


Abstract
This study evaluated the yield of whole-body 18F-FDG PET/CT for the detection of unexpected 18F-FDG-avid additional primary malignant tumors in patients being evaluated by PET/CT for known or suspected malignances. Methods: Reports from whole-body 18F-FDG PET/CT scans from June 2001 to June 2003 were reviewed, and 1,912 patients (924 men and 988 women; mean age ± SD, 58.9 ± 13.9 y) who had been scanned for known or suspected malignant lesions were included in this study. The sites of known or suspected primary tumors included lung (28.6%), colon or rectum (12.4%), head or neck (12.1%), lymph nodes (10.9%), breast (7.6%), gynecologic organs (7.1%), genitourinary organs (4.2%), esophagus (3.6%), skin (melanoma) (3.5%), pancreas (2.5%), bone or soft tissue (2.2%), and other sites (5.4%). Lesions that were newly discovered on PET/CT, had not been previously detected by other modalities, and were atypical in location for metastases on the PET/CT study were interpreted as suggestive of a new primary malignant tumor. These abnormalities were compared with the final diagnosis obtained from the medical records, including pathologic reports. Results: PET-positive lesions suggestive of new primary malignant tumors were found in 79 (4.1%) of 1,912 patients. In 22 (1.2%) of 1,912 patients, these lesions were pathologically proven to be malignant. Proven sites were lung (7 lesions), thyroid (6 lesions), colon (4 lesions), breast (2 lesions), esophagus (2 lesions), bile duct (1 lesion), and head and neck other than thyroid (1 lesion). Two new lesions in the lung and the thyroid were proven malignant in 1 patient. In 17 patients, the treatment plan was changed and the new lesion was surgically resected after the PET/CT examination. In 10 patients, PET was falsely positive after pathologic assessment. False-positive sites included thyroid (5 lesions), uterus (2 lesions), head and neck other than thyroid (2 lesions), and lung (1 lesion). In 8 patients, the PET-positive lesions were considered benign after clinical follow-up of at least 8 mo. In 39 patients, the follow-up record was not yet available and the final diagnosis of the detected lesion has not yet been resolved. Conclusion: Whole-body PET/CT detected new, unexpected 18F-FDG-avid primary malignant tumors in at least 1.2% of patients with cancer.
Whole-body PET with 18F-FDG has been used successfully and with increasing frequency in the evaluation and clinical management of an expanding number of neoplasms (1–4). Reports also indicate that 18F-FDG PET has the potential for cancer screening and can detect new malignant tumors in a small fraction of asymptomatic individuals (5,6).
In the oncology patient, 18F-FDG PET has frequently been shown to be more accurate than CT in depicting unexpected foci of metastases or recurrent tumors that either were not seen or were difficult to observe on CT scans. Moreover, during a routine interpretation of 18F-FDG PET findings, abnormal incidental foci of hypermetabolism may be identified that are unlikely to be related to the neoplasm for which the patient was being scanned (7,8).
Combined PET/CT has recently emerged as a promising hybrid imaging modality and is now beginning to be used more routinely in clinical situations (9). PET/CT allows routine and precise fusion of metabolic PET images with high-quality CT images. The location of 18F-FDG uptake can be determined precisely from these PET/CT images. PET/CT remains in the early stages of its clinical implementation and evaluation but has been shown to be more accurate than PET alone in colon and lung cancer imaging (10,11). This increased accuracy is due to fewer uncertain or equivocal findings on PET/CT than on PET alone.
The present study retrospectively evaluated the yield of whole-body 18F-FDG PET/CT for the detection of unexpected additional primary malignant tumors in patients with known or suspected malignancies.
MATERIALS AND METHODS
Patient Population
A total of 1,912 patients (924 men and 988 women; mean age ± SD, 58.9 ± 13.9 y) who had known or suspected primary malignant lesions and who had undergone whole-body 18F-FDG PET/CT from June 2001 to June 2003 were retrospectively included for analysis. The sites of the known or suspected primary tumors included lung (28.6%), colon or rectum (12.4%), head or neck (12.1%), lymph nodes (10.9%), breast (7.6%), gynecologic organs (7.1%), genitourinary organs (4.2%), esophagus (3.6%), skin (melanoma) (3.5%), pancreas (2.5%), bone or soft tissue (2.2%), and other sites (5.4%). Seventy-seven (4.0%) of the 1,912 patients had 2 or 3 known primary malignancies before the PET/CT examination. Only the results of the first scan for each patient were included in the analysis. For patients who had more than 1 scan, only their first scan was assessed for additional primary lesions, not the subsequent scans.
PET/CT Imaging
Whole-body 18F-FDG PET/CT (Discovery LS; General Electric Medical Systems) was performed. The Discovery LS allows simultaneous acquisition of 35 transaxial images with a slice thickness of 4.25 mm per bed position for the PET images. Typically, 6 or more bed positions are used for a whole-body study. Axial and transaxial image resolution is approximately 4.5 mm in full width at half maximum. The field of view and pixel size of the reconstructed PET images are 50 cm and 3.91 mm, respectively. This imaging device also allows multi-detector-row helical CT. After fasting for at least 4 h, adult patients received an intravenous injection of 8.14 MBq/kg (0.22 mCi/kg) of 18F-FDG. About 50 min later, CT images were acquired, typically from the external auditory meatus to the mid thigh for 37 s without the use of intravenous contrast medium during tidal respiration. The technical parameters for the CT portion of the examination were as follows: a detector-row configuration of 4 × 5 mm, a pitch of 6:1 (high-speed mode), a gantry rotation time of 0.8 s, a table speed of 30 mm per gantry rotation, 140 kVp, and 40–120 mA (depending on body weight). A whole-body emission PET scan for the same length of coverage was obtained 60 min after intravenous administration of 18F-FDG, with a 5-min acquisition per bed position. Attenuation-corrected PET images were reconstructed with an iterative reconstruction ordered-subset expectation maximization algorithm. The 5-mm-thick transaxial CT images were reconstructed at 4.25-mm intervals (transaxial) for fusion with the transaxial PET images. CT, PET, and fused PET/CT images (transaxial, coronal, and sagittal) were then generated on a computer workstation.
Data Analysis
All reports from clinical whole-body 18F-FDG PET/CT scans were reviewed, and the patients who had reports indicating the presence of unexpected increased 18F-FDG uptake suggestive of an additional primary malignant lesion were identified. The clinical reports were originally generated after review by a nuclear medicine attending physician and a PET/CT fellow or a resident physician, generally with a CT radiologist reviewing the CT scan as well. A suspected additional primary lesion was defined as a lesion that was newly discovered on PET/CT, was specifically reported as being suggestive of a new primary malignant tumor, and had not previously been detected by other modalities. The clinical judgment about an additional primary lesion was made by the interpreting physicians, who generally considered the lesion to be a new primary if it was in a location atypical of a metastasis from the known primary or if it was of a size atypical of a metastasis from the known primary.
All unexpected additional primary malignancies were hypermetabolic on PET, and none of the unexpected lesions were detected on review of the CT scan alone. For all such cases, the final diagnosis was obtained from the medical records, including pathologic reports by biopsy or operation. A suspected additional primary lesion was classified as true positive if it was pathologically proven to be malignant and as false positive if it was pathologically proven to be benign or was considered benign by clinical follow-up.
This retrospective study was submitted to the Institutional Review Board and was approved with waiver of informed consent of patients.
RESULTS
PET-positive lesions suggestive of new primary malignant tumors were found in 79 (4.1%) of 1,912 patients (Table 1). In 22 (1.2%) of 1,912 patients, 24 of these lesions were pathologically proven to be malignant (Table 2). The proven sites of the malignant primary lesion were lung (7 lesions), thyroid (6 lesions), colon (4 lesions), breast (2 lesions), esophagus (2 lesions), bile duct (1 lesion), and head and neck other than thyroid (1 lesion). In 1 patient who had Merkel cell carcinoma in the groin and renal cell carcinoma in the kidney before the PET/CT scan, 3 new 18F-FDG-avid lesions, comprising 2 noncontiguous lesions in the lung and 1 lesion in the thyroid, were proven malignant (poorly differentiated adenocarcinoma in the lung and papillary carcinoma in the thyroid). In 20 of the 22 patients, the histology and immunohistochemistry showed that the new lesions were clearly a different primary malignancy but not metastases from the known primary lesion (Table 2). In 1 patient with known bile duct cancer, CT showed the new lesion to be a spiculated lung nodule highly suggestive of primary lung cancer, although both lesions were proven adenocarcinoma. In 17 of the 22 patients, the treatment plan was changed after the PET/CT examination and an operation was performed to diagnose or treat the new lesion. In 10 of 79 patients, PET was proven falsely positive after pathologic assessment. False-positive sites included thyroid (5 patients with adenomatoid nodules), uterus (2 patients with normal epithelium), head and neck other than thyroid (2 patients with reactive lymph node or lymphoid hyperplasia), and lung (1 patient with benign respiratory epithelium). In 8 other patients, the PET-positive lesions were considered benign after clinical follow-up (8–23 mo; median, 15 mo). Thus, PET/CT was falsely positive for at least 18 (23%) of 79 patients with PET/CT findings suggesting the presence of an unexpected additional primary lesion. In 39 patients, follow-up clinical information or records were not yet available and the final diagnosis of the detected lesion has not yet been resolved. Of 77 of 1,912 patients who had 2 or 3 primary malignant tumors before the PET/CT examination, 7 patients had a suspected additional primary tumor on PET/CT. Among them, 1 patient had true-positive lesions confirmed by pathology, 4 patients had false-positive lesions confirmed by pathology, and the final diagnosis was not yet confirmed in 2 patients (Table 1). Representative cases are shown in Figures 1 and 2.
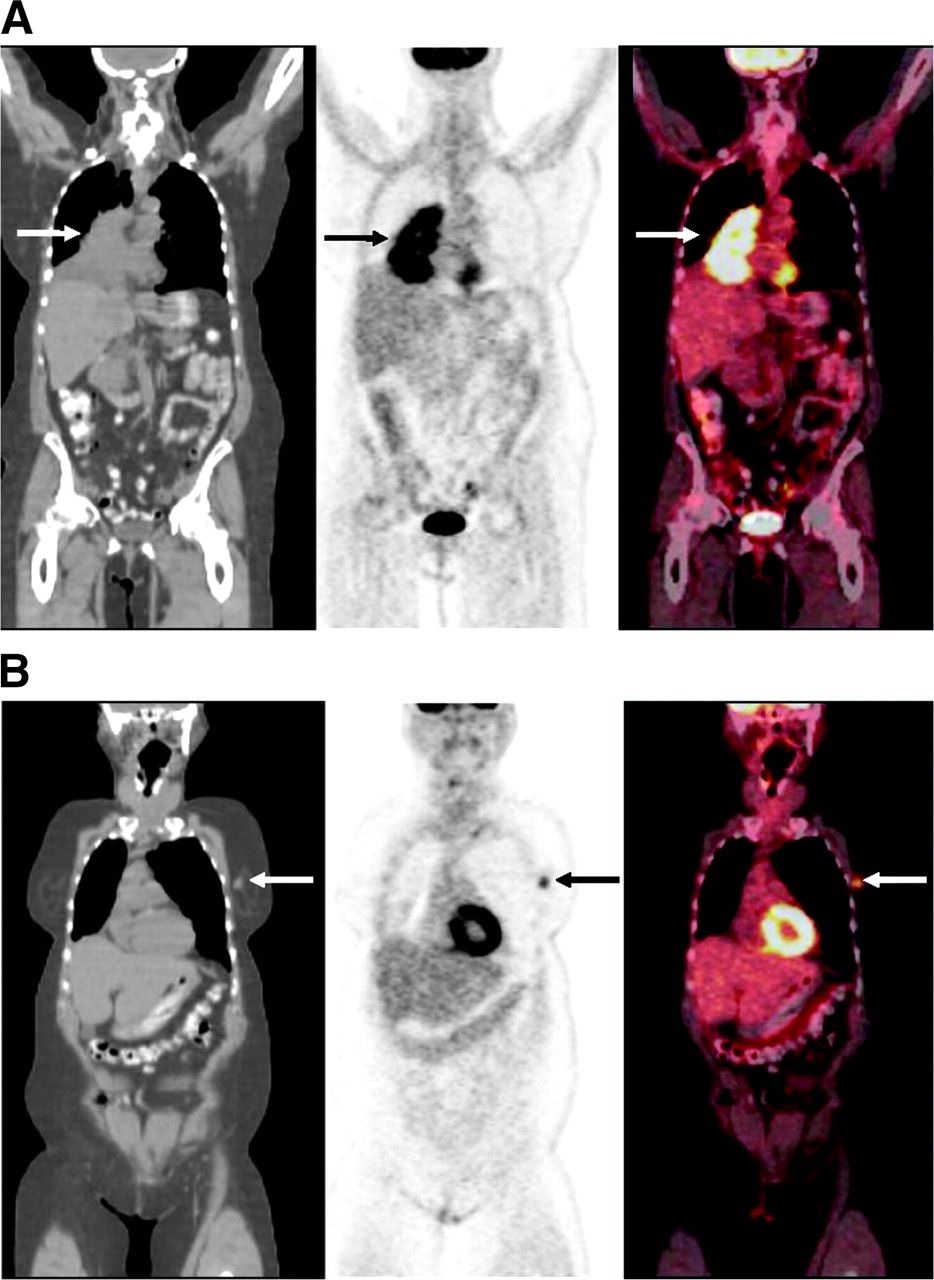
Coronal PET/CT images of 73-y-old woman with recently diagnosed cancer in right lung. (A) Images show large 18F-FDG-avid mass in right lung (arrow), consistent with patient’s known lung cancer. Biopsy revealed small cell lung cancer. (B) Anterior slices from same PET/CT study showed 18F-FDG-avid nodule in left breast (arrow), highly suggestive of malignancy. Pathology revealed infiltrating ductal carcinoma. Thus, this case was true-positive for an additional primary malignancy.

Coronal PET/CT images of 73-y-old woman with non-small cell right-upper-lobe lung cancer recently diagnosed by biopsy. (A) Lung mass shows intensely increased metabolic activity, compatible with the known lung cancer (arrow). (B) Additional slices from same PET/CT study showed increased activity in a right thyroid nodule (arrow). Fine-needle aspiration biopsy showed benign adenomatoid nodule. This case was thus falsely positive for an additional primary. Mildly increased activity seen in right axilla (arrowhead) was likely due to minimal tracer infiltration after right antecubital injection of tracer.
Summary of Results
Pathology-Proven Cases
DISCUSSION
Detection of unanticipated malignant lesions has a significant clinical impact not only on healthy individuals but also on patients with known malignant disease. In patients with known cancer, work-ups often focus on the patient’s primary disease, and incidental coexistence of another primary malignant lesion can be missed. The prevalence of additional primary neoplasms is substantial. Dong et al. reported that 8.5% of 633,964 patients with known cancers were subsequently proven to have other and previously unrecognized types of primary cancer (12). Ueno et al. reported that 5.2% of 24,498 cancer patients had multiple cancers (13). Some cancers tend to cluster because of shared risk factors, for example, smoking in cancers of the lung and of the head and neck, dietary or endocrine factors in gynecologic cancers, ultraviolet light in melanoma and skin cancer, and viral agents in cervical and anogenital cancers. Subsequent additional primary malignancies may also be associated with a potentially carcinogenic treatment of the initial cancer, such as chemotherapy, radiation therapy, or both. Further, genetic risk factors such as BRCA1 or BRCA2 mutations have been shown to predispose to multiple cancers such as breast and ovarian cancers (14).
Whole-body 18F-FDG PET can be used to survey the entire body. Yasuda et al. evaluated 18F-FDG PET for cancer screening of asymptomatic individuals (5). Malignant tumors were detected in 1.1% of participants by PET, and most of the tumors were reported to be at early curative stages. Shen et al. reported that 18F-FDG PET detected malignant lesions in 1.2% of 1,283 asymptomatic individuals (6). Despite the relatively high cost, 18F-FDG PET could be used as a screening modality for detecting asymptomatic malignancies at an early stage. Agress and Cooper recently reported the rate of detection of unexpected malignant lesions in patients with known or suspected malignancies to be at least 1.7% using whole-body 18F-FDG PET (8).
In the interpretation of 18F-FDG PET images, correlation with anatomic imaging is important not only because it can clarify the precise location of an 18F-FDG-avid focus but also because it can reduce the probability of a false-positive or false-negative result. Physiologic 18F-FDG accumulation can, in some instances, be interpreted as abnormal, which could cause unnecessary biopsy, surgery, or other therapy. Among the false-positive cases in the present study, despite PET/CT it was not possible to differentiate physiologic 18F-FDG uptake, transient inflammatory processes, and benign neoplasm from tumor. However, coregistered PET/CT might have minimized the frequency of biopsy of false-positive lesions due to physiologic 18F-FDG uptake, because biopsy of benign 18F-FDG-avid neoplasms was more common in the present study.
In the present study, the prevalence of pathology-proven additional primary malignancy on PET/CT was 1.2%, which was comparable to the results previously reported for PET alone. Because the follow-up record was not yet available and the final histologic diagnosis of the detected lesion was not resolved for 37 patients, the prevalence of additional primary malignant tumor may, in fact, be higher than the 1.2% rate we observed on PET/CT. However, even without follow-up data on those patients, the prevalence of additional primary tumor was almost the same as that of malignant tumors detected by 18F-FDG PET in asymptomatic individuals. It is clearly important to be alert to the possibility of additional primary malignant lesions on 18F-FDG PET or PET/CT, as they not uncommonly represent cancer. Histopathologic assessment of 18F-FDG-avid lesions is obviously warranted, and one of the major advantages of PET/CT is in providing a guide for tissue sampling.
Metastases of the known malignancy can also have an unusual pattern of distribution, and separating an additional primary malignancy from an unusual metastasis can be challenging. Our inclusion criteria and the definition of an additional primary lesion depended on PET/CT reports that were based on all data available to the interpreting physician. In the present study, among the 40 patients whose lesions on PET/CT were confirmed by pathology or clinical follow-up, none of the suspected lesions were metastases. However, metastases might have been present among the suspected lesions of the 39 patients whose follow-up information was not available. On the basis of our pathology-proven group, metastases are not likely to be a frequent cause of suspected additional primary lesions in the non-biopsy-proven group.
A limitation of the present study was the lack of follow-up data for many patients. The results for these patients would probably increase the prevalence of additional malignancy but might also increase the false-positive rate. Most of these patients were referred from an outside hospital for only the PET/CT scan. Because of the specific regulations of the institutional review board for the present retrospective study, we were allowed to collect the existing data records but not to contact the referring physician or patients.
False-positive PET/CT findings can cause patients to undergo additional invasive examinations. Among the cases of false-positive findings in the present study, 10 patients underwent an additional invasive examination to obtain pathologic proof of the unexpected additional lesion detected on PET/CT, and the lesion was found to be benign. If too many false positives require further aggressive examination, the potential risk or harm will surpass the possible benefit of PET/CT. However, we believe that the benefit for the 22 patients with true-positive findings in this study justifies further work-up of lesions identified with PET/CT.
Our study was limited to the evaluation of abnormalities positive at 18F-FDG PET/CT and did not provide information on false-negative malignancies. Thus, a verification bias was present. Some malignancies that were small, had modest 18F-FDG uptake, or were in organs with high physiologic 18F-FDG uptake such as kidney or brain could clearly have been missed. Further, the retrospective nature of our study did not permit determination of the independent roles of the PET and CT components of the PET/CT study. A prospective, separate comparison of the 18F-FDG PET, CT, and PET/CT images would clearly be useful to address their relative contributions to the examination.
CONCLUSION
PET/CT identified a significant number (at least 1.2%) of additional 18F-FDG-avid primary cancers on the PET/CT study of patients with known cancer. PET/CT was falsely positive in at least 0.9% of patients. Clearly, aggressive work-up of such identified lesions is essential, as patient management is frequently altered by such information. Although false positives can occur, the true-positive prevalence is substantial. Such newly identified lesions are often of early stage and thus have an excellent likelihood of being cured if treated promptly and aggressively.
Footnotes
Received Jul. 7, 2004; revision accepted Jan. 5, 2005.
For correspondence or reprints contact: Richard L. Wahl, MD, Division of Nuclear Medicine, Department of Radiology, Johns Hopkins Medical Institutions, 601 N. Caroline St., Room 3223A, Baltimore, MD 21287.
E-mail: rwahl{at}jhmi.edu
REFERENCES
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Detection of Additional Primary Neoplasms on 18F-Fluciclovine PET/CT in Patients with Primary Prostate Cancer
- Multiple primary tumours: challenges and approaches, a review
- Assessment of incidental and clinically unsuspected fluorodeoxyglucose-avid foci detected on oncological positron emission tomography/CT
- The role of the breast radiologist in evaluation of breast incidentalomas detected on 18-fludeoxyglucose positron emission tomography/CT
- Incidental findings on positron emission tomography/CT scans performed in the investigation of lung cancer
- Significance of incidental focal uptake in prostate on 18-fluoro-2-deoxyglucose positron emission tomography CT images
- Incidental findings in imaging diagnostic tests: a systematic review
- Comparison of Whole-Body PET/CT, Dedicated High-Resolution Head and Neck PET/CT, and Contrast-Enhanced CT in Preoperative Staging of Clinically M0 Squamous Cell Carcinoma of the Head and Neck
- Prospective Evaluation of Whole-Body Cancer Screening With Multiple Modalities Including [18F]Fluorodeoxyglucose Positron Emission Tomography in a Healthy Population: A Preliminary Report
- Incidental Detection of Concurrent Extramedullary Plasmacytoma and Amyloidoma of the Nasopharynx on [18F]Fluorodeoxyglucose Positron Emission Tomography/Computed Tomography
- Detection of extrapulmonary lesions with integrated PET/CT in the staging of lung cancer
- Role of Nuclear Medicine in the Management of Cutaneous Malignant Melanoma
- Focal Thyroid Lesions Incidentally Identified by Integrated 18F-FDG PET/CT: Clinical Significance and Improved Characterization