


Abstract
18F-FDG PET can help in predicting therapeutic response and outcome in patients with metastatic pulmonary tumors. However, no satisfactory biologic explanation exists for this phenomenon. The aim of this study was to investigate the underlying biologic mechanisms of 18F-FDG uptake in metastatic pulmonary tumors. Methods: One hundred forty-six patients with metastatic pulmonary tumors who underwent 18F-FDG PET before treatment were included in this study. Tumor sections were stained by immunohistochemistry for glucose transporter 1 (Glut1), glucose transporter 3 (Glut3), hexokinase I, hypoxia-inducible factor-1α (HIF-1α), vascular endothelial growth factor (VEGF), and microvessel density determined by CD34. 18F-FDG uptake and the expression of these biomarkers were correlated in primary lung cancer and benign pulmonary lesions. Results: 18F-FDG uptake in metastatic pulmonary tumors correlated significantly with the expression of Glut1 (γ = 0.4579, P < 0.0001), HIF-1α (γ = 0.3654, P < 0.0001), hexokinase I (γ = 0.3921, P < 0.0001), VEGF (γ = 0.5528, P < 0.0001), and CD34 (γ = 0.2342, P = 0.0044). 18F-FDG uptake in metastatic pulmonary tumors was significantly lower than in primary lung cancer but higher than in benign pulmonary lesions. High uptake of 18F-FDG was significantly associated with poor outcome after pulmonary metastasectomy. In patients with metastatic pulmonary tumors, 18F-FDG uptake and the expression of Glut1, HIF-1α, and VEGF were significantly higher in adenocarcinoma and squamous cell carcinoma than in sarcoma. 18F-FDG uptake was significantly correlated with tumor size (P < 0.0001), but there was no significant relationship between tumor size and the expression of these biomarkers. Conclusion: The amount of 18F-FDG uptake in metastatic pulmonary tumors is determined by the presence of glucose metabolism (Glut1), phosphorylation of glucose (hexokinase I), hypoxia (HIF-1α), and angiogenesis (VEGF and microvessel density).
The lungs are one of the major metastatic sites of neoplasms arising from other organs. If the radiologic findings are typical of pulmonary metastasis, clinicians usually diagnose it using CT of the chest. However, it is sometimes difficult to differentiate metastatic pulmonary nodules from primary lung cancer or benign lesions. In such a situation, 18F-FDG PET may be useful for differentiating malignant tumors from benign lesions (1,2). However, 18F-FDG PET is not useful in differentiating primary lung cancer from a solitary pulmonary metastasis. Therefore, resection of pulmonary metastasis has become an integral part of diagnosis and treatment if the primary malignancies outside the thorax are controlled. Recently, 1 report suggested that 18F-FDG PET has a low sensitivity in the evaluation of metastatic pulmonary nodules when pulmonary metastasectomy is being considered (3). However, metastatic pulmonary nodules are a heterogeneous group of tumors, including such histologic types as squamous cell carcinoma (SQC), adenocarcinoma, and sarcoma. Because 18F-FDG uptake is directly associated with glucose metabolism (4), the sensitivity of 18F-FDG PET differs among the various histologic types of the primary malignancies. Little is known about the relationship between 18F-FDG uptake and metastatic pulmonary tumors in patients receiving pulmonary metastasectomy.
Determination of malignant lesions with 18F-FDG PET is based on glucose metabolism (3–5). The overexpression of glucose transporter 1 (Glut1) has been shown to be closely related to 18F-FDG uptake in human cancer (3–5). Glut1 is thought to be a possible intrinsic marker of hypoxia, and the expression of Glut1 has been found to be regulated by hypoxia in a manner dependent on hypoxia-inducible factor-1α (HIF-1α) (3–5). Previous studies suggest that hypoxic conditions correspond to a higher 18F-FDG uptake (6–8). In addition, several researchers described the relationship between 18F-FDG uptake and the expression of vascular endothelial growth factor (VEGF) or microvessel density (MVD) (9–11). HIF-1α is considered to support tumor growth by the induction of angiogenesis via the expression of VEGF and by high and anaerobic metabolic mechanisms (12). Because many factors can influence the extent of 18F-FDG uptake, the underlying mechanisms for 18F-FDG accumulation are still a matter of debate in various human neoplasms. However, there is still no relevant explanation of mechanisms for 18F-FDG uptake in metastatic pulmonary tumor secondary to primary malignancies outside the thorax. Defining a correlation between these biomarkers and 18F-FDG uptake may lead to a better understanding and interpretation of 18F-FDG PET scanning in metastatic pulmonary tumors. On the basis of this background, we conducted 18F-FDG PET studies and immunohistochemical analyses in patients with metastatic pulmonary tumors. We also evaluated the biologic correlation of 18F-FDG PET in patients with primary lung cancer and benign pulmonary lesions as a solitary-pulmonary-nodule control group.
MATERIALS AND METHODS
Patients
We analyzed 169 consecutive patients who underwent 18F-FDG PET and lung resection for pulmonary metastasis from extrathoracic malignancies at Shizuoka Cancer Center between April 2003 and May 2009. Patients who underwent PET before pulmonary metastasectomy were included in the study, whereas patients who had other malignancies or received induction chemotherapy or radiation before pulmonary metastasectomy were excluded. Six patients who received induction chemotherapy or radiation therapy were excluded. The specimens of 7 patients were not available. Ten patients were excluded from analysis because they did not undergo 18F-FDG PET within 4 wk before their pulmonary resection was performed. Thus, 146 patients were analyzed in the study. All patients were imaged using 18F-FDG PET.
We evaluated the biologic correlation of 18F-FDG PET in patients with non–small cell lung cancer (NSCLC), as compared with metastatic pulmonary tumors, as an other-pulmonary-malignancy test group. NSCLC patients were consecutively assigned to in the study between December 2002 and March 2004, and 18F-FDG PET was performed as part of the preoperative work-up. These patients underwent surgical management, and the primary lesions were surgically resected. Patients with NSCLC of the adenocarcinoma or SQC type were included in this study. NSCLC patients without visible tracer uptake on 18F-FDG PET were excluded from this study. Finally, 138 patients with NSCLC (93 with adenocarcinoma and 45 with SQC) were evaluated. These 138 patients had no metastatic pulmonary tumors that were due to primary malignancies outside the thorax.
We also compared the biologic correlation of 18F-FDG uptake between a control group of patients with benign pulmonary lesions and the group with metastatic pulmonary tumors. This control group had pulmonary lesions positive for 18F-FDG uptake that had been surgically resected. Between November 2002 and August 2008, 29 consecutive such patients were included in this study. The histology of the resected benign pulmonary lesion was as follows: 11 epitheloid granulomas, 4 cryptococcomas, 4 sarcoidoses, 6 cases of inflammatory change, and 4 other types.
None of the patients had insulin-dependent diabetes, and the serum glucose levels in all patients just before 18F-FDG PET were less than 120 mg/dL. The study protocol was approved by the institutional review board.
18F-FDG PET
Patients fasted for at least 4 h before 18F-FDG PET examination. They received an intravenous injection of 18F-FDG (200–250 MBq) and then rested for approximately 1 h before undergoing imaging (4). Images were acquired using an Advance NXi PET scanner and Discovery PET/CT scanner (GE Healthcare). Two-dimensional emission scanning was performed from the groin to the top of the skull. PET/CT images were independently reviewed by 2 experienced physicians. Acquired data were reconstructed by iterative ordered-subset expectation maximization. The tumor was first examined visually for 18F-FDG accumulation, and then the peak standardized uptake value (SUV) of the entire tumor was determined. Maximal SUV (SUVmax) was defined as the peak SUV on 1 pixel with the highest counts within the region of interest. The region of interest, measuring 3 cm in diameter, was set at the mediastinum at the level of the aortic arch, and the mean SUV of the mediastinum was calculated. Finally, the T/M ratio, which is the ratio of the peak SUV of the tumor to the mean SUV of the mediastinum, was determined for each patient.
Immunohistochemical Staining
Immunohistochemical staining was performed according to the procedure described in a previous report (4). The following antibodies were used: a rabbit polyclonal antibody against Glut1 (AB15309 [Abcam], 1:400 dilution), rabbit polyclonal antibody against glucose transporter 3 (Glut3) (AB15311 [Abcam], 1:100 dilution), mouse monoclonal antibody against HIF-1α (NB100-123 [Novus Biologicals, Inc.], 1:50 dilution), rabbit monoclonal antibody against hexokinase I (Abcam, 1:200 dilution), monoclonal antibody against VEGF (Immuno-Biologic Laboratories Co., Ltd., 1:300 dilution), and mouse monoclonal antibody against CD34 (Nichirei, 1:800 dilution).
The expression of Glut1 and Glut3 was considered positive if distinct membrane staining was present. Five fields (×400) were analyzed to determine the frequency of the HIF-1α–stained nuclei and hexokinase I–stained cytoplasm. For Glut1, Glut3, HIF-1α, and hexokinase I, a semiquantitative scoring method was used (1, <10%; 2, 10%–25%; 3, 25%–50%; 4, 51%–75%; and 5, >75% of cells positive). The tumors in which stained tumor cells made up more than 25% of the tumor were graded as positive.
The expression of VEGF was quantitatively assessed according to the percentage of immunoreactive cells in 1,000 neoplastic cells. The number of CD34-positive vessels was counted in 4 selected hot spots in a ×400 field (field area, 0.26 mm2). MVD was defined as the mean count of microvessels per 0.26-mm2 field area. Sections were assessed using light microscopy in a masked fashion by at least 2 of the authors.
Statistical Analysis
Probability values of less than 0.05 indicated a statistically significant difference. The Fisher exact test was used to examine the association of 2 categoric variables. Correlations between different variables were analyzed using the nonparametric Spearman rank test. The Kaplan–Meier method was used to estimate survival as a function of time, and survival differences were analyzed by the log-rank test. A receiver-operating-characteristic analysis was performed for determining a cutoff value of 18F-FDG uptake between malignant and benign lesions. Statistical analysis was performed using JMP 8 (SAS Institute Inc.) for Windows (Microsoft).
RESULTS
Patient Characteristics
The median age of the patients was 64 y (range, 16–82 y). Eighty-one patients were men, and 65 were women. The size of resected metastatic tumors ranged from 5 to 68 mm (median, 14 mm). Eastern Cooperative Oncology Group performance status was 0–1 in all patients. Seventy-five (51%) of the 146 patients were smokers. Fifty-seven patients received adjuvant chemotherapy after pulmonary metastasectomy. The primary site was colon in 80 patients, breast in 9, head and neck in 14, genital system in 12, esophagus in 3, gastrointestinal tract in 7, and other sites in 4. The primary was sarcoma in 17. In the NSCLC and control groups, the median size of the resected lesions was 23 mm (range, 6–100 mm) and 13 mm (range, 6–75 mm), respectively.
18F-FDG PET Findings and Survival Analysis
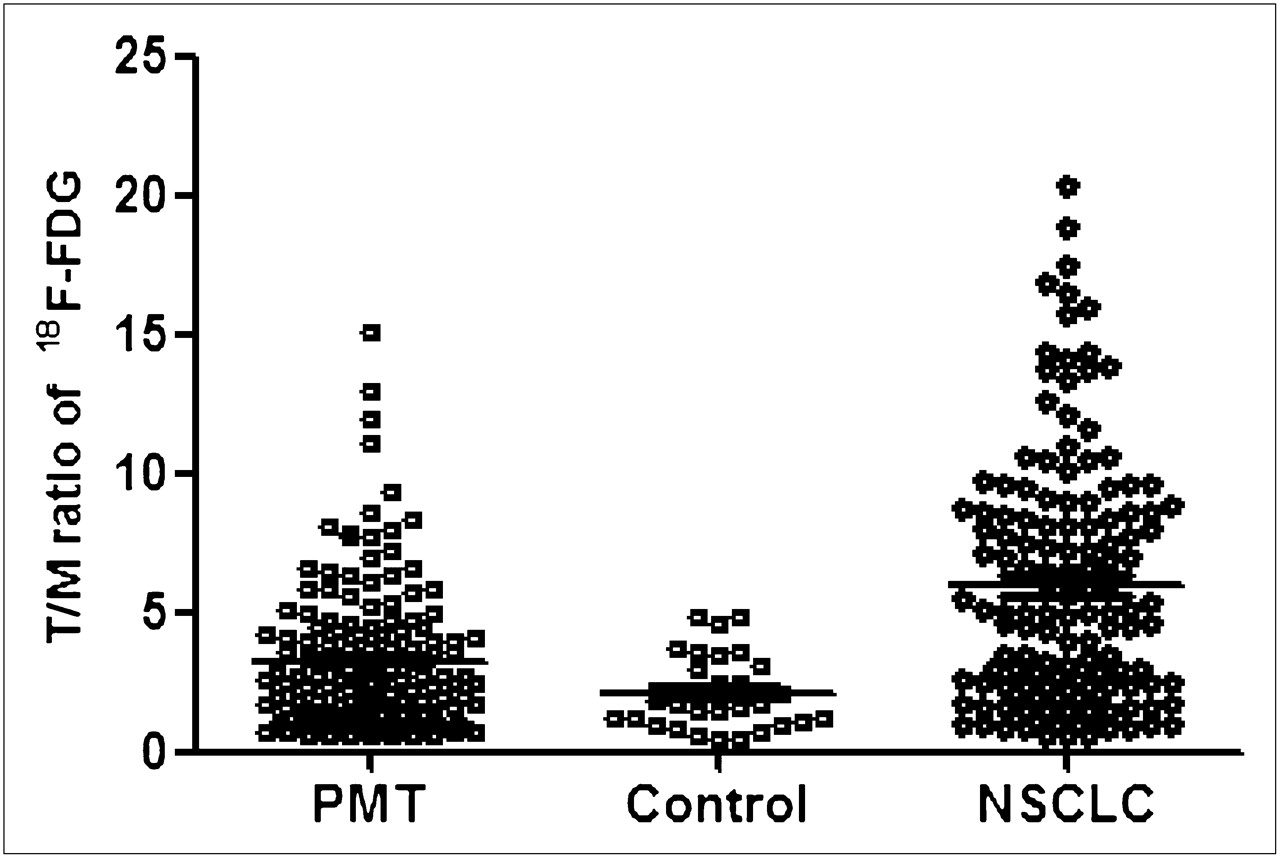
The mean (±SD) of the T/M ratio for metastatic pulmonary tumor, NSCLC, and control groups (benign pulmonary lesion) was 3.25 ± 0.22 (range, 0.95–9.43), 5.96 ± 0.38 (range, 0.8–20.3), and 2.12 ± 0.25 (range, 0.5–4.8), respectively. The T/M ratio was significantly higher in patients with metastatic pulmonary tumors (P = 0.0261) and NSCLC (P < 0.0001) than in the control group. The T/M ratio of metastatic pulmonary tumors was significantly lower than that of NSCLCs (P < 0.0001). The contribution of T/M ratio is listed in Figure 1.

Contribution of T/M ratio of 18F-FDG in metastatic pulmonary tumors, control group (benign lesion), and NSCLC. T/M ratio was significantly higher in patients with metastatic pulmonary tumors (P = 0.0261) and NSCLC (P < 0.0001) than in control group. T/M ratio of metastatic pulmonary tumors was significantly lower than that of NSCLC (P < 0.0001). PMT = metastatic pulmonary tumor.
The median value of T/M ratio in metastatic pulmonary tumors and the control group was 2.58 and 1.73, respectively. At a T/M ratio cutoff of 2.13 for positive 18F-FDG PET results, the receiver-operating-characteristic analysis revealed a 56.9% sensitivity and 62.1% specificity. Therefore, a median value of 2.13 was used as the cutoff T/M ratio in the following analyses, and a T/M ratio of more than 2.13 was defined as high uptake. The incidence of patients with a high T/M ratio was 48 (60%) of 80 for colon cancer, 5 (29%) of 17 for sarcoma, 5 (36%) of 14 for head and neck cancer, 4 (44%) of 9 for breast cancer, 8 (66%) of 12 for genital cancers, 2 (66%) of 3 for esophageal cancer, 5 (71%) of 7 for gastrointestinal cancer, and 2 (50%) of 4 for the other types of cancer (Supplemental Table 1; supplemental materials are available online only at http://jnm.snmjournals.org). According to the histologic subtype, the incidence of patients with a high T/M ratio was 61 (59%) of 103 for adenocarcinoma, 9 (69%) of 13 for SQC, and 6 (35%) of 17 for sarcoma. The incidence of a high T/M ratio was significantly higher in colon cancer than in sarcoma (P = 0.031), and no statistically significant difference was recognized between sarcoma and other cancers.
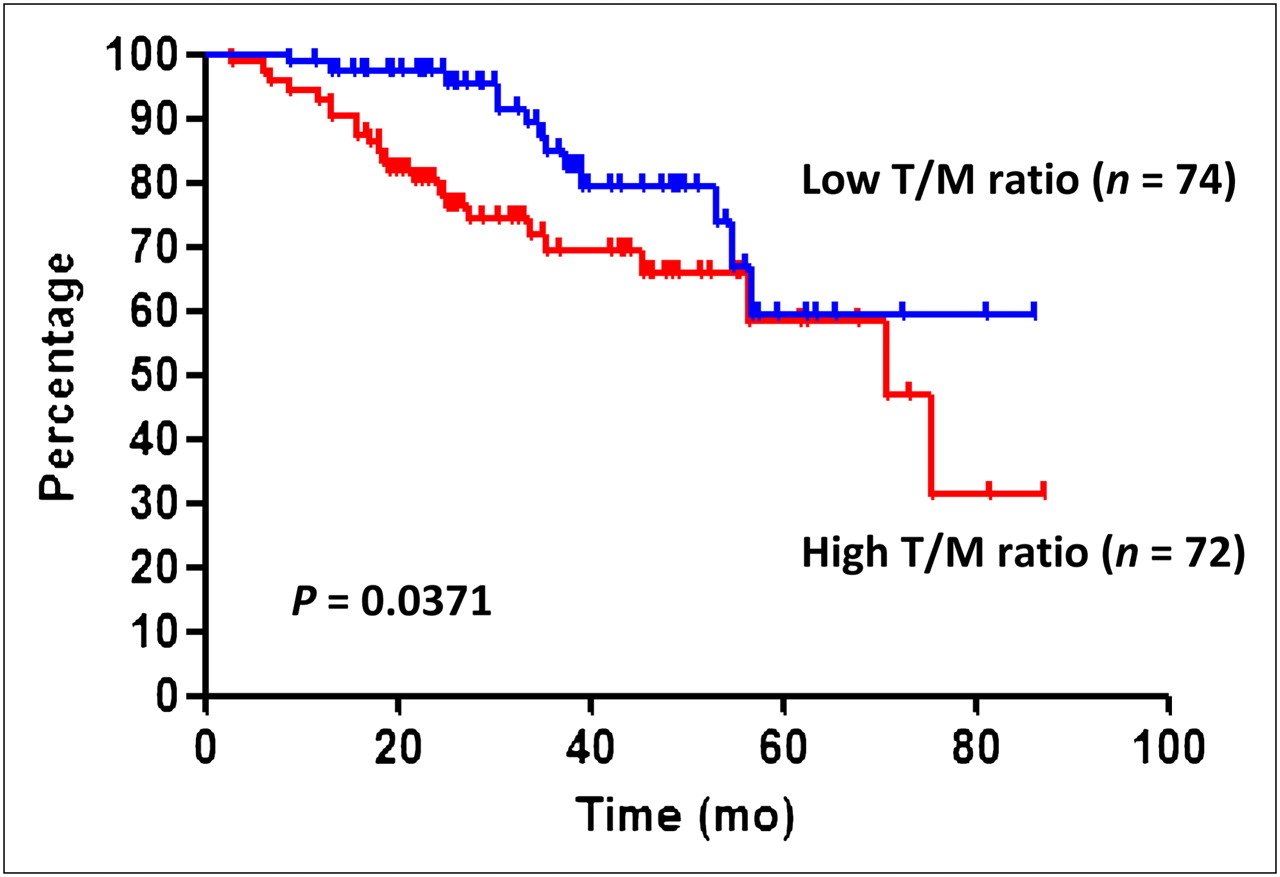
Median survival time for all patients was 75.6 mo, and the 5-y survival rate was 59.3%. The median survival time of patients with a low T/M ratio (≤2.13) was significantly longer than that of patients with a high T/M ratio (>2.13) (P = 0.0371) (Fig. 2).

Overall survival curve according to T/M ratio. Overall survival of patients with high T/M ratio was significantly longer than that of patients with low T/M ratio.
Immunohistochemical Analysis
Glut1, Glut3, hexokinase I, HIF-1α, VEGF, and CD34 immunohistochemical staining were evaluated for the 143 surgically resected pulmonary metastatic sites. Glut1 and Glut3 were detected in tumor cells and localized predominantly on their plasma membrane. A positive rate of Glut1 and Glut3 expression was recognized in 70.5% and 6.8%, respectively. A positive expression of HIF-1α was predominantly expressed in the cytoplasm, with some nuclear staining, and was recognized in 69.9%. A positive expression of hexokinase I was expressed in the cytoplasm or membrane of neoplastic cells and was recognized in 56.8%. The staining pattern of VEGF was uniformly localized in the cytoplasm or membrane. The median rate of VEGF positivity was 22.0% (range, 2%–76%); thus, 22% was chosen as a cutoff point. High expression was recognized in 48.6%. The median number of CD34 was 24 (range, 5–68); thus, 24 was chosen as a cutoff point. High expression of CD34 was seen in 42.5%. The positive rate of these biomarkers according to the primary sites is listed in Table 1. The expression of Glut1 was significantly higher in colon, head and neck, breast, and genital cancers than in sarcoma. The expression of hexokinase I was significantly higher in breast and genital cancers than in sarcoma. The expression of HIF-1α was significantly higher in colon, breast, genital, and gastrointestinal cancers than in sarcoma. The VEGF expression of breast cancer was significantly higher than that of sarcoma. No statistically significant difference in the expression of Glut3 and CD34 was observed among these biomarkers.
In the survival analysis according to these biomarkers, no statistically significant difference was observed in the expression of Glut1, Glut3, hexokinase I, HIF-1α, VEGF, or CD34.
Comparison of 18F-FDG Uptake and Biomarkers Between Pulmonary Metastases and Primary Lung Cancer
Relationship Between 18F-FDG Uptake and Different Variables
The results of the statistical analysis of correlation between T/M ratio and expression of biomarkers are listed in Supplemental Table 2.
Metastatic Pulmonary Tumors.
The T/M ratio correlated significantly with Glut1, hexokinase I, HIF-1α, VEGF, and CD34 using the Spearman rank test. The relationship between T/M ratio and these biomarkers was evaluated according to the histologic type (adenocarcinoma, SQC, and sarcoma); the expression of Glut1, hexokinase I, HIF-1α, and VEGF yielded a positive correlation.
Primary Lung Cancer and Control Group.
The T/M ratio of NSCLC correlated significantly with the expression of Glut1, hexokinase I, HIF-1α, VEGF, and CD34. In the control group, the expression of Glut1 and hexokinase I, but not HIF-1α, VEGF, or CD34, was closely related to 18F-FDG uptake.
Comparison of Metastatic Pulmonary Tumors and Primary Lung Cancer
The T/M ratio and expression of hexokinase I, HIF-1α, and VEGF were significantly higher in primary lung cancer than in metastatic pulmonary tumors, but Glut1 expression was significantly higher in metastatic pulmonary tumors (Table 1). In the analysis of patients with adenocarcinoma, the T/M ratio and Glut3 expression were significantly higher in primary lung cancer than in metastatic pulmonary tumors, but the expression of Glut1, HIF-1α, and CD34 was significantly higher in metastatic pulmonary tumors. In the analysis of patients with SQC, however, only the T/M ratio was significantly higher in primary lung cancer (vs. metastatic pulmonary tumors).
Next, we compared the T/M ratio and these biomarkers between adenocarcinoma and SQC in primary lung cancer. The T/M ratio and expression of Glut1, hexokinase I, HIF-1α, VEGF, and CD34 were significantly higher in SQCs than in adenocarcinoma. Glut3 expression was similar between adenocarcinoma and SQC.
Comparison of Malignant and Benign Lesions
The T/M ratio and expression of Glut1, hexokinase I, HIF-1α, VEGF, and CD34 were significantly higher in patients with primary lung cancer and metastatic pulmonary tumors than in controls (Table 2).
Comparison of 18F-FDG Uptake and Biomarkers Between Malignant Lesions and Benign Lesions
Comparison of 18F-FDG Uptake and Different Variables Among Metastatic Pulmonary Tumors
The T/M ratio and expression of Glut1, HIF-1α, and VEGF were significantly higher in adenocarcinoma and SQC than in sarcoma (Table 3). Glut3 expression was significantly higher in SQC and sarcoma than in adenocarcinoma. The expression of hexokinase I, HIF-1α, VEGF, and CD34 was significantly higher in SQC than in adenocarcinoma.
Comparison of 18F-FDG Uptake and Biomarkers Among Patients with Pulmonary Metastases
18F-FDG Uptake and Biomarkers According to Tumor Size Among Metastatic Pulmonary Tumors
The T/M ratio correlated significantly with tumor size (P < 0.0001), but there was no significant relationship between tumor size and the expression of Glut1, Glut3, hexokinase I, HIF-1α, or CD34. However, a significant correlation between VEGF and tumor size was observed in patients with adenocarcinoma and SQC but not with sarcoma. 18F-FDG uptake correlated significantly with tumor diameters of 10 mm or less (γ = 0.3569, P = 0.0257 [n = 39]) and more than 10 mm (γ = 0.4045, P < 0.0001 [n = 107]). Moreover, we compared lesion size among groups. The resected lesions were significantly larger in patients with NSCLC than in patients with metastatic pulmonary tumors (P = 0.0007) or the control patients (P = 0.0498) and were not significantly different between the metastatic pulmonary tumor and control groups (P = 0.9846).
DISCUSSION
This is the first, to our knowledge, retrospective study to evaluate the biologic correlation of 18F-FDG uptake and expression of biomarkers such as Glut1, Glut3, hexokinase I, HIF-1α, VEGF, and CD34 in metastatic pulmonary tumors, as compared with primary lung cancer and benign pulmonary lesions. The results revealed a statistically significant relationship between 18F-FDG activity and the expression of Glut1, hexokinase I, HIF-1α, VEGF, and MVD in patients with metastatic pulmonary tumors. However, the correlation between 18F-FDG uptake and these biomarkers was weak in patients with metastatic pulmonary tumors, as compared with primary lung cancer, regardless of the histologic subtype. In patients with metastatic pulmonary tumors, 18F-FDG uptake and the expression of Glut1, HIF-1α and VEGF were significantly higher in adenocarcinoma and SQC than in sarcoma. Although 18F-FDG uptake and Glut1 expression were similar between adenocarcinoma and SQC in metastatic pulmonary tumor patients, the expression of hexokinase I, HIF-1α, VEGF, and CD34 was significantly higher in SQC than in adenocarcinoma. In the survival analysis, a high 18F-FDG uptake was closely related to poor outcome after pulmonary metastasectomy. Moreover, 18F-FDG uptake was closely correlated with tumor size in metastatic pulmonary tumor patients with the adenocarcinoma or SQC histologic types.
Glucose metabolism (Glut1 and hexokinase I), hypoxia (HIF-1α), and angiogenesis (VEGF and CD34) have an important role in the mechanism of 18F-FDG uptake not only in patients with primary lung cancer but also in patients with metastatic pulmonary malignancies. The present study indicated that 18F-FDG uptake and these biomarkers were significantly higher in metastatic pulmonary tumors than in benign pulmonary lesions and relatively lower in metastatic pulmonary tumors than in primary lung cancer. However, Glut1 expression was significantly higher in metastatic pulmonary tumors than in primary lung cancer, and the analysis according to histology showed that Glut1 expression was higher in metastatic adenocarcinoma than in primary adenocarcinoma. Recently, the relationship between 18F-FDG uptake and Glut1 expression in metastatic pulmonary tumors was reported (13). In that study, however, only 5 patients with metastatic lesions (1 adenocarcinoma of the lung, 1 SQC of the lung, 1 renal carcinoma, 1 esophageal cancer, and 1 sarcoma) were evaluated by immunohistochemical staining. Because the results were only preliminary, it is unclear whether 18F-FDG uptake in metastatic pulmonary tumors is closely related to the expression of Glut1. Our results indicate that the degree of glucose metabolism, hypoxia, and angiogenesis in metastatic pulmonary tumors is different from that in primary lung cancer; therefore, the role of 18F-FDG PET as a molecular imaging tool may differ between metastatic and primary lung lesions. 18F-FDG uptake on PET images in primary lung cancers, as compared with metastatic lung tumors, seems to be closely associated with glucose metabolism, hypoxia, and angiogenesis.
Pulmonary metastasectomy is an important therapeutic procedure in selected patients with pulmonary metastasis. Outcome after pulmonary metastasectomy is influenced by the completeness of resection. A shorter interval of disease free, lymph nodes positive for tracer uptake and a higher number of metastatic nodules has been described to be associated with poorer outcome after resection (14). However, there are still no data about the prognostic significance of 18F-FDG uptake on PET images of patients with metastatic pulmonary tumors. The present study indicated that high 18F-FDG uptake was significantly associated with poor outcome after pulmonary metastasectomy, and the degree of the biomarkers (Glut1, Glut3, hexokinase I, HIF-1α, VEGF, and CD34) was not directly related to survival. However, it is unclear whether a high accumulation of 18F-FDG is associated with poor outcome after pulmonary metastasectomy; therefore, further study is warranted.
In the analysis according to the histologic subtype of metastatic pulmonary tumors, 18F-FDG uptake and Glut1 expression, which were similar between adenocarcinoma and SQC, were significantly lower in sarcoma than in adenocarcinoma or SQC. In primary lung cancer, a previous report demonstrated that 18F-FDG uptake in adenocarcinoma was lower than that in SQC (13), corresponding to the results of our study. Because the degree of glucose metabolism, hypoxia, and angiogenesis in primary lung cancer was higher in SQC than in adenocarcinoma, 18F-FDG uptake in SQC may be higher than that in adenocarcinoma, whereas in metastatic pulmonary tumors, no statistically significant difference in 18F-FDG uptake was observed between adenocarcinoma and SQC. Although hypoxia and angiogenesis were higher in SQC, the degree of 18F-FDG activity may be dependent on the expression of Glut1 in patients with metastatic pulmonary tumors. Moreover, the low uptake of 18F-FDG uptake in sarcoma may have resulted from the low degree of glucose metabolism, hypoxia, and angiogenesis. Recently, Reinhardt et al. analyzed the SUVmax of 168 pulmonary metastases according to the primary tumor site and described an SUVmax of sarcoma that was significantly lower than that of colon cancer (15). Our results also demonstrated that 18F-FDG uptake and Glut1 expression were significantly higher in colon cancer than in sarcoma. In their report, however, the primary tumors were melanoma for 82 patients, sarcoma for 34, head and neck cancer for 25, lymphoma for 10, colon cancer for 7, and others for 10, and the profile of the primary sites was different from that of our study. Moreover, Reinhardt et al. (15) had not investigated the analysis according to histologic types and the biologic correlation of 18F-FDG uptake.
The analysis of 438 metastatic pulmonary lesions revealed that no nodules smaller than 5 mm were positive on 18F-FDG PET, but the nodules greater than 13 mm had a sensitivity of 100% (15). 18F-FDG PET sensitivity had been also described to be significantly reduced for lesions with a diameter less than 11 mm. In the present study, a diameter greater than 10 mm was observed in 107 (73%) of 146 metastatic pulmonary nodules. The tumor size correlated closely with 18F-FDG uptake, and the correlation in metastatic nodules with a diameter of greater than 10 mm seemed to be stronger than in those with a diameter of 10 mm or less. Our results suggest that VEGF expression plays an important role in the relationship between 18F-FDG uptake and tumor size, especially in metastatic pulmonary tumor patients with adenocarcinoma or SQC. Although tumor size correlated significantly with 18F-FDG uptake, tumor size did not correlate significantly with these biomarkers, excluding VEGF. In the present study, the mean lesion size was relatively small; thus, partial-volume effects might confound the relationship between 18F-FDG uptake and tumor size and between these biomarkers and tumor size, even in lesions larger than 10 mm. This is one of our study limitations.
SUV varies with many factors, such as the interval between tracer injection and the start of the scan, the blood glucose level, and the SUVmax of the background, with significant statistical error being possible. Therefore, in recent studies18F-FDG uptake within primary tumors has been evaluated not by SUVmax but by T/M ratio (4,16). In the present study, both a PET scanner and a PET/CT scanner were used, and the SUVmax may differ between the PET machines. Thus, 18F-FDG uptake for both PET scanners was normalized using T/M ratio, as compared with the absolute SUVmax, to evaluate the exact correlation between 18F-FDG uptake on PET and these biomarkers in pulmonary lesions.
CONCLUSION
The amount of 18F-FDG uptake in metastatic pulmonary tumors was determined by the presence of glucose metabolism (Glut1 and hexokinase I), hypoxia (HIF-1α), and angiogenesis (VEGF and CD34). The relationship between 18F-FDG uptake and these biomarkers was weak in patients with metastatic pulmonary tumors, as compared with primary lung cancer. 18F-FDG uptake in metastatic pulmonary tumors was significantly higher than in benign pulmonary diseases but lower than in primary lung cancer. In patients with metastatic pulmonary tumors, 18F-FDG uptake in sarcoma was lower than that in adenocarcinoma and SQC, possibly resulting from the low expression of Glut1, HIF-1α, and VEGF. A high 18F-FDG uptake was associated with poor outcome after pulmonary metastasectomy, and tumor size correlated closely with 18F-FDG uptake in adenocarcinoma or SQC but not sarcoma. Because metastatic pulmonary tumor is a heterogeneous group of thoracic malignancies, it may be questionable whether 18F-FDG uptake within tumor cells could exactly reflect the prognostic significance after pulmonary metastasectomy and the differential diagnosis between primary lung cancer and benign pulmonary lesions. These features explain why metastatic pulmonary malignancies vary in 18F-FDG uptake and elucidate the relatively low uptake in patients with sarcoma. The relationship between 18F-FDG uptake and these biomarkers may lead to a more rational use of PET scanning in patients with metastatic pulmonary tumors.
DISCLOSURE STATEMENT
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734.
Acknowledgments
We thank the staff of the pathology department at Shizuoka Cancer Center for their technical assistance in immunohistochemical analysis. This work was supported in part by grant 21790793 from the Ministry of Education, Culture, Sports, Science and Technology, Japan, and the National Hospital Organization Policy Based Medical Services.
- © 2011 by Society of Nuclear Medicine
REFERENCES
- Received for publication January 8, 2011.
- Accepted for publication February 16, 2011.





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Is FDG-PET/CT Useful for Diagnosing Pulmonary Metastasis in Patients with Soft Tissue Sarcoma?
- Resveratrol Suppresses Cancer Cell Glucose Uptake by Targeting Reactive Oxygen Species-Mediated Hypoxia-Inducible Factor-1{alpha} Activation
- Heterogeneity in Intratumor Correlations of 18F-FDG, 18F-FLT, and 61Cu-ATSM PET in Canine Sinonasal Tumors
- Multifunctional Profiling of Non-Small Cell Lung Cancer Using 18F-FDG PET/CT and Volume Perfusion CT