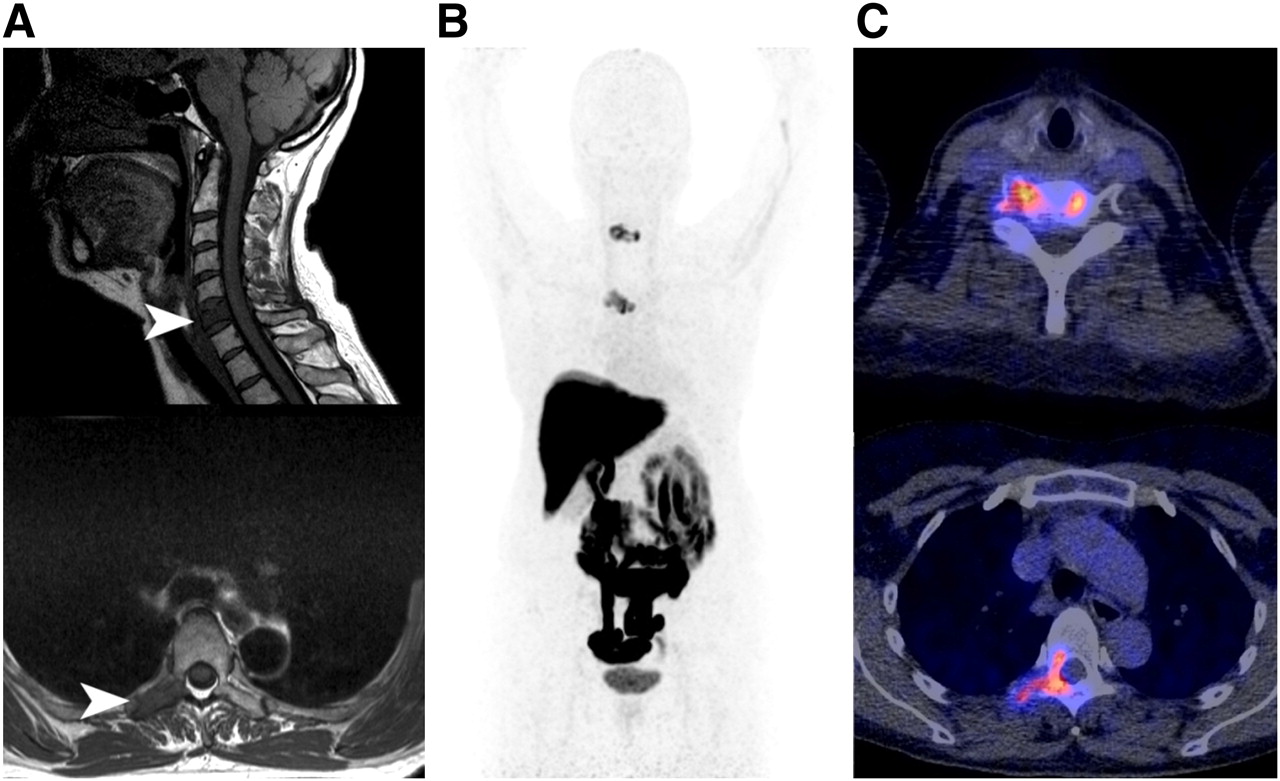
This patient presented with neurologic symptoms of root C6 5 y after primary breast cancer diagnosis. On MRI (A), pathologic processes were suspected in C6 and T4. Biopsy to prove that these were metastases and originated from prior primary breast cancer was considered too risky. 18F-FES uptake was observed in suspected metastases in C6 and T4 (B). 18F-FES PET/CT images (C) matched MRI findings. No other pathologic uptake was observed.
Questionnaires
All 3 questionnaires for the 33 patients were fully completed. Referring physicians reported an improved diagnostic understanding in 29 of the 33 patients (88%). In 18 of these patients, improved understanding was the consequence of 18F-FES PET solely, whereas in 11 patients other factors were equally or more important. Diagnostic understanding was independent of the indication for 18F-FES PET (P = 0.12), but positive 18F-FES PET results were superior (P = 0.002).
A change in therapeutic strategy based on 18F-FES PET was reported in 16 (48%) of the 33 patients. In 11 of them, information provided by 18F-FES PET was important in leading to a change in therapy, whereas in 5 patients other factors were equally or more important. Showing 18F-FES uptake in equivocal lesions led to the initiation of radiotherapy (n = 4), bisphosphonates (n = 1), and antihormonal therapy (n = 3). The presence of 18F-FES uptake in known metastases led to the initiation of a new line of antihormonal therapy (n = 4). The absence of 18F-FES uptake in known metastases and in equivocal lesions, respectively, led to the discontinuation of antihormonal therapy (n = 2) and radiotherapy (n = 2) (Table 4).
Changes in Therapeutic Strategy after 18F-FES PET
DISCUSSION
This is the first study, to our knowledge, evaluating the value of 18F-FES PET in breast cancer patients presenting with a clinical dilemma unresolved after conventional work-up. The study shows that whole-body imaging of ER expression with 18F-FES PET can be a valuable additional diagnostic tool when conventional work-up is ambiguous and biopsies are not feasible or inconclusive.
On the questionnaires, the referring physicians reported an improved diagnostic understanding in 88% (29/33) and therapy changes in 48% (16/33) of patients. We retrospectively divided patients who underwent 18F-FES PET into 3 groups. The first group underwent 18F-FES PET to establish a diagnosis in the case of equivocal or conflicting conventional work-up. Recent guidelines (European Society for Medical Oncology/National Comprehensive Cancer Network) suggest that 18F-FDG PET can be considered in the case of equivocal imaging, although biopsy is more likely to provide useful information (13,14). In our patients, 18F-FDG PET was rarely requested, for various reasons (e.g., positive 18F-FDG PET findings would not exclude inflammatory disease or would not differentiate between metastases from ER-positive breast cancer and metastases from another cancer origin) (28,29). 18F-FES PET has been shown to detect ER-positive metastases with high specificity (18–20). Therefore, this technique may be used as a surrogate for tissue biopsy when lesions are difficult to access. In our study, biopsies were not feasible or were inconclusive in several patients. We showed that 18F-FES PET could be used to prove the presence of ER-positive metastases in the case of an equivocal conventional work-up. However, 18F-FES PET cannot be used to exclude metastases in general because ER-negative metastases may be present.
In light of a possible conversion in ER phenotype, knowledge of ER expression can potentially facilitate the choice between chemotherapy and antihormonal therapy. Single-biopsy studies have shown conversion from an ER-positive to ER-negative phenotype in up to 30% of the patients. In addition, 18F-FES PET studies have shown 18F-FES–negative disease in 32%–53% of the patients, which was highly predictive of failure to respond to antihormonal therapy. We evaluated ER expression in 10 patients in whom a biopsy was problematic. All 10 had 18F-FES–positive metastases. Interestingly, our results indicated that an extensive variance in 18F-FES uptake can be present across positive lesions within individuals (coefficient of variance, 68% ± 4%). This heterogeneity matches findings of multiple biopsies from individual patients showing that a variety of ER levels can be present (30,31). Furthermore, 45% of the patients with a positive 18F-FES PET finding had both 18F-FES–positive and 18F-FES–negative metastases. This percentage was higher than previously reported (10%–24%) (32), pointing toward the relevance of 18F-FES PET, because it provides knowledge of whole-body tumor ER expression. So far, the consequence of a heterogeneous ER expression for therapy management has received strikingly little attention in the clinic and deserves further exploration.
The last group of patients in our study underwent 18F-FES PET to differentiate between distant recurrences originating from the earlier ER-positive primary breast tumor and metastases originating from a second tumor. The ER-specific 18F-FES tracer permitted noninvasive differentiation between tumor types, avoiding the necessity of additional (invasive) diagnostic procedures and leading to early institution of the right drug.
Our study and approach has limitations. We provide an analysis of the value of 18F-FES PET in the standard clinical situation. The standardized questionnaires we used can still be subject to bias and should be interpreted with caution. Therapy changes were carefully made while taking into account earlier therapies, other imaging results, and clinical presentation. Imaging analysis was performed retrospectively, possibly leading to potential bias. To minimize bias favoring 18F-FES PET, we performed a central revision of all conventional imaging. Because of the absence of a clear golden standard, sensitivities and specificities cannot be given. Prospective studies should be performed to prove that 18F-FES PET can replace the biopsy for treatment decisions.
Current 18F-FES PET studies do not describe its capacity to detect liver metastases. The physiologic uptake in the liver due to metabolization well exceeds the 18F-FES uptake that is seen in the uterus (33) or most ER-positive metastases. In our study, the detection of liver metastases by 18F-FES PET was poor, and 1 histologic ER-positive metastasis was not detected. We did observe focal cold lesions in 2 other patients. Quantification of 18F-FES uptake in these lesions was hampered by the high physiologic uptake in surrounding tissue. Because liver biopsies were not available in these patients, it is unknown whether the cold appearance can be explained by focal loss of ER expression. 18F-FES–negative liver metastases should therefore be evaluated by immunohistochemistry in future studies.
There are several factors other than ER expression that might affect 18F-FES uptake. Because of the resolution limitations of PET, small metastases may not show 18F-FES uptake. In addition, the presence of estrogen analogs such as tamoxifen can block tumor 18F-FES uptake (22). For this reason, we chose an arbitrary drug withdrawal period of 5 wk for ER ligands. Patients who discontinued fulvestrant 5 wk before 18F-FES PET had a high rate of 18F-FES–negative lesions (14/20 metastases). A 5-wk drug withdrawal period may therefore not have been sufficient to exclude occupancy of ERs by this drug with a long half-life of 40 d. The only premenopausal patient in this study had 18F-FES uptake values well below the 95% confidence interval of postmenopausal patients. In a previous study in primary breast cancer patients, only 6 of 10 patients with ER-positive tumors showed focal 18F-FES uptake (16). Although not mentioned in the discussion of this report, all 4 patients with a false-negative 18F-FES PET finding were most likely premenopausal because their ages ranged from 34 to 45 y, whereas the age of the 6 patients with a true-positive 18F-FES PET finding ranged from 56 to 71 y. Together, these data underline the possibility that background estrogen levels influence 18F-FES uptake, which warrants further exploration.
CONCLUSION
Whole-body imaging of ER expression with 18F-FES PET can aid in diagnosis and support treatment decision making in ER-positive breast cancer patients presenting with a variety of diagnostic dilemmas. On the basis of our results, we do not recommend using 18F-FES PET to evaluate liver metastases. The therapeutic consequences of having heterogeneous 18F-FES uptake and the influence of background estrogen levels should further be explored.
DISCLOSURE STATEMENT
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734.
Acknowledgments
We thank Dr. Riemer H.J.A. Slart for carefully evaluating all bone scans and Johannes H. van Snick for providing 18F-FES PET and PET/CT images for external revision. Portions of this study were supported by grant KWF-project RUG 2009-4529 of the Dutch Cancer Society. This paper was presented in part at the Annual Conference of the American Society of Clinical Oncology, June 2010, and at the Annual Congress of the European Association of Nuclear Medicine, Vienna, October 2010. No other potential conflict of interest relevant to this article was reported.
Footnotes
Published online Jan. 12, 2012.
- © 2012 by the Society of Nuclear Medicine, Inc.
REFERENCES
- Received for publication May 23, 2011.
- Accepted for publication October 7, 2011.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Impact of 18F-FES PET/CT on Clinical Decisions in the Management of Recurrent or Metastatic Breast Cancer
- Summary: Appropriate Use Criteria for Estrogen Receptor-Targeted PET Imaging with 16{alpha}-18F-Fluoro-17{beta}-Fluoroestradiol
- Value of 18F-FES PET in Solving Clinical Dilemmas in Breast Cancer Patients: A Retrospective Study
- Breast Cancer: Evaluating Tumor Estrogen Receptor Status with Molecular Imaging to Increase Response to Therapy and Improve Patient Outcomes
- 18F-FES PET/CT Influences the Staging and Management of Patients with Newly Diagnosed Estrogen Receptor-Positive Breast Cancer: A Retrospective Comparative Study with 18F-FDG PET/CT
- 18F-Fluoroestradiol PET Imaging of Activating Estrogen Receptor-{alpha} Mutations in Breast Cancer
- 18F-Fluoroestradiol Tumor Uptake Is Heterogeneous and Influenced by Site of Metastasis in Breast Cancer Patients
- In Vivo Quantification of ER{beta} Expression by Pharmacokinetic Modeling: Studies with 18F-FHNP PET
- Synthesis and Evaluation of the Estrogen Receptor {beta}-Selective Radioligand 2-18F-Fluoro-6-(6-Hydroxynaphthalen-2-yl)Pyridin-3-ol: Comparison with 16{alpha}-18F-Fluoro-17{beta}-Estradiol
- Estrogen Receptor Binding (18F-FES PET) and Glycolytic Activity (18F-FDG PET) Predict Progression-Free Survival on Endocrine Therapy in Patients with ER+ Breast Cancer
- Decoding Intratumoral Heterogeneity of Breast Cancer by Multiparametric In Vivo Imaging: A Translational Study
- 18F-Fluoroestradiol PET: Current Status and Potential Future Clinical Applications
- Nuclear Breast Imaging: Clinical Results and Future Directions
- Mouse Models of Breast Cancer: Platforms for Discovering Precision Imaging Diagnostics and Future Cancer Medicine
- Quo Vadis: PET and Single-Photon Molecular Breast Imaging
- Molecular Imaging of Biomarkers in Breast Cancer
- Translation of New Molecular Imaging Approaches to the Clinical Setting: Bridging the Gap to Implementation
- Measuring Residual Estrogen Receptor Availability during Fulvestrant Therapy in Patients with Metastatic Breast Cancer
- Assessment of Estrogen Receptor Expression in Epithelial Ovarian Cancer Patients Using 16{alpha}-18F-Fluoro-17{beta}-Estradiol PET/CT
- GPER-Targeted, 99mTc-Labeled, Nonsteroidal Ligands Demonstrate Selective Tumor Imaging and In Vivo Estrogen Binding