


Abstract
The National Oncologic PET Registry (NOPR) collected data on intended management before and after PET in cancer patients. We have previously reported that PET was associated with a change in intended management of about one third of patients and was consistent across cancer types. It is uncertain if intended management plans reflect the actual care these patients received. One approach to assess actual care received is using administrative claims to categorize the type and timing of clinical services. Methods: NOPR data from 2006 to 2008 were linked to Medicare claims for consenting patients aged 65 y or older undergoing initial-staging PET scanning for bladder, ovarian, pancreatic, small cell lung, or stomach cancers. We determined the 60-d agreement between claims-inferred care and NOPR treatment plans. Results: Patients (n = 4,661) were assessed, and 30%–52% had metastatic disease. Planned treatments were about two-thirds monotherapy, of which 46% was systemic therapy only, and one-third combinations. Claims paid by 60 d confirmed the NOPR plan of any systemic therapy, radiotherapy, or surgery in 79.3%, 64.7%, and 63.6%, respectively. Single-mode plans were much more often confirmed: systemic therapy in more than 85% of patients with ovarian, pancreatic, and small cell lung cancers and surgery in more than 73% of those with bladder, pancreatic, and stomach cancers. Intended combination treatments had claims for both in only 28% of patients receiving surgery-based combinations and in 55% receiving chemoradiotherapy. About 90% of patients with NOPR-planned systemic therapy had evaluation or management claims from a medical oncologist. An age of less than 75 y was associated more often with confirmation of chemotherapy, less often for radiotherapy but not with confirmation of surgery. Performance status or comorbidity did not explain confirmation rates within action categories, but confirmation rates were higher if the referrer specialized in the planned treatment. Conclusion: Claims confirmations of NOPR intent for initial staging were widely variable but were higher than previously reported for restaging PET, suggesting that measuring change in intended management is a reasonable method for assessing the impact diagnostic tests have on actual care.
- positron emission tomography
- cohort studies
- Medicare
- medical record linkage
- health services research
- neoplasm staging
Optimal care for a patient with a newly diagnosed solid tumor has evolved into a complex, intertwined series of steps often involving multispecialty teams. Advanced medical imaging has an important role in establishing the initial stage and usually precedes definitive treatment (1).
Since 2001, PET, alone or integrated with CT (hereinafter together referred to as PET), using 18F-FDG has been a service covered by Medicare (and most commercial insurers) for the initial staging of patients with non–small cell lung, colorectal, esophageal, and head and neck cancers, as well as lymphoma and melanoma, and its use has grown rapidly (2,3). However, at that time, PET remained a noncovered service for most less-common cancer types.
In 2005, Centers for Medicare and Medicaid Services (CMS) announced a novel coverage mechanism, “coverage with evidence development (CED),” for the otherwise noncovered cancer types and indications in conjunction with prospective data collection within a registry (4). In response to the CED requirements, the National Oncologic PET Registry (NOPR) was created and opened for accrual in 2006 (5). We have previously reported results of the impact of PET on intended management by collecting prospective questionnaire data before and after PET stratified by testing indication and by cancer type (6,7).
Limitations of the NOPR data include the following: change in planned management is only a surrogate for actual health outcomes and the care actually delivered is not documented (8,9). Although there are numerous studies of adherence to oral cancer therapies, there are few series that address the concordance between recommended actions and actual care initiated (10,11). If the concept of “change in intended management” should be carried forward and applied to future assessments of new imaging techniques, this decision is likely to be influenced by evidence of confirmation of actual actions or outcomes.
One common approach is to use and analyze administrative claims to document the patterns of use and timing of various clinical services. Oncology has been the subject of wide-ranging evaluations using SEER (Surveillance, Epidemiology, and End Results) cancer registry data and Medicare claims (12).
In this report, we linked NOPR participant’s individual identifiers with their Medicare claims. The analytic approach to this linked dataset was stratified by the clinical indication for PET: initial staging, restaging, or treatment monitoring. Here we report on intended plan initiation after PET used for staging of newly diagnosed cancer. We have previously reported results for restaging that found moderate agreement between intended and claims-inferred care (13). We hypothesized that confirmation rates would be higher than for restaging because prior treatments would not be a factor. In addition, we assessed patterns of delayed treatment and secondary decision points for combination therapies.
MATERIALS AND METHODS
NOPR is a prospective data registry (ClinicalTrials.gov #NCT00868582); its operational details, human subject protection procedures, and PET’s impact on intended management were previously reported (6,14). In brief, the PET facility collects referring physician responses on pre-PET and post-PET forms. The pre-PET form collects the testing indication, cancer type, working stage, performance status, and the referring physician’s plans if PET were not available. After PET, the referrer records an estimate of the patient’s tumor stage and management plan in light of the PET findings.
Claims Linkage
We linked NOPR data from December 2006 through 2008 for consenting participants to their Medicare claim files by matching individual identifiers (date of birth, social security number, and sex). We limited our analysis to the 7 most frequent cancer types within NOPR. As previously noted, PET was a covered service for more common cancer types, such as non–small cell lung and colorectal cancers. We stratified our analyses by testing indication (initial staging, treatment monitoring, or restaging). In addressing initial staging, we excluded kidney and prostate cancer patients because of our prior work showing poor detection of oral chemotherapy claims for kidney cancer and explicit noncoverage of initial staging PET for prostate cancer in CMS’s 2009 National Coverage Decision (15).
The analysis dataset of 4,661 was determined after the following exclusions: patients who were aged less than 65 y (9.0%); who were health maintenance organization participants (8.0%); or for whom we were unsuccessful in linking identifiers (1.5%), if the registry and claim dates for PET differed by more than 7 d (2.0%), or if the post-PET plan was “other treatment(s)” or “additional imaging” because of their low frequencies (1.5% and 3.0%, respectively).
Management Categories
Post-PET categories assessed were watching, biopsy, and treatment. Treatment categories were systemic therapy (chemotherapy or immunotherapy), radiotherapy, or surgery alone or in combination. For combination therapies, NOPR did not record their sequence or concurrence.
Claims Definitions and Time Frame
Supplemental Table 1 (supplemental materials are available at http://jnm.snmjournals.org) documents how we used administrative coding data to classify claims into inferred-care categories. The referring physician’s impression of the patient’s summary stage was abstracted from the post-PET form. We determined the Klabunde comorbidity index—derived from inpatient and outpatient physician claims in the 12 mo preceding the PET date (which approximates the date of diagnosis)—using a publically available SAS algorithm (16). The CMS provider part B taxonomy codes for physician specialty were used to categorize referring providers. If no specialty or nonphysician coding was found, then specialty was coded as other.
Although prompt treatment for newly diagnosed cancer is optimal, defining acceptable time windows either from initial diagnosis to primary surgical therapy or from surgical therapy to beginning adjuvant therapy is more problematic (17–19). The median time from diagnosis to surgery or starting neoadjuvant therapy in gastric and pancreatic cancer in 2003–2006 was between 20 and 25 d (18). In a SEER–Medicare analysis from 1999, 81% of patients started adjuvant therapy within 60 d of their surgery (19). A recent report from the National Comprehensive Cancer Network found an average time of 12 wk from diagnosis to start of adjuvant chemotherapy in early stage breast cancer (17). Because we did not have the NOPR participant’s date of cancer diagnosis, we used our best estimate of 60 d after PET for the claims-inferred action window. We also explored an extension of the time window to 180 d.
Statistical Analysis
The initial analyses treated the claims-inferred care as the reference standard to calculate measures of agreement between treatment plans and claims-inferred actual management, including positive predictive value (PPV), raw agreement, and κ (chance-adjusted agreement) (20). For the treatments (systemic therapy, radiotherapy, or surgery), agreement was defined as claims for that type action within the interval, without considering other treatments; for plans with 2 or rarely 3 different therapy modes, we defined agreement as at least 1 claim paid for 2 types. The measures of agreement were computed separately by cancer type and compared using χ2 tests.
To assess the effect of patient, cancer, and provider factors in predicting agreement, separate logistic regression models were fit for patients with plans for any systemic therapy, radiotherapy, or surgery only. The outcome was the indicator of agreement with that element of the plan. Calculations were done with PROC LOGISTIC in Linux SAS version 9.2 (http://support.sas.com/documentation/cdl/en/statug/63033/HTML/default/viewer.htm#statug_logistic_sect004.htm). This analysis plan was similar to that used in our preceding work done assessing NOPR PET for restaging (13).
RESULTS
Clinical Characteristics
Table 1 summarizes the cancer type, age, performance status, comorbidity scores, referring physician specialty, and pre-PET plan for our 4,661-patient cohort.
NOPR Cohort Clinical Characteristics for PET Imaging Performed for Initial Staging
The summary stage distribution varied across cancer types and sometimes differed from national SEER averages, suggesting that the NOPR patients were selectively referred for PET (21). When patients judged to have no evidence of residual disease (e.g., if PET was performed after a primary resection) are combined with those judged to have only local disease, NOPR patients with ovarian, pancreatic, and stomach cancers had modestly higher rates (35%–45%) of local disease than their SEER cancer-specific averages. Metastatic disease at initial staging was judged present much more commonly for bladder cancer (35%) than in SEER. Sixty-day mortality overall was 10% ranging from 5% in ovarian to 13% in small cell lung (SCL) and pancreatic cancers.
Referring physicians were identified as medical oncologists in slightly more than half of patients; were more than 10% surgeons in pancreatic and stomach cancer patients; and were more than 10% radiation oncologists in bladder, pancreatic, and SCL cases.
NOPR Plan
After PET, staging appeared to be clinically complete in 90% (i.e., only 10% had plans for imaging or biopsy). Excluding that 10% of patients, the intended plan was new or additional treatment in 82.9% of patients (range, 79%–91%) and watching in 9.8% (Table 2). Modest frequency variations by cancer type were noted in the planned treatment (of any type), watching, or biopsy.
NOPR-Intended Management Plan After PET for Initial Staging by Cancer Type
Planned treatments were single modality in about two thirds of patients and combination therapies in one third. The most common treatment plan was systemic therapy alone (45.7%; range, 35%–69%). Almost all combination-therapy patients had plans including systemic therapy, so that 78.4% (range, 69%–92%) had systemic-therapy plans in their intended care. Radiotherapy was planned for one third of patients, usually in combination with chemotherapy or surgery. Surgery plans were equally split between surgery only or surgery plus chemotherapy or radiotherapy. Surgery was planned most frequently in stomach cancer (48%) as opposed to 20% of bladder, ovarian, and pancreatic cancer patients.
60-Day Agreement
Table 3 shows the agreement measures by cancer type for NOPR-intended treatments—any systemic therapy, radiotherapy, or surgery—and claims-inferred actions at 60 d.
Agreement Measurements by Type of Intended Therapy at 60 Days After PET
For any systemic therapy, the combined PPV was 79.3% ranging by type from more than 86% in ovarian and SCL, and more than 79% in bladder, to only 68% in stomach cancer. For plans of any radiotherapy, the combined PPV was 64.7%, with only modest differences between cancer types. Plans for any surgery had a PPV of 71.4% in stomach cancer and ranged between 50% and 60% in the other cancer types.
In aggregate, raw agreement between NOPR plans and claims at 60 d was 74.1% for any systemic therapy, 80.8% for any radiotherapy, and 77.9% for any surgery. Kappas were 0.40 for systemic therapy, 0.53 for radiotherapy, and 0.43 for surgery.
In addition to imperfect PPVs, raw agreement was affected by claims, likely capturing a second decision point. For example, in patients with intended surgery-only plans, there were claims for both surgery and systemic therapy in 19% of bladder, 30% of stomach, and 38% of pancreatic cancer patients, likely reflecting appropriate care after surgical staging. Conversely, many systemic therapy–only plans likely also represented neoadjuvant intent with a deferred surgery decision. In pancreatic cancer, 20% (n = 105) of patients with chemotherapy-only plans had surgery and chemotherapy claims at 60 d.
Single vs. Combination Therapy and Time Window
Table 4 shows results of extending the time frame to 180 d for claims confirmation of mono- and combination therapies. The PPVs for chemotherapy only in pancreatic, ovarian, and SLC patients were noticeably high (85%–91%) at 60 d, and extending the time window to 180 d increased PPVs by 1%–3%. Radiotherapy was most frequently planned together with chemotherapy. In these cases, claims for both treatment types at 60 d were only 47%–62%; however, extending the time window to 180 d increased the confirmation index by 7%–16%. Cases having surgery-only plans had surgical claims at 60 d in 80% of stomach and 74% of bladder or pancreatic cancers. By 180 d, surgery claims increased an additional 16% in bladder and 6% in pancreatic or stomach cancer patients.
Impact of Time Interval After PET on Claims Confirmation (PPV) of Post-PET Plan
The lowest rates and widest variation with time were found in confirming claims with surgery plus other treatments. By 60 d, claims for surgery plus chemotherapy or radiotherapy ranged from 23% to 36% in bladder, stomach, and pancreatic cancers. However, by 180 d, combined claims increased to 51%–61%.
Although extending action windows to 180 d tended to increase agreement with explicitly planned actions, it had the opposite effects for unplanned actions: by 180 d, more actions occur that were absent in the NOPR plan. For instance, the status of no chemotherapy by plan matched to claims 71.6% over 30 d, but this dropped to 42.5% over 180 d. Correspondingly, the κ statistic declined from 0.42 to 0.29, from a fair to a poor level of agreement.
Specialist Claims
Using the provider specialty codes, we explored whether patients had evaluation and management (E&M) claims from the specialist associated with the intended treatment, even if therapy claims were not found. This was true for medical oncology and chemotherapy.
Figure 1 shows that within 30 d most patients with chemotherapy planned had E&M medical oncologist claims—even in the absence of paid chemotherapy claims. Overall, E&M oncologist claims were found in 87% at 30 d, rising to 92% at 60 d. Almost all SCL patients having medical oncologist E&M claims also had chemotherapy claims. In contrast, 24% of stomach cancer patients with chemotherapy plans had medical oncologist visits but no detected chemotherapy claims by 60 d.
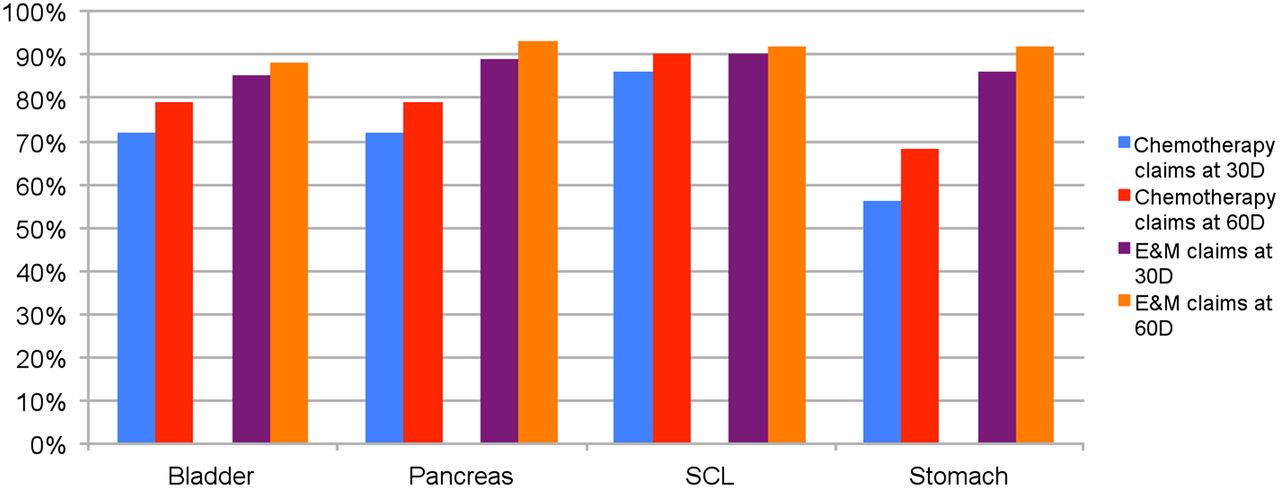
Frequency of chemotherapy claims and E&M claims by cancer type among subjects for whom NOPR intended-management plan was chemotherapy. We excluded ovarian cancer because gynecologic oncologists in addition to medical oncologists often give systemic therapies.
Predictors
The results when we assessed the impact of patient (age, performance status, comorbidity), cancer (type, summary stage), and referring provider (specialty, pre-PET plan) factors in a logistic regression model in predicting agreement by treatment type at 60 d are summarized in Table 5 (full details are provided in Supplemental Table 2).
Factors Associated with Agreement of Treatment Plan and Claims for Treatment
Patients aged 75 y or less were associated with higher claims agreement for chemotherapy, slightly lower agreement for radiotherapy, and not associated for surgery.
The impact of stage varied by treatment type. Patients having local disease with plans for surgery had claims confirmation in 73% versus 53% in nodal/regional disease. Radiotherapy agreement rates were similar for local and nodal/regional disease at 72% and were markedly less commonly planned or confirmed for metastatic disease. Claims confirming chemotherapy plans did not differ among patients with nodal/regional, single-site, or multisite metastasis at about 82%–84% but were lower with local disease (76%).
If the referring physician was the specialist providing the treatment type, there was much higher concordance for surgery or radiotherapy plans but minimal differences for medical oncologists and chemotherapy.
DISCUSSION
The NOPR management plan reflects the physician’s intentions shortly after receiving the PET report and not necessarily the patient’s agreement to the plan. Agreement between claims-inferred management (assuming these are complete and accurate) and the NOPR plan may be affected by patient treatment preferences revealed in subsequent consultations or the physician’s level of commitment to his or her plan. Unexpected shifts in a patient’s symptoms and clinical course could also impact the intended plans’ feasibility. This analysis of 5 cancer types when PET was used as part of initial staging found claims-validated monotherapy plans in over three fourths of patients within 60 d. However, for combination therapy, a 60-d window was too short to fully capture clinical actions inferred from claims analysis. One relevant NOPR data limitation was that the post-PET questionnaire did not document whether combination therapy plans were to be concurrent or sequential. Therefore, for sequential plans, it is likely that the decision to give the anticipated second therapy encompassed a further decision point dependent on reassessment. For combined chemoradiotherapy plans, claims for both therapies increased by over 10% using a 180- vs. 60-d window. A second decision point was even more likely with surgery-based combination therapies where the chemotherapy sequencing was not specified (neoadjuvant vs. adjuvant).
Although this study uses as its starting point the unverified NOPR plan data and claims-inferred actions as the actual care, it is notable that there is no gold standard for the study design under which maximum concordance between plan and execution occurs and how high that concordance is. A more ideal design might involve a structured interview with each physician after PET once a care plan is established with the patient, documenting nuances of the plan, and a manual chart or electronic record review. Additionally, one might also collect information on patient perspective—after initial post-PET clinical consultation.
Outside oncology, there are many examples in surgical randomized trials showing that actual delivery rates of randomly assigned therapy are often substantially different from intention to treat. For example, 2 y after treatment assignment for lumbar spinal stenosis, 43% had surgery after being assigned nonsurgical treatment and only 67% completed assigned surgery (22). In coronary artery disease trials, crossover from medical therapy to surgical intervention occurs in 10%–20% of patients and surgical refusal in 2%–10% (23,24). Crossover in abdominal aortic aneurysm trials are even higher (25). Thus, even if our plan and execution data points were obtained by more resource-intensive methodologies, it is unlikely that high (e.g., >90%) agreement would occur.
There is a substantial, growing literature addressing the desire of cancer patients for information and participation in decision making in their care (26,27). These studies have predominantly addressed preference-based primary therapy decisions in breast and prostate cancer. In general, older patients and those with metastatic cancers deferred more to physician recommendations (26,28). To the best of our knowledge, few studies address discrepancies between physician plan, patient preference, and actual therapy received, factors that may explain some observed differences in intended versus claims-inferred management. One notable report is CanCORS, which assessed over 5,000 newly diagnosed lung or colorectal cancer patients, one fifth presenting with metastatic disease; 24% of CanCORS patients did not receive the treatment discussed (26,28).
Agreement studies within cancer registries focus on registry classification accuracy either when an independent record reabstraction (29) is made or when registry treatments are compared with claims-inferred care. Since 2000, numerous SEER–Medicare linkage reports have assessed claims completeness in identifying chemotherapy type (30–32), surgery (33), and radiation (34). Most studies did not focus on the claims’ temporal accuracy. Since 2004, SEER guidelines require that all information be gathered through completion of first-course surgery or be available within 4 mo of diagnosis in the absence of disease progression (29). Our analysis shows that a 60-d window is likely too narrow for assessing planned treatment completion, particularly in patients with less-aggressive, local disease and for combination therapies. However, lengthening this window may also result in false-positives if claims are made for reasons not closely associated with the original post-PET plan (e.g., unplanned treatment at 3–6 mo for unexpectedly aggressive metastatic disease).
Two recent reports provide some context for our findings. In a comparison of Medicare administrative claims against clinical trial data (as a reference standard), Lamont et al. assessed patient cohorts from 6 CALGB first-line chemotherapy trials in breast, colorectal, and lung cancer (30). They found that 78% of claims correctly identified the drugs given and the correct treatment schedule. In a second study, Lund et al. reported National Cancer Institute Patterns of Care studies in 4 cancer types where SEER initial treatment plans were directly validated against hospital and outpatient records that were reabstracted for chemotherapy (35). They found that the claim sensitivities were time dependent, ranging from 36%–50% at 2 mo to 84%–96% at 6 mo.
Our analysis was not powered to, and did not attempt to, stratify patients by stage within each cancer type, and we did not assess whether either the planned or the claims-inferred management in each patient agreed with authoritative clinical practice guidelines. Our findings that about 90% of patients with an intended plan including chemotherapy had E&M (office visit) claims from a medical oncologist within 60 d even in the absence of chemotherapy claims suggest appropriate consultation for informed decision making was available—that is, patients who did not receive chemotherapy did not fail to see an oncologist.
The above concerns should not divert attention from the primary clinical endpoint and findings that NOPR was designed to measure—does PET as part of initial cancer staging lead to a change in (intended) clinical management? We have previously reported that during the first 2 y of NOPR data collection, PET was associated with a 40% change in intended management if additional imaging was a post-PET option or a 13% change if no benefit was assumed in cases where additional imaging was chosen. Using a design similar to that of the NOPR, Scott et al. from Australia have reported series involving smaller patient numbers (range, 71–129) and centers (n = 3–6) but with detailed medical record follow-up to assess intended versus actual management (36–38). They found that PET (without CT) used for initial staging of head and neck and esophageal cancer and lymphoma was associated with a 34%–38% change in intended management and that the agreement at 3–6 mo between the post-PET plan and actual care ranged from 53% in esophageal cancer to 74% in lymphoma and head and neck cancer. Our results from a national registry with little control over center-to-center data quality are quite similar.
We have previously noted that PET-associated changes in intended management would not always be beneficial (because PET has both false-negative and false-positive results) (14). Moreover, changes in intended actions have a presumed, but uncertain, relationship to more tangible health outcomes, such as progression-free or overall survival (39). However, given the above limitations, we were gratified to observe that claims at 60 d confirmed chemotherapy plans in 90% of SCL cancer patients and surgery in 80% with stomach cancer, assuming that in most cases PET results were accurate and accepted contemporary treatment is beneficial.
CONCLUSION
If future evaluations of new imaging techniques are initiated under the CMS CED policy, there are lessons to be learned from the NOPR experience. For example, the type and extent of prior imaging or treatment are likely to impact the agreement rates between intended and actual care. Although refinements in granular detail of intended management plans (e.g., specific drugs, sequencing for combination therapies) warrant consideration, our results suggest that the principal future change should be at least 1 additional follow-up data collection point—to confirm the actual initiation or cessation of treatment or changes in the use of relevant diagnostic studies. Innovative study designs that allow for investigation of the patient’s role as a factor in planned versus received care at preference-sensitive decisions points should be piloted. We hypothesize that differences in treatment urgency and acceptability likely explain discordance more than inaccurate assessment of physicians' intended plans. The inability to make inferences about the impact of diagnostic imaging on patient outcomes outside a randomized trial will remain. A modest greater time investment and energy of all parties (patients, referring physicians, interpreting physicians, and registry analysts) and an expanded informed consent will be needed to strengthen the value of diagnostic registries for comparative effectiveness research.
DISCLOSURE
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734. This study was supported by the National Cancer Institute Grand Opportunity Award RC2CA148259. No other potential conflict of interest relevant to this article was reported.
Footnotes
Published online Nov. 12, 2013.
- © 2013 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication March 20, 2013.
- Accepted for publication May 30, 2013.





{kind=link}
Jump to section
Related Articles
Cited By...
- Intended Versus Inferred Treatment After 18F-Fluoride PET Performed for Evaluation of Osseous Metastatic Disease in the National Oncologic PET Registry
- Techniques, Benefits, and Challenges of PET-MR
- Impact of 18F-Fluoride PET on Intended Management of Patients with Cancers Other Than Prostate Cancer: Results from the National Oncologic PET Registry