


Abstract
The purpose of this study was to evaluate the effects of pegfilgrastim, a long-acting granulocyte colony-stimulating factor, on the normal biodistribution of 18F-FDG in an animal model and in humans. Methods: Two groups of 12 rats received a single subcutaneous injection of either normal saline or pegfilgrastim. One, 7, 14, and 21 d after injection, biodistribution studies were performed 1 h after 18F-FDG injection. Sixteen breast cancer patients underwent baseline 18F-FDG PET/CT and, approximately 1 wk after receiving 1 dose of docetaxel and adjunctive pegfilgrastim, follow-up 18F-FDG PET/CT (scan 2). Standardized uptake values corrected for lean body mass (SUL) were determined for several normal organs before and after therapy. Results: In rats, bone marrow 18F-FDG uptake (standardized uptake value) was higher in the pegfilgrastim group 1 d after injection (mean ± SD, 8.3 ± 4.1 vs. 2.5 ± 0.2, P < 0.05), whereas 18F-FDG uptake in blood was lower (0.41 ± 0.06 vs. 0.49 ± 0.01, P < 0.05). In patients, mean SUL was higher in bone marrow (4.49 ± 1.50 vs. 1.33 ± 0.22, P < 0.0001), spleen (3.29 ± 0.83 vs. 1.23 ± 0.23, P < 0.0001), and liver (1.45 ± 0.25 vs. 1.31 ± 0.23, P = 0.01) but lower in brain (4.18 ± 0.76 vs. 5.14 ± 1.44, P < 0.01) on scan 2 than on the baseline scan. Conclusion: In both the animal model and humans, pegfilgrastim markedly increased bone marrow uptake of 18F-FDG and reduced 18F-FDG uptake in some normal tissues. These profound alterations in 18F-FDG biodistribution induced by pegfilgrastim must be considered when one is evaluating quantitative 18F-FDG PET scans for tumor response to therapy.
PET with 18F-FDG is a useful noninvasive imaging tool for evaluating tumor response to therapy (1–3). Typically, a baseline scan and then a follow-up scan after treatment are obtained. In the interval between scans, patients with nonmyeloid malignancies may receive adjunctive hematopoietic cytokines to counteract the myelosuppressive side effects of the administered chemotherapeutic agents. Filgrastim (Neupogen; Amgen Inc.) and pegfilgrastim (Neulasta; Amgen Inc.) are granulocyte colony-stimulating factors (G-CSFs) that act on the monocyte–macrophage hematopoietic cell lineage to stimulate progenitor proliferation, differentiation, and functional activation of the mature hematopoietic cells (4–6). The 2 agents have been shown to have similar efficacy in decreasing the incidence of chemotherapy-induced neutropenia and the resulting complicated infections (7–9).
Pegfilgrastim, a covalent conjugate of filgrastim and monomethoxypolyethylene glycol (10), was approved by the Food and Drug Administration in 2002. Pegfilgrastim and filgrastim have the same mechanism of action, but the addition of the glycol moiety reduces renal clearance of pegfilgrastim, compared with that of filgrastim, prolonging the serum half-life of the drug in vivo (10,11). In humans, clearance of pegfilgrastim depends on neutrophil receptor binding and correlates directly with serum neutrophil count. Consequently, pegfilgrastim can be administered as a single dose rather than the daily doses required for filgrastim (10), and this advantage has led to its increased and preferred use.
Clinical studies have demonstrated that the administration of short-acting hematopoietic cytokines, such as filgrastim, to patients shortly before imaging evaluation with 18F-FDG PET markedly increases 18F-FDG accumulation in bone marrow (12–16) and spleen (16). Bone marrow is a frequent site of metastatic disease in several tumor types, and this altered biodistribution should not be interpreted as diffuse metastases to bone marrow or bone.
Similar to the findings reported after the administration of short-acting G-CSF, we have observed increased 18F-FDG accumulation in the bone marrow and spleen of patients who have received a long-acting G-CSF, pegfilgrastim, shortly before 18F-FDG PET. The effects of pegfilgrastim on normal 18F-FDG biodistribution have not, however, been formally evaluated. At the time of the initial publications evaluating the effects of hematopoietic growth factors on 18F-FDG biodistribution, pegfilgrastim was not yet approved by the Food and Drug Administration for routine use in the care of oncology patients.
We hypothesized that the expected preferential accumulation of 18F-FDG in bone marrow and spleen after pegfilgrastim could decrease the bioavailability of 18F-FDG to other normal organs and to tumor. This result has not been reported in previous preclinical biodistribution (15) or patient (16) studies. In addition, we hypothesized that the effects of pegfilgrastim might last longer than the effects of filgrastim because of its longer serum half-life in patients both with and without neutropenia (11).
The purpose of this study was to evaluate, in an animal model and in patients, the effect of pegfilgrastim on uptake of 18F-FDG in bone marrow and spleen, the time course of these effects, and the effect of pegfilgrastim on normal biodistribution of 18F-FDG.
MATERIALS AND METHODS
Animal Studies
Twenty-four healthy, female Lewis rats (Charles River Laboratories) were divided into 2 groups. Twelve rats received a single subcutaneous injection of normal saline, and 12 rats received a single dose of pegfilgrastim (100 μg/kg subcutaneously). At 1, 7, 14, and 21 d after injection of pegfilgrastim or saline, 3 rats from each group were sacrificed and biodistribution studies performed. All rats were kept fasting overnight and received a 7.4-MBq (200 μCi) injection of 18F-FDG via the tail vein. Approximately 1 h after 18F-FDG injection, the rats were sacrificed and normal organs excised. Bone marrow was removed from both femurs by curettage after fracture of the cortical bone (15). Tissues were weighed, and 18F-FDG activity in the tissues determined by γ-counting. Decay-corrected 18F-FDG activity in tissues is presented as standardized uptake values.
Patients and Treatment Regimen
This study was a retrospective analysis of 18F-FDG PET/CT scans of 16 women with newly diagnosed breast carcinoma who were participating in a pilot study at our institution evaluating response patterns to neoadjuvant chemotherapy. The study was approved by our institutional review board, and informed written consent was obtained for both the treatment and the imaging portions of the study.
The patients had infiltrating breast carcinoma of clinical stage T1c, T2, T3, or T4; any N; and M0 and had not received any prior therapy, including surgical resection of the primary tumor. The inclusion criteria included adequate blood counts, defined as an absolute neutrophil count of at least 1,500/mm3, a platelet count of at least 100,000/mm3, and a hemoglobin level of at least 8 g/dL. Patients were excluded from the study if they were pregnant or nursing, and none was diabetic.
Patients received preoperative chemotherapy with 4 cycles of docetaxel (Taxotere; Aventis Pharmaceuticals Inc.). Docetaxel (100 mg/m2) was administered on day 1 of each 14-d cycle. Because neutropenia is a side effect of docetaxel, a 6-mg subcutaneous injection of pegfilgrastim was administered to all patients on day 2 of each cycle as adjunctive therapy to maintain dose density.
18F-FDG PET/CT was performed as part of the clinical trial to evaluate the usefulness of early metabolic imaging for predicting tumor response or resistance to therapy. 18F-FDG PET/CT images were obtained just before the start of therapy and then at about day 8, after the first cycle of chemotherapy. Patients received single doses of docetaxel and pegfilgrastim in the interval between PET/CT scans.
18F-FDG PET/CT
The patients fasted for a minimum of 4 h and had blood glucose levels no greater than 200 mg/dL just before injection of the 18F-FDG. A weight-based dose of 18F-FDG (8.14 MBq/kg [0.22 mCi/kg]) was injected intravenously in the arm contralateral to the primary breast carcinoma. The mean 18F-FDG radioactivity injected for all scans was 618 ± 167 MBq (16.7 ± 4.5 mCi). Oral, but not intravenous, contrast material was administered for the CT portion of the study.
After an approximately 60-min uptake phase, a combined PET/CT scan (Discovery LS; GE Healthcare) was obtained from the mid-skull level to the mid-femur level. Whole-body CT was performed first, with a 4-slice multidetector helical scanner and the following parameters: 140 kV, weight-based amperage (range, 80–160 mA), 0.8 s per CT rotation, a pitch of 6, a table speed of 22.5 mm/s, 722.5-mm coverage, and a 31.9-s acquisition time. A CT transmission map was generated for image fusion. Emission data were acquired for 5 min at each bed position.
PET images were reconstructed using the ordered-subset expectation maximization algorithm (2 iterations, 28 subsets), an 8-mm gaussian filter with a 128 × 128 matrix, and CT attenuation correction.
Quantitative Image Analysis
Regions of interest (ROIs) of nearly constant size and location were manually drawn on sections of spleen (number of pixels, 109 ± 19), liver (427 ± 28), lung (95 ± 20), and brain (70 ± 10) on 3 consecutive transaxial PET slices. The mean number of pixels did not significantly differ between the baseline scan and scan 2 for the ROIs of any organ. ROIs were drawn in the inferior right hepatic lobe (to avoid large veins or the biliary tree), the posterior right upper lobe of the lung, and the left cerebellum. The mean standardized uptake value corrected for lean body mass (SULmean) was determined for the ROI on each transaxial PET slice, and the average SULmean of the 3 transaxial slices was used for further analysis. The SULmean in brain could not be determined for 4 patients because only a small portion of the cerebellum was included in the images.
SULmean in bone marrow was determined by placing a 1.5-cm circular ROI in the middle of T10, T11, and T12 and taking the average SULmean of bone marrow in these 3 vertebral bodies. To determine the SULmean of blood, we placed 1.2-cm circular ROIs in the center of the ascending aorta, from the level of the carina cranially, on 6 consecutive transaxial PET slices and used the average of these. The maximum standardized uptake value corrected for lean body mass (SULmaximum) was determined for the primary tumors. All ROIs were placed using CT guidance.
Statistical Analysis
For the animal studies, differences in tissue uptake of 18F-FDG between the pegfilgrastim and saline groups were compared by the t test. ANOVA was used to evaluate changes in 18F-FDG uptake in bone marrow over time in the animal studies. For patient studies, paired t tests were used to compare the average SULmean values of normal organs on the baseline and follow-up PET/CT scans and to compare patient and technical parameters that can affect the standardized uptake value corrected for lean body mass (SUL). A P value of less than 0.05 was considered significant, using a 1-tailed t test.
RESULTS
Animal Studies
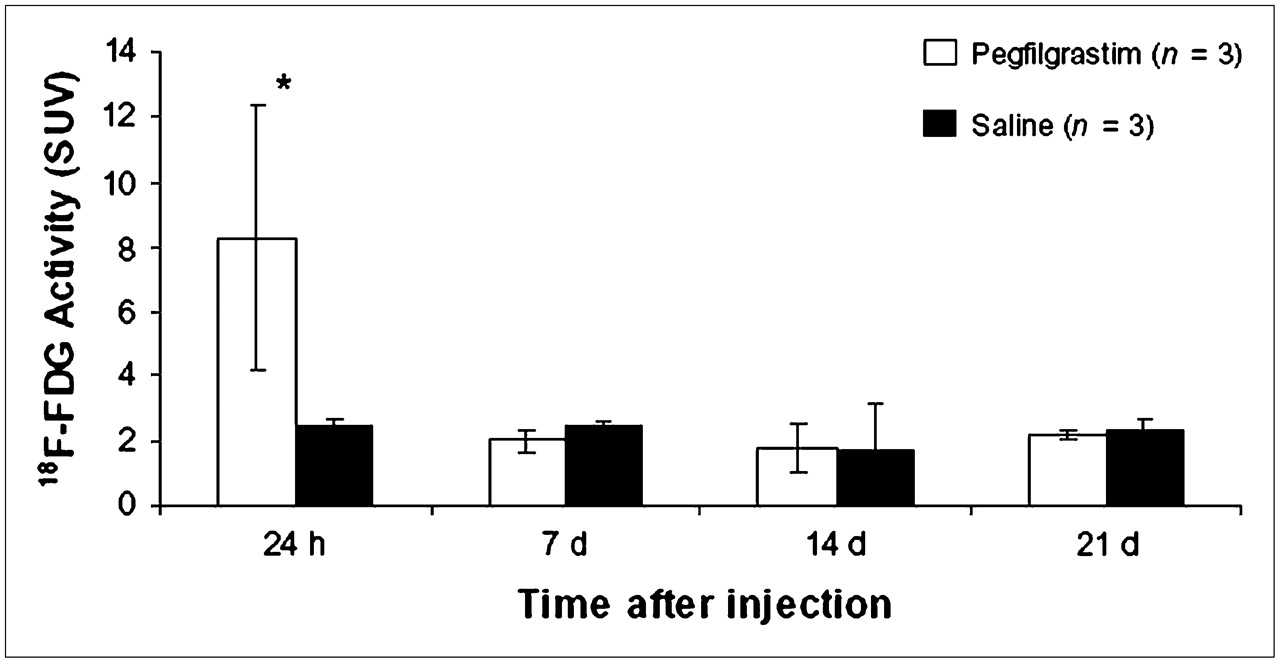
18F-FDG activity in normal tissues at 1 h after radiotracer injection is presented in Figure 1. Twenty-four hours after pegfilgrastim or saline administration, 18F-FDG activity (standardized uptake value) in bone marrow was much higher in the pegfilgrastim group than in the saline group (8.3 ± 4.1 vs. 2.5 ± 0.2, P < 0.05), whereas activity in blood (0.41 ± 0.06 vs. 0.49 ± 0.01) and kidneys (1.3 ± 0.2 vs. 1.7 ± 0.2) was lower (P < 0.05). Activity in brain tended to be lower in the pegfilgrastim group (6.8 ± 1.2 vs. 8.2 ± 0.7, P = 0.07).

18F-FDG activity in tissues of rats. Values are mean ± SD (n = 3 rats per group). (A) At 24 h after injection, 18F-FDG activity is higher in bone marrow and lower in blood and kidneys in pegfilgrastim group (*P < 0.05). (B) At 7 d after injection, 18F-FDG uptake is lower in bone marrow and liver and higher in muscle in pegfilgrastim group (*P < 0.05).
Seven days after pegfilgrastim or saline injection, the level of 18F-FDG activity in most tissues was similar between the pegfilgrastim and saline groups. 18F-FDG activity in bone marrow (2.0 ± 0.3 vs. 2.5 ± 0.2, P = 0.05) and liver (0.53 ± 0.03 vs. 0.66 ± 0.04, P < 0.01) was significantly lower in the pegfilgrastim group than in the saline group, whereas significantly higher activity was found in muscle (1.2 ± 0.2 vs. 0.55 ± 0.2, P = 0.01). Almost all tissues showed no significant differences in 18F-FDG uptake between the pegfilgrastim and saline groups at 14 and 21 d (data not shown). The only exceptions were colon and bone, which showed decreased activity (respectively, 3.7 ± 0.5 vs. 3.0 ± 0.2, P = 0.04, and 0.25 ± 0.05 vs. 0.20 ± 0.2, P = 0.05) in the saline group at 21 d. Bone marrow uptake of 18F-FDG was significantly higher (P < 0.05) in the rats receiving the dose of pegfilgrastim 24 h before the 18F-FDG study (8.3 ± 4.1) than in the rats receiving the dose 7, 14, or 21 d before the 18F-FDG study (2.0 ± 0.3, 1.8 ± 0.8, and 2.2 ± 0.1, respectively; Fig. 2). This was not the case in the control group.
18F-FDG activity in bone marrow of rats vs. time. Values are mean ± SD (n = 3 rats per group at each time point). Bone marrow 18F-FDG activity was higher (*P < 0.05) in rats 24 h after pegfilgrastim injection. This increase was not observed after injection of saline.
Patient Studies
All 16 patients received the prescribed single doses of docetaxel and pegfilgrastim during the interval between the baseline PET/CT scan and scan 2. All patients received pegfilgrastim 1 d after receiving docetaxel. The mean interval was 14 ± 11 d (range, 8–52 d) between the baseline PET/CT scan and scan 2; 7 ± 0.7 d between docetaxel administration and scan 2; and 6 ± 0.7 d between pegfilgrastim administration and scan 2. Patient and technical parameters that can affect SUL determination are shown in Table 1.
Parameters That Can Affect SUL Measurement
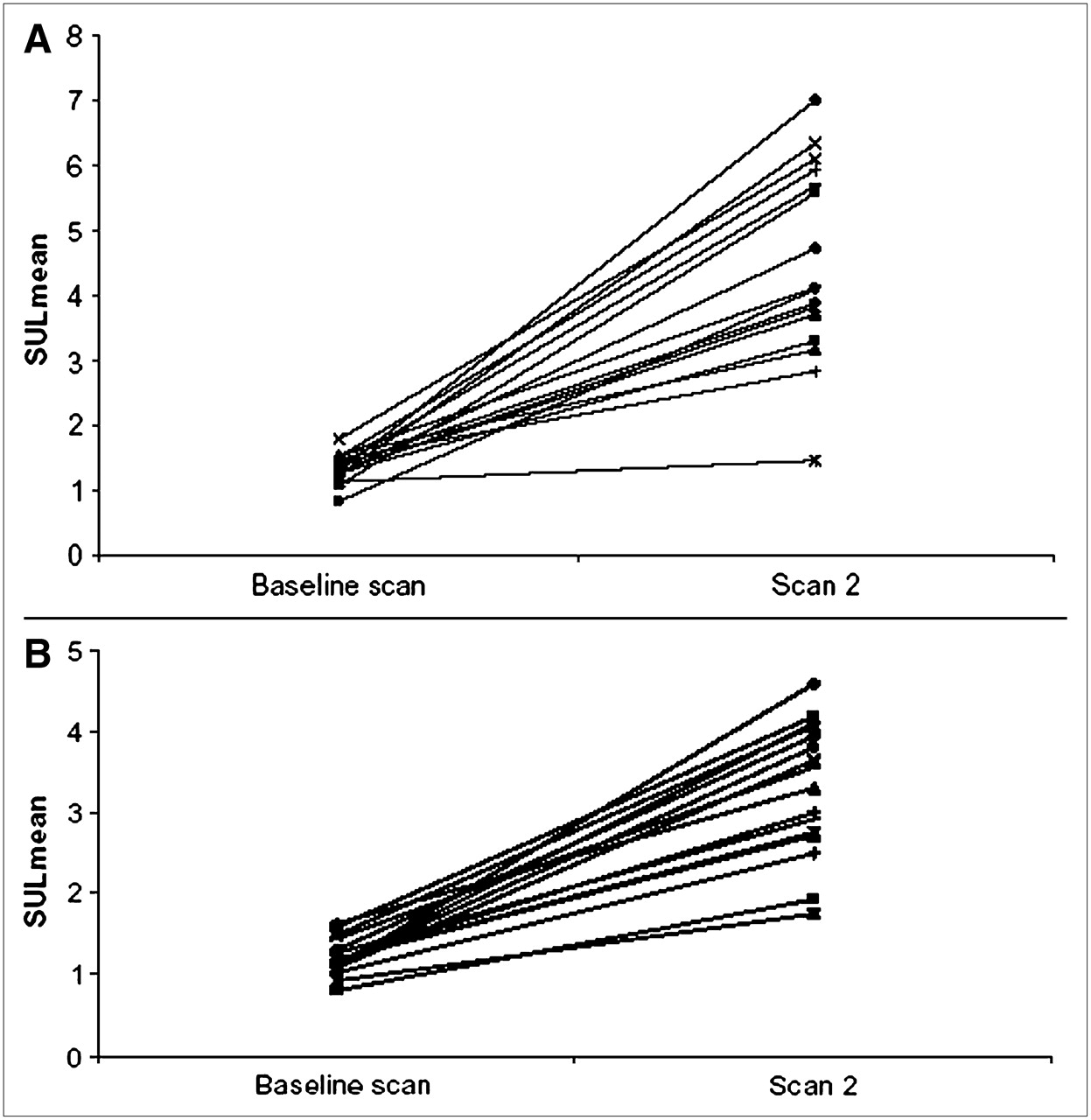
18F-FDG uptake in the bone marrow and spleen of individual patients is shown in Figure 3. The average SULmean was significantly higher in bone marrow (4.49 ± 1.50 vs. 1.33 ± 0.22, P < 0.0001) and spleen (3.29 ± 0.83 vs. 1.23 ± 0.23, P < 0.0001) on scan 2 than on the baseline scan. SULmean in blood, brain, liver, and lung on the baseline scan and scan 2 is presented in Table 2. Mean 18F-FDG uptake in brain was significantly less on scan 2 than on the baseline scan (4.18 ± 0.76 vs. 5.14 ± 1.44, P < 0.01), and 18F-FDG uptake was lower in blood on scan 2; however, this difference did not reach statistical significance (0.87 ± 0.18 vs. 0.93 ± 0.16, P = 0.08). 18F-FDG uptake in liver was higher on scan 2 than on the baseline scan (1.45 ± 0.25 vs. 1.31 ± 0.23, P = 0.01). Images from a representative case are shown in Figure 4. Tumor SULmaximum decreased significantly between the baseline scan and scan 2 (6.25 ± 5.07 vs. 3.74 ± 2.10, P = 0.02); however, the full results for tumor response will be reported elsewhere.

18F-FDG uptake in bone marrow (A) and spleen (B) in patients (n = 16) at baseline and after single doses of adjuvant pegfilgrastim (scan 2). Average SULmean in bone marrow and spleen is significantly higher on scan 2 (P < 0.0001).
18F-FDG Uptake (SULmean) in Normal Organs of Patients Before and After Therapy

Maximum-intensity-projection images at baseline (A) and after single doses of docetaxel and pegfilgrastim (B) in patient 9. Diffusely increased 18F-FDG activity is seen in bone marrow (arrowhead) and spleen (curved arrow) on scan 2. Multifocal right breast cancer has intense 18F-FDG activity on both scans; however, activity appears less intense on scan 2 (straight arrows). Physiologic 18F-FDG activity is seen in brain, kidneys, bladder, liver, and colon.
DISCUSSION
Our rat study showed that pegfilgrastim induces a rapid rise in 18F-FDG uptake in bone marrow 24 h after administration of a single dose—a result that can be explained by increased cellular proliferation and metabolism in bone marrow because of pegfilgrastim-induced stimulation of neutrophil progenitor cells (4–6). This same finding for bone marrow was previously observed in different strains of rats after administration of a shorter-acting G-CSF, filgrastim (15), and was expected given that both drugs have the same mechanism of action. Unlike what happens in humans, and for unclear reasons, neither of the G-CSF agents seems to increase 18F-FDG uptake in rat spleen. One consideration is that the effects of pegfilgrastim on 18F-FDG uptake in spleen occur at time points different from those evaluated in this and previous studies.
In our patient study, bone marrow and splenic uptake of 18F-FDG was increased at 6–8 d after administration of a single 6-mg dose of pegfilgrastim in combination with chemotherapy. This effect was previously reported after patients had received short-acting G-CSF and granulocyte-macrophage colony-stimulating factor (12–16) but not after longer-acting pegfilgrastim. The explanation for the increased 18F-FDG uptake in bone marrow is posited to be the same in humans as in animals: increased cellular proliferation and metabolism in bone marrow because of pegfilgrastim-induced stimulation of neutrophil progenitor cells.
Our patient study also clearly demonstrated a rise in splenic uptake of 18F-FDG after pegfilgrastim administration, in accord with the effect of filgrastim on 18F-FDG uptake in spleen (16). In none of our patients did the pretherapy PET/CT studies performed just 2 wk before scan 2 show splenic disease. It is unlikely that such disease developed in the short interval between the scans. The diffuse increase in splenic 18F-FDG activity on the follow-up scan most likely represented G-CSF–induced extramedullary hematopoiesis, a phenomenon that has been reported to occur after administration of high-dose G-CSF (17,18). Increased hematopoiesis in spleen has been observed after shorter, intermittent therapy with G-CSF (19), and in the initial study reporting G-CSF–induced 18F-FDG uptake in spleen, patients had also received relatively few doses of short-acting G-CSF (16).
One limitation of this study was that the pegfilgrastim was administered as an adjunct to chemotherapy. Because we did not evaluate any patients who received chemotherapy alone, we cannot definitively state that the increased 18F-FDG activity in bone marrow was due to pegfilgrastim alone. That possibility is likely, however, because previous studies have demonstrated no significant rise in bone marrow SUL on serial 18F-FDG PET scans of patients who received chemotherapy, of several types, alone (15).
The results of our study also demonstrated that long-acting G-CSF affected 18F-FDG biodistribution in several normal organs. We observed significant declines in 18F-FDG uptake in brain on 18F-FDG PET patient scans obtained 6–8 d after pegfilgrastim administration, and 18F-FDG uptake in blood tended (P = 0.08) to be slightly lower at this time point. Sugawara et al. did not observe significant declines in blood SUL during or after G-CSF treatment (15); however, in their subgroup of patients receiving G-CSF, blood SUL was lower after G-CSF treatment than at baseline. The small number of patients likely limited the statistical power of that study. To our knowledge, the present report is the first on the effect of filgrastim or pegfilgrastim on 18F-FDG uptake in brain.
18F-FDG uptake is a measure of 18F activity in tissues and correlates somewhat with tumor blood flow and inversely with the serum concentration of glucose (20). Metabolic glucose rate can be calculated using a 3-compartment model. Free 18F-FDG in blood serves as the source of the precursor intracellular pool of 18F-FDG that is phosphorylated and retained within tumor cells (21). This model assumes the availability of sufficient radiotracer in the blood to enter the cell. Our study suggested that less 18F-FDG activity is in the blood, and thus in the brain, of patients who recently received G-CSF therapy, probably because of preferential 18F-FDG uptake by bone marrow and spleen.
The more rapid neutrophil response and mobilization of the peripheral blood progenitor cells induced by pegfilgrastim (10) may increase the glycolytic requirements of these organs. This possibility has potentially significant implications in the interpretation of 18F-FDG PET scans for following tumor response to therapy. The reduction of a tumor's source of 18F-FDG (blood) could result in erroneous underestimation of true SUL, not because of decreased tumor metabolism but just because less 18F-FDG was available to enter the cell and the glycolytic pathway. Because G-CSF is given as adjunctive therapy and not at baseline, underestimation of tumor SUL is more likely on posttherapy scans. Tumor response could be falsely interpreted if the underestimated tumor SUL is then compared with baseline SUL. Metabolic tumor-response criteria will need to take into account the changes in normal 18F-FDG biodistribution caused not only by antineoplastic agents but also by adjunctive therapies.
We attempted to determine the time course of pegfilgrastim effects on 18F-FDG uptake in rat bone marrow but found that, by day 7 after pegfilgrastim administration, 18F-FDG uptake in bone marrow had already normalized. This finding was surprising but probably explainable by the fact that we studied healthy rats, with normal neutrophil counts, who were likely able to clear the drug rapidly. In addition, overall metabolism may be faster in rats than in humans. We hypothesize that the effects of pegfilgrastim on 18F-FDG uptake in bone marrow might last longer in patients with lower neutrophil counts.
An unexpected finding in our patient study was the significant rise in 18F-FDG uptake in liver after chemotherapy and pegfilgrastim administration. This finding was not observed in the animals who received pegfilgrastim alone. We suspect the rise in liver 18F-FDG activity may have been secondary to the effects of docetaxel. Docetaxel is metabolized in liver, predominantly by the CYP3A4 isoenzyme (22). Induction of CYP3A4 transcription by hepatic nuclear factor 4 has been suggested (23,24), and hepatic nuclear factor 4 has also been shown to regulate transcription of genes involved in glucose entry into hepatocytes and glucose metabolism (25). It is possible that upregulation of hepatic nuclear factor 4 in the presence of docetaxel leads to increased glucose metabolism in liver.
CONCLUSION
The results of this study demonstrate that long-acting G-CSF has substantial effects on the normal biodistribution of 18F-FDG in rats and humans. These effects have significant implications for the interpretation of 18F-FDG PET scans obtained shortly after G-CSF therapy. Increased bone marrow and splenic 18F-FDG uptake should not be misinterpreted as metastases but could mask metastases in these organs. The decreased radiotracer activity in blood may lower the bioavailability of 18F-FDG to tumors, resulting in lower tumor SUL, similar to what was seen with the lower brain 18F-FDG uptake. Future criteria for PET evaluation of the metabolic response of tumors to therapy should take into account the changes in normal 18F-FDG biodistribution caused by both antineoplastic agents and adjunctive therapies.
Acknowledgments
The clinical trial was supported in part by NCI AVON Progress for Patients CA-88843-AV-15, by Damon Runyon-Lilly Clinical Investigator Award CI-3 from the Damon Runyon Cancer Research Foundation, and by NCI CA52880. Dr. Vered Stearns is a paid consultant to Aventis, Inc. The terms of this arrangement are being managed by the Johns Hopkins University in accordance with its conflict-of-interest policies.
References
- Received for publication December 14, 2005.
- Accepted for publication January 30, 2006.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Interobserver Agreement of Interim and End-of-Treatment 18F-FDG PET/CT in Diffuse Large B-Cell Lymphoma: Impact on Clinical Practice and Trials
- TBCRC 008: Early Change in 18F-FDG Uptake on PET Predicts Response to Preoperative Systemic Therapy in Human Epidermal Growth Factor Receptor 2-Negative Primary Operable Breast Cancer
- Pitfalls of Interim Positron Emission Tomography Scanning in Diffuse Large B-Cell Lymphoma
- 123I-MIBG Scintigraphy and 18F-FDG PET in Neuroblastoma
- Dynamic and Static Approaches to Quantifying 18F-FDG Uptake for Measuring Cancer Response to Therapy, Including the Effect of Granulocyte CSF