


Abstract
In this retrospective study, we investigated whether the 18F-FDG uptake pattern and CT findings improved the accuracy over the standardized uptake value (SUV) for differentiating benign from malignant focal thyroid lesions incidentally found on 18F-FDG PET/CT. We also defined the prevalence of these lesions and their risk for cancer. Methods: 18F-FDG PET/CT was performed on 1,763 subjects without a previous history of thyroid cancer from May 2003 to June 2004. Two nuclear medicine physicians and 1 radiologist interpreted PET/CT images, concentrating on the presence of focal thyroid lesions, the maximum SUV of the thyroid lesion, the pattern of background thyroid 18F-FDG uptake, and the CT attenuation pattern of the thyroid lesion. Results: The prevalence of focal thyroid lesions on PET/CT was 4.0% (70/1,763). Diagnostic confirmation was done on 44 subjects by ultrasonography (US)-guided fine-needle aspiration (n = 29) or US with clinical follow-up (n = 15). Among 49 focal thyroid lesions in these 44 subjects, 18 focal thyroid lesions of 17 subjects were histologically proven to be malignant (papillary cancer in 16, metastasis from esophageal cancer in 1, non–Hodgkin's lymphoma in 1). Therefore, the cancer risk of focal thyroid lesions was 36.7% on a lesion-by-lesion basis or 38.6% on a subject-by-subject basis. The maximum SUV of malignant thyroid lesions was significantly higher than that of benign lesions (6.7 ± 5.5 vs. 10.7 ± 7.8; P < 0.05). When only the maximum SUV was applied to differentiate benign from malignant focal thyroid lesions for the receiver-operating-characteristic curve analysis, the area under the curve (AUC) of PET was 0.701. All 16 focal thyroid lesions with very low attenuation or nonlocalization on CT images, or with accompanying diffusely increased thyroid 18F-FDG uptake, were benign. When those lesions were regarded as benign lesions, irrespective of the maximum SUV, the AUC of PET/CT was significantly improved to 0.878 (P < 0.01). Conclusion: Focal thyroid lesions incidentally found on 18F-FDG PET/CT have a high risk of thyroid malignancy. Image interpretation that includes 18F-FDG uptake and the CT attenuation pattern, along with the SUV, significantly improves the accuracy of PET/CT for differentiating benign from malignant focal thyroid lesions.
Thyroid incidentalomas are defined as newly identified focal thyroid lesions encountered during imaging study, such as CT and MRI, to evaluate nonthyroid disease. The clinically relevant issue is whether thyroid incidentalomas are benign or malignant. High-resolution ultrasonography (US) studies report a prevalence of thyroid nodules ranging from 19% to 46% in the general population, and the risk of cancer in these thyroid nodules is very low, ranging from 1.5% to 10% (1). Moreover, none of these modalities (US, CT, MRI) is specific for thyroid malignancy (2–4).
PET using 18F-FDG is a noninvasive whole-body imaging technique used to evaluate various kinds of malignancies, including thyroid cancer, that show increased glucose use compared with normal tissues (5,6). Several retrospective studies have reported that thyroid incidentalomas with focal increased 18F-FDG uptake were found in 1.2%–4.3% of patients or healthy subjects on PET examinations (7–10). The risk of malignancy ranged from 14% to 47% in those studies. Although there was a significant difference in standardized uptake values (SUVs) between benign and malignant thyroid lesions, it is still difficult to differentiate benign from malignant thyroid incidentalomas by SUV alone in any individual case because of significant overlap between benign and malignant lesions (5–10).
The recently developed integrated PET/CT system makes it possible to fuse anatomic images with functional images through the equipment, which results in better anatomic localization and an improvement of diagnostic accuracy when using the PET/CT fusion image (11,12). Although CT does not help in differentiating benign from malignant thyroid nodules, there are several findings favoring a benign lesion, such as a cystic nodule or multiple nodules (2–4). One recent study reported the evaluation of thyroid incidentalomas using integrated PET/CT (10). However, due to a small number of subjects, the CT data were not used, in addition to PET data, to characterize the focal thyroid lesions. It was also suggested that diffusely increased 18F-FDG uptake in the thyroid gland favored benign conditions such as chronic thyroiditis or Graves' disease (8,13,14). Therefore, in this study, we performed a retrospective review of our institutional experience with incidentally found focal thyroid lesions on 18F-FDG PET/CT in healthy subjects who appeared for voluntary cancer screening as well as in patients with suspected or known cancer. In addition to the SUV analysis, we also investigated whether noncontrast CT findings and the 18F-FDG uptake pattern of the thyroid gland were helpful in characterizing focal thyroid lesions.
MATERIALS AND METHODS
Subjects
From May 2003 to June 2004, 1,782 consecutive subjects (mean age, 55.7 ± 12.3 y) underwent 18F-FDG PET/CT in our institution. Among them, 19 subjects with known thyroid cancer or a previous history of thyroid surgery were excluded from the study population. The final study population was 1,763 subjects, including patients with a known history of chronic thyroiditis (n = 3) or Graves' disease (n = 2). Among them, PET/CT was performed on 196 healthy subjects (mean age, 51.9 ± 9.2 y) without a previous history of cancer who underwent voluntary cancer screening and 1,567 patients (mean age, 56.2 ± 12.5 y) with suspected or known nonthyroidal cancer. When a focal thyroid lesion was incidentally found on PET/CT, we usually recommended high-resolution thyroid US examination irrespective of the SUV on the initial official interpretation of PET/CT images. The ethics committee of our institution reviewed and approved the study protocol.
18F-FDG PET/CT
All subjects fasted for at least 6 h before the PET study. PET/CT scanning was performed using a Discovery LS PET/CT scanner (GE Healthcare). Whole-body CT was performed by a continuous spiral technique using an 8-slice helical CT with a gantry rotation speed of 0.8 s. The CT scan data were collected with 40–120 mAs adjusted to the patient's body weight, 140 keV, a section width of 5 mm, and a table feed of 5 mm per rotation. No intravenous or oral contrast material was used. After the CT scan, an emission scan was obtained from thigh to head for 5 min per frame, 45 min after the intravenous injection of 370 MBq 18F-FDG. Attenuation-corrected PET images using CT data were reconstructed by an ordered-subsets expectation maximization algorithm (28 subsets, 2 iterations). Commercial software (eNTEGRA; Elgems) was used to accurately coregister the separate CT and PET scan data.
Image Analysis
The SUVs were acquired using the attenuation-corrected images, the amount of injected 18F-FDG, the body weight of each patient, and the cross-calibration factors between the PET and the dose calibrator. The PET image, the noncontrast CT image, and the fused PET/CT image were reviewed retrospectively by 2 nuclear medicine physicians and 1 radiologist at the same time. All image interpretations were performed by these reviewers, who were unaware of the results of the other imaging examinations and the final pathologic results. Image interpretation concentrated on the presence of focal thyroid lesions on CT or PET images, the maximum SUV of the focal thyroid lesions, the presence of diffusely increased thyroid 18F-FDG uptake surrounding a focal thyroid lesion, the attenuation of a focal thyroid lesion on CT images, the presence of calcification within a focal thyroid lesion on the CT images, and the presence of abnormal cervical lymph nodes on PET/CT images.
In this study, a focal thyroid lesion was defined as focally increased 18F-FDG uptake on PET images or a discernible focal lesion on CT images without occupying the whole thyroid gland, whereas diffuse uptake was defined as 18F-FDG uptake in the whole thyroid gland. We did not evaluate the histology of thyroid glands that demonstrated only diffuse 18F-FDG uptake, because previous reports have indicated that the majority of these represent benign conditions, such as chronic thyroiditis or Graves' disease, and generally do not need histologic diagnosis (8,13,14). However, focally increased 18F-FDG thyroid uptake accompanying diffuse thyroid uptake was considered a focal thyroid lesion deserving of further evaluation; these were included in this study. A focal thyroid nodule on a CT image with mild 18F-FDG uptake similar to that of the normal thyroid gland was also regarded as a focal thyroid lesion in this study. Patterns of a focal thyroid lesion on PET/CT images were classified according to their attenuation on CT images: no discernible lesion on CT images with focally increased 18F-FDG uptake; a higher attenuation lesion than that of normal thyroid tissue; attenuation similar to that of normal thyroid; lower attenuation than that of normal thyroid; and much lower attenuation than that of normal thyroid (mean attenuation value of a 5 × 5 pixel rectangular region of interest located in a center of the lesion < 25 Hounsfield units).
High-Resolution Thyroid US and US-Guided Fine-Needle Aspiration (FNA)
High-resolution thyroid US examination was performed by radiologists, who were informed of the PET/CT findings before US, using a 10-MHz linear array transducer (Philips Electronics). They located focal thyroid lesions described in a PET/CT report and evaluated them for the presence of a thyroid nodule and for size (in longest diameter), internal content, echogenicity, halo, margin, and intralesional calcification of the thyroid nodule (15–17). FNA was performed using a 21-gauge needle on a 10-mL syringe under US guidance. US guidance was used to confirm the placement of the needle in the focal thyroid lesion detected on a PET/CT scan. Aspiration was done twice for each nodule. Specimens were smeared on glass slides, air dried, and stained using the Papanicolaou method. In our institution, when no nodule coinciding with a focal thyroid lesion on a PET/CT scan was found, or the nodule was <1.5 cm in diameter and had features typical of a remote probability for malignancy (<2%; US index points, ≤1), FNA was not done (17). The subject was clinically monitored, consistent with a strategy based on our previous large retrospective study, and on other reports (15–17).
Statistical Analysis
The Mann–Whitney U test and χ2 test were used to compare PET/CT findings between benign and malignant thyroid lesions. A receiver-operating-characteristic (ROC) curve analysis was done to measure and compare the accuracy of PET/CT parameters to differentiate benign from malignant thyroid lesions. The diagnostic accuracies of various PET/CT parameters were expressed as the area under the corresponding ROC curve (AUC). An Apple Macintosh version (January 1991) of a ROC analysis software as described by Charles E. Metz (Department of Radiology, University of Chicago) was used for this data analysis (18). A modified nonpaired t test was used to determine if there were statistically significant differences between the AUCs (18). P values < 0.05 were considered to indicate a statistically significant difference. Numeric data were expressed as mean ± SD.
RESULTS
Of the 1,763 subjects (1,164 men, 599 women) 70 (4.0%) had incidentally found focal thyroid lesions on PET/CT scans. No history of thyroid disease was found in these 70 subjects at the time of PET scanning. Among them, 17 subjects had focal thyroid nodules on CT images with mild 18F-FDG uptake similar to that of normal thyroid. These nodules were not identified when we reviewed the PET images alone. In another 13 subjects, it was difficult to differentiate focally increased thyroid uptake from cervical lymph node uptake when reviewing PET images alone. Therefore, PET/CT images provided us with additional information from PET images alone regarding the presence of focal thyroid lesions, or of anatomic localization, in 42.9% (30/70) of the subjects. The prevalence of a focal thyroid lesion on PET/CT in patients with suspected or known cancer (65/1,567; 4.1%) was higher than that in healthy subjects (5/196; 2.6%), but no statistical difference was found (P > 0.05).
Among 70 subjects with incidentally found focal thyroid lesions on PET/CT scans, further evaluation was not performed on 25 subjects because of refusal of additional work-up, loss of clinical follow-up, or extensive stage IV disease of another underlying primary malignancy. Of these 25 subjects, 10 had a thyroid nodule on CT with mild 18F-FDG uptake similar to that of normal thyroid gland. Further examination with thyroid US was undertaken in the remaining 45 subjects with focal thyroid lesions. One subject underwent US FNA for a focal thyroid lesion with indeterminate finding for malignancy on US; however, the aspirated specimen was inadequate for diagnosis, and further diagnostic confirmation was not done. Thus, this patient was excluded from further analysis.
Finally, 49 focal thyroid lesions from the 44 subjects (male-to-female ratio, 19:25; mean age, 55.7 ± 10.1 y; 40 patients with alleged malignancy, 4 healthy subjects) who underwent further diagnostic confirmation were included in the analysis. Histologic confirmation was obtained in 34 thyroid lesions from the 29 subjects (by FNA in 19, by FNA and surgery in 10). Among them, 18 focal thyroid lesions from the 17 patients with alleged malignancy were histologically proven to be malignant (papillary carcinoma in 16, metastatic squamous cell carcinoma from the esophagus in 1, non–Hodgkin's lymphoma in 1). The remaining 16 thyroid lesions from the 12 subjects were histologically proven to be benign (nodular hyperplasia in 10, chronic thyroiditis in 3, follicular adenoma in 1, follicular adenoma with background chronic thyroiditis in 1, Hürthle cell adenoma in 1). In 2 subjects with follicular adenoma, the final diagnosis was determined by surgery, because the pathologic findings of FNA showed a follicular neoplasm indeterminate for malignancy.
The remaining 15 lesions from 15 subjects had typical features of a benign lesion with a rare probability for malignancy (<2%) or had no focal thyroid lesions on thyroid US corresponding to the focal 18F-FDG uptake; these patients were clinically monitored without FNA (15–17). During a mean follow-up of 14.5 ± 5.2 mo, there was no clinical or radiologic evidence of thyroid malignancy in any of these 15 subjects.
Therefore, the cancer risk of focal thyroid lesions on PET/CT was 36.7% (18/49) on a lesion-by-lesion basis or 38.6% (17/44) on a subject-by-subject basis. One of 6 focal thyroid lesions in the 6 subjects with mild 18F-FDG uptake similar to that of normal thyroid gland was proven to be malignant (papillary carcinoma). Another 4 subjects had multifocal thyroid lesions. The final pathologic diagnoses were chronic thyroiditis in 1 subject, nodular hyperplasia in 1 subject, papillary carcinoma with nodular hyperplasia in 1 subject, and multifocal papillary carcinoma in the remaining subject.
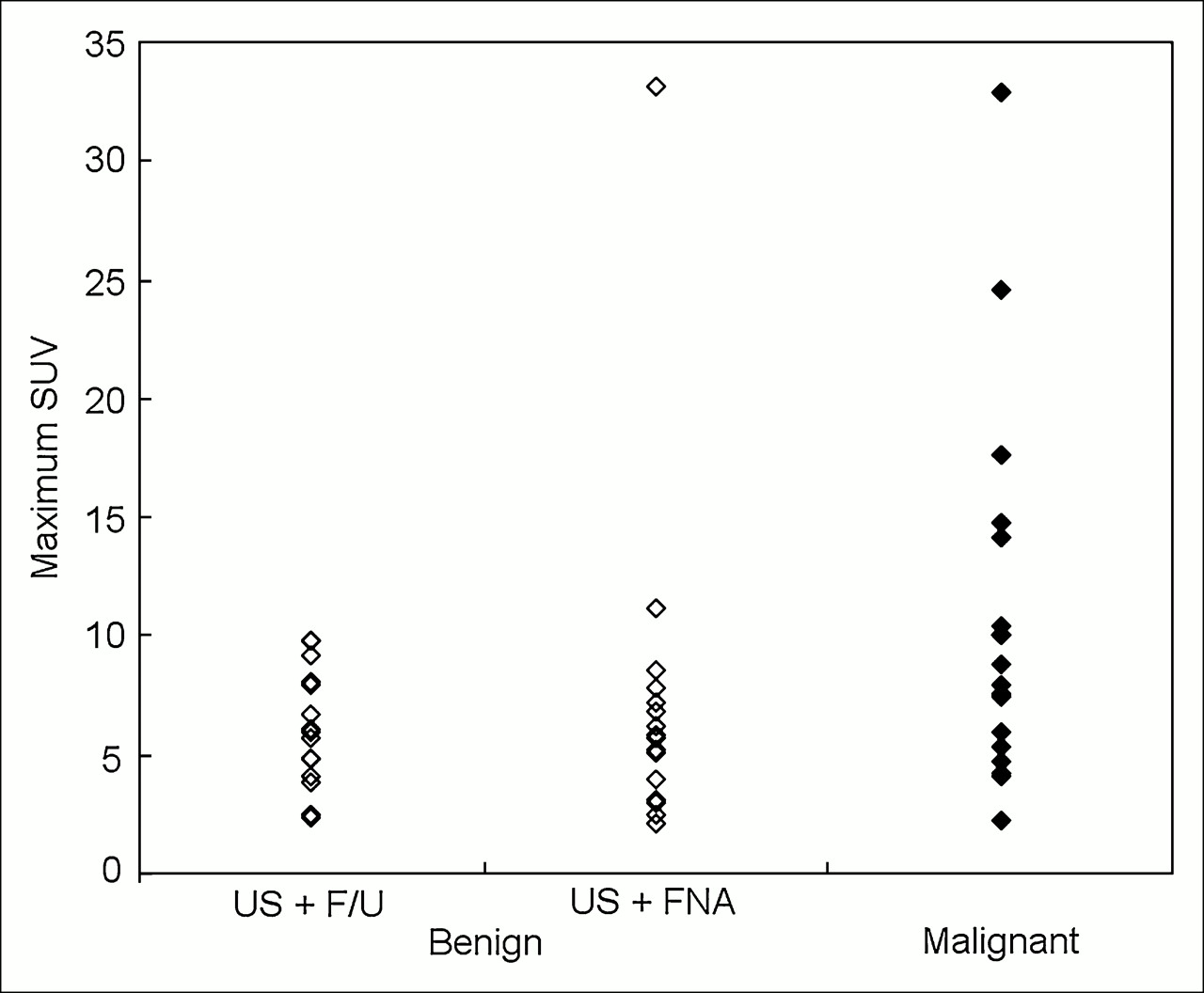
Table 1 shows the comparisons of PET/CT findings between benign and malignant focal thyroid lesions incidentally detected on PET/CT. The maximum SUV of malignant thyroid lesions was significantly higher than that of benign lesions (Fig. 1). Most of the malignant thyroid lesions (88.9%; 16/18) had low attenuation on CT. All focal thyroid lesions with a diffuse increase in surrounding thyroid uptake, or very low attenuation on CT, were benign (Figs. 2 and 3). Focally increased 18F-FDG uptake in the thyroid without a corresponding discernible focal anatomic lesion on CT also indicated a benign lesion with 100% certainty. All 5 subjects with focal thyroid lesions and diffusely increased thyroid uptake (1 subject had 3 focal thyroid lesions) were in euthyroid status by in vitro thyroid function tests, and they had no symptoms suggesting functional thyroid disease. Although thyroid autoantibodies in blood were not measured in these 5 subjects, 3 of them were suggested to have chronic thyroiditis on pathologic examination (n = 2) or US (n = 1).

Maximum SUV of benign and malignant focal thyroid lesions incidentally found on 18F-FDG PET/CT and undergoing further diagnostic confirmation. F/U = clinical follow-up.

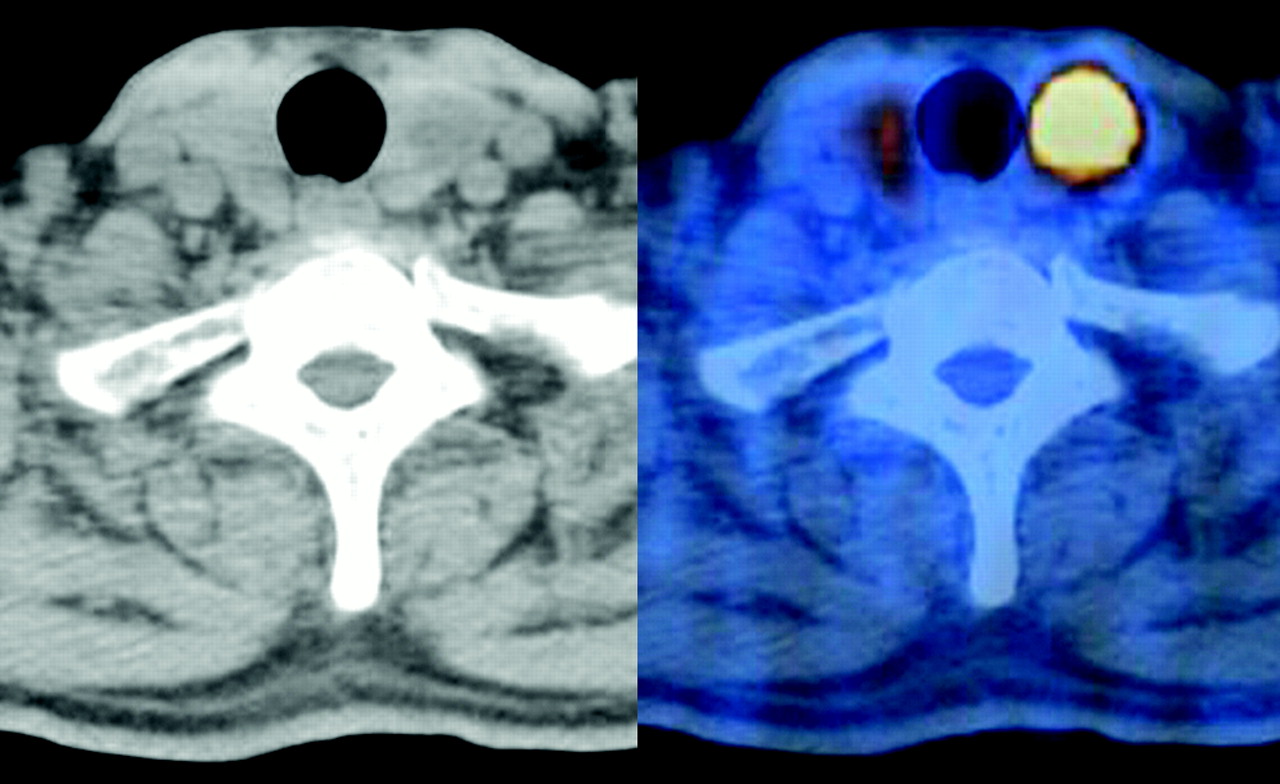
CT (left) and fused PET/CT (right) images of 65-y-old male patient with esophageal cancer showed abnormally high focal 18F-FDG uptake in left thyroid gland (maximum SUV = 33.1). CT attenuation of that lesion was very low (3.6 Hounsfield units), and surrounding thyroid gland had diffusely increased 18F-FDG uptake. Follicular adenoma with lymphocytic thyroiditis was confirmed after thyroidectomy.

CT (left) and fused PET/CT (right) images of 56-y-old female patient with non–small cell lung cancer showed abnormal focal 18F-FDG uptake in right thyroid gland (maximum SUV = 5.3). That lesion had low CT attenuation (76 Hounsfield units) without calcification, and 18F-FDG uptake of surrounding thyroid gland was not increased. Papillary carcinoma was confirmed histopathologically.
Comparisons of PET/CT Findings Between Benign and Malignant Focal Thyroid Lesions Incidentally Detected on 18F-FDG PET/CT and Undergoing Further Diagnostic Confirmation
There was no significant correlation between maximum SUV and size by US of focal thyroid lesions (r = 0.21; P = NS). When focal thyroid lesions were classified into 2 groups according to the size by US (<10 mm [n = 21] vs. ≥10 mm [n = 28]), no significant difference in maximum SUV between the 2 groups was found (7.11 ± 3.34 vs. 9.01 ± 8.26; P = NS).
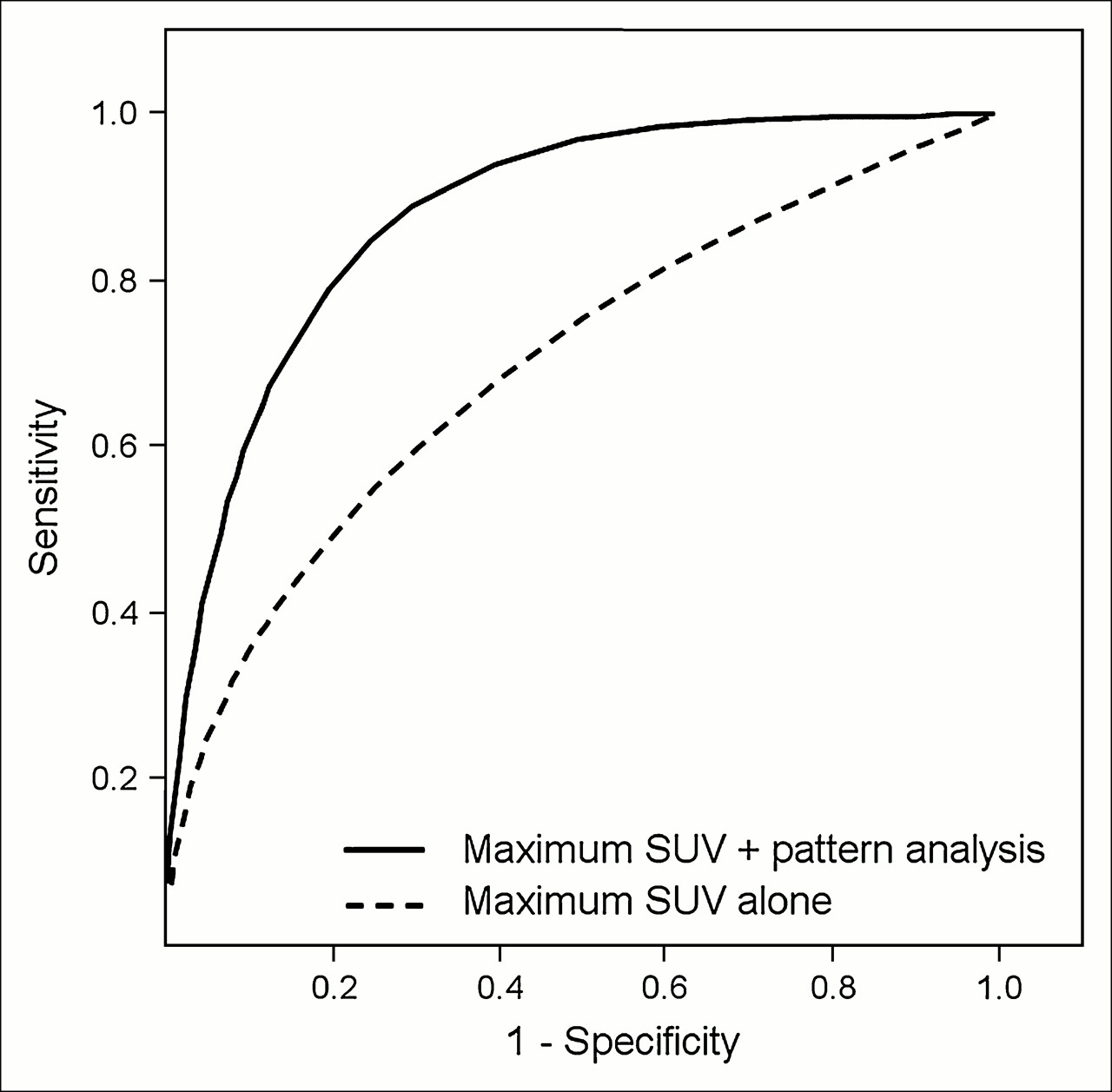
When only maximum SUV was used to differentiate benign from malignant focal thyroid lesions for the ROC curve analysis, the AUC of PET was 0.701 ± 0.079 (Fig. 4). When a focal thyroid lesion with very low attenuation or nonlocalization on CT images, or with accompanying diffusely increased thyroid 18F-FDG uptake, was regarded as a benign lesion irrespective of maximum SUV, the AUC of PET/CT was significantly improved to 0.878 ± 0.049 (P < 0.01; Fig. 4). Using these combined criteria, and the ROC curve analysis, the most likely point not to overlook a malignancy was the point at which the sensitivity was 89.9% and the specificity was 70.1%, with a cutoff maximum SUV of 4.2. When these 16 focal, benign thyroid lesions with very low attenuation or nonlocalization on CT images, or with accompanying diffusely increased thyroid 18F-FDG uptake, were excluded from the analysis, the risk of cancer in the focal thyroid lesions incidentally found by PET/CT was increased from 36.7% (18/49) to 54.5% (18/33).
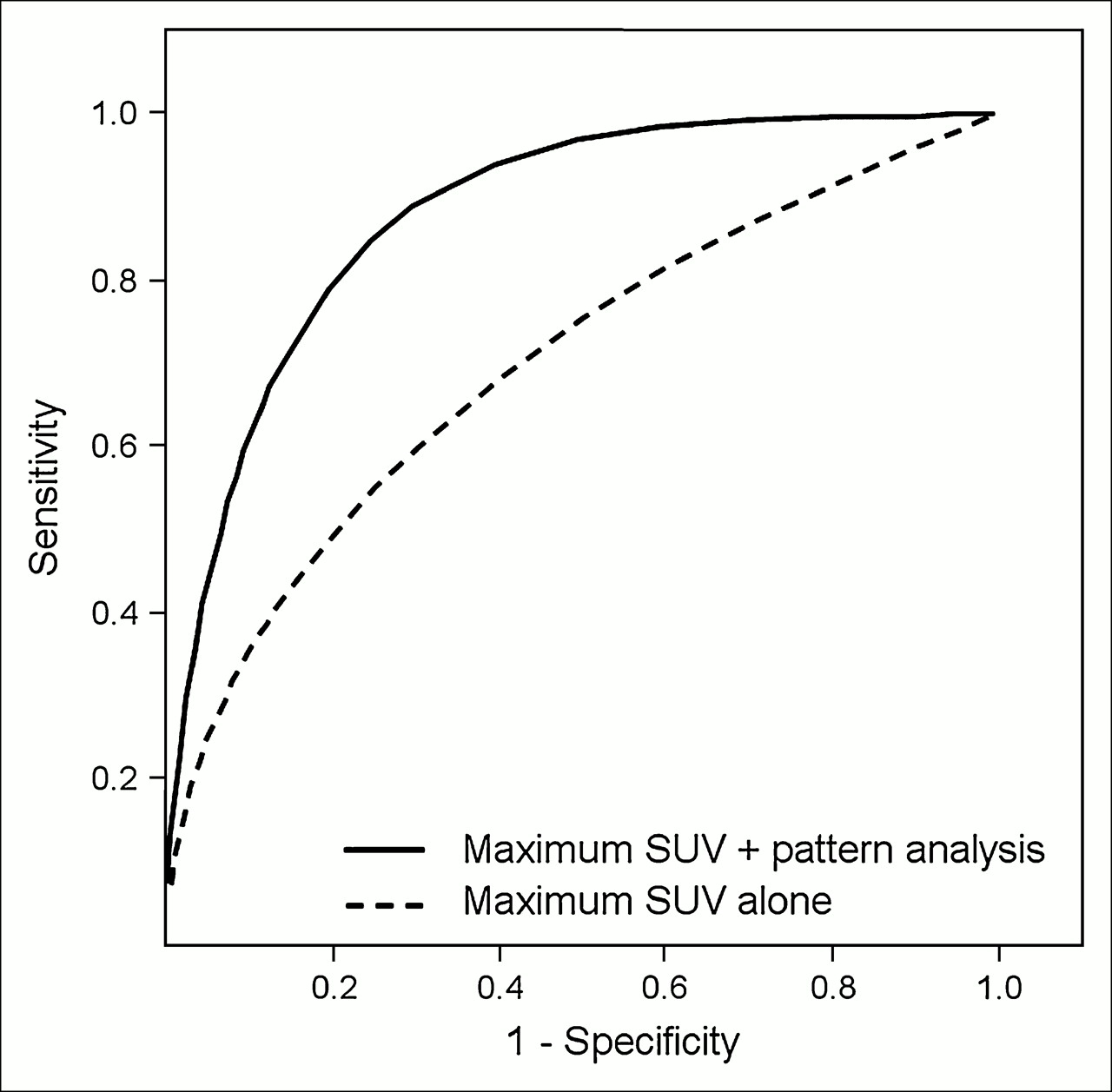
ROC curves of PET/CT when maximum SUV or maximum SUV with CT attenuation and 18F-FDG uptake pattern was applied for differentiation between benign and malignant focal thyroid lesions. The AUC of PET/CT was significantly increased when analysis of CT attenuation and 18F-FDG uptake pattern was added to maximum SUV (0.701 ± 0.079 vs. 0.878 ± 0.049; P < 0.01).
DISCUSSION
Because thyroid nodules are relatively common, it is important to identify which nodules are at risk for containing malignancy. This holds true, as well, for thyroid nodules found incidentally on examinations to evaluate other nonthyroidal disease. In our study, focal thyroid lesions incidentally identified by 18F-FDG PET/CT occurred with a prevalence of 4.0%, which is somewhat high in comparison with previous reports (7–10). The use of PET/CT may contribute to this high prevalence. When focally increased uptake is found in the anterior neck, it is sometimes difficult to determine whether the lesion corresponds to thyroid, lymph node, or other organs on the basis of PET images alone. In this study, PET/CT images provided us with further information, in addition to PET images alone, relating to the presence of focal thyroid lesions or anatomic localization in 43% of the subjects with focal thyroid lesions. A recent study using PET/CT in patients with non–small cell lung cancer also reported a relatively high prevalence of 4.3% with regard to focal thyroid 18F-FDG uptake, similar to our results (10).
The cancer risk of focal thyroid lesions found on 18F-FDG PET/CT was 37% on a subject-by-subject basis, similar to previous PET studies (7–10). This high risk of malignancy supports the performance of a further diagnostic procedure, such as US FNA, in subjects with focal thyroid lesions on PET/CT. Maximum SUVs of malignant focal thyroid lesions were significantly higher than those of benign lesions. However, it was difficult to differentiate benign from malignant focal thyroid lesions only by maximum SUV. Although focal thyroid lesions with a high SUV (>10.0) had a high likelihood of malignancy, thyroid lesions with a low-to-moderate SUV (≤10.0) did not always mean a high likelihood of a benign lesion (Fig. 1). Therefore, new criteria other than SUV are necessary to improve accuracy in characterizing focal thyroid lesions on PET. Our results indicate that the 18F-FDG uptake and CT attenuation pattern, in addition to the SUV analysis, are helpful in characterizing the focal thyroid lesion incidentally found on PET/CT. In other words, we found that accompanying diffusely increased 18F-FDG thyroid uptake, or very low attenuation, or no discernible thyroid nodule on CT favored benign thyroid lesions irrespective of the SUV. With these combined CT and PET criteria, the AUC of PET/CT for characterizing focal thyroid lesions was significantly improved from 0.701 to 0.878. This indicates that PET/CT is superior to conventional PET not only for identifying but also for characterizing focal thyroid lesions.
Diffusely increased 18F-FDG uptake in the thyroid gland favored benign conditions, such as chronic thyroiditis or Graves' disease (8,13,14). However, the clinical significance of a thyroid lesion with both focal and diffusely increased 18F-FDG thyroid uptake is not well known. In this study, all 5 subjects with such a pattern had no malignant thyroid tumors. This indicates that a diffuse-plus-focal 18F-FDG uptake pattern on PET might be associated with a benign condition, similar to a diffuse 18F-FDG uptake pattern. All focal thyroid lesions with very low attenuation or no discernible thyroid nodule on CT were benign in this study. Very low attenuation on CT indicates that the focal thyroid lesion had a cystic component, which favors benign histology in the thyroid gland (2–4).
A variable degree of 18F-FDG uptake in differentiated thyroid carcinoma has been reported (5–10). Although there are no previous reports that compare the degree of 18F-FDG uptake with glucose transporter expression directly, a variable degree of GLUT1 expression in differentiated thyroid carcinoma has been reported in several studies (19–21). This variable degree of GLUT1 expression in differentiated thyroid carcinoma may contribute to the variable degree of 18F-FDG uptake on PET in such patients. Many previous studies suggest that high 18F-FDG uptake and increased GLUT1 expression in differentiated thyroid carcinoma is associated with poor functional differentiation and an unfavorable prognosis (20,22). However, most of the previous studies dealt with recurrent or metastatic thyroid cancer after surgery. The prognostic significance of preoperative 18F-FDG PET in differentiated thyroid carcinoma deserves further investigation.
In this study, the prevalence of focal thyroid lesions on PET/CT appeared to be higher in patients with suspected or known cancer than in healthy subjects. Furthermore, all cases of ultimately proven thyroid malignancy occurred in patients with alleged cancer. A previous history of cancer is one of major risk factors for developing another kind of cancer (23). Patients with suspected or alleged cancer were older than the group of healthy subjects (mean age, 56.2 ± 12.5 y vs. 51.9 ± 9.2 y; P < 0.001). It is known that the prevalence of thyroid nodules and of thyroid cancer increases with age. These facts may contribute to the different prevalence of focal thyroid lesions and thyroid cancer between patients and healthy subjects.
The emergence of a second primary cancer is one of the important prognostic factors after treatment in patients with cancer (23). In this context, early diagnosis and treatment for the second primary cancer is important. In this study, PET/CT detected unexpected papillary thyroid carcinoma in 15 patients with alleged cancer. Most of them (13/15; 86.7%) had an early stage of thyroid cancer, ranging from stage I to stage III and showing a favorable prognosis of >80% 5-y survival (24). Recent studies suggest that PET/CT is useful in detecting unexpected second primary cancer or metastasis (25,26). Most of the second primary cancers (85.2%) detected on PET/CT were found to be early-stage disease (stage I or II), coinciding with our results (26). This suggests that early detection of the second primary cancers by PET/CT, including thyroid cancer, may have a favorable influence on the survival of such patients.
This study had several limitations. Retrospective design was one of the limitations. Because of this retrospective design, further evaluation was not done in about one third of the subjects who had focal thyroid lesions incidentally found on PET/CT. To minimize the radiation exposure of the subjects, low-dose, whole-body CT was used in this study, which is relatively inferior to conventional diagnostic high-dose CT in terms of CT image quality. Furthermore, one half of focal thyroid lesions on PET/CT had a size of <10 mm, which may result in a partial-volume effect on CT images. We cannot exclude the possibility that the use of low-dose CT might affect our results to characterize focal thyroid lesions. Another limitation was that a relatively small number of the subjects had focal thyroid lesions, although the number was larger than that in previous studies (5–9). In our institute, a further prospective study is under way with a larger number of subjects to validate these new combined CT and PET criteria for focal thyroid lesions.
CONCLUSION
Focal thyroid lesions incidentally found by 18F-FDG PET/CT indicate a high risk of thyroid malignancy that deserves further diagnostic confirmation. Image interpretation using the 18F-FDG uptake and CT attenuation pattern, along with the SUV, significantly improves the accuracy of PET/CT for differentiating benign from malignant focal thyroid lesions. Further diagnostic confirmation of focal thyroid lesions on PET/CT is mandatory, especially when those lesions have high focal 18F-FDG uptake (maximum SUV > 4.2) and low attenuation on CT (not cystic) without diffusely increased thyroid 18F-FDG uptake.
Acknowledgments
This study was supported by a grant from the Korea Health 21 R&D Project, Ministry of Health and Welfare, Republic of Korea (02-PJ3-PG6-EV06-0002).
References
- Received for publication August 11, 2005.
- Accepted for publication November 7, 2005.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Relationship Between FDG Uptake and the Platelet/lymphocyte Ratio in Patients With Breast Invasive Ductal Cancer
- Thyroid nodules: a clinical update for primary care
- Secondary thyroid malignancy from metastatic colon lymphoma
- Relationship Between FDG Uptake and Neutrophil/Lymphocyte Ratio in Patients with Invasive Ductal Breast Cancer
- Malignancy rate of focal thyroid incidentaloma detected by FDG PET-CT: results of a prospective cohort study
- Clinicopathological Features of Cases with Primary Breast Cancer not Identified by 18F-FDG-PET
- Assessment of incidental and clinically unsuspected fluorodeoxyglucose-avid foci detected on oncological positron emission tomography/CT
- Incidental findings on positron emission tomography/CT scans performed in the investigation of lung cancer
- Incidental Focal 18F-FDG Uptake in the Pituitary Gland: Clinical Significance and Differential Diagnostic Criteria
- Incidental thyroid "PETomas": clinical significance and novel description of the self-resolving variant of focal FDG-PET thyroid uptake
- The Role of 18F-Fluorodeoxyglucose Positron Emission Tomography in Thyroid Neoplasms
- Reply:
- Hybrid SPECT-CT and PET-CT imaging of differentiated thyroid carcinoma
- The Significance and Management of Incidental [18F]Fluorodeoxyglucose-Positron-Emission Tomography Uptake in the Thyroid Gland in Patients with Cancer
- Incidental thyroid nodule
- PET/CT assessment of clinically unsuspected, incidental FDG-avid lesions in oncological patients
- Management of the Solitary Thyroid Nodule
- Clinical Significance of Diffusely Increased 18F-FDG Uptake in the Thyroid Gland
- Clinical Role of 18F-FDG PET/CT in the Management of Squamous Cell Carcinoma of the Head and Neck and Thyroid Carcinoma