


Abstract
Idiopathic Parkinson disease is a common neurodegenerative disorder for which misdiagnosis occurs in up to 30% of patients after initial assessment and in 10%–15% even after long-term follow-up. Vesicular monoamine transporter type 2 (VMAT2) imaging with PET allows assessment of the integrity of the presynaptic dopaminergic pathway. We investigated the management impact of VMAT2 imaging in patients with clinically uncertain Parkinsonian syndromes. Methods: Forty-seven patients with clinically uncertain Parkinsonian syndromes (mean age ± SD, 56.9 ± 14.9 y; age range, 21–80 y) were referred from movement disorder specialists. All participants underwent a 20-min PET acquisition 2 h after injection of 250 MBq of 18F-AV-133, and the resulting images were quantitatively assessed. Clinical impact was recorded as high, moderate, or low based on diagnosis and management questionnaires completed by the referring specialists before and after release of the PET results. Management impact was high if there was a change in diagnostic category, moderate if there was a change in medication, and low if there was no change. Results: VMAT2 PET changed the diagnosis in 11 (23%) and medication in 25 (53%) participants. Management impact was high in 23%, moderate in 38%, and low in 39% of the participants. High diagnostic confidence increased from 11% of patients to 80% after the release of the scan results. Conclusion: 18F-AV-133 had substantial management impact in patients with clinically uncertain Parkinsonian syndromes. VMAT2 imaging with 18F-AV133 might improve diagnosis, prognosis, and appropriate use of medication, translating into better patient outcomes.
Idiopathic Parkinson disease (iPD) is a common neurodegenerative disorder with an incidence of about 17 per 100,000 per year (1,2). The pathophysiology of iPD includes loss of dopaminergic neurons in the substantia nigra and thereby loss of dopaminergic terminals in the striatum. This terminal loss correlates with the extrapyramidal symptoms of the disease. Although bradykinesia, rigidity, and resting tremor remain the clinical diagnostic criteria for iPD, reports of diagnostic accuracy compared with postmortem diagnosis varied from 70% in early stage disease to 90% in advanced stage in a tertiary referral movement disorder clinic (3–5). However, about 1 in 5 patients presenting with Parkinsonian features do not meet these diagnostic criteria (6) or may have additional clinical features suggesting another disease process. Under these circumstances, the patient may be labeled as clinically uncertain Parkinson syndrome (CUPS) (7). Several conditions might overlap with iPD, leading to misdiagnosis or diagnostic uncertainty. Among these, disorders in which the dopaminergic pathways are intact include essential tremor, dystonia, drug-induced parkinsonism, and symptoms without dopaminergic deficit, or disorders in which there is dopaminergic neuronal loss plus more extensive neurodegeneration, such as multiple-system atrophy, progressive supranuclear palsy, and corticobasal degeneration.
The shortcomings of clinical examination alone and the advantages of early diagnosis and early treatment necessitate a method for more accurate and early diagnosis.
The integrity of the nigrostriatal system can be evaluated noninvasively using PET and SPECT to provide clinical information that can assist in the early and differential diagnosis of iPD (8–14). Several radioligands have been developed for this purpose to image either presynaptic targets such as the dopamine transporter (DAT), vesicular monoamine transporter type 2 (VMAT2), dihydroxyphenylalanine decarboxylase activity, or postsynaptic D2 dopamine receptors (6). VMAT2 is involved in the uptake and storage of dopamine and other monoamines into presynaptic vesicles. It is mainly located at the nerve endings as well as nerve cell bodies and dendrites (15). Reduction in VMAT2 in the striatum reflects loss of nigrostriatal terminals (16,17). The in vivo measurement of VMAT2 density has been shown to be potentially useful for the early and differential diagnosis of iPD (18,19).
18F-AV-133 is an 18F-labeled dihydrotetrabenazine analog. This compound binds selectively and with high affinity to VMAT2 (19,20) and can sensitively detect monoaminergic terminal reductions in patients with Parkinson disease (PD) and dementia with Lewy bodies (15). Although DAT imaging has been shown to improve diagnostic accuracy for iPD and have substantial management impact in CUPS, VMAT2 imaging with 18F-AV-133 has potential advantages such as better image quality and quantification, shorter time between tracer administration and scanning, shorter scan duration, and no requirement for prior blockade of the thyroid to prevent radioactive iodine uptake.
This study aimed to assess the impact of VMAT2 imaging using 18F-AV133, on management of clinically uncertain Parkinson syndrome.
MATERIALS AND METHODS
Study Design and Subject Selection
The study was approved by the Austin Health Human Research Ethics Committee. All participants provided written informed consent before their participation in the study. The study used a prospective experimental study design. Study participants comprised patients with atypical features of parkinsonism who were referred from movement disorder specialists practicing in private or public clinics across Melbourne, Australia.
Inclusion Criteria
Participants were required to be older than 18 y and English speaking. Participants were also required to have more than 7 y of education and to have adequate visual and auditory acuity to complete the clinical and cognitive assessment.
Exclusion Criteria
Patients were excluded if they had a history of cancer (other than skin or in situ prostate cancer) within the previous 5 y. Persons were also excluded if they were unable to give informed written consent.
Pregnancy was excluded in women of childbearing age by blood test just before the scan.
Assessments and Evaluation
Each participant underwent neuropsychologic assessment and neurologic examination. The neuropsychologic assessment involved the Mini-Mental State Examination, clinical dementia rating, hospital anxiety and depression scale, logical memory score, and verbal fluency scores. The neurologic evaluation comprised the Hoehn and Yahr score and a motor subscale of the Unified Parkinson Disease Rating Scale score.
Questionnaires
The referring neurologists were required to complete diagnosis and management questionnaires at baseline and after the release of the AV-133 PET scan results.
The baseline questionnaire detailed the current management; the investigations completed; the most likely diagnosis from 6 categories (psychosomatic, dystonia, neurodegenerative, drug-induced, cerebrovascular disease, other [including essential tremor]); and the confidence, expressed as a percentage, in that diagnosis. If the clinician thought the diagnosis was a neurodegenerative disorder, they were required to specify whether this was thought to be PD, multiple-system atrophy, progressive supranuclear palsy, cortical basal ganglionic degeneration, uncertain type, or other. Their confidence in the specific neurodegenerative disorder diagnosis was also recorded.
Details of proposed long-term management, including medication plan, referral to other health providers, and follow-up visit frequency, were also recorded. Subsequent questionnaires were issued after the scan results were released and the management impact determined on these same areas.
Management Impact
Outcome measures were defined as high, moderate, or low management impact. Management impact was defined as high if there was a change in diagnostic category from a progressive neurodegenerative disorder to a nondegenerative disorder or vice versa after the PET scan results, moderate if there was a resultant change in medication, or low if the results confirmed clinical diagnosis or the result was discrepant and ignored.
Confidence in diagnosis was rated into 3 categories as possible (<50%), likely (>50%), and highly likely/definite (>90%) both before and after the release of scan results.
PET Acquisition
A 20-min emission PET scan was obtained 2 h after intravenous administration of approximately 250 MBq of 18F-AV133. The images were reconstructed using a 3-dimensional row-action maximum-likelihood algorithm (15) and were corrected for attenuation using a transmission scan from a rotating 137Cs source.
Image Analysis
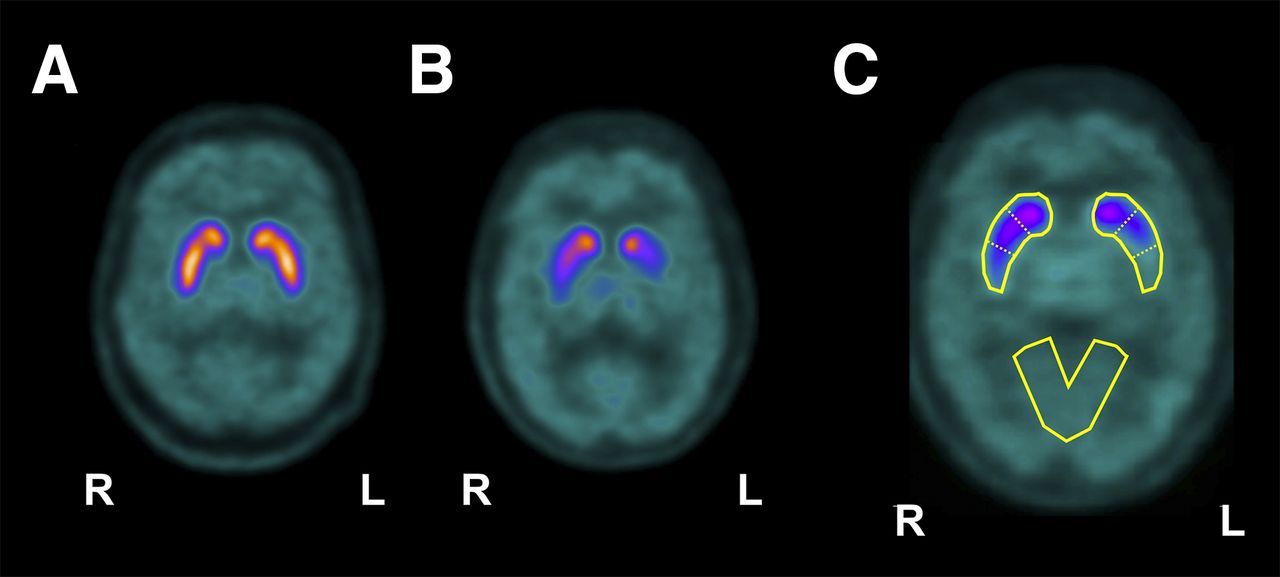
As previously reported, tissue ratios for the caudate nuclei and anterior and posterior putamen were calculated using the primary visual cortex as a reference region, and compared with a locally derived reference range (Fig. 1) (21). A reduction of more than 50% in the most affected posterior putamen compared with the mean of a previously obtained normal control group (Fig. 2) was considered consistent with iPD or PD plus syndrome. This cutoff was based on observations from histopathologic studies that have documented loss of more than 50% of dopamine terminal markers in the posterior putamen in early symptomatic PD cases (22).

Representative 18F-AV-133 VMAT2 PET images of a normal age-matched volunteer (A) showing symmetric distribution of the tracer in basal ganglia, and PD patient (B) showing marked reduced and asymmetric tracer retention in basal ganglia, more pronounced in left putamen. Images were quantified using predefined region-of-interest template (C) that was applied on spatially normalized 18F-AV-133 images. Region-of-interest template sampled caudate nuclei, anterior and posterior putamen, and primary visual cortex that was used as reference region.

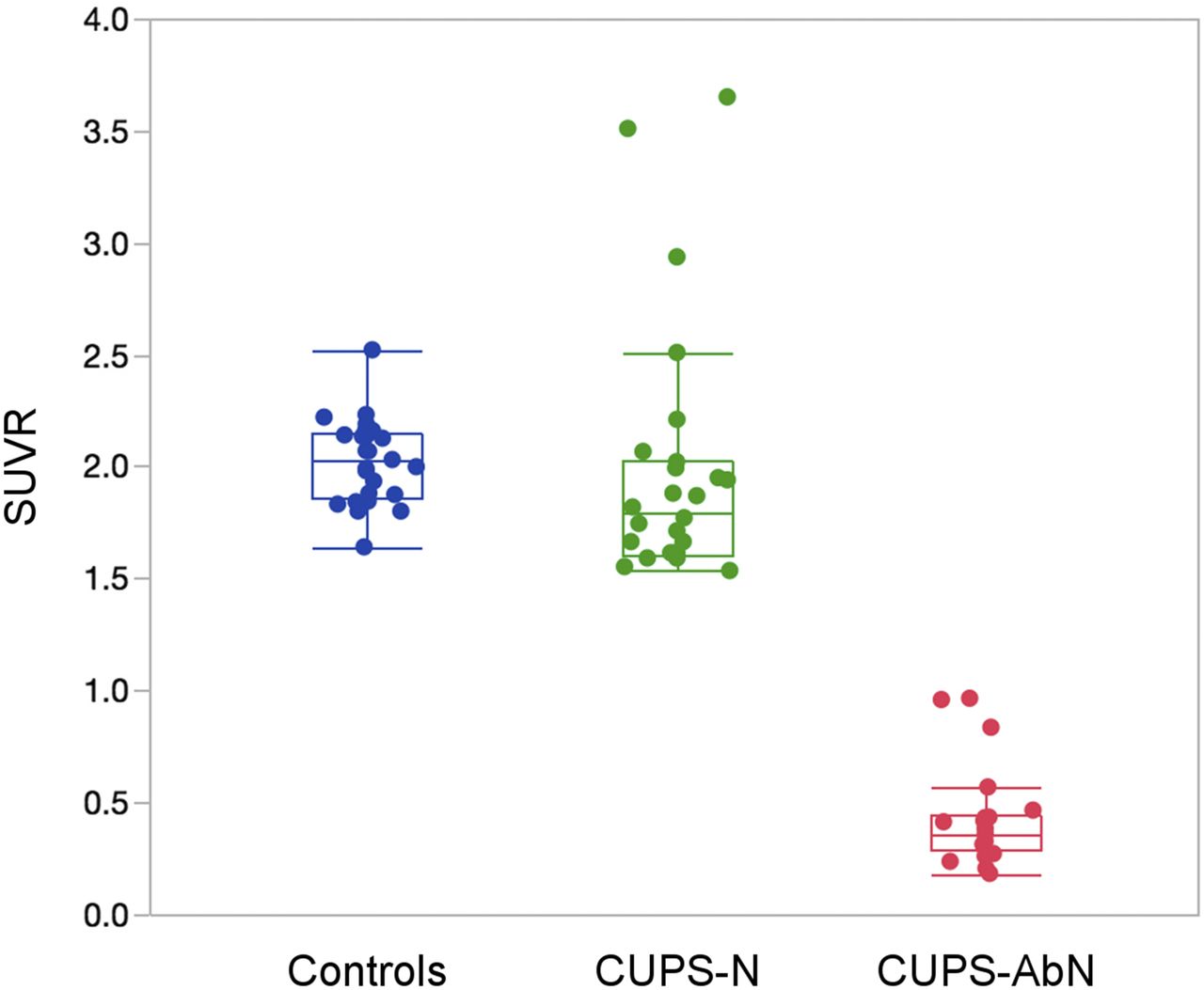
SUV ratios of posterior putamen in normal controls (blue), CUPS with normal scan findings (CUPS-N) (green), and CUPS with abnormal scan findings (CUPS-AbN) (red).
RESULTS
Patient Demographics
The study consisted of 47 participants. Patient demographics are displayed in Table 1. There were 25 men (53%) and 22 women (47%) who ranged in age from 21 to 80 y. The mean age was 56.9 y. Only 1 participant had a Hoehn and Yahr score of zero, and no one had a score of 4.0 or 5.0. The mean baseline Mini–Mental State Examination score was 29, and no participant had a score below 25.
Patient Demographics
Diagnosis Before Scanning
Most patients (30 [64%]) were initially diagnosed as having neurodegenerative disease, as seen in Table 2. Of these, 20 were thought to have iPD, 7 unknown, 1 multiple-system atrophy, 1 progressive supranuclear palsy, and 1 other. Seven (15%) patients were thought to have a psychogenic condition; 4 (9%) were diagnosed as dystonia and 3 (6%) as drug-induced. Three patients were thought to have essential tremor (classified as other).
Scan Results and Diagnosis Before and After Results
Scan Findings
Twenty-two patients (47%) had abnormal scan findings (i.e., more than 50% reduction in 18F-AV133 uptake in the posterior putamen). In these abnormal scan findings, reduction was more than 80% in 14, 60%–79% in 5, and 51%–59% in 2 (Fig. 2). Age correction was applied but had no impact on the measures.
Diagnosis Change
Data for the diagnosis change was obtained from the management impact questionnaires. More than 75% of the postscan release questionnaires were completed within 4 mo of the baseline questionnaire, and all were returned within a year.
The initial diagnosis was changed in 12 (26%) patients after the release of the scan results. One of these was a change from dystonia to psychogenic and so was not considered as high impact based on our definition. Of the normal scan findings, the diagnosis was changed in 36% (9/25), and that value was 9% (2/22) for the abnormal scan findings.
Medication Change
With regard to medications, 53% (25/47) of the participants had changes to their regimen after the scan results were released. When the scan results were abnormal, 54.5% (12/22) had change, predominantly an increase in PD treatment, whereas 52% (13/25) of those with a normal scan finding had change, predominantly withdrawal of PD medications.
Management Impact and Diagnostic Confidence
Management impact was high in 23%, moderate in 38%, and low in 39% of patients (Fig. 3). Before the PET scan, clinician confidence was high (very likely/definite) for only 11% of the patients, but increased to 81% after the release of the scan results. Overall, there was an increase in diagnostic confidence in 74% of patients after the scan.
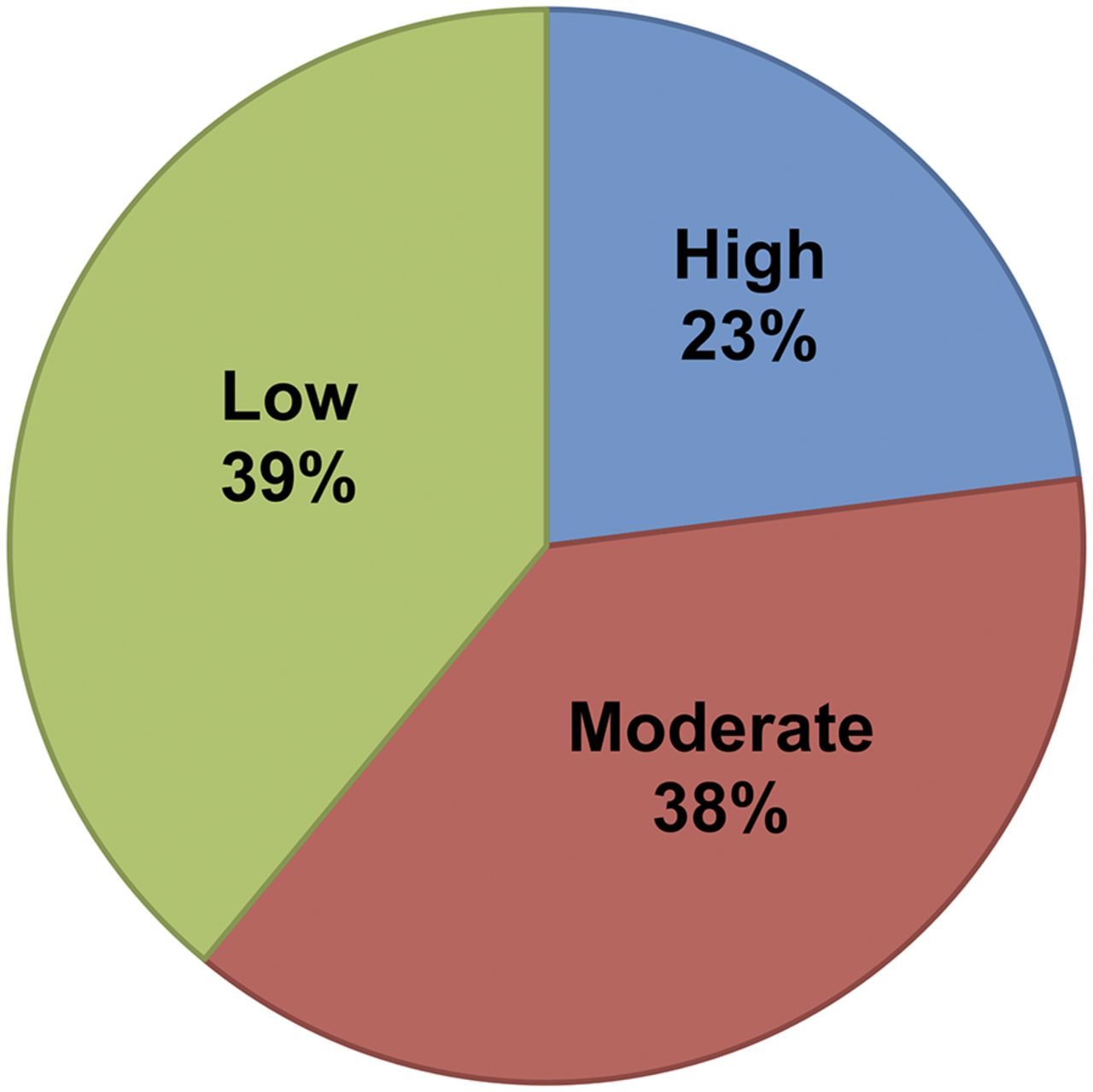
Postscan management impact.
Confidence in the diagnosis increased after scanning, as illustrated in Table 3. This increase in confidence occurred whether the scan results were abnormal (16/22 or 73%) or normal (19/25 or 76%). In addition, 4 of the 25 (16%) normal scan findings resulted in a decrease in confidence with or without a change in diagnosis. This was only the case for 1 of the 22 abnormal scan results (4.5%).
Clinical Confidence Before and After Scanning
DISCUSSION
This study sought to determine whether the result of VMAT2 imaging with 18F-AV133 affected the diagnosis and clinical management of patients with CUPS. Our findings indicated a moderate to high impact in 61% of the cases (38% moderate and 23% high impact). We obtained an increase in diagnostic confidence in 74% of cases after the scan result was released and a 23% change in diagnosis.
These findings are comparable to studies using the SPECT DAT imaging agent 123I FP-CIT (DaTscan) when assessing loss of striatal dopaminergic innervation in CUPS. Seifert et al. reported that the DaTscan result led to a change of diagnosis in 31% and impacted clinical management in 58% of their patients (23). This is comparable to our values of 23% diagnosis change and 61% impact (combined moderate and high). However, their study was retrospective compared with our prospective design. Løkkegaard et al. demonstrated that the results of DaTscan led to a change of either diagnosis or clinical management in 27% of patients (24).
Clinician confidence was also affected by the 18F-AV133 scans. Clinician confidence increased in 74% of the cases after the scan result was revealed. DaTscan studies conducted by both Kupsch et al. (25) and Seifert et al. (23) also demonstrated significant changes in confidence in diagnosis after release of results. Interestingly, Kupsch et al. followed up after 4 wk, 12 wk, and 1 y and reported a further increase in confidence in the diagnosis at each follow-up interval (25), indicating that diagnosis assisted by striatal dopaminergic innervation imaging remained robust over time.
In our study, clinician confidence was equally increased whether the scan was normal or abnormal. This contrasts with the findings by Catafau et al. (7) in their study with DaTscan. They found an increase in confidence when the scan results were abnormal but a decrease in confidence when the scan results were normal (7).
The medication regimen was affected in 53% of the patients. The changes ranged from commencement of a new agent and cessation of an agent to change in the dose. Studies conducted with DaTscan also attributed a significant portion of their management change after scanning to medication changes (7,23–25).
Of the 22 patients with abnormal scan findings, 14 had a reduction in VMAT2 binding compared with the mean of controls, of more than 80%. This highlights the fact that diagnostic uncertainty can manifest even with a high degree of dopaminergic loss.
We chose a reduction in relative binding in the posterior putamen of greater than 50% to be abnormal. This value was chosen because previous postmortem studies have shown that a reduction of about 50% of dopaminergic neurons was necessary to produce clinical symptoms sufficient for the diagnosis of PD to be made (22). In our group, 50% reduction corresponds to 3 SDs below the mean of a reference group consisting of healthy normal adults who underwent VMAT2 PET imaging with 18F-AV133. As such, we believe that we are justified in using that value for this application though it would not be appropriate if preclinical detection of iPD is the goal.
There were some limitations to this study. First, there was no pathologic confirmation of the diagnosis in those with abnormal scans nor was there confirmation from longitudinal clinical follow-up. Prior studies have demonstrated a high concordance of DaTscan findings with postmortem diagnosis, and similar studies would be useful for VMAT2 imaging.
The study population was generally referred from movement disorder specialists in Melbourne, and so the demographics of the study participants reflect that of the local, predominantly Caucasian, population. There was no control arm in this study such as CUPS patients without VMAT2 imaging. Therefore, it is possible that diagnosis and clinician confidence changed because of the passage of time or repeated clinical assessment. A controlled study is needed to address this issue.
The findings in this study provide further evidence for the use of imaging as a complementary aide in managing CUPS. Although the findings are similar to those obtained with the SPECT imaging agent DaTscan, 18F-AV133 PET has logistic advantages including shorter uptake and scanning times and no patient preparation. 18F-AV133 PET also produces high-quality images that allow more accurate quantification, and this may be important if monitoring change over time as in therapeutic drug trials.
CONCLUSION
Significant impact in management and confidence in the diagnosis was derived from imaging VMAT2 with 18F-AV133 and PET in patients with CUPS.
DISCLOSURE
This was an investigator-initiated study supported by a grant from Avid Radiopharmaceuticals. This study was also supported in part by funds from the Austin Hospital Medical Research Foundation. Christopher Rowe, MD, has received research grants from GE Healthcare, Piramal Imaging, Navidea, and Avid Radiopharmaceuticals. Victor L. Villemagne, MD, has been an honorary speaker for Avid Radiopharmaceuticals. No other potential conflict of interest relevant to this article was reported.
Acknowledgments
We thank Drs. Andrew Evans, David Williams, John Drago, Andrew Hughes, John Merory, Katrina Reardon, and Katya Kotschet for their role in patient recruitment.
Footnotes
Published online May 10, 2017.
- © 2017 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication December 24, 2016.
- Accepted for publication April 13, 2017.





{kind=link}
{kind=link}
{kind=link}