


Abstract
Our objective was to compare the predictive significance of 18F-FDG PET/CT findings and circulating tumor cell (CTC) count in patients with bone metastases from breast cancer treated with standard systemic therapy. Methods: Breast cancer patients with progressive bone-only metastatic disease without visceral metastases starting a new line of systemic therapy underwent 18F-FDG PET/CT and had CTC counts determined before and during treatment. Disease status was reassessed by CTC count (≥5 vs. <5 CTC/7.5 mL of blood) and 18F-FDG PET/CT approximately 2–4 mo after initiation of the new systemic therapy. Results: CTC counts at follow-up agreed with the 18F-FDG PET/CT assessment in 43 (78%) of the 55 evaluable patients. Of the 12 patients with discordant CTC and 18F-FDG PET/CT results, 8 (66%) had ≥5 CTCs, with no evidence of progressive disease at the time of the 18F-FDG PET/CT study, whereas 4 (33%) had <5 CTCs, with evidence of progressive disease by 18F-FDG PET/CT. 18F-FDG PET/CT findings and follow-up CTC counts were found to be significantly associated with both progression-free survival (P = 0.02 and P < 0.0001, respectively) and overall survival (P = 0.02 and P = 0.01, respectively). In multivariate analysis, the 18F-FDG PET/CT assessment remained as the only predictive factor for progression-free survival (P < 0.0001), whereas estrogen receptor status was the only predictive factor for overall survival (P = 0.01). Conclusion: 18F-FDG PET/CT is a useful tool for therapeutic monitoring in patients with bone metastases from breast cancer. Prospective studies are needed to define the role of 18F-FDG PET/CT and CTC in the setting of response discordance to establish bone-dominant disease as a tumor-response measurable disease.
Bone metastases occur during the course of metastatic breast cancer (MBC) in nearly two thirds of patients and represent the first site of metastasis in about one third of patients (1–4). Patients with bone metastases from breast cancer have a life expectancy of several years, and both local (radiotherapy and surgery) and systemic (hormone therapy, chemotherapy, trastuzumab, and bisphosphonates) modalities are available to treat bone metastases (5). How best to monitor the response of bone metastases from breast cancer to systemic therapy represents a critical issue in clinical practice and in phase II–III trials.
Both 18F-FDG PET/CT and circulating tumor cell (CTC) counts have been studied in patients with bone metastases from breast cancer. 18F-FDG PET/CT is more sensitive than conventional imaging for detecting MBC (6) and has improved anatomic correlations, resulting in more accurate measurement of bone metastases in MBC (7,8). The presence of CTC before treatment is an independent predictor of progression-free survival (PFS) and overall survival (OS) in patients with MBC (9). 18F-FDG PET/CT and CTC measurement showed a high sensitivity in the detection of bone relapse or progression of breast cancer (6,10), and we previously found that the presence of extensive bone metastases as detected by 18F-FDG PET/CT was associated with increased CTC numbers in MBC (10). Specifically, we showed that CTC numbers were higher in patients with bone metastases than in those with no bone lesions (mean, 65.7 vs. 3.3, P = 0.0122) and higher in patients with 3 or more bone metastases than in those with fewer bone lesions (mean, 77.7 vs. 2.6, P < 0.001) (10). Furthermore, we found that CTC counts were lower in patients with lymph node or chest wall metastases without bone lesions (mean, 1.4 ± 2.0 CTCs) (10).
In this study, we sought to determine the predictive significance of CTC counts and 18F-FDG PET/CT findings in patients with bone metastases from breast cancer treated with standard systemic therapies. We also sought to determine the correlation between CTC counts and 18F-FDG PET/CT findings in such patients.
MATERIALS AND METHODS
Patients
This study was conducted using the MD Anderson Cancer Center Breast Medical Oncology database. We identified all patients who had received systemic treatment for bone metastases from breast cancer—including patients with intrathoracic lymph node or chest wall metastases in addition to bone metastases—from December 2004 to May 2008. Patients with visceral metastases were excluded. All patients underwent 18F-FDG PET/CT scans and CTC enumeration within 3 wk before starting a new treatment as the standard of care. Metabolically active disease by 18F-FDG PET/CT was identified in all patients. Disease status was reassessed by 18F-FDG PET/CT and CTC count at approximately 2–4 mo after the initiation of the new systemic treatment, depending on treatment type and schedule. Fifty-five patients met these criteria and were included in the study. The retrospective protocol was approved by the Institutional Review Board of the MD Anderson Cancer Center, with a waiver of the requirement for informed consent.
Response Evaluation by 18F-FDG PET/CT
18F-FDG PET/CT scans were obtained using a multislice PET/CT camera (Discovery ST, STE, or RX, with 8-, 16-, or 64-slice CT; GE Healthcare) using a standard clinical protocol (11). PET and CT images were reconstructed and reviewed on an Advantage workstation (GE Healthcare). In a region of interest, only the lesions that exhibited the most substantial 18F-FDG uptake were selected as the target lesions for evaluating response to therapy.
There is no accepted standard for 18F-FDG PET/CT response for bone metastases from breast cancer; however, progressive disease (PD) versus nonprogressive disease (non-PD) has been validated as a predictor of survival in patients with MBC, including patients with bone metastases, and showed a 75% overall agreement with CTC counts in a previous study (12). Thus, in the current study, increased 18F-FDG uptake in a target lesion that was also enlarged on CT (i.e., ≥20% increase in the longest diameter) or a new metabolically active lesion was considered indicative of PD, whereas substantially unchanged or decreased 18F-FDG uptake without substantial increase in lesion size was considered indicative of non-PD. Because progressive sclerosis on CT is also a marker of response in bone metastases, the increase of bone lesions without a clear evidence of 18F-FDG uptake has not been considered indicative of progression.
Detection and Enumeration of CTC
The CellSearch System (Veridex LLC) was used for the enumeration of CTCs (13). Blood samples were collected and CTCs enumerated as previously described (9). Patients were categorized according to CTC counts as having a favorable (<5 CTC/7.5 mL of blood) or unfavorable (≥5 CTC/7.5 mL of blood) outcome of systemic therapy (9).
Statistical Analysis
PFS was defined as the time elapsed between the date of baseline CTC blood sampling and the date of clinical disease progression or death or, if neither progression nor death occurred during follow-up, the date of the last follow-up visit. OS was defined as the time elapsed between the date of baseline CTC blood sampling and the date of either death or, if death did not occur during the follow-up period, the last follow-up visit. Student t and Fisher exact tests were used to test for statistically significant differences between the patients with <5 CTCs/7.5 mL of blood and those with ≥5 CTC/7.5 mL of blood. Kaplan–Meier survival plots were generated by CTC count and 18F-FDG PET/CT assessment (non-PD or PD), and the curves were compared using log-rank testing. Cox proportional hazards regression was used to test the statistical significance of selected potential prognostic factors for PFS and OS. A P value of less than 0.05 was considered statistically significant.
RESULTS
Patient Characteristics
Between December 30, 2004, and May 31, 2008, 55 patients received systemic therapies for either bone metastases only (n = 26) or bone metastases and intrathoracic lymph node or chest wall metastases (n = 29) and underwent both CTC and PET/CT evaluation. Thirty-six patients (65%) had received prior treatment for MBC with hormone therapy (23 cases), chemotherapy with or without hormone therapy (9 cases), or HER2-targeted therapies combined with chemotherapy or hormone therapy (4 cases). Nineteen patients (35%) had newly diagnosed MBC. The clinical characteristics of the 55 patients evaluated are summarized in Table 1. In this cohort, 36 patients (65%) at baseline and 22 patients (40%) at follow-up had ≥5 CTC/7.5 mL of blood. The median CTC count per 7.5 mL of blood was 13 (range, 0–694) at baseline and 3 (range, 0–760) at follow-up. The average time ± SD between baseline and follow-up blood sampling was 16.9 ± 9.1 wk (range, 4.3–38.7 wk) and between baseline and follow-up 18F-FDG PET/CT was 16.9 ± 8.3 wk (range, 8.1–35.7 wk).
Clinical Characteristics of Study Population (n = 55)
Relationship Between CTC Count and Disease Progression as Determined by 18F-FDG PET/CT
CTC count at follow-up (<5 CTC/7.5 mL of blood or ≥5 CTC/7.5 mL of blood) agreed with 18F-FDG PET/CT assessment (non-PD or PD) in 43 patients (78%). Among the remaining 12 patients, 4 (33%) with fewer than 5 CTCs at follow-up were found to have evidence of PD by 18F-FDG PET/CT, whereas 8 (67%) with persistent CTCs (≥5) at follow-up did not.
Among the 4 patients with <5 CTCs at follow-up and PD by 18F-FDG PET/CT, 3 had <5 CTCs at baseline and received chemotherapy only (2 cases) or chemotherapy plus trastuzumab (1 case); 1 patient had a baseline CTC count of 262 CTC/7.5 mL of blood that was undetectable (CTC = 0), despite PD with liver metastases after 5 mo of hormone therapy.
Among the 8 patients with a persistence of ≥5 CTCs at follow-up without evidence of PD by 18F-FDG PET/CT, 5 patients had impending tumor progression at a median follow-up of 56 d (range, 24–92 d), 1 experienced PD after 7 mo, and 2 remained progression-free at 24 and 36 mo. The latter 2 patients received chemotherapy in addition to hormone therapy. Among the 6 patients with evidence of PD by 18F-FDG PET/CT, 5 patients—including 4 with estrogen receptor (ER)–positive tumors—were treated with chemotherapy only and the sixth was treated with chemotherapy in addition to hormone therapy.
CTC and 18F-FDG PET/CT Ability to Predict Survival
In all 55 patients, the mean PFS was 10.5 ± 7.2 mo (range, 1.9–33.8 mo), and the mean OS was 18.1 ± 6.7 mo (range, 3.1–36.8 mo). At the time of analysis, 7 patients (13%) were considered progression-free—with an average follow-up time of 18.0 ± 8.3 mo (range, 10.0–33.8 mo)—and 18 patients (33%) had died.
Follow-up CTC count (<5 CTC/7.5 mL of blood or ≥5 CTC/7.5 mL of blood) and 18F-FDG PET/CT assessment (non-PD or PD) were found to be significantly associated with both PFS (P = 0.02 and P < 0.0001, respectively) and OS (P = 0.02 and P = 0.01, respectively). The baseline CTC count was not a significant predictor for either PFS (P = 0.78) or OS (P = 0.74).
Median PFS was 13 mo in patients with both <5 CTCs and 18F-FDG PET/CT nonprogression, 6 mo in patients with <5 CTCs or 18F-FDG PET/CT nonprogression but not both, and 5 mo in patients with neither <5 CTCs nor 18F-FDG PET/CT nonprogression (P < 0.00002). Median OS was not reached (>31 mo) in patients with both <5 CTCs and 18F-FDG PET/CT nonprogression, was 24 mo in patients with <5 CTCs or 18F-FDG PET/CT nonprogression but not both, and was 18 mo in patients with neither <5 CTC nor 18F-FDG PET/CT nonprogression (P = 0.02).
Tables 2 and 3 summarize factors associated with PFS and OS estimates, respectively. Follow-up CTC counts and 18F-FDG PET/CT assessment (PD vs. non-PD) were significantly associated with PFS (Fig. 1), but 18F-FDG PET/CT assessment remained significant only in a multivariate analysis (Table 2). ER status was significantly associated with OS (Fig. 2) and was the only variable that remained significant in a multivariate analysis (Table 3).
Factors Associated with PFS
Factors Associated with OS
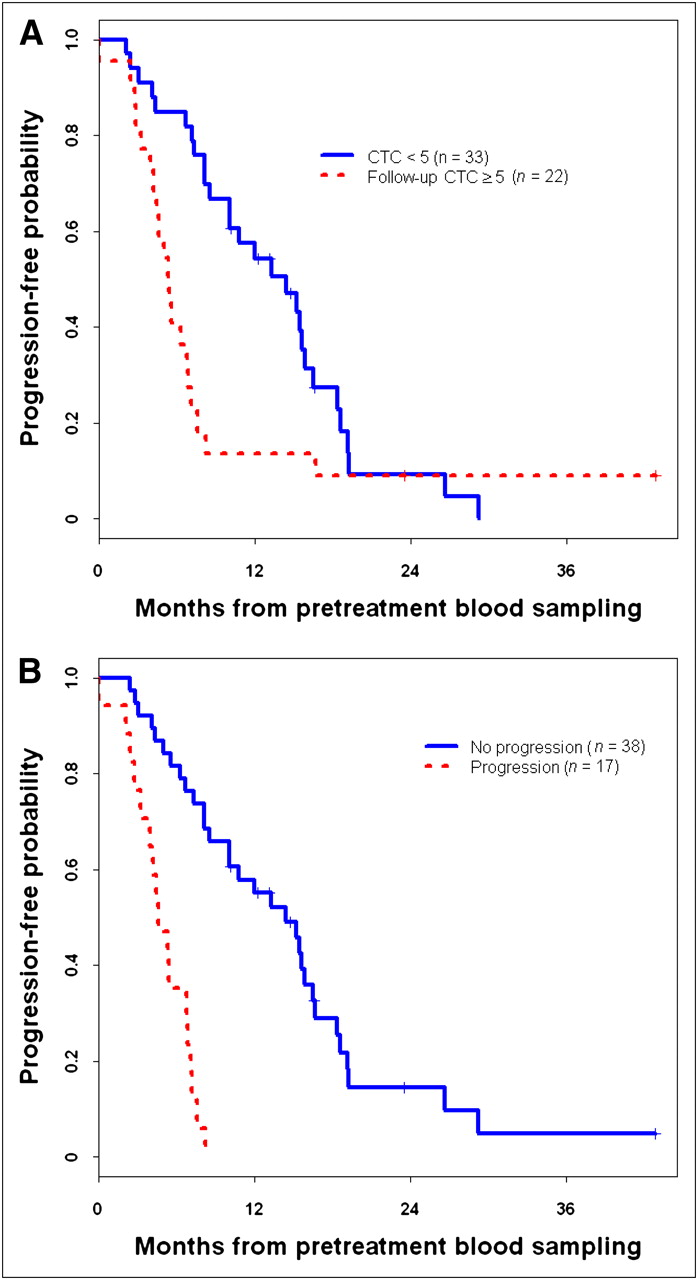
Kaplan–Meier estimates of PFS by follow-up CTC count (A) and 18F-FDG PET/CT response (B). (A) For patients with follow-up CTC count < 5: patients at risk = 33 at 0 mo, 17 at 12 mo, and 2 at 24 mo and survival rate = 100% at 0 mo, 54% at 12 mo, and 14% at 24 mo. For patients with follow-up CTC count > 5: patients at risk = 22 at 0 mo, 3 at 12 mo, 1 at 24 mo, and 1 at 36 mo and survival rate = 100% at 0 mo, 14% at 12 mo, 8% at 24 mo, and 8% at 36 mo. (B) For 18F-FDG PET/CT nonprogression patients: patients at risk = 38 at 0 mo, 20 at 12 mo, 3 at 24 mo, and 1 at 36 mo and survival rate = 100% at 0 mo, 55% at 12 mo, 17% at 24 mo, and 6% at 36 mo. For 18F-FDG PET/CT progression patients: patients at risk = 17 at 0 mo and 6 at 6 mo and survival rate = 100% at 0 mo and 35% at 6 mo.
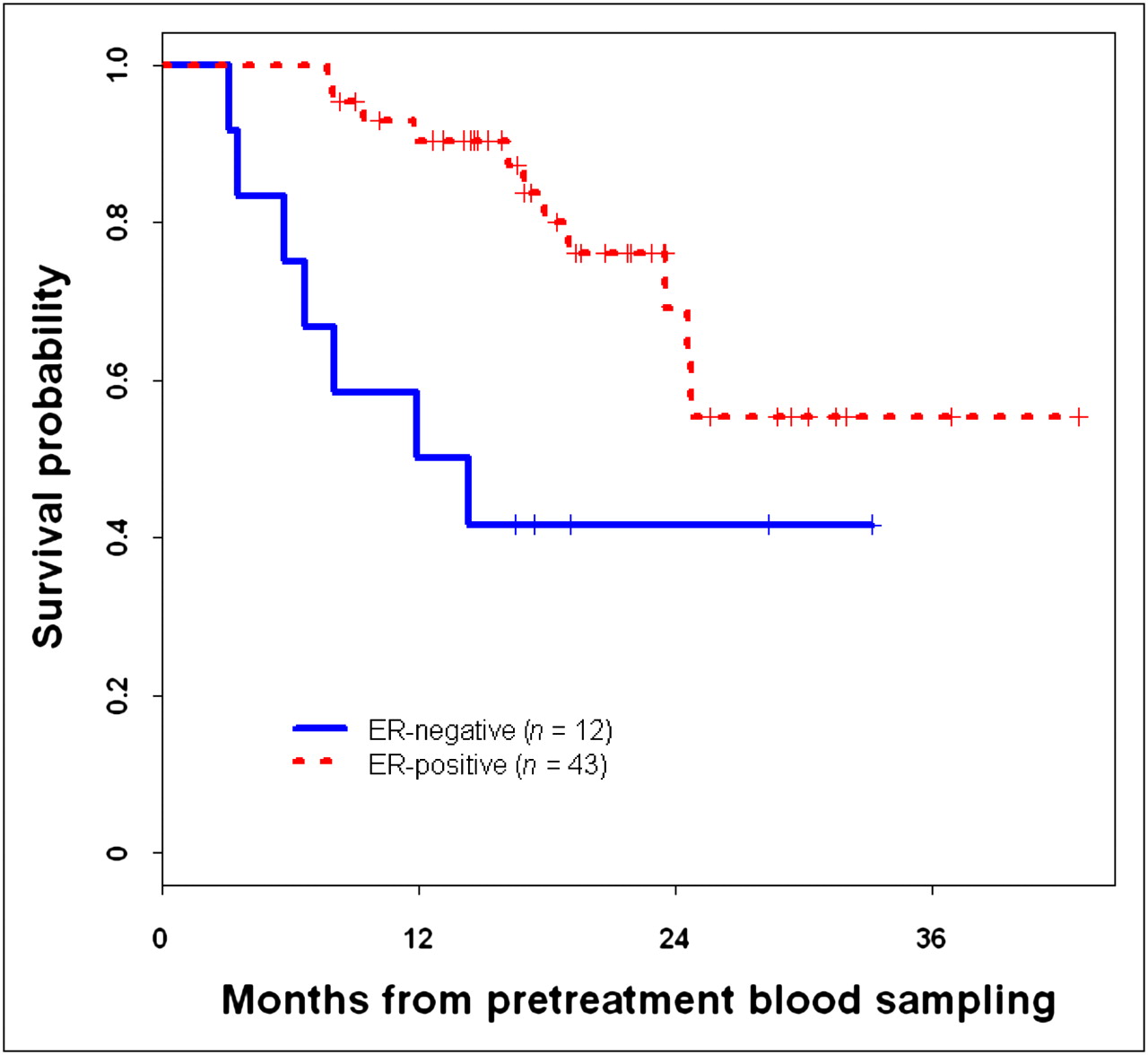
Kaplan–Meier estimates of OS by ER status. For ER-negative patients: patients at risk = 12 at 0 mo, 6 at 12 mo, and 2 at 24 mo and survival rate = 100% at 0 mo, 50% at 12 mo, and 39% at 24 mo. For ER-positive patients: patients at risk = 43 at 0 mo, 36 at 12 mo, 10 at 24 mo, and 2 at 36 mo and survival rate = 100% at 0 mo, 90% at 12 mo, 73% at 24 mo, and 52% at 36 mo.
DISCUSSION
The therapeutic monitoring of bone metastases from breast cancer represents a critical issue in clinical practice and experimental trials. Results of the present study showed that follow-up CTC levels and 18F-FDG PET/CT assessment (PD vs. non-PD) are significantly associated with both PFS and OS. However, in multivariate analysis, 18F-FDG PET/CT assessment (PD vs. non-PD) remained the only predictive factor for PFS, whereas ER status remained the only predictive factor for OS. In addition, CTC counts at follow-up agreed with the 18F-FDG PET/CT assessment in 43 (78%) of the 55 patients. Of the 12 patients with discordant CTC and 18F-FDG PET/CT results, 8 patients (66%) had a persistence of ≥5 CTCs. Interestingly, among these 8 patients, 5 hormone receptor–positive patients treated with chemotherapy only (n = 4) or chemotherapy and hormone therapy (n = 1) experienced impending tumor progression, with a median follow-up of 56 d (range, 24–92 d). Two hormone receptor–positive patients treated with chemotherapy and hormone therapy were progression-free at 24 and 36 mo. Finally, follow-up CTC count was significantly associated with PFS (Fig. 1), whereas ER status was significantly associated with OS (Fig. 2).
Our study had some limitations. It was retrospective, with patients under different systemic therapies. However, these data indicate that 18F-FDG PET/CT could be useful for monitoring response to systemic therapies in patients with bone metastases, even if a role for CTC cannot be excluded in selected cases. Moreover, several authors have previously reported ER expression, HER2 gene amplification, and other markers by CTC, despite the lack of expression or gene amplification in the primary tumor (14–16). Further molecular characterization of CTC might help to select effective targeted therapies, monitor their efficacy, and improve knowledge about the biology of bone metastases from breast cancer.
In addition, our results confirm a possible relationship between high levels of CTC and extensive bone involvement as detected by 18F-FDG PET/CT in patients with relapsed or progressive MBC. In our series, which included patients with MBC with bone metastases but not visceral metastases, 5 or more CTCs were evident in 65% of patients at baseline and 40% at follow-up. In contrast, in other series with unselected patients with MBC, 5 or more CTCs were apparent in 45%–50% of patients at baseline and 25%–30% at follow-up (9,16). Other reports also showed that CTC counts both at baseline and at follow-up were higher in patients with MBC with bone metastases than in patients with MBC in general, using either bone scanning or 18F-FDG PET/CT (10,17). In contrast, in all early and 1 recent prospective study on CTC in MBC, bone metastases were studied with standard imaging techniques. Because patients with bone metastases were included in a generic no-visceral-metastases group, the effect of bone metastases on CTC levels could have been underestimated; the inclusion of patients with bone metastases could help explain the poor survival rates in these early trials for patients with nonvisceral disease (9,18–20). A major limitation of the use of CTC counts for therapeutic monitoring in patients with MBC is that nearly 50% of such patients do not have increased levels of CTC at progression (9); however, CTC counts seemed higher in MBC cases with bone metastases. Moreover, the PET classification of response that we used (non-PD vs. PD) might be optimized, and such optimization might lead to a better predictive value of 18F-FDG PET/CT with respect to PFS and OS (7,8,12). The integrated use of 18F-FDG PET/CT and CTC might lead to a significant improvement in monitoring the response of bone metastases from breast cancer to systemic therapy, and this should be prospectively investigated.
CONCLUSION
To our knowledge, this is the first study to assess the role of 18F-FDG PET/CT and CTC counts in the therapeutic monitoring of bone metastases in patients with breast cancer. The multivariate analysis indicated that 18F-FDG PET/CT was the only predictive sign; however, the combination of FDG PET/CT and CTC might be a useful tool to monitor response to therapy in patients without measurable extraosseous disease, especially in patients with elevated CTC at baseline. The discordance of 18F-FDG PET/CT assessment and CTC count needs to be evaluated in a prospective study to determine the value of 18F-FDG PET/CT and CTC individually and in combination. A prospective study could validate the benefit of these 2 approaches used separately and in combination in determining prognosis, monitoring response, and establishing bone-dominant disease as a tumor response–measurable disease.
Acknowledgments
We thank Stephanie P. Deming (Department of Scientific Publications, The University of Texas MD Anderson Cancer Center) for editorial assistance. This study was funded in part by a grant from the State of Texas Rare and Aggressive Breast Cancer Research Program. This research was supported in part by the National Institutes of Health through MD Anderson Cancer Center Support Grant CA016672 and by the Nellie B. Connally Breast Cancer Research Fund.
- © 2010 by Society of Nuclear Medicine
REFERENCES
- Received for publication February 17, 2010.
- Accepted for publication April 20, 2010.





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Impact of FDG PET Imaging for Expanding Patient Eligibility and Measuring Treatment Response in a Genome-Driven Basket Trial of the Pan-HER Kinase Inhibitor, Neratinib
- Prospective Study of Serial 18F-FDG PET and 18F-Fluoride PET to Predict Time to Skeletal-Related Events, Time to Progression, and Survival in Patients with Bone-Dominant Metastatic Breast Cancer
- Circulating Tumor DNA Reflects Tumor Metabolism Rather Than Tumor Burden in Chemotherapy-Naive Patients with Advanced Non-Small Cell Lung Cancer: 18F-FDG PET/CT Study
- Imaging Bone Metastases in Breast Cancer: Staging and Response Assessment
- Microtube Device for Selectin-Mediated Capture of Viable Circulating Tumor Cells from Blood
- 18F-FDG PET/CT Predicts Survival After Radioembolization of Hepatic Metastases from Breast Cancer
- Circulating Tumor Cells and PET