


Abstract
Acute myeloid leukemia (AML) is a neoplasm of hematopoietic stem cells with partial or complete loss of the ability to differentiate but with preserved proliferation capacity. The aim of our study was to evaluate if the in vivo proliferation marker 3′-deoxy-3′-18F-fluorothymidine (FLT) is suitable for visualizing leukemia manifestation sites and if 18F-FLT is a surrogate marker for disease activity. Methods: In this pilot study, 10 patients with AML underwent pretherapeutic imaging with 18F-FLT PET or 18F-FLT PET/CT. The biodistribution of 18F-FLT was assessed 60 min after intravenous injection of the radiotracer. Standardized uptake values were calculated for reference segments of bone marrow, spleen, and normal organs. 18F-FLT PET in 10 patients with benign pulmonary nodules and the absence of malignant or inflammatory disease served as controls. Results: Retention of 18F-FLT was observed predominantly in bone marrow and spleen and was significantly higher in AML patients than in controls (mean 18F-FLT SUV in bone marrow, 11.5 and 6.6, P < 0.05; mean 18F-FLT SUV in spleen, 6.1 and 1.8, P < 0.05). Outside bone marrow, focal 18F-FLT uptake showed extramedullary manifestation sites of leukemia in 4 patients (meningeal disease, pericardial, abdominal, testicular, and lymph node), proven by other diagnostic procedures. Conclusion: This pilot study indicated that PET using 18F-FLT is able to visualize extramedullary manifestation sites of AML and reflects disease activity. Because 18F-FLT uptake in bone marrow is caused by a combination of both neoplastic and normal hematopoietic cells, the correlation of 18F-FLT uptake in bone marrow and leukemic blast infiltration did not reach statistical significance.
Acute myeloid leukemia (AML) is a clonal disease of hematopoietic progenitor cells that lose the ability to differentiate and to respond to normal regulators of cellular proliferation. Genetic factors are regarded as the most important factors for prediction of response to treatment and patient outcome (1). In the care of patients with AML—in contrast to malignant lymphoma (2)—imaging techniques based on morphologic (CT, MRI) or functional (PET, scintigraphy) alterations play only an ancillary role, for example, for management of infections or detection of uncommon manifestation sites. Extramedullary disease in lymph nodes, the central nervous system, or soft tissue seems to be of increasing significance in patients with relapse after allogeneic stem cell transplantation (3–7). To know about extramedullary manifestations is important for long-term disease control, because some of these sites may not be reached by standard chemotherapy. Standard diagnostic procedures such as lumbar puncture with cerebrospinal fluid cytology have proven to be of high specificity but lack sensitivity despite additional flow cytometry (8).
PET using the glucose analog 18F-FDG enables detection of various hematologic neoplasms due to altered glucose consumption and allows assessment of response early in the course of treatment (9,10). Increased 18F-FDG uptake in extramedullary leukemia has been demonstrated in case reports (11), but leukemic manifestations in areas of high glucose metabolism such as the meninges or the pericardium may not be detected by 18F-FDG PET.
PET using 11C- or 18F-labeled DNA precursors has a potential for specific imaging of proliferation in vivo. 11C-thymidine represents the native thymidine molecule and has been evaluated in preclinical and clinical studies (12,13). However, because of the rapid in vivo degradation and short half-life of 11C, this tracer was regarded as inappropriate for routine clinical use. In 1998, Shields et al. introduced 3′-deoxy-3′-18F-fluorothymidine (FLT) as a thymidine analog that is resistant to in vivo degradation and accumulates predominantly in proliferating tissues (14). Recently, we have shown that 18F-FLT is suitable for detection of malignant lymphoma and superior tumor grading (15). Because of physiologically increased uptake of 18F-FLT in the bone marrow, 18F-FLT PET has also been suggested for bone marrow imaging (16). More recently, our group has shown that radiolabeled thymidine analogs such as 5-123I-iodo-4′-thio-2′-deoxyuridine (123I-ITdU) can be used for induction of leukemia cell kill by mediating nanoirradiation to DNA (17).
Here, we assessed the biodistribution of 18F-FLT in patients with AML and the utility of 18F-FLT PET for visualizing extramedullary manifestation sites of AML and evaluating disease activity.
MATERIALS AND METHODS
Study Inclusion Criteria
This prospective study comprised 10 patients (4 men and 6 women) with a mean age of 47 y (range, 23–70 y; Table 1). Patients with high-risk AML scheduled for subsequent myeloablative treatment and bone marrow transplantation were eligible to participate in this study. One patient had newly diagnosed AML exhibiting unfavorable cytogenetics (patient 1; Table 1), 7 patients were recruited because of clinical evidence or morphologic proof of relapse, and 2 patients were recruited because of refractory disease. Ten healthy controls who were examined previously for further work-up of indeterminate pulmonary nodules served as a reference. Patients who had radio- or chemotherapy within 4 wk were excluded from this series. All patients gave written informed consent to participate in the study, which was approved by the local ethical committee. Bone marrow aspiration cytology was performed on all patients, followed by morphologic analysis, immunophenotyping, and cytogenetic studies. Two hematologists interpreted the results on the basis of the current World Health Organization classification (18).
Patient Characteristics
Synthesis of 18F-FLT
18F-FLT was produced using the method of Machulla et al., with minor modifications (19). 18F-fluoride was produced via the 18O(p,n)18F nuclear reaction by bombardment of isotopically enriched 18O-H2O with a 16.5-MeV proton beam at a PETtrace cyclotron (GE Healthcare). The detailed synthesis protocol was described elsewhere (20).
Data Acquisition, 18F-FLT PET, and 18F-FLT PET/CT
In 5 patients, PET was performed using a high-resolution full-ring scanner (ECAT HR+; Siemens/CTI), which produces 63 contiguous slices per bed position. The axial field of view is 15.5 cm per bed position. Five bed positions were measured in each patient, covering a total field of view of 77.5 cm. The emission scan was started 60 min after intravenous injection of approximately 370 MBq of 18F-FLT and included the base of the skull, neck, thorax, abdomen, pelvis, and proximal femora in all patients. In 3 patients, the entire skull was included in the emission scan. In patient 2, the extremities were additionally scanned. The acquisition time was 7 min per bed position. Three-minute transmission scans with a 68Ge/68Ga ring source were obtained for attenuation correction after tracer application. Images were reconstructed using an iterative reconstruction algorithm described by Schmidlin et al. (21). In the other 5 patients, integrated PET and helical CT using a PET/CT scanner (Discovery LS; GE Healthcare) was performed. The CT acquisition protocol included a low-dose CT scan (26 mAs, 120 kV, 0.5 s per rotation, 5-mm slice thickness) from the top of the skull to the mid thigh for attenuation correction, followed by the PET scan. All PET scans were acquired in 2-dimensional mode with an acquisition time of 3 min per bed position. Forty contiguous slices were acquired per bed position; the matrix size was 128 × 128, and slice thickness was 3.4 mm. Images were reconstructed by an attenuation-weighted ordered-subsets expectation maximization algorithm (4 iterations and 8 subsets) followed by a postreconstruction smoothing gaussian filter (5 mm in full width at half maximum). Emission data were corrected for randoms, dead time, scatter, and attenuation, and we used the same reconstruction algorithm as was applied for the conventional PET data. Patients serving as controls were imaged with 18F-FLT PET using the same protocol as was mentioned above without CT coregistration.
Image Interpretation and Quantification of 18F-FLT Uptake
All images were evaluated by 2 experienced nuclear medicine physicians. Focal 18F-FLT uptake in organs with usually mild homogeneous activity or in lymph nodes that usually present without tracer uptake were interpreted as potential manifestation sites of leukemia. Circular regions of interest were drawn containing the area with focally increased 18F-FLT uptake to calculate respective standardized uptake values (18F-FLT SUV). A single circular region was used for SUV calculation of disease manifestation sites. Mean and maximum SUVs were calculated for bone marrow (lumbar vertebra 4) and spleen, and mean values were calculated for reference segments of the lungs, liver, kidneys, intestines, bone (skull), and brain using the same approach as for leukemia manifestation sites.
Data Analysis
After completion of the study, the results of clinical tests indicating disease activity, morphometry, cytochemistry, cytogenetics, and 18F-FLT PET findings were correlated. GraphPad Prism software (version 4.03; GraphPad) was used for statistical analyses. Data are presented as mean, median, range, and SD. 18F-FLT uptake in bone marrow and spleen in leukemia patients and healthy controls was compared using the Wilcoxon signed rank test. Differences were considered statistically significant at a P level of less than 0.05. Linear regression analysis was performed to test for a potential correlation between the number of blasts identified at bone marrow puncture (BMP) and 18F-FLT uptake in bone marrow.
RESULTS
Patients
In 9 of 10 patients, reference methods indicated active disease. One patient with a history of acute myclomonocytic leukemia (patient 10) was included because of clinical suspicion of relapse; however, bone marrow biopsy revealed a second complete remission. The majority of patients were recruited because of relapse of AML (Table 1). Two patients had refractory disease with leukemic blast infiltration of 80% (patient 2) or 100% (patient 9). One patient was recruited with an initial diagnosis of AML and unfavorable cytogenetics (patient 1). Outside the study protocol, 1 patient underwent 18F-FLT PET 4 wk after subsequent myeloablative radiochemotherapy, bone marrow transplantation, and transplant failure (patient 11).
Imaging AML with 18F-FLT PET
In all patients with AML, bone marrow represented the organ with the highest uptake of the thymidine analog 18F-FLT (Figs. 1–3⇓⇓). Four patients presented with 18F-FLT uptake in the proximal femora and humeri not visible in controls, indicating bone marrow expansion (Fig. 2). Extensive bone marrow expansion was present in patient 2. A whole-body PET scan showed intense tracer uptake also in the bone marrow cavity of the distal femora, tibiae, and fibulae (Fig. 1). Of note, no tracer uptake in the skull or in the forearm skeleton was observed, indicating specific retention of 18F-FLT in bone marrow. Additionally, focal uptake in projection of the right testicle was observed. A testicular manifestation of leukemia was further confirmed cytologically in this patient (Fig. 1).
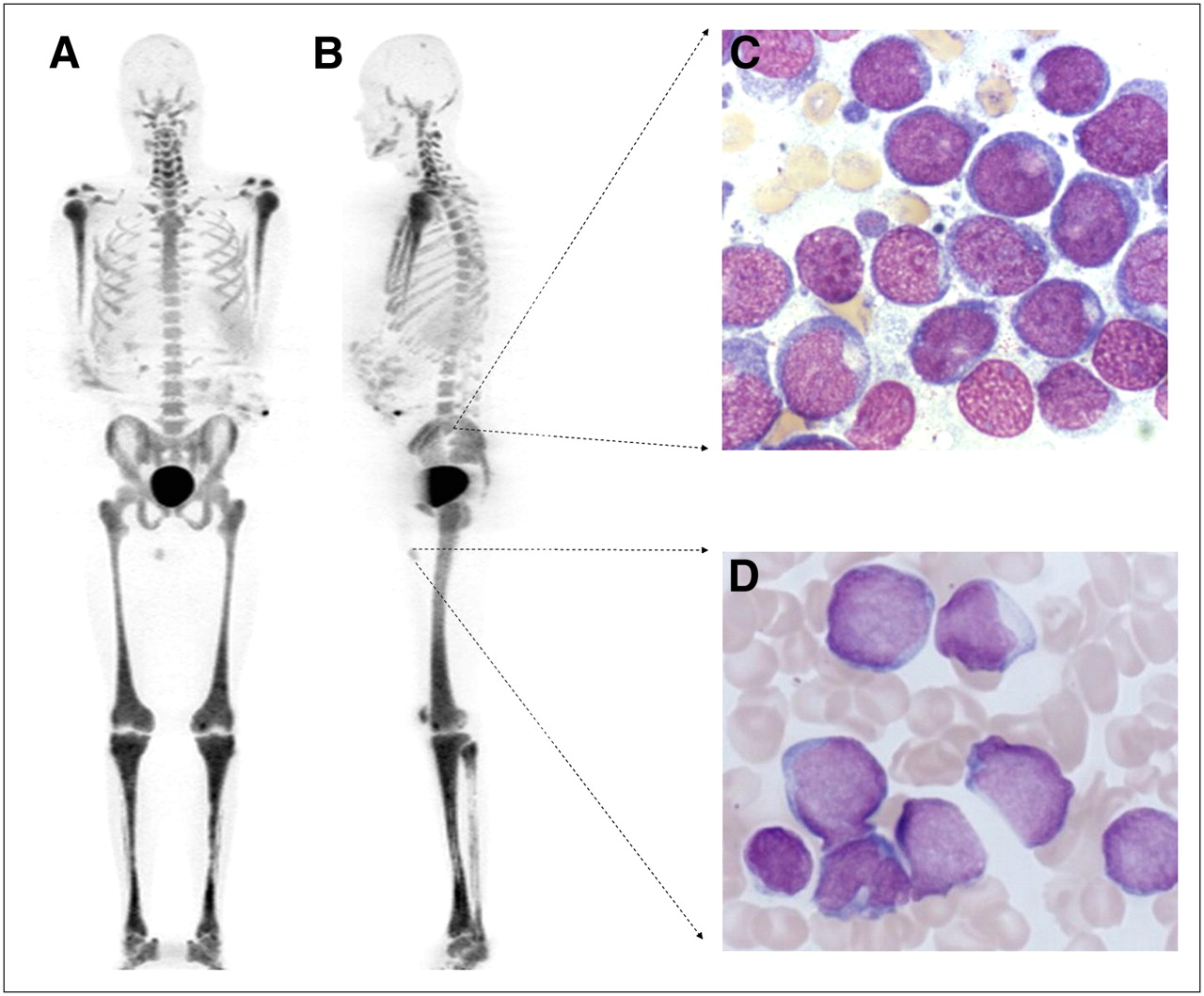
(A and B) Biodistribution of in vivo proliferation marker 18F-FLT in patient with refractory AML (patient 4) 60 min after injection of radiotracer (whole-body view [3-dimensional], maximum-intensity projection). Shown are intense uptake of 18F-FLT in hematopoietic bone marrow of central bones and extensive bone marrow expansion with intense tracer uptake. Tracer uptake is absent from bones not containing hematopoietic marrow (forearms and skull). Scans also indicate intense focal extramedullary 18F-FLT uptake in projection of right testicle. (C) Hematoxylin staining of peripheral blood demonstrating 99% leukemic blasts. (D) Biopsy verification of testicular leukemia manifestation.
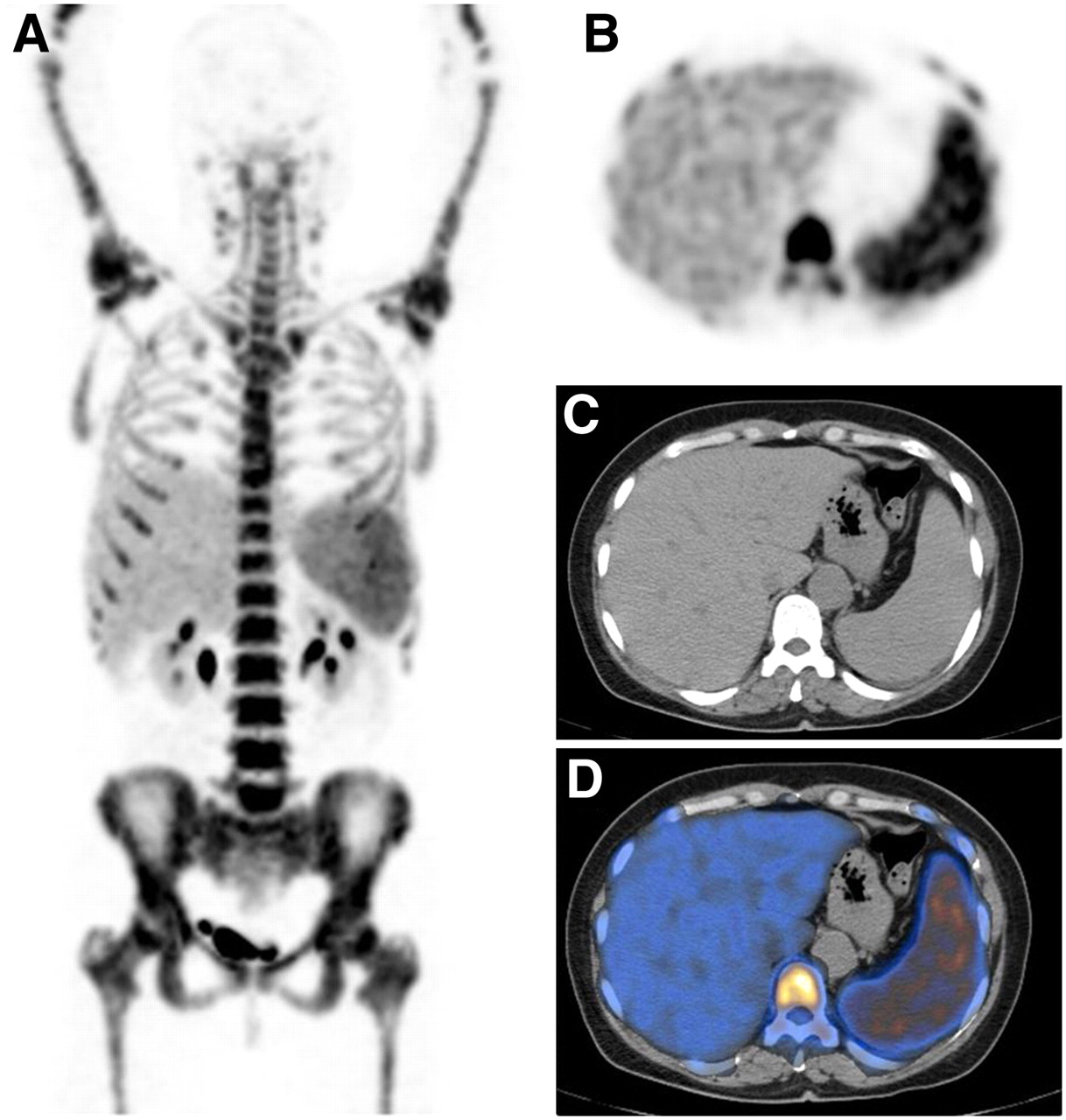
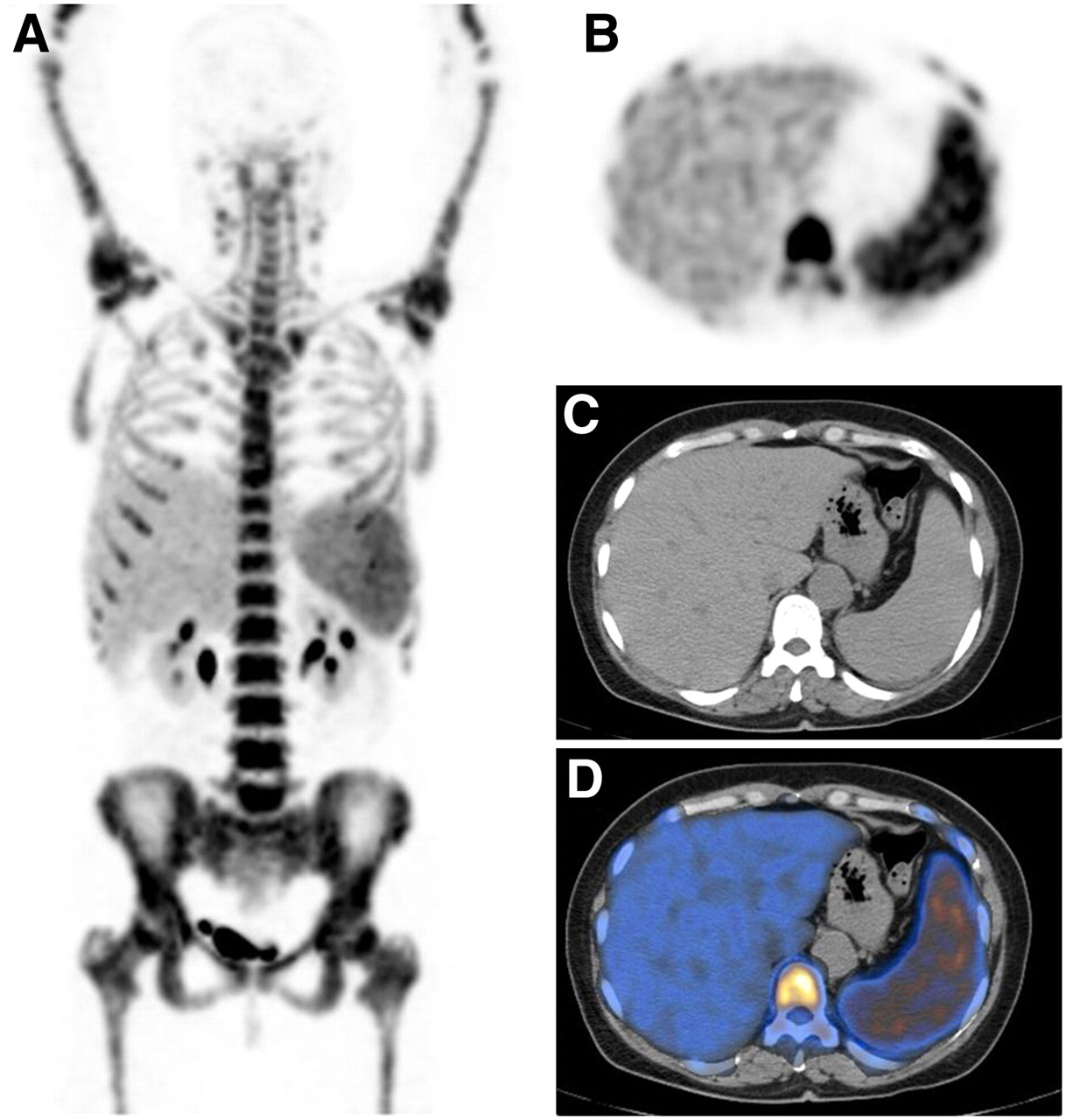
One of 2 typical distribution patterns of 18F-FLT in patient with initial diagnosis of AML. (A) 18F-FLT PET (whole-body view [3-dimensional], maximum-intensity projection) demonstrating intense tracer uptake in bone marrow and spleen. Distribution pattern in other organs is normal, as observed in controls. (B) Transaxial section of 18F-FLT PET demonstrating intense tracer uptake in bone marrow and spleen. (C) Corresponding section of helical CT demonstrating enlarged spleen. (D) Fused image (18F-FLT PET/CT).

A second distribution pattern of 18F-FLT in AML patients with active disease. Maximum-intensity projection of 18F-FLT PET shows moderate 18F-FLT uptake in bone marrow (A). Also visible are intense meningeal 18F-FLT uptake (B), pericardial/mediastinal uptake (D), peritoneal uptake (F), and iliac uptake (H). Corresponding CT sections indicate no intracranial pathology (C) but pericardial effusion and mediastinal lymphadenopathy (E), peritoneal effusion (G), and enlarged iliac lymph nodes (I). Meningeal disease and further extramedullary leukemia manifestation sites (peritoneal and iliac lymph nodes) have been verified morphologically.
The spleen was the organ with the second highest uptake of 18F-FLT (Fig. 2; Table 1). In 6 patients with high 18F-FLT uptake in the bone marrow and spleen, no extramedullary focal lesions were identified at 18F-FLT PET. A different biodistribution pattern was observed in 4 patients also presenting with extramedullary lesions having focally increased 18F-FLT uptake. Increased meningeal tracer uptake indicated meningeal disease in 2 patients, as was further confirmed cytologically (Fig. 3). Lymph node manifestations were visualized in 2 patients; manifestations in the thyroid, pericardium, and abdomen in another patient (Fig. 3). Interestingly, after concomitant myeloablative treatment and transplant failure, no uptake of 18F-FLT was present in the bone marrow and spleen in 1 patient (Fig. 4).
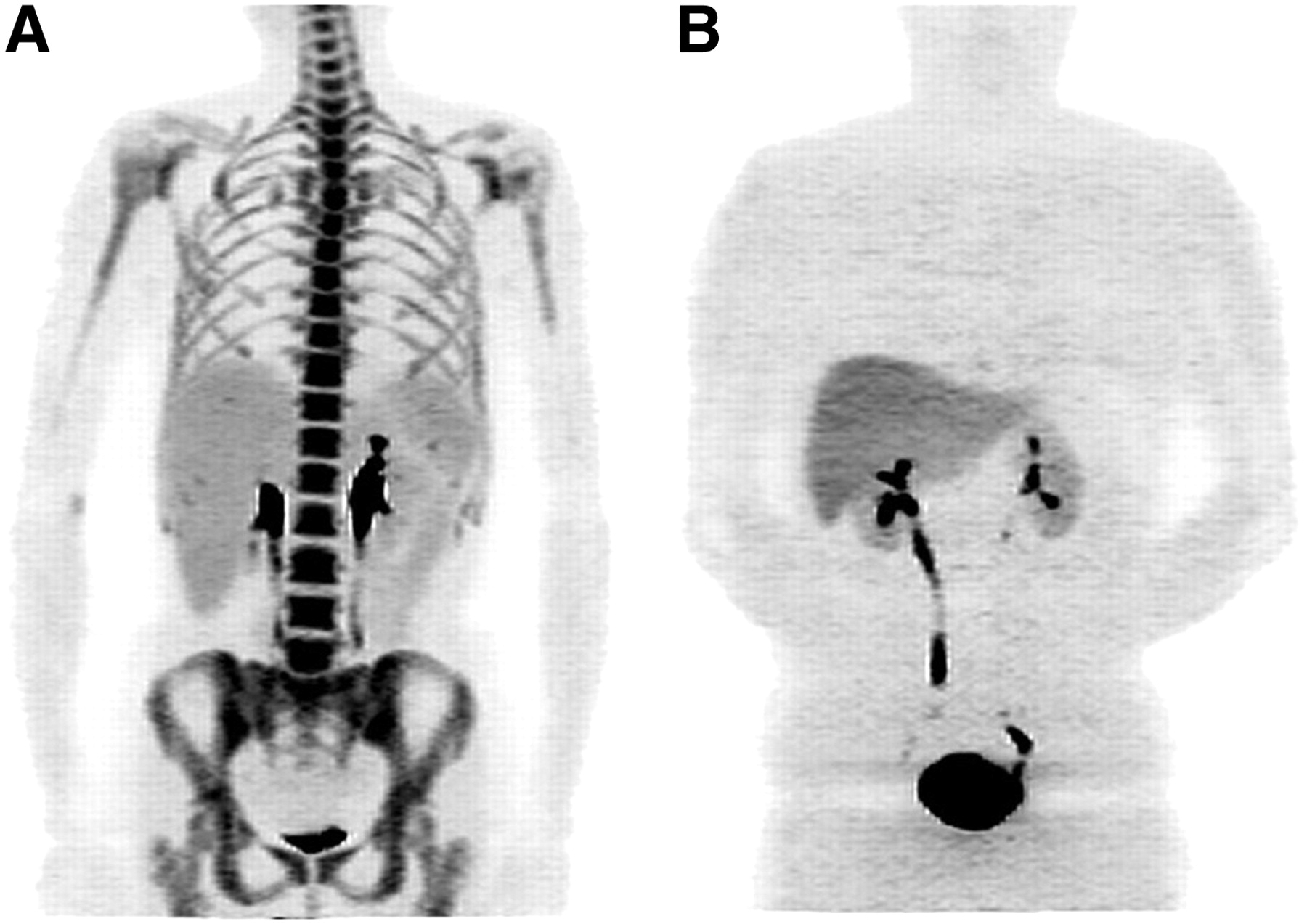
(A) Maximum-intensity projection (MIP) of 18F-FLT PET in patient 9 with active disease and intense tracer uptake in bone marrow and spleen. (B) MIP of 18F-FLT PET in patient 11 (not included in prospective study collective) after myeloablative treatment. At time of imaging, failure of bone marrow transplantation was diagnosed. No tracer uptake in bone marrow could be observed; administered activity was completely excreted by liver and kidneys.
Group Comparison of 18F-FLT Biodistribution
Semiquantitative evaluation of 18F-FLT uptake in bone marrow returned an average mean SUV of 11.5 ± 3.1, which was significantly higher than in controls (mean 18F-FLT SUV, 6.6 ± 1.2, P < 0.05; Fig. 5). The average maximum 18F-FLT value was also significantly higher (13.9 ± 4.5 vs. 9.7 ± 2.1, P < 0.05). Both mean and maximum 18F-FLT SUVs were significantly higher in the spleen, which showed only background activity in controls (mean 18F-FLT SUV, 6.1 ± 4.5 and 1.8 ± 0.7, P < 0.05; maximum 18F-FLT SUV, 7.6 ± 5.9 and 3.1 ± 2.3, P < 0.05; Fig. 5). However, there was an overlap of bone marrow or spleen 18F-FLT uptake in patients with leukemia and in controls (Fig. 6).

Biodistribution of 18F-FLT in bone marrow, spleen, and normal organs in patients with leukemia (10 patients) and in controls (10 patients). Mean uptake values of 18F-FLT are shown. Significantly higher 18F-FLT uptake in bone marrow (P < 0.05) and spleen, and significantly lower 18F-FLT uptake in liver, was seen in leukemia patients than in controls (P < 0.05).

(A) Scattergram of mean 18F-FLT SUVs indicating significantly higher 18F-FLT uptake in bone marrow of patients with leukemia (10 patients) than in controls (10 patients, P < 0.05), with some overlap between groups. (B) Significantly higher 18F-FLT uptake in spleen of patients with AML than in controls (P < 0.05). *) indicates values of patient 10 with second complete remission.
Interestingly, retention of 18F-FLT in the liver was significantly lower in AML patients than in controls (average mean 18F-FLT SUV, 3.4 ± 1.1 and 5.0 ± 1.9; average maximum 18F-FLT SUV, 4.2 ± 1.5 and 6.5 ± 2.5; P < 0.05). Biodistribution of 18F-FLT in other normal organs was similar to that of controls. Accordingly, statistical analysis did not reveal significant differences of 18F-FLT biodistribution in the lungs, intestines, kidneys, brain, or bone (Fig. 5).
Correlation of 18F-FLT Uptake in Bone Marrow and Number of Blasts Identified at BMP
Linear regression analysis of bone marrow uptake of 18F-FLT and number of leukemic blasts identified by BMP revealed no significant correlation for either mean 18F-FLT SUV (r2 = 0.24, P = 0.22) or maximum 18F-FLT SUV (r2 = 0.23, P = 0.18).
DISCUSSION
Recently, the thymidine analog 18F-FLT was suggested for noninvasive assessment of proliferation and more specific imaging of a variety of solid neoplasms, including lymphoma (15,20,22–24). To our knowledge, this was the first study showing the biodistribution of 18F-FLT in patients with AML. Here, we have demonstrated that 18F-FLT PET is feasible for noninvasive visualization of leukemia manifestation sites. An interesting finding is a varying distribution pattern in patients with AML. Whereas the majority of patients showed intense uptake of the radionucleoside in bone marrow and spleen, extramedullary lesions were detected in 4 patients. Because lymph node basins, spleen, abdomen, mediastinum, thyroid, long bones, and brain present with missing or only marginal background activity in controls, lesions with focally increased 18F-FLT uptake reflecting elevated proliferative activity could easily be detected by visual image interpretation. It remains to be determined if knowledge of extramedullary manifestation sites affects the therapeutic strategy or estimation of individual prognosis. However, these initial results warrant an analysis of a larger series of patients.
Besides visualization of leukemia manifestation sites, 18F-FLT potentially represents an imaging biomarker for disease activity. The significantly higher uptake of 18F-FLT in bone marrow and spleen observed in patients with relapsed, refractory, or untreated leukemia than in controls is presumably related to deregulated cell cycle progression of leukemic blasts. Recently, our group demonstrated rapid uptake of 18F-FLT in an aggressive lymphoma cell line (DoHH2) (23) and of the related nucleoside 123I-ITdU in HL60 leukemia cells (17). Leukemic blasts exhibit a more than 10-fold overexpression of thymidine kinase 1, which is a key enzyme for intracellular trapping of nucleosides such as 18F-FLT (25,26). Also, nucleoside transporters (ENT-1) are markedly overexpressed, facilitating uptake of nucleosides such as cytosine arabinoside or 18F-FLT (27).
In a pilot study, we recently demonstrated proliferation-dependent 18F-FLT uptake in a follicular lymphoma cell line (23) and in a mouse lymphoma xenotransplant model (28). In a first clinical trial comprising 34 patients with low- or high-grade lymphoma, linear regression analysis indicated a significant correlation between 18F-FLT uptake and proliferation fraction as indicated by Ki-67 immunostaining (r = 0.84, P < 0.0001) (15). A similar correlation between 18F-FLT retention and proliferation fraction was described in other solid tumors (20,24). However, because normal bone marrow also shows a physiologically increased proliferation rate and therefore increased 18F-FLT uptake (20), the proliferative activity of leukemic blasts and normal bone marrow cannot be distinguished with 18F-FLT PET. This is particularly the case in the posttreatment situation, which applies to 9 of 10 patients of our series. Accordingly, there was only a tendency toward higher retention of 18F-FLT in bone marrow containing high numbers of leukemic blasts—a difference that did not reach statistical significance (r2 = 0.24, P = 0.22). The lack of a strong correlation between the 18F-FLT SUV and blasts in the bone marrow suggests that 18F-FLT uptake is not related exclusively to the neoplastic compartment. A more valid assessment of the ability of 18F-FLT to assess disease activity and extent should be evaluated in patients with newly diagnosed AML.
Imaging proliferation in leukemia potentially enables estimation of response to treatment and patient outcome, which has been shown recently in clinical trials including patients with malignant lymphoma, breast cancer, or glioma (29–33). In an animal model of fibrosarcoma, it was reported that 18F-FLT uptake decreased early after antiproliferative treatment with 5-fluorouracil or cisplatin (30). In a mouse lymphoma xenotransplant model, a significant decrease in 18F-FLT uptake had already been observed 48 h after chemotherapy with cyclophosphamide (28). However, data are preliminary, and clinical trials comprising more patients are needed to further validate 18F-FLT as a marker for therapy response.
In a patient with temporary transplant failure after myeloablative chemoradiotherapy, no 18F-FLT accumulation in bone marrow or spleen was observed, further illustrating the selective uptake of 18F-FLT in proliferating tissues (Fig. 4). The selectivity of 18F-FLT also suggests a therapeutic role of radiolabeled nucleosides. Antimetabolites such as cytosine arabinoside are standard drugs for induction treatment of leukemia but are not potent enough to maintain long-term disease-free survival (34). Coupling Auger-electron–emitting isotopes may be appropriate for nanoirradiation of DNA and entire leukemic cell kill. Recently, our group demonstrated specific induction of apoptosis and leukemic cell kill with the Auger-electron–emitting radionucleoside 123I-ITdU (17). These in vitro results are encouraging and will be recapitulated in animal models and potentially in the human disease.
Several limitations have to be considered when transferring our results to the clinic. Our results apply to a pilot study comprising 10 patients only. The patient collective was also heterogeneous and did not cover all genetic subtypes of AML. As previously reported for the standard radiotracer 18F-FDG, false-positive findings may also occur using 18F-FLT as a PET tracer because an increased proliferation rate is not specific to malignant tumors. 18F-FLT acts as a chain terminator and is only marginally incorporated into DNA and therefore not a direct measure of proliferation (22). In vitro studies indicate that 18F-FLT uptake is closely related to thymidine kinase 1 activity and respective protein levels (35), as well as to expression of nucleoside transporters in the cellular membrane (36). 18F-FLT is considered to reflect thymidine kinase 1 activity and, hence, S-phase fraction rather than DNA synthesis. Both thymidine kinase and ENT are overexpressed in leukemia, facilitating preferential uptake of 18F-FLT. However, the detailed uptake mechanism of 18F-FLT is yet unknown, and the influence of membrane transporters and various nucleoside metabolizing enzymes remains to be determined. 18F-FLT undergoes glucuronidation leading to enhanced liver uptake (15), which was also observed in our series. Because of negligible background uptake of 18F-FLT in the brain and the skull (Figs. 1–3⇑⇑ and 5), specific imaging of proliferation may be appropriate for detection of meningeal disease, which could be demonstrated in 2 members of the patient collective. However, the numbers were small, and the sensitive detection of meningeal disease may not hold up in a larger series.
CONCLUSION
We have demonstrated preferential uptake of 18F-FLT in leukemia manifestation sites indicating that molecular imaging of leukemia based on deregulated cell cycle progression is feasible. Implications for clinical management and assessment of individual prognosis need to be addressed in a larger series.
Acknowledgments
This work was supported in part by grant Bu-1424/1 (KFO 120, P3) from Deutsche Forschungsgemeinschaft (DFG, German Research Foundation).
Footnotes
-
↵* Contributed equally to this work.
-
COPYRIGHT © 2008 by the Society of Nuclear Medicine, Inc.
References
- Received for publication June 22, 2008.
- Accepted for publication July 24, 2008.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- The prevalence of extramedullary acute myeloid leukemia detected by 18FDG-PET/CT: final results from the prospective PETAML trial
- PET Imaging of Proliferation with Pyrimidines
- Multiplexed mAbs: a new strategy in preclinical time-domain imaging of acute myeloid leukemia
- 18F-FDG-PET/CT for detection of extramedullary acute myeloid leukemia
- Imaging Colon Cancer Response Following Treatment with AZD1152: A Preclinical Analysis of [18F]Fluoro-2-deoxyglucose and 3'-deoxy-3'-[18F]Fluorothymidine Imaging
- Neoplastic meningitis in patients with acute myeloid leukemia scheduled for allogeneic hematopoietic stem cell transplantation
- PET/CT with 18F-FLT Is Unlikely to Cause Significant Hepatorenal or Hematologic Toxicity
- Incidental Detection of Acute Lymphoblastic Leukemia on [18F]Fluorodeoxyglucose Positron Emission Tomography