


Abstract
The primary aim of this study was to use serial 18F-3′-deoxy-3′-fluorothymidine (FLT) PET/CT to measure tumor cell proliferation during radiotherapy of squamous cell carcinoma (SCC) of the esophagus. Methods: Twenty-one patients with inoperable locally advanced SCC of the esophagus underwent serial 18F-FLT PET/CT during radiotherapy. Each patient received a pretreatment scan, followed by 1–3 scans after delivery of 2, 6, 10, 20, 30, 40, 50, or 60 Gy to the tumor. Results: Among the 19 patients who completed radiotherapy without interruption, parameters reflecting 18F-FLT uptake in the tumor (i.e., maximum tumor standardized uptake value [SUVmax] and proliferation target volume) decreased steadily. All patients demonstrated an almost complete absence of proliferating esophageal tumor after 30 Gy and a complete absence after 40 Gy. In the 2 patients whose radiotherapy course was interrupted, 18F-FLT uptake in the tumor was greater after the interruption than before the interruption. Marked early reduction of 18F-FLT uptake in irradiated bone marrow was observed in all patients, even after only 2 Gy. All showed a complete absence of proliferating marrow in irradiated regions after 10 Gy. Both patients who underwent scans after completing the entire radiotherapy course showed no tumor uptake on 18F-FLT PET/CT but high uptake on 18F-FDG PET/CT. Pathologic examination of these regions revealed inflammatory infiltrates but no residual tumor. Conclusion: 18F-FLT uptake can be used to monitor the biologic response of esophageal SCC and normal tissue to radiotherapy. Increased uptake of 18F-FLT after treatment interruptions may reflect accelerated repopulation. 18F-FLT PET/CT may have an advantage over 18F-FDG PET/CT in differentiating inflammation from tumor.
Radiotherapy plays an important role in the treatment of locally advanced esophageal cancer. With definitive chemoradiation, however, 2-y survival is only 30%−40% and locoregional failure 50%, even with high doses of radiation (1,2). Treatment effectiveness may be limited by accelerated repopulation of clonogenic tumor cells, which can be stimulated by therapeutic interventions such as radiotherapy and which has been shown to contribute to radiation resistance in several malignancies, such as squamous cell carcinoma (SCC) of the head and neck. Analysis by Kajanti et al. (3) investigating the effect of overall treatment time on local control in radical radiotherapy for SCC of the esophagus suggested that because of repopulation, shortening of overall treatment time could be beneficial.
The development of 18F-3′-deoxy-3′-fluorothymidine (FLT) as a PET tracer has enabled in vivo demonstration of cell proliferation (4). 18F-FLT is a pyrimidine analog that, after uptake into the cell, is phosphorylated by thymidine kinase 1 into 18F-FLT monophosphate, causing intracellular sequestration of radioactivity. Thymidine kinase 1 is a principal enzyme in the salvage pathway of DNA synthesis and exhibits increased activity during the S phase of the cell cycle. 18F-FLT uptake, therefore, reflects cellular proliferation. A strong correlation has been demonstrated between 18F-FLT uptake and proliferation rate as measured by the Ki-67 index (5–8).
The primary aim of this study was to use serial 18F-FLT PET/CT scans to evaluate tumor cell proliferation during radiotherapy of esophageal SCC. We also investigated the effects of radiotherapy on bone marrow proliferation and compared the efficacy of 18F-FLT PET with that of 18F-FDG PET in differentiating residual tumor from inflammation.
MATERIALS AND METHODS
Patients
Between February and September 2009, 21 consecutive inoperable patients with SCC of the esophagus at Shandong Cancer Hospital and Institute were accrued to this study. Patients were eligible if they had stage I–IV histologically proven SCC of the esophagus, Eastern Cooperative Oncology Group performance status 0–1, and the ability to undergo serial PET/CT. Exclusion criteria included prior thoracic radiotherapy or complete macroscopic excision of the tumor. Patients were treated in accordance with our current clinical guidelines and received concurrent chemoradiotherapy, sequential chemotherapy and radiation, or radiotherapy alone. Three patients receiving concurrent chemoradiotherapy were participants in Erbitux Combined with Chemo-Radiotherapy in Esophageal Squamous Cell Carcinoma (EXCEL), a clinical trial investigating concurrent administration of cetuximab, paclitaxel, and cisplatin with radiotherapy.
Radiotherapy delivered 60 Gy in 30 fractions over 6 wk, using 6- or 15-MV photons in 3-dimensional conformal radiotherapy or conventional plans. Concomitant or sequential chemotherapy consisted of cisplatin (75 mg/m2, day 1) and 5-fluorouracil (1,000 mg/m2/24 h by continuous infusion on days 1 through 4). Patients in the EXCEL trial received cetuximab (400 mg/m2 on day 1 of week 1, followed by 250 mg/m2 on day 1 of weeks 2–8), paclitaxel (45 mg/m2 on day 1 of weeks 2–8), and cisplatin (20 mg/m2 on day 1 of weeks 2–8).
All patients gave written informed consent. The study protocol was approved by the Medical Ethics Committee of the Shandong Cancer Hospital and Institute.
Radiopharmaceuticals
18F-FLT was synthesized by a cyclotron (MiniTrace; GE Healthcare) and synthesizer (TracerLab FxFN; GE Healthcare). Raw materials and agents for the synthesis were purchased from the same supplier. 18F-FLT was synthesized according to the method of Machulla et al. (9). 18F-FLT was produced by fluorination with 18F-fluoride of the 4,40-dimethoxytrityl–protected anhydrothymidine, followed by a deprotection step. After purification by reversed-phase high-performance liquid chromatography, the product was made isotonic and passed through a 0.22-μm filter. Labeling yield, radiochemical purity, and specific radioactivity of the products were checked and recorded after each production. The products had to meet prespecified criteria (e.g., radiochemical yield > 10% and radiochemical purity > 95%) to qualify for use in imaging.
Imaging Protocol
The patients fasted for 6 h and rested for 15 min before administration of 300–400 MBq of radioactive tracer. After receiving the injection, the patients drank 500 mL of water for optimal hydration and to stimulate excretion of 18F-FLT. PET/CT scans were acquired 50–60 min after injection. Scanning was performed in partial-body mode from the seventh cervical vertebra to the abdomen, for 2 min per bed position. The axial field of view covered 14.5 cm, with an axial sampling thickness of 4.25 mm per slice. Images were reconstructed using an iterative technique and were interpreted on Xeleris workstations (GE Healthcare) by an experienced nuclear medicine radiologist. Maximum tumor standardized uptake value (SUVmax) and proliferation target volume were measured by a clinical investigator and an experienced nuclear medicine specialist. Because our previous study on 18F-FLT PET/CT identified an SUVmax cutoff of 1.4 as providing the closest estimate of gross tumor volume for esophageal cancer (10), regions of interest were drawn around tumor volumes with an SUVmax greater than 1.4 to create the proliferation target volume.
Timing of Scans
Baseline 18F-FLT PET/CT scans were obtained within 3 d before commencement of treatment (tumor dose [TD], 0 Gy). Patients continued on the study even if 18F-FLT was not visible on the baseline scan to explore whether lesions initially undetectable by 18F-FLT might become visible during radiotherapy because of accelerated repopulation. Each patient was scheduled to have 2–4 scans during the treatment delivery period, with the TD at the time of imaging indicated in Table 1; on-treatment 18F-FLT PET/CT scans were obtained at a TD of 2, 6, 10, 20, 30, 40, 50, or 60 Gy (i.e., after radiotherapy) to provide a range of TD points for assessment of cell proliferation. Scanning at TDs of 2 and 6 Gy was designed to capture information on initial DNA damage. Scanning at TDs of 10 and 20 Gy was intended to evaluate early response to treatment. Scanning at TDs of 30, 40, or 50 Gy was intended to explore ongoing tumor response and the possibility of accelerated repopulation recommencing later in the treatment course. The postradiotherapy scans were intended to compare 18F-FLT PET/CT with 18F-FDG PET/CT with regard to their ability to differentiate residual tumor from inflammation.
Patient Characteristics
RESULTS
Patient characteristics are summarized in Table 1. The median time between injection of 18F-FLT and initiation of the emission scan was 56 min (range, 52–82 min). In all patients, intense physiologic 18F-FLT uptake was seen in bone marrow (reflecting active cellular proliferation), liver (because of glucuronidation of 18F-FLT), and urinary tract (demonstrating renal clearance). 18F-FLT uptake was seen in all primary lesions and lymph node metastases on pretreatment scans except in patient 5, who showed tumoral 18F-FLT uptake similar to background activity. This patient had received 3 cycles of induction chemotherapy with paclitaxel and fluorouracil before radiotherapy (Fig. 1). The mean SUVmax of the primary esophageal tumor was 9.7 (range, 1.1–15.2), and the mean proliferation target volume was 21.9 cm3 (range, 0–34.8 cm3). The mean SUVmax of lymph node metastases was 4.6 (range, 3.4–8.5), and the mean proliferation target volume was 11.2 cm3 (range, 3.2–21.6 cm3).

This patient had induction chemotherapy before radiotherapy. From left to right are shown CT, PET, fused PET/CT, and maximum-intensity-projection images. Arrows indicate esophageal tumor. (A) Before radiotherapy, SUVmax was 1.2 and proliferation target volume was 0. (B) After 30 Gy/15 fractions, SUVmax was 1.1 and proliferation target volume was 0. (C) After 50 Gy/25 fractions, SUVmax was 1.2 and proliferation target volume was 0.
On-Treatment 18F-FLT PET/CT: Tumor Repopulation
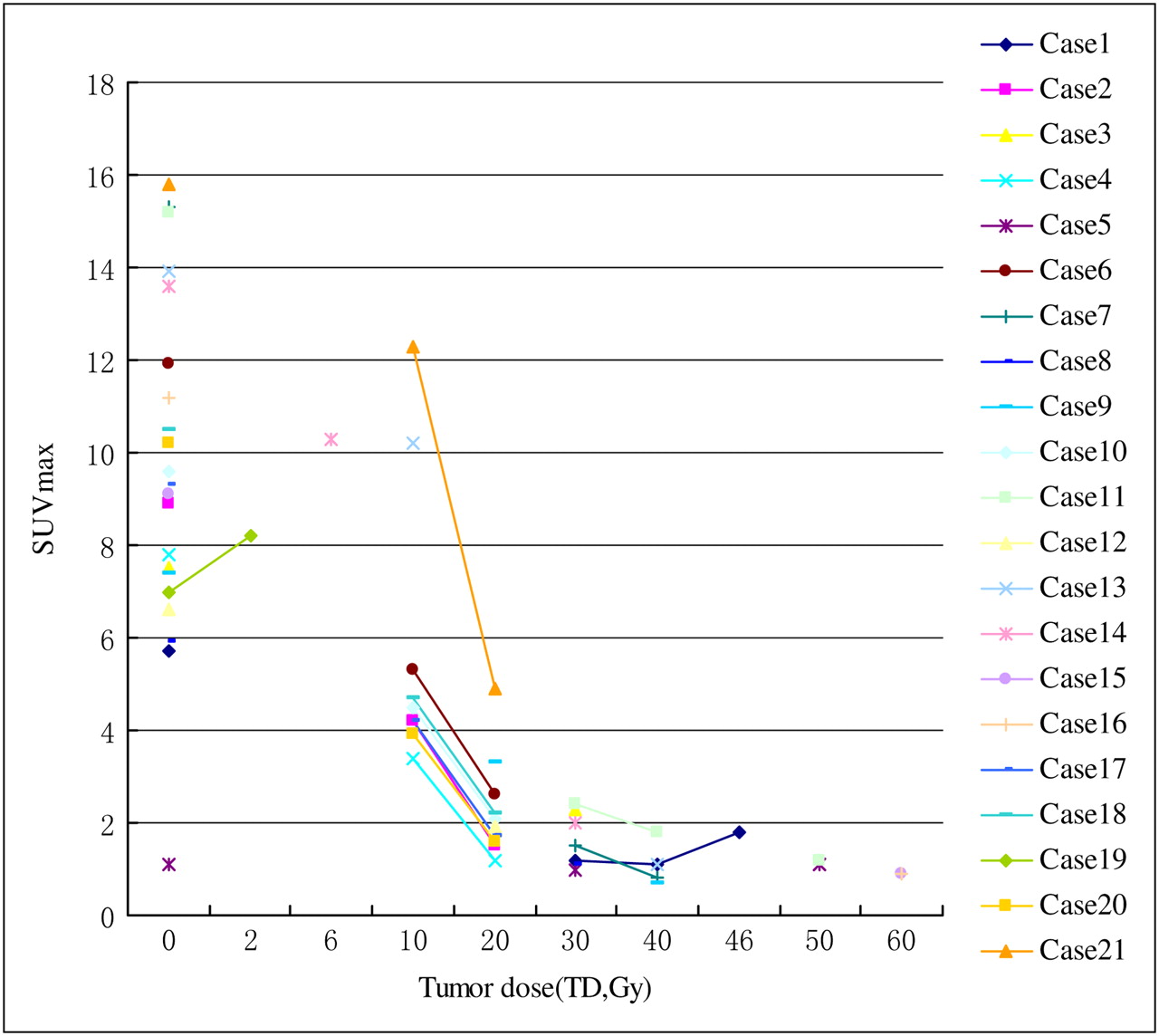
Nineteen of 21 patients received radiotherapy without interruption. In these patients, tumoral SUVmax (Fig. 2) and proliferation target volume (Fig. 3) diminished gradually with increasing TD. These parameters suggest an almost complete absence of detectable tumor proliferation by a TD of 30 Gy and a complete absence at a TD of 40 Gy and beyond. Supplemental Figure 1 illustrates the gradual reduction of 18F-FLT uptake in the tumor and bone marrow of patient 11—a finding that is characteristic of all 19 patients (supplemental materials are available online only at http://jnm.snmjournals.org).
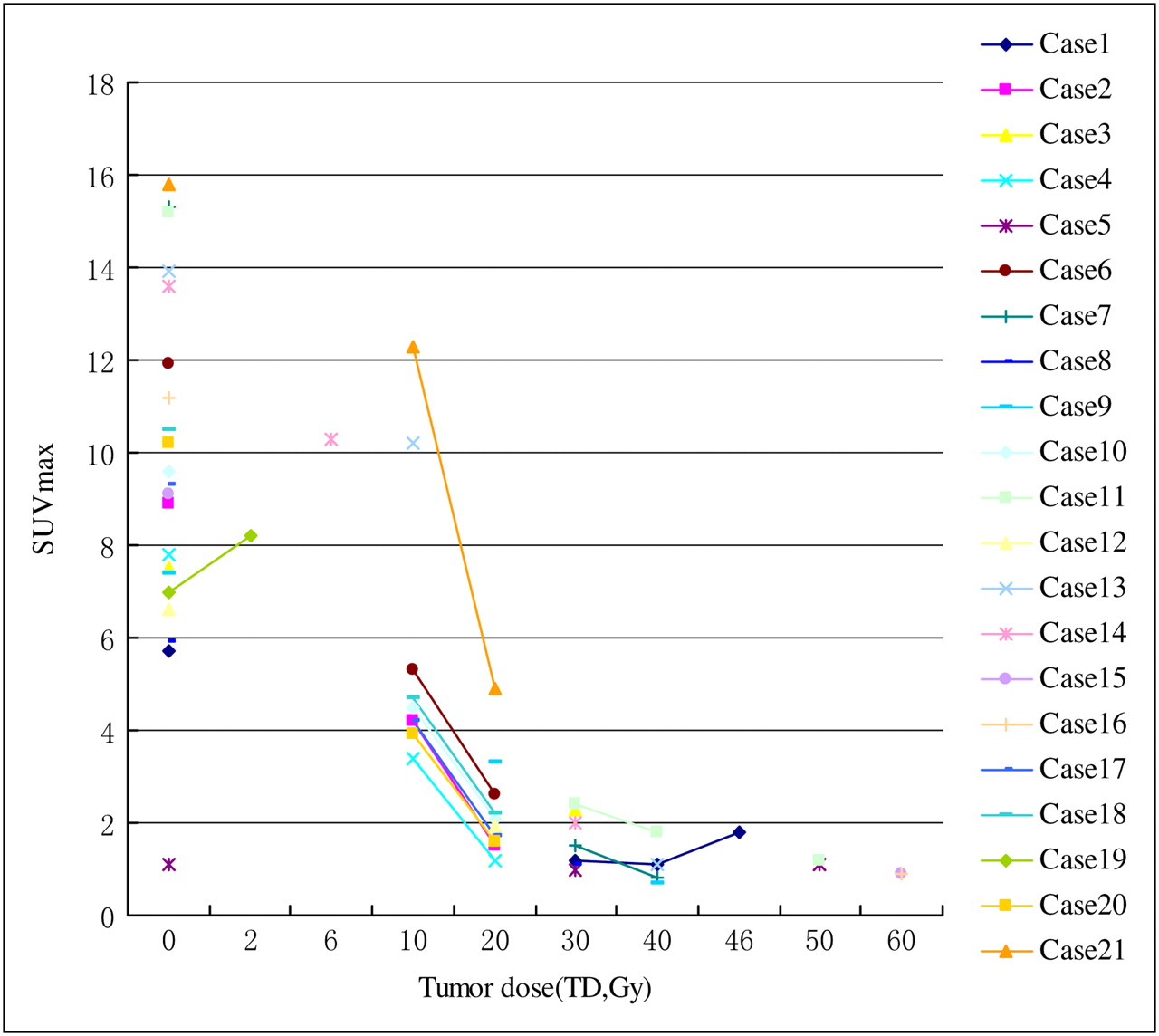
Tumoral SUVmax on 18F-FLT PET at different TDs.

Proliferation target volume (pTV) on 18F-FLT PET at different TDs.
Two patients had unplanned interruptions of their radiotherapy course, which had corresponding increases in 18F-FLT uptake suggestive of tumor repopulation. Patient 19 had a 2-d treatment disruption after only a single 2-Gy fraction, because of malfunction of the linear accelerator. After this disruption, tumoral SUVmax and proliferation target volume rose above baseline whereas 18F-FLT uptake in irradiated bone marrow decreased (Fig. 4). Patient 1 had a 5-d suspension in treatment after a TD of 46 Gy because of grade III bone marrow suppression according to the Common Terminology Criteria for Adverse Events, version 3.0 (CTCAE 3.0). After radiotherapy on a Tuesday, he received human granulocyte colony-stimulating factor from Wednesday to Friday, rested on Saturday and Sunday, and had the 18F-FLT PET/CT scan on Monday. In this patient, 18F-FLT tumoral uptake reduced gradually from TD 0 Gy to TD 30 and 40 Gy and then increased after the treatment interruption at TD 46 Gy, though uptake remained less than at baseline (Supplemental Fig. 2).
Tumor repopulation after interruption of treatment. From left to right are shown axial CT, axial PET, sagittal PET, sagittal fused PET/CT, and maximum-intensity-projection images. Pink arrows indicate esophageal tumor. (A) Before radiation therapy, tumor SUVmax was 7.02 and proliferation target volume was 23.8 cm3. (B) At TD of 2 Gy/1 fraction, after treatment break, SUVmax was 8.22 and proliferation target volume was 27.9 cm3. Radiation field included only left half of vertebrae at these levels (blue arrows represent incident beam). 18F-FLT uptake in irradiated bone marrow decreased (white arrows).
On-Treatment 18F-FLT PET/CT: Lymph Node Metastasis Repopulation
In all patients, trends in 18F-FLT uptake in lymph node metastases reflected trends in uptake in the primary tumor, with SUVmax and proliferation target volume lowering gradually with radiotherapy except after breaks in treatment. SUVmax and proliferation target volume tended to decline less sharply in lymph nodes than in the primary tumor. In patient 1, lymph node uptake reduced gradually from TD 0 Gy to TD 30 and 40 Gy and then increased after treatment interruption at TD 46 Gy.
On-Treatment 18F-FLT PET/CT: Normal-Tissue Response
18F-FLT uptake declined markedly in irradiated bone marrow. These striking changes, corresponding to the paths of the radiation beams, were apparent even after the delivery of only 2 Gy (Fig. 4). By TD 10 Gy, all demonstrated complete absence of uptake in irradiated ribs, sternum, and spine, clearly outlining the boundaries of the radiation fields and suggesting absence of cell proliferation in irradiated marrow after a relatively low radiation dose. This observation held true for patients scanned at later TD points. Marrow uptake did not increase immediately after treatment interruptions, arguing against marrow repopulation. Figures 5B and 5C show that irradiated bone marrow can, however, eventually regain proliferative ability after completion of radiotherapy. In patients who received induction chemotherapy before radiotherapy (patients 3 and 5), preradiotherapy uptake of 18F-FLT was lower than in other patients.

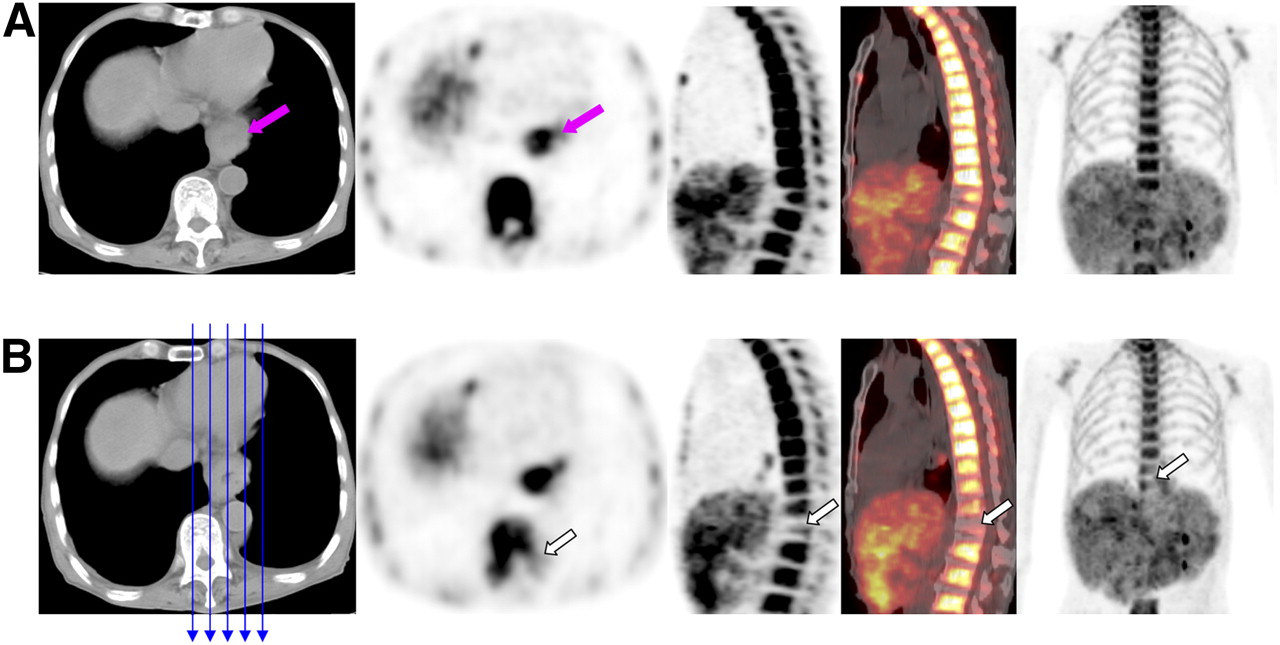
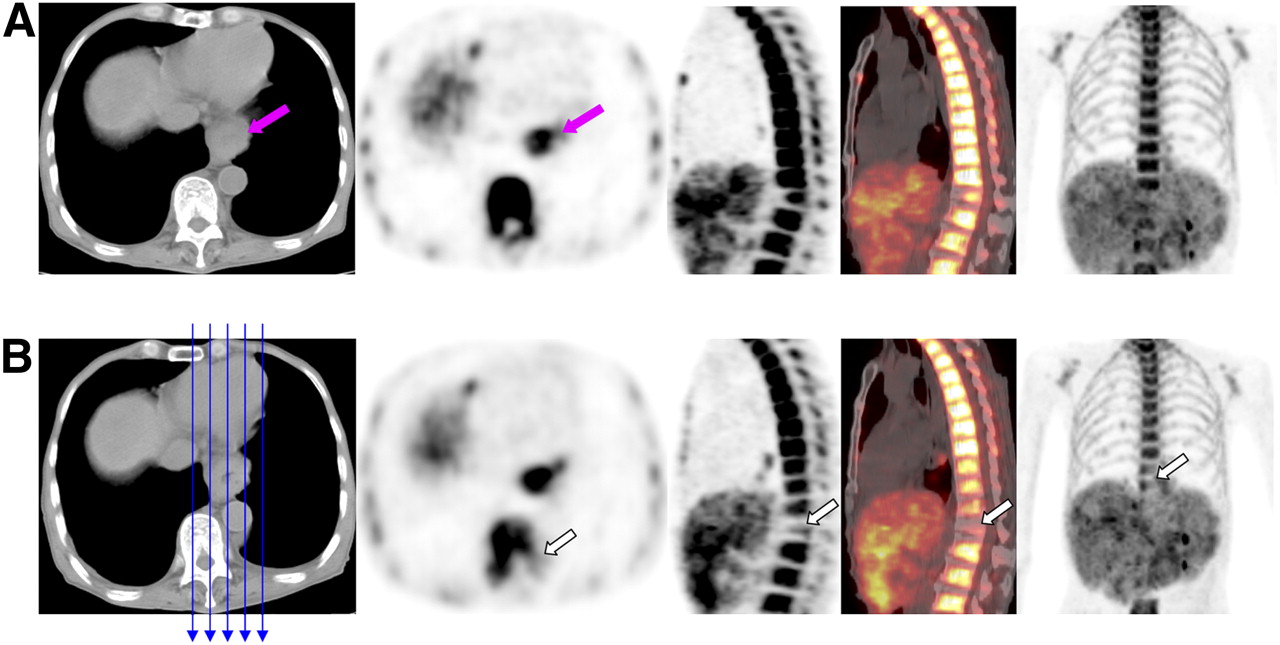
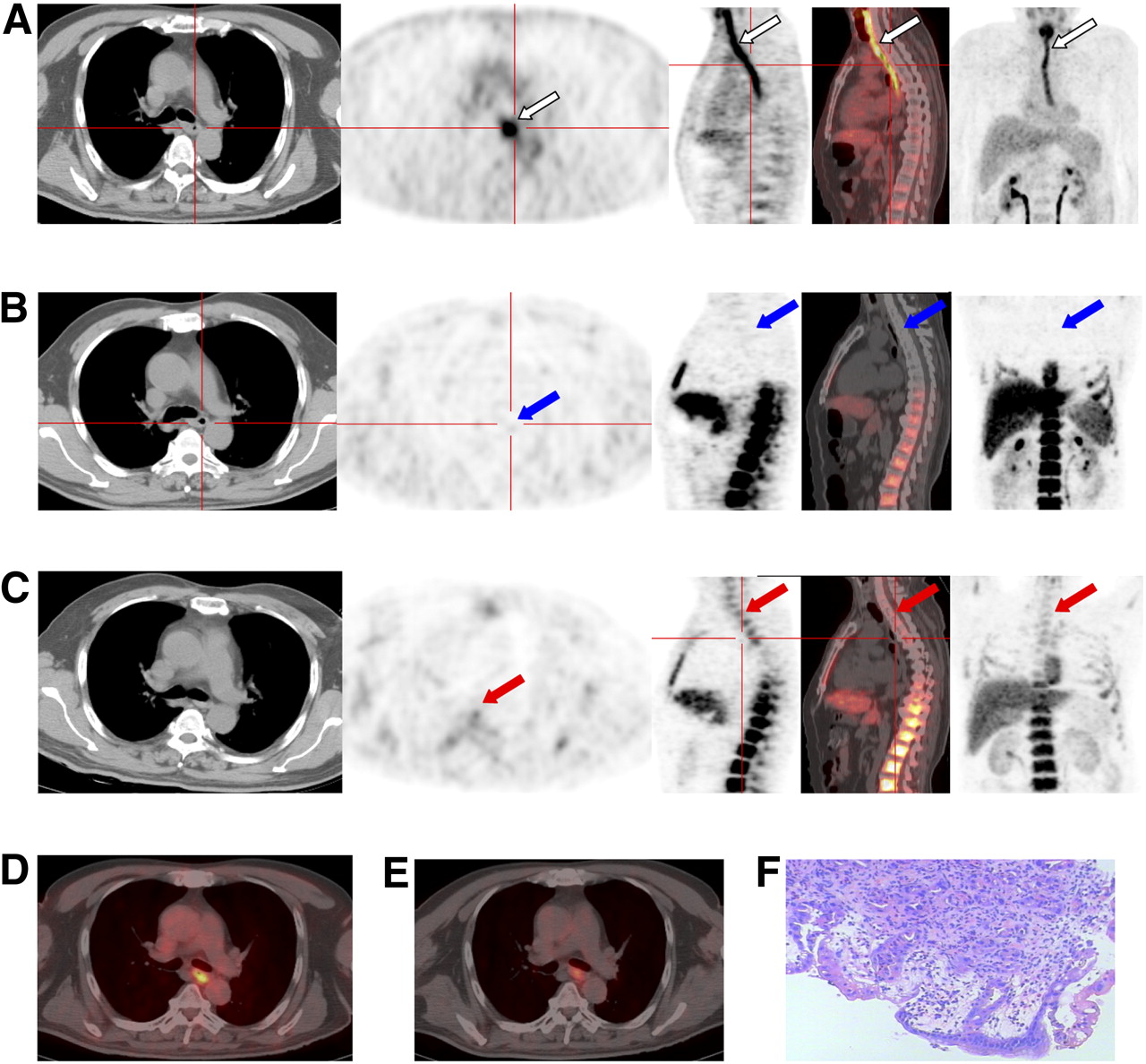
In patient 15, 18F-FLT PET is more effective than 18F-FDG PET in distinguishing residual tumor from inflammation after radiotherapy. From left to right are shown axial CT, axial PET, sagittal PET, sagittal fused PET/CT, and maximum-intensity-projection images. (A) Postradiotherapy 18F-FDG PET shows high uptake (arrows) in primary esophageal tumor. (B) Corresponding 18F-FLT PET shows complete absence of uptake in primary esophageal tumor and irradiated vertebrae (arrows). (C) In 18F-FLT PET scan 1 mo after completion of radiotherapy, primary esophageal tumor still shows no uptake but irradiated vertebrae show more uptake than just after completion of radiotherapy (arrows). (D) Postradiotherapy 18F-FDG PET/CT axial slice has SUVmax of 9.5. (E) Corresponding delayed (after 30 min) 18F-FDG PET/CT axial slice has SUVmax of 7.7. (F) Photomicrograph of endoscopic biopsy specimen of esophageal tumor shows inflammatory infiltrates and interstitial expansion (×100).
18F-FLT PET and 18F-FDG PET: Inflammation and Tumor
After completion of radiotherapy (patients 15 and 16), the primary tumor region demonstrated absence of 18F-FLT uptake but high 18F-FDG uptake. Delayed 18F-FDG PET images (obtained 30 min later) showed slightly lower uptake of 18F-FDG. These patients had grade II esophagitis according to CTCAE 3.0. Subsequent endoscopic biopsy confirmed the presence of inflammatory infiltrates and interstitial expansion without evidence of malignancy (Fig. 5). One month after concurrent chemoradiotherapy, follow-up imaging including CT and plain films with oral barium indicated that the primary tumors approached a complete response according to the Response Evaluation Criteria in Solid Tumors.
DISCUSSION
Serial 18F-FLT PET/CT scans elegantly demonstrated the gradual decline in tumor cell proliferation during radiotherapy of esophageal SCC. Tumor proliferation in this study decreased successively with increasing dose and was almost absent after delivery of about 40 Gy, that is, after 4 wk of uninterrupted radiotherapy.
Serial 18F-FLT PET/CT scans also demonstrated tumor repopulation after interruptions in radiotherapy. Similar to SCC of the head and neck, SCC of the esophagus is considered a rapidly proliferating tumor and is thought to exhibit the phenomenon of accelerated repopulation described by Withers and Taylor (11) in experiments on fractionated radiotherapy. Although the classic understanding of repopulation holds that it occurs preferentially after around 4 wk of radiotherapy, repopulation was observed in this study after treatment breaks at 46 Gy and as early as 2 Gy. Fowler (12) suggested that repopulation begins early. Experimental data from Schmidt-Ullrich et al. (13) support this hypothesis, showing that molecular processes of accelerated repopulation, mediated through radiation-induced receptor activation and cellular growth stimulation, occur after a single 2-Gy fraction. Everitt et al. (14) also observed a “flare” of 18F-FLT uptake in primary non–small cell lung cancer after only 2 Gy.
Accelerated repopulation is believed to contribute to radioresistance, implying that in esophageal SCC, interruptions in radiotherapy are counterproductive. Our results suggest that radiotherapy should be completed without interruption; treatment breaks and split-course radiotherapy should be avoided. When treatment breaks are necessary, adding radiation fractions to the end of treatment to escalate total dose or increasing the dose per fraction may be obligatory to counteract the effects of repopulation. Shortening duration of treatment a priori may preempt repopulation. Zhao et al. (15) demonstrated the effectiveness of late-course accelerated hyperfractionated radiotherapy in the nonsurgical management of locally advanced esophageal SCC in a phase III prospective trial.
The theory of accelerated repopulation has been based on cellular and animal experiments, whereas our clinical study directly detected repopulation in humans. Future studies should investigate the clinical significance of 18F-FLT PET, which is noninvasive and easily repeatable, in detecting repopulation in esophageal SCC and other rapidly proliferating tumors, such as malignancies of the head and neck.
Serial 18F-FLT PET/CT scans in this study also depict the effects of radiotherapy on bone marrow proliferation. Marked early reduction of proliferation in irradiated marrow was observed after only 2 Gy and complete absence of proliferation after 10 Gy. Accelerated repopulation was not observed in marrow during treatment breaks. Posttreatment scans suggest, however, that bone marrow eventually regains its ability to proliferate after completion of radiotherapy. Preradiotherapy scans after induction chemotherapy reflect systemic suppression of hematopoiesis. These results insinuate a role for 18F-FLT PET in monitoring bone marrow suppression during or after radiotherapy or chemotherapy.
This study also suggests a role for 18F-FLT PET in differentiating inflammation from residual tumor, as currently used imaging modalities are nonspecific in this regard. Endoscopic ultrasound after radiotherapy is poor at distinguishing tumor from posttherapeutic fibrosis or inflammation. 18F-FDG PET relies on metabolic differences in glucose use, but glucose accumulates both in tumor and in inflammatory cells, and inflammatory cells are common in irradiated esophageal tissue (16–18). Uptake on 18F-FDG PET, therefore, could represent either residual tumor or esophagitis. This study suggests that 18F-FLT PET may discriminate tumor from esophagitis more effectively, which could have important clinical applications.
One potential application of 18F-FLT PET is early assessment of treatment response. 18F-FLT PET has been used to monitor response to chemotherapy, which may have implications on survival (19–22). Changes in 18F-FLT uptake early in chemotherapy may correlate with outcomes in patients with breast or brain tumors (19). One in vitro study demonstrated that 18F-FLT uptake in esophageal cancer cells decreased early after incubation with various cytotoxic drugs (23). If studies confirm that early changes in 18F-FLT uptake predict ultimate tumor response, early identification of nonresponders to neoadjuvant chemotherapy or radiation could direct alterations in therapy to potentially improve outcomes.
Our study suggests that 18F-FLT PET provides treatment response data incremental to CT alone. After 3 cycles of induction chemotherapy, patient 5 (Fig. 1) demonstrated tumoral SUVmax similar to background, though tumor appeared to remain on CT. Similarly, patients 11 (Supplemental Fig. 1) and 1 (Supplemental Fig. 2) exhibited reductions in tumoral SUVmax to background levels after radiotherapy, despite residual tumor on CT. CT identifies residual tumor with poor specificity. Additional investigations should confirm whether 18F-FLT PET depicts treatment response more accurately. A comprehensive study examining the relationship between early changes on 18F-FLT PET and outcomes such as treatment response, local failure rate, and survival is ongoing at our institution.
18F-FLT PET/CT could also be used to determine a biologic target volume for radiotherapy. “Dose painting” via intensity-modulated radiation therapy could potentially be used to escalate dose to regions of clonogenic proliferation.
Our study is limited by its small sample size. Additional research is needed to confirm the validity of these findings.
CONCLUSION
This pilot study suggests that 18F-FLT PET/CT can demonstrate the distinctive biologic response of esophageal SCC to radiotherapy, including its potential for accelerated repopulation. 18F-FLT PET/CT can also depict the effects of radiotherapy on bone marrow and may differentiate between residual tumor and inflammation. 18F-FLT PET/CT, as a noninvasive and reliable imaging technique, may eventually help oncologists assess treatment response, estimate clonogenic repopulation during radiotherapy, or evaluate the effectiveness of neoadjuvant therapy. Additional investigation with larger patient numbers is needed to validate these findings.
Acknowledgments
We thank our chief nurse, Ningsha Yu, for her great assistance and support of the research.
Footnotes
-
COPYRIGHT © 2010 by the Society of Nuclear Medicine, Inc.
References
- Received for publication October 28, 2009.
- Accepted for publication January 5, 2010.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- 18F-FLT PET/CT Adds Value to 18F-FDG PET/CT for Diagnosing Relapse After Definitive Radiotherapy in Patients with Lung Cancer: Results of a Prospective Clinical Trial
- Hybrid Imaging PET/CT with Application of 18F-Fluorothymidine in Patients with Head and Neck Carcinoma Undergoing Radiotherapy
- Predicting Response to Neoadjuvant Chemoradiotherapy in Esophageal Cancer with Textural Features Derived from Pretreatment 18F-FDG PET/CT Imaging
- Role of Positron Emission Tomography for the Monitoring of Response to Therapy in Breast Cancer
- PET Imaging of Proliferation with Pyrimidines
- 18F-FLT PET During Radiotherapy or Chemoradiotherapy in Head and Neck Squamous Cell Carcinoma Is an Early Predictor of Outcome
- In Vivo Imaging of Cell Proliferation Enables the Detection of the Extent of Experimental Rheumatoid Arthritis by 3'-Deoxy-3'-18F-Fluorothymidine and Small-Animal PET
- Usefulness of 3'-Deoxy-3'-18F-Fluorothymidine PET for Predicting Early Response to Chemoradiotherapy in Head and Neck Cancer