


Abstract
PET provides a noninvasive means to evaluate the functional integrity of the presynaptic monoaminergic system in the living human brain. Methods: In this study, a novel 18F-labeled tetrabenazine derivative, 18F-(+)fluoropropyldihydrotetrabenazine (18F-AV-133), was used for the noninvasive assessment of the vesicular monoamine transporters type 2 (VMAT2) in 17 Parkinson disease (PD) patients and 6 healthy controls. The binding potential (BP) of 18F-AV-133 was calculated using Logan graphical analysis. Voxel-based and volume-of-interest–based analyses of BP images were performed to examine brain regional reductions in VMAT2 density in PD. Results: VMAT2 BP was decreased by 81% in the posterior putamen, 70% in the anterior putamen, and 48% in the caudate nucleus of PD patients. Voxel-based analysis demonstrated VMAT2 reductions in the striatum and mid brain of PD patients. Furthermore, VMAT2 BPs in the caudate nuclei significantly correlated with the clinical severity of PD. Conclusion: These findings indicate that the novel 18F-labeled ligand 18F-AV-133 can sensitively detect monoaminergic terminal reductions in PD patients. Studies with 18F-AV-133 may allow the presymptomatic identification of individuals with disorders characterized by degeneration of dopaminergic nigrostriatal afferents.
Parkinson disease (PD) is a common neurodegenerative disorder clinically characterized by resting tremor, rigidity, bradykinesia, and gait disturbance resulting in falls. The extrapyramidal symptoms in PD are caused by the loss of dopamine neurons in the substantia nigra, with consequent prominent dopaminergic terminal loss in the striatum. Increasing evidence suggests that the noninvasive evaluation of nigrostriatal dopaminergic integrity by PET and SPECT may provide useful clinical information for the early diagnosis of PD (1–6). Several radiotracers have been proposed for this purpose, including 18F-labeled levodopa (18F-FDOPA), for assessing presynaptic dopamine synthesis; 11C-WIN-35,428 and 123I-β-CIT, for binding to the dopamine transporter (DAT); and 11C-labeled dihydrotetrabenazine (11C-DTBZ), for binding to the vesicular monoamine transporter type 2 (VMAT2) (1–6). VMAT2 is the transporter responsible for the uptake and storage of dopamine and other monoamines into vesicles in monoamine-containing neurons. VMAT2 is mainly located on synaptic vesicles at the nerve terminals but also on dense core vesicles in nerve cell bodies and dendrites (7). Previous PET studies with 11C-DTBZ have shown decreased binding to VMAT2 in the striatum of PD patients (5,8,9). A reduction of VMAT2 reflects the degeneration of nigrostriatal dopaminergic neurons and is less susceptible than DAT to compensatory changes occurring with the loss of dopaminergic neurons (9,10). The in vivo measurement of VMAT2 density could, thus, be useful for the early and differential diagnosis of PD.
A novel 18F-labeled tetrabenazine derivative, 18F-(+)fluoropropyldihydrotetrabenazine (18F-AV-133), that selectively binds with high affinity to VMAT2 has been developed to assess VMAT2 density in vivo with PET (11,12). To evaluate the utility of this novel tracer for assessing presynaptic neuronal integrity in PD, a PET study was performed to compare 18F-AV-133 binding in PD patients and healthy controls (HCs).
MATERIALS AND METHODS
Subjects
Written informed consent was obtained from all participants. Approval for the study was obtained from the Austin Health Human Research Ethics Committee. HCs were recruited by advertisement in the community, and participants fulfilling clinical criteria for PD (13) were recruited from movement disorder clinics. Seventeen PD subjects aged 67.4 ± 9.3 y (mean ± SD; range, 53–82 y) and 6 age-matched HCs aged 65.2 ± 4.5 y (range, 57–70 y) were included in the study.
All subjects underwent neurologic and neuropsychologic examination. Fifteen patients were receiving carbidopa–levodopa, 1 was receiving selegiline, and 1 was receiving levodopa and benserazide. The neurologic evaluation included the assessment of duration of illness, Hoehn and Yahr score, and motor subscale (section III) of the Unified Parkinson Disease Rating Scale (UPDRSm) while the patient was not taking medication (24 h after the last medication dosage). Furthermore, clinical laterality symptoms were assigned scores (Table 1) to allow correlational analysis with the 18F-AV-133 PET results. Treatment was resumed before the PET scan. The neuropsychologic evaluation included the mini–mental state examination (MMSE), clinical dementia rating (CDR), hospital anxiety and depression scale (HADS), fluctuating assessment scale, logical memory score, and verbal fluency scores.
Clinical Laterality Scores
Radiosynthesis of 18F-AV-133
18F-AV-133 was obtained by nucleophilic substitution of the mesylate precursor AV-244 using previously described methods (12), with slight modifications. AV-244 (2 mg in 1 mL of 50:50 dimethylsulfoxide:acetonitrile [DMSO:ACN]) was reacted with azeotropically dried 18F for 10 min at 90°C. Unreacted fluoride was eliminated from the crude reaction via tC18 Sep Pak (Waters Corp.) purification. 18F-AV133 was eluted off the Sep Pak with ACN (1 mL) and purified via semipreparative high-performance liquid chromatography (Zorbax Eclipse XDB-C18 column; Agilent Technologies) (5 μm, 9.4 × 250 mm eluted with 45:55 ACN:20 mM ammonium acetate, 4.0 mL/min flow rate, 11-min retention time). The 18F-AV133 fraction was collected and reformulated for injection using a tC18 Sep Pak. The final dose was filtered through a Millex AV polyvinylidene difluoride 0.22-μm filter. The average non–decay-corrected radiochemical yield was 24% after a synthesis time of 60 min, with a radiochemical purity of greater than 95% and a specific activity ranging from 44.4 to 207.9 GBq/μmol.
Imaging Studies
Each subject received approximately 250 MBq of 18F-AV-133 by intravenous injection over 1 min. Imaging was performed with a Phillips Allegro PET camera (spatial resolution, 5.2 mm in full width at half maximum). A rotation transmission sinogram in 3-dimensional (3D) mode with a single 137Cs point source was acquired before the injection of the radiotracer for attenuation-correction purposes. An initial 90-min dynamic list-mode emission image was acquired in 3D mode after the injection of 18F-AV-133. List-mode raw data were sorted offline into 4 × 30-s, 9 × 1-min, 3 × 3-min, 10 × 5-min, and 2 × 10-min frames. Further images were obtained at 120–140 and 180–200 min after injection. The sorted sinograms were reconstructed using a 3D row-action maximum-likelihood algorithm.
All subjects received a 3D T1-weighted magnetization-prepared rapid-acquisition gradient-echo MRI scan for screening of other diseases and coregistration with the PET images.
Image Analysis
The dynamic PET images were converted into binding potential (BP) parametric images through Logan graphical analysis with PMOD software (version 3.0; PMOD Technologies), using the primary visual cortex, a region relatively devoid of monoaminergic terminals, as input function (14). Parametric 18F-AV-133 PET/MRI coregistered images were spatially normalized into the Montreal Neurologic Institute MRI brain template standard stereotactic space using statistical parametric mapping software (SPM5; Wellcome Department of Cognitive Neurology). Spheric volumes of interest (VOIs) (5 mm in diameter) were placed over a spatially normalized MR image in the caudate nucleus, anterior and posterior putamen, and mid brain. VOIs were then transferred onto BP parametric images, and regional BP values were calculated using PMOD. Asymmetry indices between right (R) and left (L) caudate and putamen were calculated as follows: (R − L)/([R + L]/2).
Statistical Analysis
Regional BP values were statistically compared using the Student t test, and clinical data were statistically compared using the Mann–Whitney U test. Correlations between the 18F-AV-133 BP values and clinical data were performed using a nonparametric Spearman rank correlation analysis. Statistical significance for each analysis was defined as a P value less than 0.05. These analyses were performed using Prism 5 (GraphPad Software). Additionally, SPM5 was used to evaluate intergroup BP differences on a voxelwise basis. Group comparisons between PD patients and HCs were performed by voxel-by-voxel t tests, accepting only voxels surviving false-discovery rate correction for the entire volume at a P value less than 0.05, to avoid false-positive results.
RESULTS
Demographic and clinical data are summarized in Table 2. The PD group contained a higher proportion of men than did the HC group. All patients were considered to have mild to moderate PD (off-medication state Hoehn and Yahr scores, 1–3: stage 1, n = 4; stage 1.5, n = 2; stage 2, n = 4; stage 2.5, n = 2; and stage 3, n = 1 patients). The UPDRSm in the off-medication state and HADS were significantly higher in PD patients than in HCs. There was no difference between the groups in CDR, fluctuating assessment scale, logical memory score, and verbal fluency score. The Hoehn and Yahr and UPDRS scores in the off-medication state were unavailable in 4 PD patients.
Demographic Characteristics of Subjects
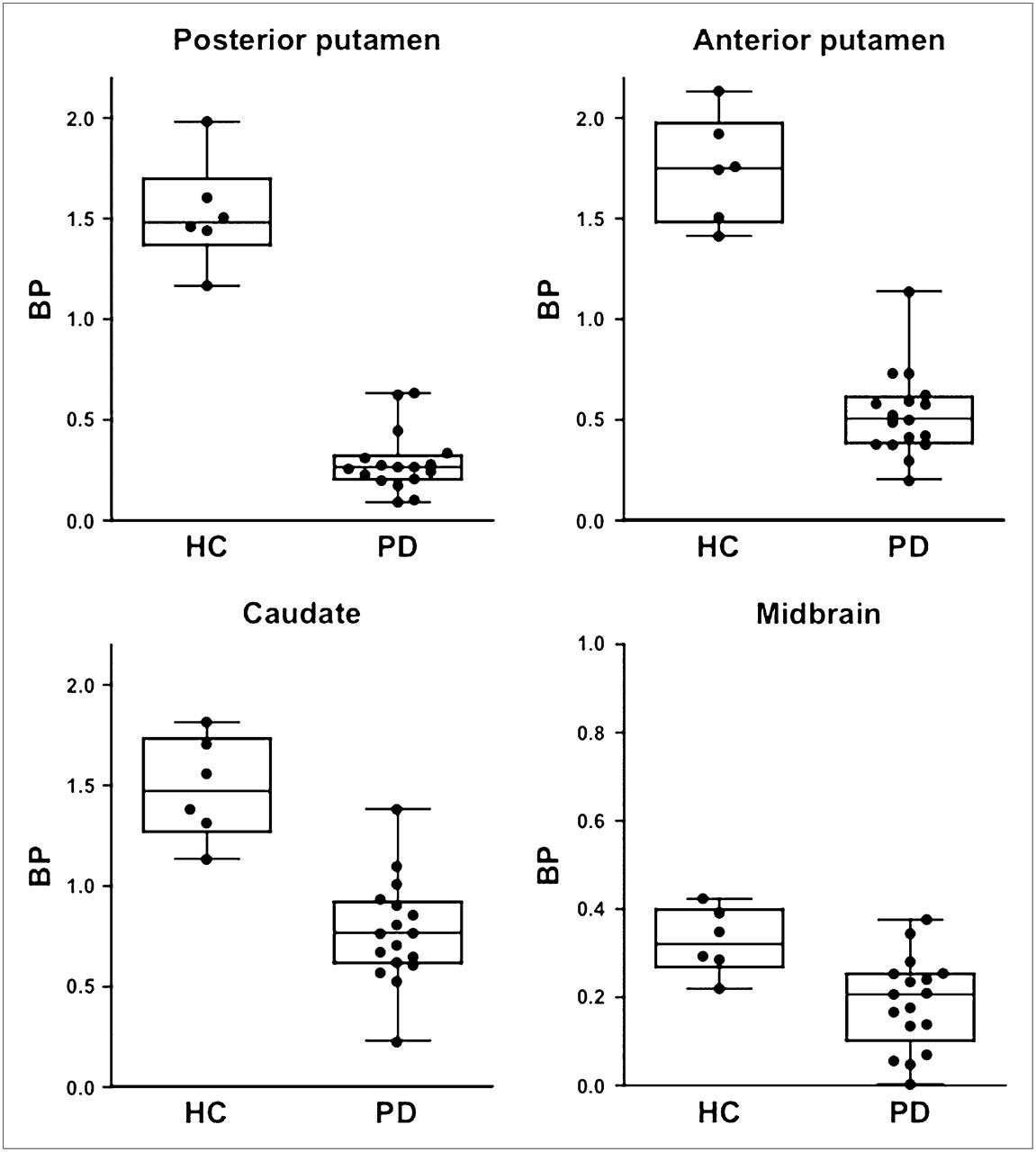
Lower 18F-AV-133 BPs were observed in the putamen, caudate, and mid brain of PD patients. Representative 18F-AV-133 BP PET images in a healthy elderly control (66-y-old man) and a PD patient (61-y-old man; Hoehn and Yahr score, 2) are shown in Figure 1A. Voxel-based group comparison of 18F-AV-133 BP images showed significantly lower BP in PD patients than in HCs in the striatum (L: −30, −4, 2, x, y, z; Z = 7.07; R: 32, −4, 8, x, y, z; Z = 6.69) and substantia nigra (L: −6, −20, −14, x, y, z; Z = 3.67; R: 10, −18, −14, x, y, z; Z = 3.45) (Fig. 1B). In contrast, no brain region in PD patients showed significantly higher 18F-AV-133 BP than that in the brain region of HCs. VOI-based analysis similarly indicated a significantly lower BP in the caudate nucleus, putamen, and mid brain of PD patients (Fig. 2; Table 3). No overlap was observed between the 18F-AV-133 BP values in the putamen of PD patients and HCs. The greatest BP decline in PD was observed in the posterior putamen (−81%), followed by the anterior putamen (−70%), caudate (−48%), and mid brain (−43%). In the posterior putamen, 18F-AV-133 BP values in all PD patients were more than 3 SDs below those in HCs.
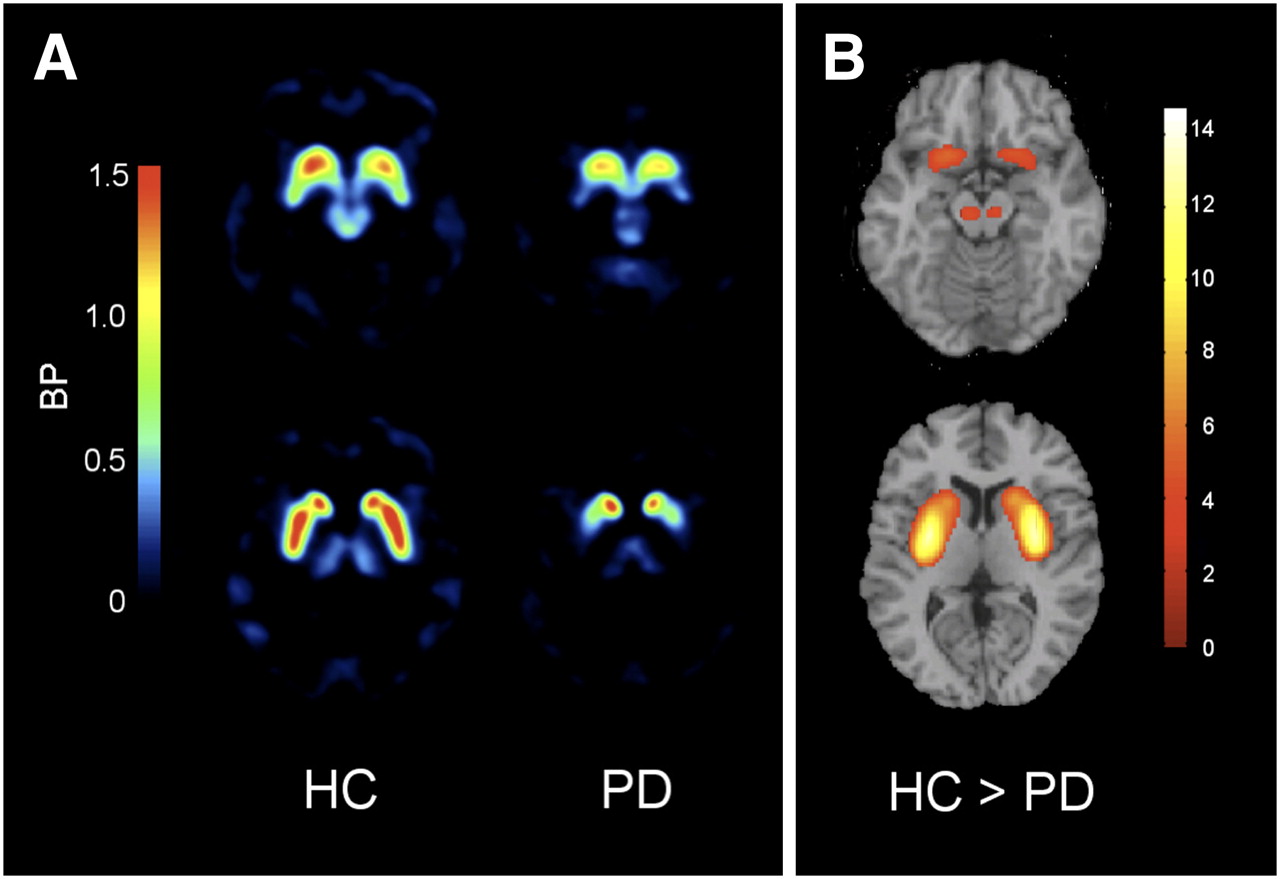
(A) Representative images of 18F-AV-133 PET BP in HC and PD patient. (B) Areas of reduction in BP of PD patients, compared with HCs, in SPM analysis. Color bars represent t values. P < 0.05, corrected for multiple comparisons.

18F-AV-133 PET BP from VOI analysis in HCs and PD patients.
BPs of 18F-AV-133 PET
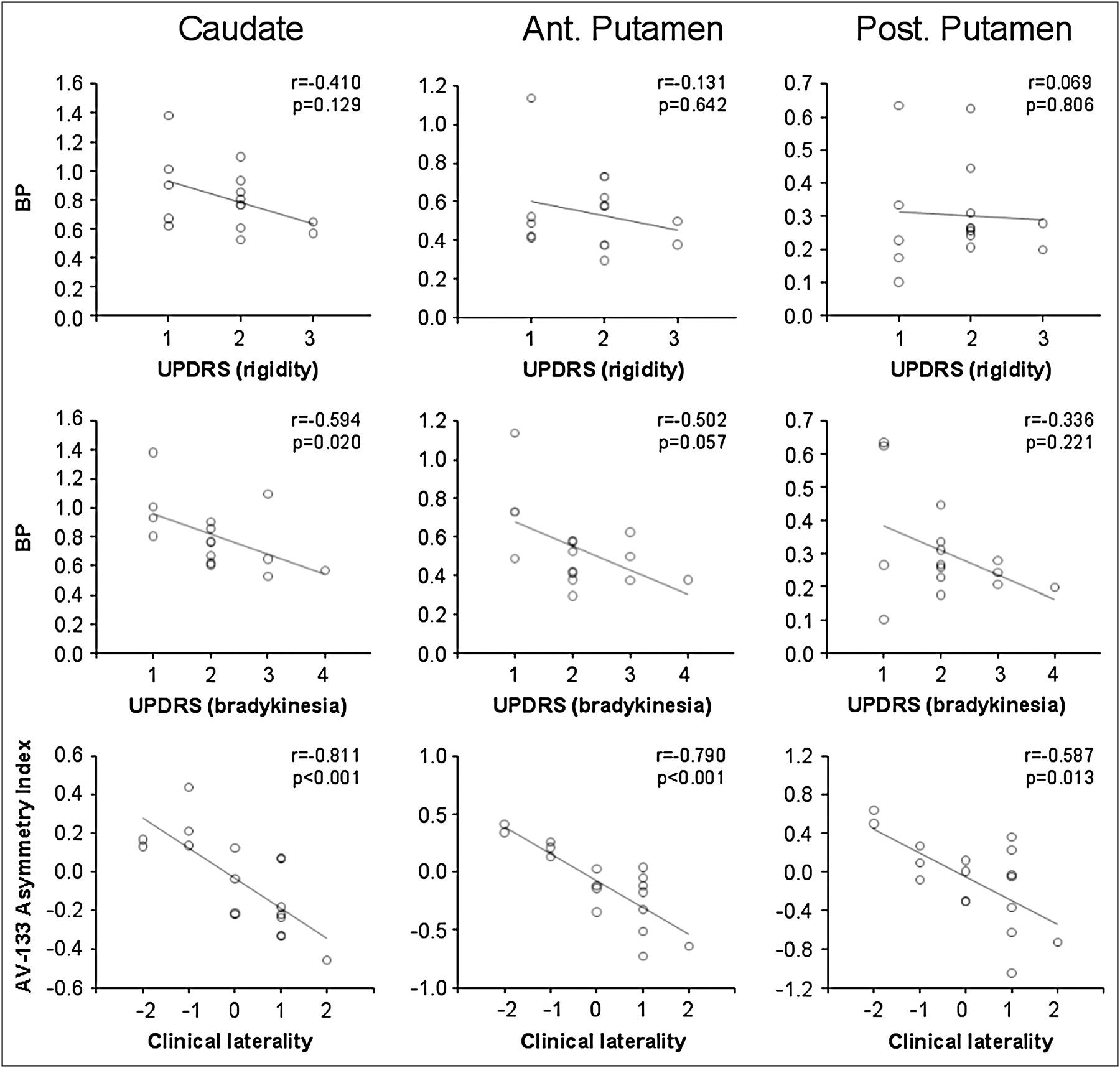
The correlation between regional BP values and UPDRSm and HADS scores was also examined. As shown in Figure 3, UPDRSm bradykinesia subscores in PD patients negatively correlated with 18F-AV-133 BP values in the caudate (r = −0.59, P = 0.02), and a trend was observed in the anterior putamen (r = −0.50, P = 0.06). However, no significant correlations were found in the posterior putamen or when the UPDRSm rigidity subscores were examined. No significant correlation was observed between regional BP values and the HADS scores. Conversely, there was a significant inverse correlation between 18F-AV-133 asymmetry indices in the striatum and the clinical laterality scores (Fig. 3).
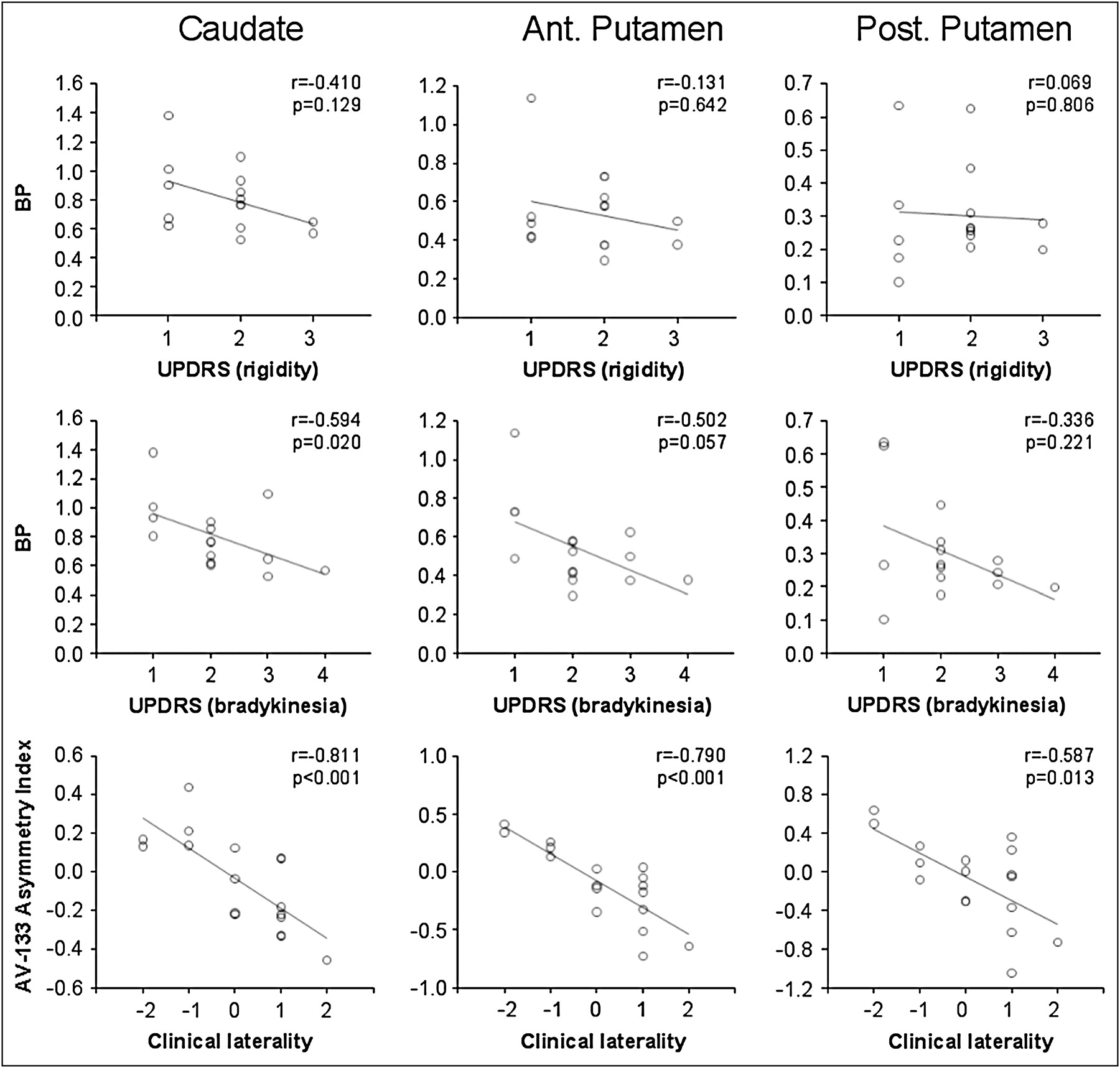
Correlation of rigidity and bradykinesia subscores of UPDRSm and clinical laterality ratings with 18F-AV-133 PET BP in striatum. Although there was strong association between asymmetry indices and laterality scores, only VMAT2 BP in caudate correlated with bradykinesia UPDRSm subscores. Ant. = anterior; Post. = posterior.
DISCUSSION
Both DAT and VMAT2 have been proposed as markers of dopaminergic nerve terminal integrity. Imaging with DAT-specific radioligands has been reported to be a sensitive index of presynaptic neuronal degeneration, enabling the early and accurate diagnosis of patients with suspected PD (15). However, DAT is susceptible to dopaminergic regulation and can be altered by treatment with l-DOPA, deprenyl, cocaine, and amphetamine (16). In contrast, whereas VMAT2 is common to all monoaminergic neurons and not just dopaminergic ones, it is less susceptible to the effects of l-DOPA or other dopaminergic drugs (16–18). Thus, VMAT2 imaging may be a more reliable marker to monitor dopamine terminal integrity in PD patients. Currently, 11C-DTBZ is the only available PET tracer for the noninvasive quantification of VMAT2 density in the brain. Unfortunately, the 20-min radioactive decay half-life of 11C limits the use of 11C-DTBZ to centers with an on-site cyclotron and 11C radiochemistry expertise. Consequently, access to 11C-DTBZ is restricted, and the high cost of studies is prohibitive for routine clinical use. To overcome these limitations, a tracer for imaging VMAT2 that can be labeled with 18F is required. The 110-min radioactive decay half-life of 18F permits the centralized production and regional distribution as currently practiced worldwide in the supply of 18F-FDG for clinical use.
The current PET study showed significantly lower VMAT2 densities as measured by 18F-AV-133 in the putamen, caudate, and substantia nigra of PD patients. The greatest VMAT2 reductions were observed in the posterior putamen (−81%), followed by the anterior putamen (−70%), and caudate nucleus (−48%). These results are consistent with previous 11C-DTBZ PET results showing the highest reduction (71%−77%) in the posterior putamen of PD patients (8,9,19,20). Our observations are also consistent with postmortem reports showing 88% reduction of VMAT2 immunoreactivity in the putamen of PD patients (21). There was no intergroup overlap between the putaminal BP of PD patients and controls. Actually, BP values in the posterior putamen of all PD patients were more than 3 SDs below those of HCs. These results suggest that 18F-AV-133 is a highly sensitive tool to detect early dopaminergic dysfunction in PD patients. A longitudinal study in mildly affected PD patients or individuals at risk of PD will elucidate the usefulness of this tracer for early or presymptomatic diagnosis of PD (6). As shown in previous PET and SPECT studies (19,22,23), the evaluation of presynaptic dopaminergic integrity would also be useful in the differential diagnosis of dementia with Lewy bodies (DLB) from Alzheimer disease (AD), for which severe nigrostriatal dopaminergic degeneration, similar to that observed in PD, is present in DLB but not in AD. Additional studies comparing 18F-AV-133 binding in DLB and AD patients are warranted. Likewise, VMAT2 imaging could be applied to evaluate cases of familial PD for the detection of nigrostriatal degeneration at early, presymptomatic stages and the assessment of subjects with rapid eye movement sleep behavior disorder and also to evaluate subjects considered to have mild cognitive impairment who might present with mild or inconclusive motor symptoms suggestive of a pre-DLB stage.
Dopamine is released not only from axon terminals in the striatum but also from the cell bodies and dendrites in the substantia nigra. Consistently, VMAT2 is also localized in extrastriatal regions including the substantia nigra (7). Human PET studies using stereoisomers of 11C-DTBZ demonstrated specific in vivo binding of 11C-DTBZ in the mid brain (24), and in vivo studies in mice showed 18F-AV-133 binding to VMAT2 in the substantia nigra (11). Previous 11C-DTBZ PET studies demonstrated a 50% VMAT2 reduction in the substantia nigra of PD patients (20). In a similar fashion, the present study demonstrated a 43% reduction of 18F-AV-133 binding in the substantia nigra of PD patients, consistent with previous reports of VMAT2 reduction in the PD brain (20,24).
Significant correlations between clinical severity PD scores and 18F-AV-133 binding were observed in the caudate nucleus but not in the putamen. This result conflicts with previous PET reports showing correlation of UPDRS score with 11C-DTBZ binding or 18F-FDOPA uptake in the putamen (9,25). The lack of correlation in the putamen might be caused by the limited sample size or, more likely, a floor effect because the putamen is more severely affected than the caudate nucleus.
Depression is one of the most common complications in PD, contributing to poor quality of life and disability. HADS scores, mainly driven by the depression scales, were significantly higher in PD patients. A VMAT2 inhibitor, reserpine, is known to induce depressionlike symptoms in humans. Although a previous study demonstrated the association of lower striatal VMAT2 density and cocaine-induced mood disorders (26), we did not find a correlation between HADS scores and 18F-AV-133 binding in PD patients, suggesting a weak association between striatal VMAT2 density and mood function in PD patients. A strong inverse correlation was found between 18F-AV-133 asymmetry indices and clinical laterality scores, indicating that 18F-AV-133 can correctly identify the most affected side. Additional studies using larger sample populations and less affected individuals are required to more fully examine the correlation of regional 18F-AV-133 binding with clinical severity of PD.
CONCLUSION
Significant VMAT2 reductions were successfully detected in the striatum and mid brain of PD patients with 18F-AV-133. These observations indicate that 18F-AV-133 is a suitable ligand for the noninvasive assessment of VMAT2 density in the human brain.
Acknowledgments
We thank Drs. Sylvia Gong, Henry Tochon-Danguy, and Andrew Hughes for their crucial role in patient recruitment and PET examinations, and Tania Petts, Tim Saunder, and Jason Bradley for their role during PET examinations and image processing. This study was supported in part by funds from Avid Radiopharmaceuticals Inc. and the Austin Hospital Medical Research Foundation.
Footnotes
-
COPYRIGHT © 2010 by the Society of Nuclear Medicine, Inc.
References
- Received for publication September 1, 2009.
- Accepted for publication October 30, 2009.





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Imaging Dopaminergic Neurotransmission in Neurodegenerative Disorders
- Parkinson Disease: Translating Insights from Molecular Mechanisms to Neuroprotection
- Diagnostic accuracy of imaging brain vesicular monoamine transporter type 2 (VMAT2) in clinically uncertain parkinsonian syndrome (CUPS): a 3-year follow-up study in community patients
- Management Impact of Imaging Brain Vesicular Monoamine Transporter Type 2 in Clinically Uncertain Parkinsonian Syndrome with 18F-AV133 and PET
- In Vivo Detection of Monoaminergic Degeneration in Early Parkinson Disease by 18F-9-Fluoropropyl-(+)-Dihydrotetrabenzazine PET
- Monoamine transporters: Structure, regulation, and clinical implications
- Nigrostriatal Dopamine Terminal Imaging with Dopamine Transporter SPECT: An Update
- Biomarkers for Parkinson's Disease
- Whole-Body Biodistribution and Radiation Dosimetry of 18F-FP-(+)-DTBZ (18F-AV-133): A Novel Vesicular Monoamine Transporter 2 Imaging Agent