


Abstract
Since 2006, the National Oncologic PET Registry has collected prospective data on 18F-FDG PET performed for cancer indications in Medicare beneficiaries under the coverage-with-evidence-development (CED) policy of the Centers for Medicare & Medicaid Services. In April 2009, coverage for PET performed to inform the initial treatment strategy of most solid tumors was expanded by the Centers for Medicare & Medicaid Services, but they continued to require CED for subsequent treatment strategy evaluations for many cancers. Methods: For all years, we assessed National Oncologic PET Registry data for bladder, kidney, pancreas, prostate, stomach, small cell lung, uterine, and all other cancers that required CED. We compared clinical profiles and changes in intended management by interval (before or after April 2009, designated as the 2006 and 2009 cohorts) for PET scans performed for restaging or suspected recurrence (2006, n = 30,911; 2009, n = 54,747) or for chemotherapy monitoring (2006, n = 10,234; 2009, n = 15,611). Results: There were slight differences between time periods but little difference by cancer type or patient age within a time period. For restaging or suspected recurrence, comparing the 2006 and 2009 cohorts, total change in intended management for all cancer types was about 33% in those younger than 65 y and about 35% in those older than 65 y (range by cancer type, 31%–41%). The referring physician impression of disease extent (restaging) or prognosis (chemotherapy monitoring) after PET was similar between cohorts. In the 2009 cohort, PET for chemotherapy monitoring was associated with a 25% increase in plans to continue therapy and a complementary decline in plans to adjust therapy. The greatest management impact of PET was during chemotherapy monitoring in the 2009 cohort, where a post-PET prognosis judged to be worse than before PET was associated with a plan to discontinue that therapy in 90% and to change to a different therapy in 65%. Conclusion: Our data demonstrate a similar impact of PET on planned management of cancer patients before and after the 2009 expansion of coverage. These results strongly suggest it is unlikely that new useful information will be obtained by extending the coverage of certain cancer types and indications only under CED. Future research on advanced imaging in the management of patients with cancer should focus on optimal sequencing and frequency of PET and other imaging modalities.
Over the last 15 y, the Centers for Medicare & Medicaid Services (CMS) has sequentially expanded the coverage of PET and integrated PET/CT with 18F-FDG for Medicare beneficiaries on a cancer-by-cancer and indication-by-indication basis (1). Since 2001, 18F-FDG PET has been covered across the cancer management continuum (excluding treatment monitoring and surveillance) for non–small cell lung, colorectal, esophageal, and head and neck cancers, as well as melanoma and lymphoma. In addition, for more narrowly defined indications, PET was also covered for breast, thyroid, and cervical cancers (2). However, as of 2005, one fourth of Medicare beneficiaries who developed cancer had a noncovered type of cancer (e.g., pancreatic cancer or endometrial cancer) (3). For these less common cancer types, policymakers and the oncology community recognized it was unlikely that sufficient clinical evidence would be developed to inform a PET coverage decision on a cancer-by-cancer and indication-by-indication basis, each requiring a new coverage decision by CMS. Therefore, in 2005, CMS announced a new coverage mechanism for the otherwise noncovered cancers and indications under its coverage-with-evidence-development (CED) policy (4,5). In response to the CED requirements, the National Oncologic PET Registry (NOPR) was created under the sponsorship of the Academy of Molecular Imaging. The NOPR opened for accrual in 2006, thereby allowing Medicare beneficiaries with these less common cancer types to have equal access to PET in order to inform clinical management decisions, in conjunction with prospective data collection within the registry (5,6). The primary objective of the NOPR is to measure the impact of PET on the referring physicians’ intended patient management by collecting questionnaire data before PET and again after the PET results are available for decision making.
Previously, we have reported NOPR findings on the impact of PET on intended patient management, including analyses of data collected during the first year of operation, 2-y data restricted to patients with confirmed cancer, data related to the use of PET as an adjunct for treatment monitoring, and data for dedicated brain PET (7–10). The common result of these different analyses was that the results of PET were associated with a reported change in intended management in about one third of cases, with minimal clinically important differences across analyses by cancer type or indication.
In part as a result of these publications, in April 2009 CMS substantially revised its coverage policy for cancer-related PET (1). For all solid tumors (other than prostate cancer), PET became a universally covered one-time service to determine the location and tumor extent for initial treatment planning. However, CMS made much more conservative changes in its coverage of PET used for planning a subsequent treatment strategy: new coverage of this type was offered only to patients with ovarian and cervical cancers, and myeloma. As a result, for a long list of infrequent cancer types, which together represent about 10% of incident cases in the elderly, PET outside of initial management continued to be covered by CMS only under the CED program.
In this report, we compare the impact of PET on intended management for the 7 most common cancer types that remained in NOPR after 2009 (bladder, kidney, pancreas, prostate, small cell lung, stomach, and uterus) and an aggregation of all other types for the periods before and after April 2009 (designated NOPR 2006 and NOPR 2009, respectively) when the use was categorized as subsequent treatment planning, including restaging or detection of suspected recurrence (henceforth collectively designated as restaging) or treatment monitoring. We hypothesized that there would be no clinically meaningful differences between the NOPR 2006 and NOPR 2009 cohorts for these cancer types individually or in aggregate.
MATERIALS AND METHODS
NOPR Design and Workflow
The NOPR is a prospective data registry that collects information from the PET facility, from the physician requesting the PET scan, and from the interpreting physician's PET report. Detailed descriptions of NOPR operations, human subject protection procedures, and results for the impact of PET on physicians’ intended management were previously reported (7–10). Both patient and physician consent were required for the research use of their data. The research conducted using NOPR data is registered as NCT00868582 at ClinicalTrials.gov.
In brief, the PET facility is responsible for collecting referring physician responses on a pre-PET form and on a post-PET form. The pre-PET form collects the specific testing indication, the patient's cancer type, a working stage assessment, the performance status, and the referring physician's management plans if PET were unavailable. After PET completion, the PET facility uploads the PET report to the database. The final step is the completion of the post-PET form by the referring physician to record the management plan chosen in light of the PET findings.
Endpoints and Analysis Plan
For all indications, the primary endpoint was the impact of PET on physicians’ intended management dichotomized as either “treatment” (e.g., surgery, chemotherapy, radiation, or other active treatment for the cancer, alone or in combination) or “nontreatment” (e.g., observation, alternative imaging, or other noninvasive testing, biopsy, or supportive care). A “change in management” was defined as a switch from treatment to nontreatment or vice versa. Our prior reports found that PET led to a change in intended management in 35%–40% of cases, with a switch from treatment to nontreatment being 3-fold more likely than the converse (8,9).
We also calculated an “imaging-adjusted impact” score, in which cases were excluded from the numerator when the plan before PET was another type of imaging and the plan after PET was treatment. These cases were, however, included in the denominator in calculating the frequency of a management change (8). We believe this method reflects a lower boundary for the impact of PET on intended management, because it assumes that the impact of PET would be the same as the alternative mode of imaging.
Treatment monitoring refers to the use of PET to monitor tumor response to treatment during a planned course of therapy (usually when a change in therapy is being considered) (7). Since the purpose of scanning done for treatment monitoring differs from that done for restaging, additional data were collected on the pre-PET questionnaire for this indication, including treatment goal (curative vs. palliative) and estimated prognosis. Beginning in 2009, further additions to the pre-PET form included duration of treatment before imaging and impression of response to date. The specific drugs used and further details of preceding treatment (if metastatic disease) were beyond the scope of the registry. Given that the patient was currently receiving therapy, the endpoints were continuing, modifying, switching, or stopping therapy, as well as first performing biopsy or other imaging. For this report, we restricted our assessment to chemotherapy monitoring.
NOPR 2006–2011 Accrual
NOPR 2006 opened for patient accrual on May 8, 2006, and closed on April 3, 2009. Nearly 1,900 PET facilities representing more than 90% of all U.S. PET sites participated. Complete data were submitted for approximately 133,000 scans. NOPR 2009 opened on April 6, 2009. As of November 30, 2011, complete data were submitted for about 72,000 scans. The research dataset, which consists of cases with both patient and referring physician consent for research, represented approximately 88% of scans and varied minimally from year to year.
Cancer Types
Bladder, kidney, pancreas, prostate, small cell lung, stomach, and uterine cancers were the highest-frequency cancer types for which the NOPR data collection requirements were in effect for both the 2006 and the 2009 cohorts. These 7 cancer types represent about 80% of all cases in NOPR 2009. All remaining solid cancer types (except for cervical cancer) were combined into an aggregate “other” category. Cervical cancer was not included because the CED requirement for this cancer was removed by CMS shortly after the beginning of NOPR 2009. The average monthly accrual rate for the included cancers and indications doubled in NOPR 2009, compared with NOPR 2006.
Statistical Analysis
A change in intended management after PET was modeled as a binary variable on the basis of a binomial distribution. Changes were defined at the PET scan level: for patients having more than one NOPR PET scan, the impact on management was treated as independent of preceding findings.
For comparisons of the frequency of change in intended management in the 2006 and 2009 cohorts, we used χ2 analysis. The 95% confidence intervals are constructed with the exact method for binomial distribution. All statistical analyses were performed using SAS, version 9.1 (SAS Institute).
RESULTS
Clinical Characteristics
Table 1 shows the clinical characteristics of NOPR participants stratified by time interval, testing indication, and patient age in aggregate for all cancer types. Patients under 65 y old (disabled) comprised about 10% of participants, with a slight increase in NOPR 2009. The average age of the Medicare elderly participants was 75.0 y, stable from year to year, and similar for restaging and chemotherapy monitoring. PET studies were performed with PET/CT scanners in 90% and 97% of NOPR 2006 and NOPR 2009 cases, respectively.
Clinical Characteristics of NOPR Cohorts
Patients whose clinical indication for testing was chemotherapy monitoring differed from other patients. In the chemotherapy monitoring cohort, 17% of patients had Eastern Cooperative Oncology Group performance status scores of 2, 3, or 4. When the indication for testing was restaging, performance status scores of 2–4 were reported only 12% of the time. Performance status scores did not differ by age (greater or less than 65).
Patients tested for restaging versus chemotherapy monitoring also differed in the referring physician summary stage. For the restaging indication, 45%–50% of patients were judged to have either no or a low probability of recurrence. In the chemotherapy cohort, only about 14% were judged to have no or a low probability of recurrence. The frequency of metastatic disease was 35%–40% in the restaging cohorts versus 63%–66% of those having chemotherapy monitoring. There were minimal differences in the distribution within a testing indication by age or time period.
In 2009, NOPR added questions on the duration of chemotherapy given before the PET study. About 6% of patients underwent PET after less than 1 mo of therapy, 32% after 1–3 mo, and 28% after 3–6 mo; about one third had already received more than 6 mo of treatment when the PET was performed.
After the PET study, referring physicians were asked 2 related, but slightly different, questions regarding disease burden or prognosis. Specifically, after PET for restaging, physicians were asked to record their impression of the extent of disease (less extensive, unchanged, or more extensive than estimated before PET). After PET for chemotherapy monitoring, physicians were asked to record the change in prognosis (better, unchanged, or worse) in light of the PET findings.
Physicians changed their estimates of disease extent about two thirds of the time after PET for restaging. Disease extent was judged to be less than anticipated in 35%–37%, unchanged in 33%–35%, and more extensive in 30%. These results were similar in the NOPR 2006 and 2009 cohorts.
The physician's prognosis after PET for chemotherapy monitoring also changed about 70% of the time and was not meaningfully different between the 2006 and 2009 cohorts. A better prognosis than anticipated occurred in about 40%, no change in 31%, and a worse prognosis in 29%. Intracategory differences between the time periods were less than 2%.
Restaging or Suspected Recurrences
Table 2 shows the impact of PET on intended management for restaging for all cancer types stratified by time interval and age. The overall frequency of management change was calculated as the sum of a change from a nontreatment plan (predominantly other imaging, if PET were not available) to treatment and from treatment to nontreatment (predominantly to watching or supportive care).
Impact of PET on Intended Management for Restaging
The dominant impact was a change from nontreatment to treatment. In the 2009 cohort about 2% more scans led to a change in intended management from nontreatment to treatment than in the 2006 cohort (30% vs. 28%). The reverse pattern, changing from treatment to nontreatment, declined by 2% (from ∼8% to ∼6%) from 2006 to 2009. The overall impact of 35% was essentially unchanged in 2006 and 2009 (χ2 = 0.23, P = 0.62). In each period, the impact was about 2% less in those less than 65 y old versus more than 65 y old.
Table 3 shows the changes in intended management associated with PET when used in restaging stratified by cancer type and testing interval in patients over age 65 y. An overall pattern of a 4- to 5-fold larger change from nontreatment to treatment than the converse was seen. For all cancer types except prostate cancer, there was no difference between time cohorts in the impact of PET on intended management.
Impact of PET on Intended Management for Restaging in Patients Older Than 65 Years
The imaging-adjusted impact, the more conservative estimate of the change in intended management, is shown in Tables 2 and 3. The overall imaging-adjusted impact was slightly higher in NOPR 2006 than in NOPR 2009 (15.1% vs. 12.5%) and was similar in both age groups within a time period. Table 3 shows for patients over 65 y old that the imaging-adjusted impact stratified by cancer type and time interval showed the same temporal trends.
Chemotherapy Monitoring
Table 4 shows the impact of PET on intended management during chemotherapy monitoring stratified by time interval and cancer types. There is a distinct change in intended management by time interval but nonmeaningful differences within time intervals. For all cancer types combined and for each individually, continuing the current chemotherapy (type, dose, and schedule) was more frequent in NOPR 2009 than in NOPR 2006 (46.9% in 2009 vs. 34.7% in 2006 [χ2 = 253, P < 0.0001]). The increased frequency of continuing the current chemotherapy was greater in patients with bladder, prostate, and small cell lung cancer (∼17%).
Impact of PET on Intended Management During Chemotherapy Monitoring
The frequency of switching to another type of chemotherapy clustered at around 25% of cases and minimally differed by cancer type or time period. Stopping chemotherapy treatment and switching to watching or supportive care declined slightly in all cancer types except for pancreas in NOPR 2009. Stopping therapy was most common in bladder and small cell lung cancer at about 20%. The increase in plans to continue the current chemotherapy in 2009 was almost balanced by the concurrent decrease in plans to adjust the dose or schedule of the current chemotherapy (14.6% vs. 6.3%, NOPR 2006 vs. 2009).
Prognostic Estimate and Change in Chemotherapy Monitoring Plan
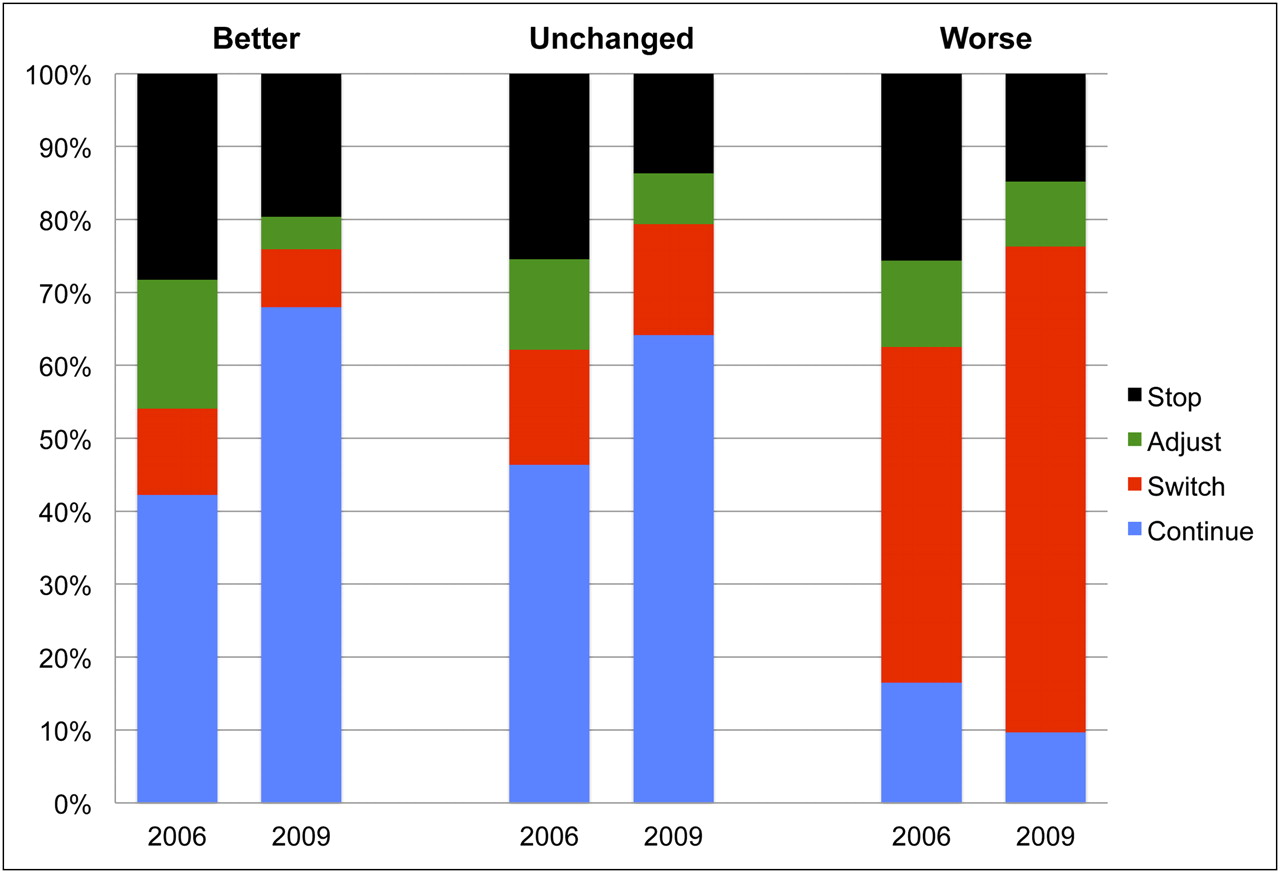
Figure 1 shows the intended chemotherapy plans after PET in relationship to the change in prognosis (better, no change, or worse) indicated by the PET findings and the time interval.
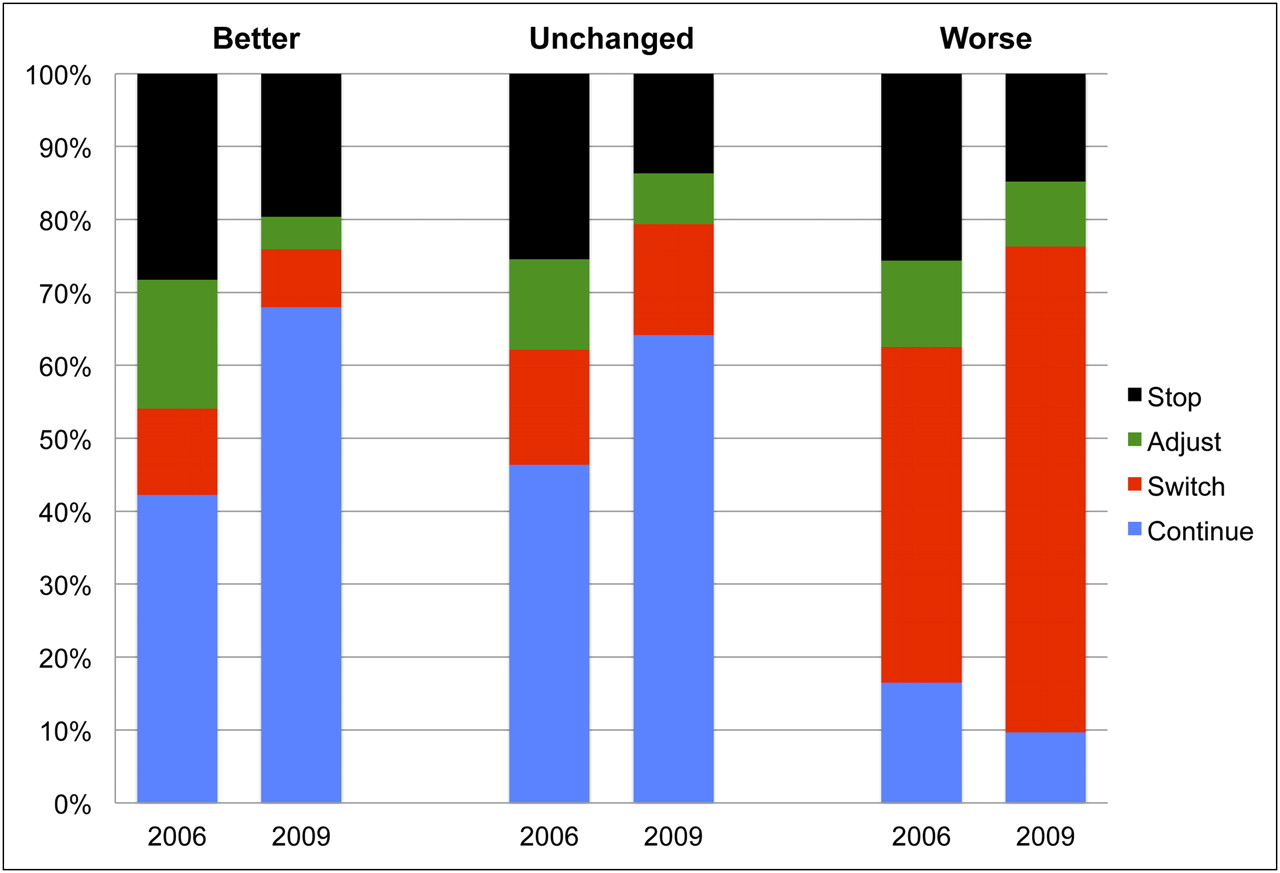
Impact on management after PET for chemotherapy monitoring stratified by post-PET prognosis. Data are shown for patients undergoing PET for chemotherapy monitoring in NOPR 2006 (n = 10,234) or NOPR 2009 (n = 15,609) for any cancer type. Intended plans for other imaging or biopsy, which accounted for about 5% of cases, were excluded for clarity.
If the post-PET prognostic impression was better or unchanged, continuing the same chemotherapy dose and schedule was the dominant plan. The frequency of continuing the current therapy was greater in NOPR 2009 than in NOPR 2006 (66% vs. 44%). However, if the prognosis was judged to be worse, about two thirds of patients would be switched to another therapy in both the 2006 and the 2009 cohorts.
DISCUSSION
We have studied the CMS CED program for PET by comparing the NOPR 2006 and NOPR 2009 cohorts. In 2009, CMS provided coverage for nearly all primary cancers when PET was used in initial treatment management. Thus, in comparison to NOPR 2006, the ongoing NOPR 2009 program tracks a smaller group of cancers and primarily when PET is used for management other than the initial treatment strategy (i.e., for restaging and detection of suspected recurrence or for chemotherapy monitoring). We report data separately for the 7 most common cancer types in NOPR 2009, as well as for a remaining category encompassing “other solid tumors.” We have stratified the tumor-specific data based on the clinical indication for PET (restaging, detection of suspected recurrence, or chemotherapy monitoring) and the time period (before or after April 2009).
We found that when used for subsequent treatment planning, a NOPR PET scan was associated with about a 35% change in intended management. The observed intended management change was minimally different between cancer types, time periods (before or after 2009), and age (when comparing younger, disabled Medicare beneficiaries with the traditional Medicare population aged 65 y and over).
The imaging-adjusted impact of PET, calculated by assuming that a pre-PET plan of another type of imaging would have led to the same postimaging management plan as PET, showed a slight decline with time but was greater than 10% in all cancer types. As we have noted previously (8), the imaging-adjusted impact is a lower bound on the change in intended management, since a substantial body of literature shows that PET is more accurate—both more sensitive and more specific—than conventional cross-sectional imaging (11). The decline in imaging-adjusted impact from NOPR 2006 to NOPR 2009 is likely explained by referring physician's gradually shifting their use of PET from a test done after body CT or MRI to one done in lieu of these other imaging methods. Therefore, some patients found to have extensive disease on CT previously would have undergone only CT, but such patients are now included in the PET group.
The role of PET in chemotherapy monitoring as a tool to measure therapy response as a guide to treatment adaptation is still evolving (12–14). Promising results have been reported in lymphoma, especially Hodgkin lymphoma (15). However, for solid tumors, there is little published information yet available about the impact of PET used for treatment adjustment during a planned course of therapy, nor is there consensus about when during a planned course of therapy PET should be done or standardization of the quantitative parameters (usually peak standardized uptake values) that should be assessed. Nonetheless, about 22% of NOPR 2009 scans were undertaken for chemotherapy treatment monitoring purposes.
To better assess this use of PET, in 2009 NOPR began collecting data on the duration of the current treatment at the time of a scan ordered for treatment monitoring. However, there are several limitations to the data. Although the concept of treatment monitoring is often assumed to require a baseline image for comparison, NOPR did not require that a preceding PET scan be available and we did not assess the rate or timing of prior scans in this study. About one third of patients had already received 6 mo or more of therapy. Therefore, it is uncertain whether these late scans could be alternatively classified as restaging rather than treatment monitoring. For this analysis, we used the classification reported by the referring physician.
We found that the principal impact of PET on management during chemotherapy occurred in patients whose PET scans showed more extensive disease or a worse prognosis than was anticipated. In these patients, the impact of imaging results was large and was consistent across cancer types and time intervals. Referring physician responses indicate that they planned to continue chemotherapy unchanged in only 10% of patients when PET indicated a worse prognosis than anticipated.
If referring physicians judged the post-PET prognosis to be better or unchanged, they intended to continue the current therapy more often in the NOPR 2009 cohort than in the NOPR 2006 cohort. We speculate that this decision was due to the use of PET earlier, on average, in the course of a planned treatment or to increased confidence in using PET to guide decision making.
CONCLUSION
Our analysis shows wide-ranging similarities across a broad spectrum of tumor types that are still being included in the Medicare CED process under NOPR 2009. The similarities across cancer subtypes were also robust to the study period (2006, 2009) and the indication for which a PET scan was ordered. To date, over 70,000 PET studies have been accrued for these cancers under NOPR 2009. There is little indication, either from the time series trend or from the type-specific data, that simply expanding the volume of scan data from further patients will provide much additional clinically meaningful insight into the impact of PET on intended management of these patients. A second key finding occurs when the present data are compared with our multiple prior publications on the NOPR 2006 cohort, where PET under CED was discontinued for many cancer types and indications in April 2009. There are few if any impactful differences between those types of patients (and cancers) now covered without CED and those remaining under the CED registry protocol.
Although PET has a primary and fundamentally accepted role in oncology today, there remain open questions as to how PET should be most effectively sequenced with other imaging resources in patient care pathways and what protocols will be most accurate and efficient when PET is used for chemotherapy monitoring. A paradigm different from that of the NOPR program will be necessary to better define plans that assess and compare care pathways that implement the available advanced imaging modalities for major decision points in cancer care. NOPR has been successful, however, in providing clear data on the previously little-researched question of whether the impact of PET on different cancers would be similar in actual clinical practice in the Medicare population. Even with less common cancers, the impact of PET on physician decision making for patient management seems remarkably uniform.
DISCLOSURE STATEMENT
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734.
Acknowledgments
Funding for development of the NOPR was provided by the Academy for Molecular Imaging, but the registry is otherwise self-supported by the fees paid by participating PET facilities. No other potential conflict of interest relevant to this article was reported.
Footnotes
Published online Mar. 23, 2012.
- © 2012 by the Society of Nuclear Medicine, Inc.
REFERENCES
- Received for publication January 31, 2012.
- Accepted for publication February 23, 2012.





{kind=link}
Jump to section
Related Articles
Cited By...
- The Future of Nuclear Medicine as an Independent Specialty
- Proceedings: Pathways for Successful Translation of New Imaging Agents and Modalities--Phase III Studies
- Impact on Patient Management of [18F]-Fluorodeoxyglucose-Positron Emission Tomography (PET) Used for Cancer Diagnosis: Analysis of Data From the National Oncologic PET Registry
- 18F-Fluoride PET Used for Treatment Monitoring of Systemic Cancer Therapy: Results from the National Oncologic PET Registry
- Follow-up or Surveillance 18F-FDG PET/CT and Survival Outcome in Lung Cancer Patients
- Impact of 18F-Fluoride PET on Intended Management of Patients with Cancers Other Than Prostate Cancer: Results from the National Oncologic PET Registry
- Impact of 18F-Fluoride PET in Patients with Known Prostate Cancer: Initial Results from the National Oncologic PET Registry
- Intended Versus Inferred Care After PET Performed for Initial Staging in the National Oncologic PET Registry
- A Broader Importance of NOPR to the Future of Nuclear Imaging