


Abstract
We previously reported aggregate data showing that PET was associated with a change in intended management for over one third of patients participating in the National Oncologic PET Registry (NOPR). Here, we present results for specific cancer types and indications for testing. Methods: The NOPR collected questionnaire data from referring physicians on intended management before and after PET. Data were available from 40,863 PET studies done at 1,368 centers. The impact of PET was assessed for 18 cancer types in patients with pathologically confirmed cancer by type and indication for testing (initial staging, restaging, or detection of suspected recurrence), other than treatment monitoring. Results: When intended management was classified as treatment or nontreatment, physicians changed their intended management for 38.0% of cases (95% confidence interval = 37.6%−38.5%). The frequencies of changes in management ranged from 48.7% for myeloma to 31.4% for nonmelanoma skin cancer. Comparisons across testing indications revealed that only in multiple myeloma did PET have a consistently greater impact on intended management. When the intended management plan before PET was treatment, a change in the intent of treatment (curative vs. palliative) or a major change in the modality of treatment occurred at similar frequencies across different cancer types. Conclusion: The impact of PET on physicians' intended management for patients with known cancer was consistent across cancer types.
PET, alone or integrated with CT (PET/CT) (hereafter collectively referred to as PET) and performed with the radiopharmaceutical 18F-FDG is a molecular imaging technique that assesses regional glucose metabolism (1). In clinical practice, 18F-FDG PET is most widely used for the imaging of patients with cancer. Currently, the Centers for Medicare & Medicaid Services (CMS) provides coverage for PET performed on Medicare beneficiaries for 9 common malignancies (2). In 2005, the CMS established a new coverage policy, called “coverage with evidence development” (2,3), to expand the evidence base for evaluating selected promising technologies, including PET for noncovered indications. In response to this policy change, the National Oncologic PET Registry (NOPR) was developed to collect data on the clinical utility of PET to meet requirements for coverage with evidence development (4). The NOPR opened in May 2006.
We recently reported aggregate results from the first year of data collected by the NOPR on the impact of the use of PET for cancer diagnosis, initial staging, restaging, or detection of suspected recurrences of previously noncovered cancers in Medicare beneficiaries (5). Overall, we found that the impact of PET on intended management for these previously noncovered cancers was similar to that previously reported for covered cancers. For the purposes of guiding clinical practice and shaping coverage policy, it is important to determine the relative effects of PET for different cancer types and indications for testing. In this article, we report results by cancer type for the first 2 y of data collected by the NOPR from 40,863 PET scans. We restricted our analysis to the use of PET for staging, restaging, or detection of suspected recurrences in patients with pathologically proven cancers.
MATERIALS AND METHODS
The NOPR is a prospective data registry that collects information from the PET facility, from the physician requesting the PET scan, and from the interpreting physician's PET report. Detailed descriptions of NOPR operations and human subject protection procedures were reported previously (6,7). Submission of data to the registry is required by CMS as a condition for coverage. All data are entered by participating PET facilities via a secure Web-based interface and are stored at the American College of Radiology. The NOPR home page and Web application, including all forms, are located at http://www.cancerPETregistry.org/.
In brief, the PET facility is responsible for collecting information from the referring physician on a “pre-PET” form and a “post-PET form.” The pre-PET form focuses on information regarding the specific indication for testing; the patient's cancer type (if known) and working stage assessment; the patient's performance status; whether the referring physician will also be the treating physician; and the referring physician's management plan if PET were not available. Once a PET scan has been completed, the PET facility uploads the PET report to the database. The final step is the completion of the post-PET form by the referring physician to assess the management plan in light of the PET findings.
Data collection is conducted in accordance with a protocol approved by the American College of Radiology Institutional Review Board. The research database consists only of cases in which both patient and physician have given consent.
Outcomes
As we reported previously (5), the primary endpoint was the impact of PET on physicians' intended management. Intended management was dichotomized as either treatment (e.g., surgery, chemotherapy, radiation, or other treatment, alone or in combination) or nontreatment (e.g., observation, noninvasive imaging, biopsy, or supportive care). A change in management was defined as a switch from treatment to nontreatment or vice versa. In our previous report (5), we noted that PET led to a change in intended management in 36.5% of cases; a switch from treatment to nontreatment was 3-fold more likely than the converse.
The inclusion of cases for which the plan before PET was imaging may have overestimated the impact of PET. Specifically, it is possible that, if these patients had alternatively undergone another type of imaging (e.g., CT or MRI), the management plan after that imaging would have been the same as the management plan after PET. To address this concern, we performed a sensitivity analysis in which all cases for which the initial management plan was additional imaging were considered to have no change in management. Specifically, cases in which the plan before PET was another type of imaging and the plan after PET was treatment were excluded from the numerator but included in the denominator in calculating the frequency of a management change. We believe that the resulting estimate represents a lower boundary of the impact of PET on intended management with respect to our primary endpoint. This calculated frequency was subsequently referred to as the “imaging-adjusted impact.”
Alternative endpoints also were assessed as previously reported (5). These approaches assessed how often the intent of planned therapies changed from curative to palliative (or vice versa) or how often a change in the type of therapy or the number of therapies (as an indirect indicator of care intensity) occurred.
Statistical Analysis
A change in intended management after PET was modeled as a binary variable on the basis of a binomial distribution. Changes were defined at the PET scan level and were assumed to be independent for different patients, cancer types, or indications for testing. A total of 13.6% of patients in the cohort (see later discussion) had 2 or more scans; however, because almost all of the multiple scans were obtained for different indications in the cancer care continuum (initial staging, restaging, or detection of suspected recurrence) over a potential 2-y period, they were treated as independent scans.
Changes in the intended management plan were analyzed for each cancer type and specific indication for testing. Only combinations of cancer types and indications with at least 200 cases were separately reported; cancer types with at least 500 cases across all indications also were separately reported. An association between 2 binary variables was quantified with an odds ratio, which was constructed by removing a base group from the entire cohort and then comparing changes in that base group with changes in the remaining cases in the cohort. For example, a change in management for prostate cancer was compared with that for all nonprostate cancers. When multiple testing was involved, a Bonferroni correction was applied to the P values. All 95% confidence intervals (CI) were 2-sided and were calculated with gaussian approximation. All statistical analyses were performed with SAS version 9.1 (SAS Institute Inc.).
RESULTS
Definition of Cohort
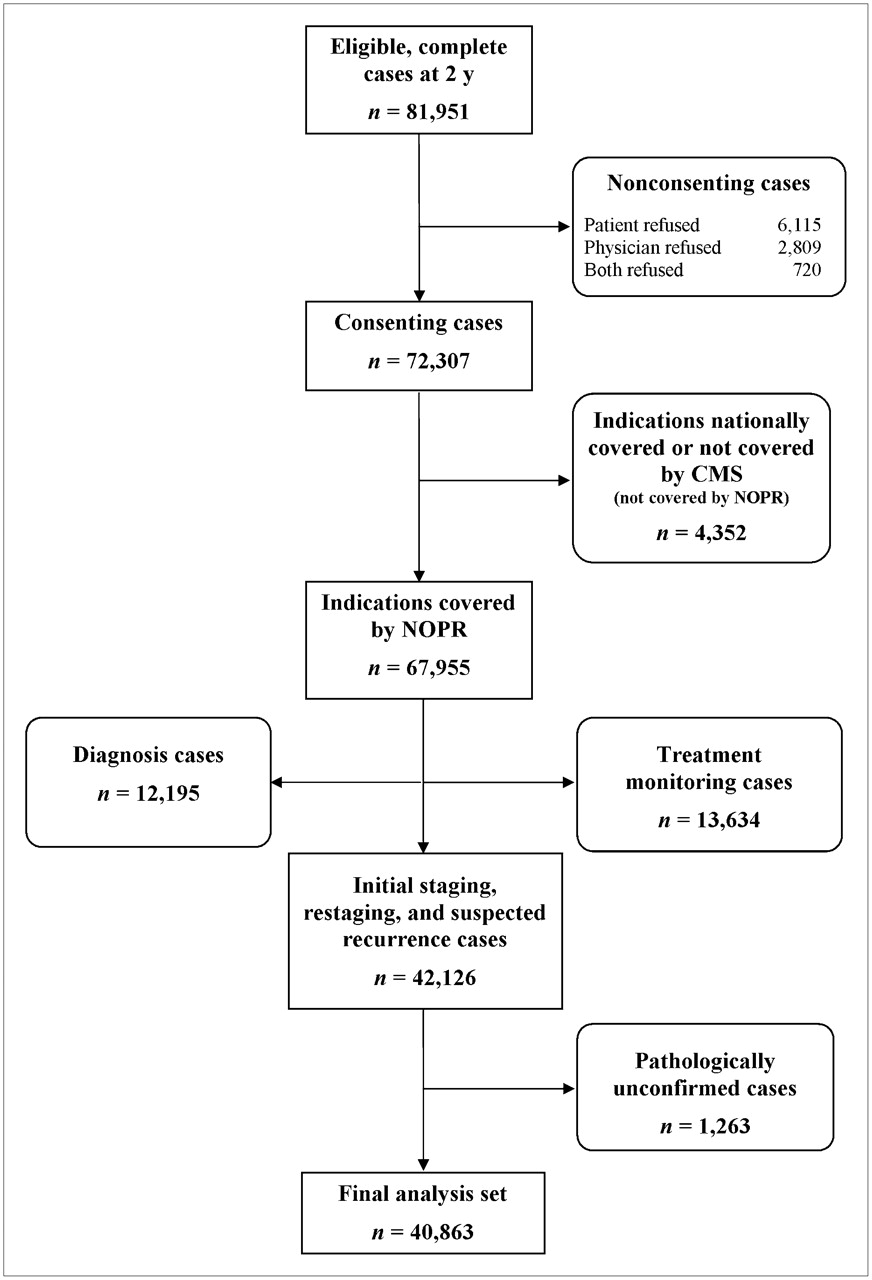
Figure 1 shows how the 2-y NOPR cohort was defined for this analysis. By definition, all patients were Medicare beneficiaries. The NOPR began accepting patients on May 8, 2006. As of May 7, 2008, 81,951 PET studies were registered, had complete data submitted, and were potentially eligible for inclusion (Fig. 1). Of these, 9,644 cases (11.8%) were excluded because the patients or the referring physicians did not consent to the use of their data for research purposes. Another 4,352 cases (5.3%) were excluded because the PET study appeared to have been requested for a cancer type and indication already covered or specifically not covered by Medicare (2).

Development of 2-y NOPR cohort (see text for details). Numbers represent PET scans, not individuals having scans.
For this analysis of the impact of PET for specific cancer types, only patients with histologically confirmed cancers of known origins and undergoing PET for initial staging, restaging, or detection of suspected recurrences were included. Therefore, we excluded cases in which PET was performed for cancer diagnosis, including cancer of unknown primary origin, or for monitoring of a response to treatment during a planned course of chemotherapy or radiotherapy. In addition, we also excluded 1,263 cases in which PET was requested for initial staging, restaging, or detection of suspected recurrences but the referring physician indicated that the cancer was not pathologically confirmed.
The final analysis cohort thus consisted of 40,863 scans performed in 34,536 patients; 14,365 scans were for initial staging of newly diagnosed cancer, 14,584 scans were for restaging of cancer after completion of a course of treatment, and 11,914 scans were for the evaluation of a suspected recurrence of a previously treated cancer.
Participating Centers and Patient Profiles
Table 1 summarizes the cohort demographics. The mean patient age was 72.4 y. There were nearly equal numbers of men and women. Most patients (88.2%) had an Eastern Cooperative Oncology Group performance status of 0 or 1. The summary cancer stage before PET was judged as no evidence of disease in 12.0% of cases, locoregional disease in 33.5%, metastatic disease in 29.4%, and unknown or uncertain in 25.1%. Most of the scans (88.7%) were obtained with a PET/CT scanner. Patients were enrolled from 1,368 PET centers across the United States. As noted earlier, 34,536 patients participated; 86.4% of patients had a single scan, and 13.6% had 2 or more scans.
NOPR Cohort Characteristics
Impact on Treatment and Nontreatment Decisions
Table 2 shows the impact of PET on intended management overall and stratified by cancer type. Overall, PET led to a change in intended management from treatment to nontreatment or vice versa in 38.0% (95% CI = 37.6%−38.5%) of cases. Among the 4,704 patients (13.6%) who had at least 2 PET scans, the frequency of a change in intended management with the first scan (39.2% [95% CI = 37.8%−40.6%]) was slightly but significantly higher than that with the second scan (6.2% [95% CI = 34.8%−37.6%]). Among the 1,167 patients who had 3 or more scans, the value for the third or subsequent scans was approximately 34%. The fraction of patients who had 2 or more scans was notably higher than average for ovarian cancer (19.5%) and myeloma (17.7%) and notably lower than average for prostate cancer (6.0%) and liver cancer (7.2%).
Impact of PET on Intended Management by Cancer Type*
There were 16 cancer types with at least 500 cases in the cohort. These are listed in Table 2, in order of descending frequency, along with the frequency of a change in intended treatment or nontreatment after PET, the odds ratio for a change in management for each specific cancer compared with other cancers, the frequency of alternative imaging as the plan before PET, and the imaging-adjusted impact on intended management.
The frequency of a change in intended management by cancer type ranged from a low of 31.4% for nonmelanoma skin cancers to a high of 48.7% for myeloma. The frequency of a change in intended management for 7 of the 16 cancer types differed significantly from that for all other types, as indicated by the odds ratio. Myeloma was the only cancer type among these 7 with an odds ratio (1.58) that was notably different from 1.0.
Table 2 also shows the imaging-adjusted impact of PET on intended management. Overall, the imaging-adjusted impact of PET was 14.7% (95% CI = 14.3%−15.0%); the cancer-specific values varied relatively little, ranging from a low of 9.6% for nonmelanoma skin cancers to 16.2% for ovarian cancer. The imaging-adjusted impact of PET for myeloma (11.5%) was lower than the average for all cancers.
Table 3 shows that, as previously reported, a change from nontreatment to treatment was substantially more likely than a change from treatment to nontreatment (30.0% vs. 8.0% overall), and this was true across all cancer types. Table 3 also shows modifications in intended management when the plan before PET was treatment. A change in the goal of treatment from curative to palliative (or vice versa) occurred in 14.1% of cases overall, with relatively little variation as a function of cancer type (range = 10.0%−18.2%). In 15.1% of cases (range = 7.3%−20.7%), when treatment was planned before PET, the plan after PET was changed to either supportive care or observation; this change occurred most often in cancer of the kidney and least often in other female genital cancers. A major change in planned treatment (e.g., from surgery to chemotherapy) occurred in 8.6% of cases overall (range = 5.1%−14.7%), most often in tumors of the liver and intrahepatic bile ducts and least often in myeloma and nonmelanoma skin cancers. A minor change in planned treatment (e.g., the addition or deletion of a mode of therapy) was more common (23.3% of cases overall) and occurred most frequently in cervical cancer (34.7%) and least frequently in myeloma (9.7%).
Details and Alternative Endpoints of Impact of PET on Intended Management by Cancer Type*
Testing Indications
Table 4 shows the aggregated results for all cancers stratified by testing indication. PET was associated with essentially equivalent changes in intended management for the testing indications: 39.8% of cases for initial staging, 35.9% for restaging, and 38.5% for detection of suspected recurrences. On the basis of the imaging-adjusted impact, however, the impact of PET was significantly greater when PET was performed for detection of suspected recurrences (18.8%; odds ratio = 1.56) than when it was performed for initial staging (13.4%) or restaging (12.6%). For each testing indication, the frequency of a change in intended management with PET/CT was slightly but not significantly greater than that with PET alone (data not shown).
Summary by Testing Indication for All Cancer Types in NOPR
Initial Staging.
Table 5 summarizes the impact of PET on intended management for initial staging by cancer type. Prostate cancer was the most common cancer type in the initial staging subgroup. The impacts of PET by cancer type were tightly clustered, except that the impact was lower in patients with prostate cancer (32.0%; odds ratio = 0.67) and higher in those with myeloma (52.2%; odds ratio = 1.68). However, the imaging-adjusted impacts for myeloma and prostate cancer were not different from those for other cancer types.
Impact of PET on Intended Management for Initial Staging by Cancer Type*
Restaging.
Table 6 shows the impact of PET performed for cancer restaging. For this indication, the impact of PET on intended management showed the widest variation by cancer type within a testing indication. PET studies in patients with connective tissue, nonmelanoma skin, and cervical cancers led to changes in intended management in about 25% of patients; this frequency was lower than that for other cancers (odds ratios = 0.53–0.69). The lower frequency of change in management for these cancers persisted in the imaging-adjusted impact as well (range = 6.3%−10.5%).
Impact of PET on Intended Management for Restaging by Cancer Type*
Detection of Suspected Recurrence.
Table 7 summarizes the impact of PET performed for detection of suspected cancer recurrences. Suspected recurrences of ovarian and prostate cancers were by far the most frequent in our cohort. According to our primary definition of a change in intended management, patients with myeloma (50.9%) and ovarian cancer (44.5%) were more likely and those with kidney cancer (32.4%) and stomach cancer (29.3%) were less likely to have a change in management after PET. However, on the basis of the imaging-adjusted impact, the only cancer type for which a notable difference from other cancer types was seen was primary brain cancer; for the latter, a change in management occurred in 28.4% of patients (odds ratio = 1.73).
Impact of PET on Intended Management for Detection of Suspected Recurrence by Cancer Type*
DISCUSSION
The large number of patients enrolled in the NOPR presented an unprecedented opportunity to assess the relative impact of PET on intended patient management across a diversity of cancer types. Here, we report on the relative impact of PET on patients with 18 different types of known cancers for 3 distinct indications (initial staging, restaging, and detection of suspected recurrence). With the notable sole exception of multiple myeloma, there were no cancer types for which the impact of PET was consistently higher or lower than average across all the indications studied. Moreover, there were only a small number of instances in which the change in management for a particular combination of cancer type and indication was significantly different from that for other cancer types studied for that indication. In our opinion, these few combinations are not likely to reflect major biologic or clinically meaningful differences in the ability of PET to influence patient management.
Our initial report of overall NOPR results (5) included data for PET scans obtained in some patients without documented cancer or with cancer of undocumented origin; these scans were obtained to determine whether a suspect lesion was cancer, to detect a primary tumor site in a patient with a presumed paraneoplastic syndrome, or to detect a primary tumor site in a patient with confirmed or strongly suspected metastatic disease. For the current analysis of the results for individual cancer types, we excluded data collected for these cancer diagnosis indications, because our goal was to assess the performance of PET in relation to cancer type and this goal required limiting the dataset to pathologically confirmed cancers of known origins. The impact of PET in an expanded cohort for these cancer diagnosis indications will be reported separately.
Our analysis of the imaging-adjusted impact of PET on intended management showed an overall change in 14.7% of patients, with a modestly higher impact in the subset of patients referred for the detection of suspected recurrences. As noted earlier, this imaging-adjusted impact estimate can be considered a hypothetical lower boundary of the impact of PET, but the true impact is likely to be higher. This is because it has been amply documented that PET is generally more sensitive and specific than CT, MRI, or other imaging methods for the detection of cancer (on both a patient basis and a lesion basis) (8–11). Moreover, it has been shown that the improved accuracy of PET compared with conventional imaging methods leads to more frequent upstaging or downstaging and, accordingly, to more frequent management changes.
The imaging-adjusted impact of PET seemed to show less variation across cancer types than did the primary nontreatment–treatment endpoint. The reasons for this finding are unclear. The NOPR did not collect information about whether and when other imaging procedures may have been performed before PET. Thus, we are unable to determine which of several possible circumstances might have led referring physicians to select another type of imaging as their intended management plan if PET was not available. Possible circumstances include situations in which PET was requested as the first imaging test instead of as an alternative imaging procedure, PET was requested after CT or MRI of one body region to evaluate the rest of the body (the alternative being to perform CT or MRI of the rest of the body), PET was requested immediately after inconclusive CT (the alternative being to perform MRI), or PET was requested for interval follow-up of previously inconclusive findings on CT or MRI (the alternative being to repeat those tests).
The NOPR data provide no direct insights into the factors that influence a referring physician to order PET during the continuum of care of a cancer patient. The practice-based nature of the NOPR data and our primary finding of little variation in impact across cancer types—despite the expectation that PET would be of limited value for some cancers, such as those that are typically considered to have relatively poor 18F-FDG avidity (e.g., prostate carcinoma (12))—may indicate that referring physicians are quite selective in ordering PET.
To estimate the number of patients potentially eligible for participation in the NOPR, we obtained incidence data by cancer type for patients over age 65 from the United States Cancer Statistics for 2004 (the most recent year for which data are available) (13). These were compared with the numbers of NOPR PET scans in 2007 for the same cancer types for patients over age 65. Using this simple approximation, we estimated that for most cancer types, between 10% and 20% of patients participated in the NOPR. Our estimate ranged from a low of about 3% of prostate cancer patients to about 38% of ovarian cancer patients (data not shown).
CONCLUSION
We believe that the NOPR results show the impact of PET to be strikingly consistent for a wide range of cancers. Accordingly, the use of PET in management for patients with known cancer should not be restricted by cancer type or testing indication.
Acknowledgments
We thank the many individuals at the Academy of Molecular Imaging, American College of Radiology, American College of Radiology Imaging Network, Society of Nuclear Medicine, American Society of Clinical Oncology, and Centers for Medicare & Medicaid Services who contributed to the development of the National Oncologic PET Registry. Funding for development of the National Oncologic PET Registry was provided by the Academy for Molecular Imaging, but the registry is otherwise self-supported by fees paid by participating PET facilities.
Footnotes
-
COPYRIGHT © 2008 by the Society of Nuclear Medicine, Inc.
References
- Received for publication August 7, 2008.
- Accepted for publication September 9, 2008.





{kind=link}
Jump to section
Related Articles
Cited By...
- Impact of 68Ga-PSMA-11 PET on the Management of Recurrent Prostate Cancer in a Prospective Single-Arm Clinical Trial
- Proceedings: Pathways for Successful Translation of New Imaging Agents and Modalities--Phase III Studies
- Increasing PET Use in Small Cell Lung Cancer: Survival Improvement and Stage Migration in the VA Central Cancer Registry
- Controversies on the Use of Radioiodine in Thyroid Cancer: We Need More and Better Data
- Intended Versus Inferred Treatment After 18F-Fluoride PET Performed for Evaluation of Osseous Metastatic Disease in the National Oncologic PET Registry
- The National Oncologic PET Registry (NOPR): A Monumental Effort by a Few Leaders
- Hospice Admission and Survival After 18F-Fluoride PET Performed for Evaluation of Osseous Metastatic Disease in the National Oncologic PET Registry
- PET of Glucose Metabolism and Cellular Proliferation in Prostate Cancer
- Impact on Patient Management of [18F]-Fluorodeoxyglucose-Positron Emission Tomography (PET) Used for Cancer Diagnosis: Analysis of Data From the National Oncologic PET Registry
- 18F-Fluoride PET Used for Treatment Monitoring of Systemic Cancer Therapy: Results from the National Oncologic PET Registry
- Impact of 18F-Fluoride PET on Intended Management of Patients with Cancers Other Than Prostate Cancer: Results from the National Oncologic PET Registry
- Impact of 18F-Fluoride PET in Patients with Known Prostate Cancer: Initial Results from the National Oncologic PET Registry
- Application of FDG-PET in Cervical Cancer and Endometrial Cancer: Utility and Future Prospects
- Intended Versus Inferred Care After PET Performed for Initial Staging in the National Oncologic PET Registry
- The Medical Imaging & Technology Alliance Conference on Research Endpoints Appropriate for Medicare Coverage of New PET Radiopharmaceuticals
- The Lack of Evidence for PET or PET/CT Surveillance of Patients with Treated Lymphoma, Colorectal Cancer, and Head and Neck Cancer: A Systematic Review
- Impact of 18F-FDG PET Used After Initial Treatment of Cancer: Comparison of the National Oncologic PET Registry 2006 and 2009 Cohorts
- Contribution of Imaging to Cancer Care Costs
- Nuclear Medicine at a Crossroads
- Incidental Diagnosis of Thrombus Within an Aneurysm on 18F-FDG PET/CT: Frequency in 926 Patients
- Prostate Cancer: PET with 18F-FDG, 18F- or 11C-Acetate, and 18F- or 11C-Choline
- Whole-Body 18F-FDG PET/CT: The Need for a Standardized Field of View--A Referring-Physician Aid
- Clinical Value of Fluorine-18 2-Fluoro-2-Deoxy-D-Glucose Positron Emission Tomography/Computed Tomography in Bladder Cancer
- Economic Evaluation of PET and PET/CT in Oncology: Evidence and Methodologic Approaches
- Economic Evaluation of PET and PET/CT in Oncology: Evidence and Methodologic Approaches
- PET and PET/CT Reports: Observations from the National Oncologic PET Registry
- The PET/CT Report: The Most Important Part of the Study
- Superiority of Magnetic Resonance Imaging Over Conventional Radiographs in Multiple Myeloma
- Expert Opinions on Positron Emission Tomography and Computed Tomography Imaging in Lymphoma
- A new pet for myeloma
- NCCN Task Force: Clinical Utility of PET in a Variety of Tumor Types