


Abstract
Osteomyelitis complicates up to one third of diabetic foot infections, is often due to direct contamination from a soft-tissue lesion, and represents a clinical challenge. Early diagnosis is important since antibiotic therapy can be curative and may prevent amputation. The present study assessed the role of PET/CT using 18F-FDG for the diagnosis of diabetic foot osteomyelitis. Methods: Fourteen diabetic patients (10 men and 4 women; age range, 29–70 y) with 18 clinically suspected sites of infection underwent PET/CT after the injection of 185–370 MBq of 18F-FDG for suspected osteomyelitis complicating diabetic foot disease. PET, CT, and hybrid images were independently evaluated for the diagnosis and localization of an infectious process. Additional data provided by PET/CT for localization of infection in the bone or soft tissues were recorded. The final diagnosis was based on histopathologic findings and bacteriologic assays obtained at surgery or at clinical and imaging follow-up. Results: PET detected 14 foci of increased 18F-FDG uptake suspected as infection in 10 patients. PET/CT correctly localized 8 foci in 4 patients to bone, indicating osteomyelitis. PET/CT correctly excluded osteomyelitis in 5 foci in 5 patients, with the abnormal 18F-FDG uptake limited to infected soft tissues only. One site of mildly increased focal 18F-FDG uptake was localized by PET/CT to diabetic osteoarthropathy changes demonstrated on CT. Four patients showed no abnormally increased 18F-FDG uptake and no further evidence of an infectious process on clinical and imaging follow-up. Conclusion: 18F-FDG PET can be used for diagnosis of diabetes-related infection. The precise anatomic localization of increased 18F-FDG uptake provided by PET/CT enables accurate differentiation between osteomyelitis and soft-tissue infection.
Osteomyelitis of the foot is a challenging diagnosis and affects up to 15% of diabetic patients, often as the result of direct contamination from a soft-tissue lesion (1). Early diagnosis of osteomyelitis in the diabetic foot is crucial because antibiotic therapy can be curative and may prevent amputation. Plain radiography is usually the first imaging technique when bone infection is suspected. CT is also used routinely although not considered accurate in this clinical setting (1–3). Despite drawbacks, MRI is considered the modality of choice for the diagnosis of diabetic foot osteomyelitis and associated soft-tissue abnormalities, with a high reported sensitivity and specificity (1,4–6).
Nuclear medicine plays an important role in the evaluation of infection (7,8). 18F-FDG PET is a useful clinical tool for assessing malignancies. 18F-FDG, a nonspecific tracer of increased intracellular glucose metabolism, accumulates in sites of infection and inflammation as well (9–11). PET is highly sensitive but may be unable to define the anatomic location of a focus of increased 18F-FDG accumulation. The hybrid PET/CT technology, providing precise registration of metabolic and structural imaging data, obtained in the same session on a single device, may improve diagnosis and localization of infection (12).
The purpose of the present study was to assess the role of PET/CT using 18F-FDG in evaluating the diabetic foot for diagnosis and localization of an infectious process to the pedal skeleton or the soft tissues.
MATERIALS AND METHODS
Patient Population
Fourteen consecutive diabetic patients (one type 1 and 13 type 2 diabetes mellitus) with suspected foot infection were prospectively evaluated using PET/CT. The study included 10 men and 4 women, with a mean age of 54 y (range, 29–70 y). Infected diabetic foot was suspected on the basis of the presence of necrotic ulcers, nonhealing wounds, cellulites, or severe foot pain, with or without systemic fever. The 14 patients presented with 18 sites suggestive of infection, including 7 in the forefoot, 1 in the mid foot, and 10 in the hind foot. All patients underwent bone scintigraphy using 99mTc-methylene diphosphonate within a week before the PET/CT study. The clinical characteristics of the patient population and reasons for referral are presented in Table 1; bone scintigraphy results are presented in Table 2. The Institutional Review Board of the hospital approved the study, and each patient gave written informed consent.
Clinical Characteristics of 14 Diabetic Patients with 18 Sites of Suspected Foot Infection
Imaging Findings and Final Diagnosis in 18 Sites in 14 Patients with Suspected Diabetic Foot Infection
PET/CT Acquisition and Processing
Patients were instructed to fast, except for glucose-free oral hydration, for 4–6 h before the injection of 185–370 MBq (5–10 mCi) of 18F-FDG and to keep their regular drug schedule. Blood glucose levels were measured before injection and at the end of the study. None of the patients were withdrawn from the study because of high blood glucose levels, and no additional glucose control drugs were used. PET and non–contrast-enhanced CT of the lower limbs were done 1 h after the injection of 18F-FDG using a PET/CT system (Discovery LS; General Electric Medical Systems), combining a third-generation multislice spiral CT scanner with a dedicated full-ring PET scanner with bismuth germanate crystals. The PET and CT devices were mechanically aligned back to back and shared a table. Proper registration of the 2 images was ensured by shared positional information on the table and patient for both the CT and the PET acquisitions. Data obtained from the CT scan were used for low-noise attenuation correction of PET emission data and for fusion with attenuation-corrected PET images. PET images were reconstructed iteratively using ordered-subset expectation maximization software (Xeleris; General Electric Medical Systems). PET, CT, and fused PET/CT images were available for review, displayed in axial, coronal, and sagittal planes. The PET data were displayed as noncorrected and attenuation-corrected images and also in a rotating maximum-intensity projection.
Interpretation and Analysis of PET/CT Images
All studies were interpreted prospectively by reviewers who were aware of the patient’s clinical history and the results of previous imaging studies. Initially, 2 experienced nuclear medicine physicians interpreted the stand-alone 18F-FDG PET images. Every focus of increased 18F-FDG uptake was recorded, and 18F-FDG uptake with an intensity higher than that of surrounding tissues was defined as an infectious process. A PET study showing at least 1 site of abnormal 18F-FDG uptake was considered positive for infection. A PET study showing no sites of abnormal 18F-FDG uptake was considered negative. Maximum standardized uptake values (SUVs) were measured for all foci of increased 18F-FDG activity using the software supplied by the vendor of the scanner.
An experienced skeletal radiologist reviewed the CT component of the studies without knowing the PET results. All morphologic abnormalities seen on CT were recorded. CT findings considered positive for osteomyelitis included cortical lysis, areas of bone resorption, and periosteal reaction. The diagnosis was reinforced when soft-tissue processes such as abscess, cellulitis, or skin ulcers were seen near the bony lesion. Equivocal CT findings were bone changes of diabetic osteoarthropathy such as osseous fragmentation, sclerosis, subluxation, or dislocation in the mid foot or hind foot or extensive bone resorption in the forefoot. In the presence of these findings osteomyelitis could not be definitely excluded. Negative CT findings were no areas of abnormal bone structure.
A team of nuclear medicine physicians and a radiologist interpreted the fused PET/CT images after the PET and CT reviews. Precise localization of 18F-FDG on the soft tissues or the skeleton, specifically to certain bones, as provided by PET/CT, was recorded. Fused images provided additional information when they allowed more precise localization of the sites of increased 18F-FDG uptake than was obtained by PET images alone.
A final diagnosis of osteomyelitis, soft-tissue infection, or noninfected site was confirmed by histopathologic findings and bacteriologic assays obtained at surgery or by decision of the referring clinical team after further imaging workup or clinical follow-up.
RESULTS
Fourteen patients with 18 sites of clinically suspected infection were evaluated for diabetic foot osteomyelitis (Table 2). PET detected 14 foci of increased 18F-FDG uptake in 10 patients. All 14 sites were considered positive for infection, but PET alone could not precisely localize these foci to bone or soft tissue.
PET/CT localized 8 foci in 4 patients to bone, indicating a diagnosis of osteomyelitis. Five foci were localized to metatarsal bones and 1 lesion each to the medial cuneiform, lateral malleolus, and calcaneus. CT indicated bone changes consistent with osteomyelitis in 5 of these 8 sites. Two additional foci of increased 18F-FDG uptake demonstrated equivocal findings on CT, and 1 focus showed no abnormalities in bone structure. All 4 patients had a final diagnosis of bone infection. One patient had osteomyelitis confirmed by histology and bone culture (isolation of Acinetobacter and Proteus mirabilis). A second patient was diagnosed with osteomyelitis on the basis of the histologic results of tissue samples obtained at surgery and sterile bone culture results (probably due to previous broad-spectrum antibiotic treatment). A third patient was diagnosed on the basis of clinical observation of the bony structures during surgical amputation and on preoperative radiography studies showing bone changes consistent with osteomyelitis. Serial radiography studies of a fourth patient showed bone changes consistent with osteomyelitis that resolved after administering intravenous antibiotic and hyperbaric oxygen therapy.
PET/CT excluded osteomyelitis in 5 sites in 5 patients by localizing the abnormal 18F-FDG uptake solely to soft-tissue infection. CT indicated bone changes consistent with osteomyelitis in 2 of these 5 sites. For 2 sites, CT demonstrated equivocal findings, and 1 site showed no change in bone structure. All 5 patients treated for soft-tissue infection showed good clinical response and no further evidence of osteomyelitis during a 6- to 12-mo follow-up.
One site of mildly increased focal 18F-FDG uptake was localized by PET/CT to diabetic osteoarthropathy changes demonstrated on CT. This patient had no evidence of osteomyelitis after further imaging workup and clinical follow-up over 14 mo.
Four patients showed no abnormal 18F-FDG uptake. On CT, 1 of these 4 patients had severe structural changes in the mid and hind foot, and osteomyelitis could not be excluded. CT of the other 3 patients showed no skeletal lesions. None of these 4 patients showed evidence of osteomyelitis at clinical and imaging follow-up over 9–14 mo.
PET therefore identified 14 foci of abnormal 18F-FDG uptake in 10 patients as consistent with infection. PET/CT confirmed the diagnosis in 13 of the 14 suggestive foci (93%) and correctly localized 8 sites to bone and 5 lesions to soft-tissue infection, whereas 1 site defined as infection on PET was localized and defined by PET/CT as diabetic osteoarthropathy. Maximum SUV in the sites of abnormal 18F-FDG uptake ranged from 1.4 to 11.1 (average, 5.4) (Table 2).
CT characterized 11 lesions as positive or equivocal for osteomyelitis—findings that were further confirmed at 6 sites (55%). CT findings were normal for 4 infectious foci detected on PET, with osteomyelitis confirmed in 2 of these lesions (50%).
Blood glucose levels at the time of the study ranged from 4.7 to 18.3 mmol/L (84–330 mg/dL). Glucose levels exceeded 11.1 mmol/L (200 mg/dL) in 7 of the 14 patients, including 2 patients with negative and 5 patients with positive PET findings.
DISCUSSION
Osteomyelitis and septic arthritis complicate up to one third of diabetic foot infections that require hospitalization and often result from contaminated soft tissues. Early diagnosis is difficult to achieve through noninvasive imaging studies. Nuclear medicine and radiologic imaging techniques, although commonly used, may lack accuracy (1,13).
CT is used routinely because it is widely available, but it is of limited diagnostic value in early stages of acute osteomyelitis of the foot and in patients with diabetic osteoarthropathy. Bone structure changes are seen on radiographs 1–2 wk after the onset of an infectious process, but the time lag is somewhat shorter with CT (14–16). Diagnosing osteomyelitis using radiography or CT may be complicated by the fact that infection and neuropathic osteoarthropathy of the foot frequently coexist in diabetic patients (15).
MRI, because of its high sensitivity and specificity, is considered the modality of choice for diagnosing osteomyelitis of the foot and for identifying associated soft-tissue abnormalities such as cellulitis, phlegmon, abscess, sinus tracts, and ulcers (16). However, MRI findings of acute osteomyelitis may be similar to those of acutely evolving neuropathic osteoarthropathy, biomechanical stress changes related to altered weight bearing, and bone marrow signal changes after orthopedic surgery and trauma (1,4,16). Finally, MRI of the small bones of the forefoot may be technically difficult because of coil designs and field heterogeneity at the margin of the coil (6).
Combined bone 99mTc-methylene diphosphonate and 111In-labeled white blood cell scintigraphy are highly sensitive procedures but may be hampered by coexisting pathologic processes such as neuroarthropathy, trauma, or cellulitis (3). 18F-FDG, an indicator of increased intracellular glucose metabolism, accumulates in sites of infection (17,18). Recent experimental data in an animal model suggest that 18F-FDG accumulates specifically in osteomyelitis rather than in the bone healing process (19). 18F-FDG PET has the advantage of a shorter study time, higher resolution, and relatively higher target-to-background ratio than other nuclear medicine procedures (11). As with other infection-specific scintigraphic techniques, PET, despite its high sensitivity for identifying infectious processes, may be unable to precisely locate the abnormal tracer accumulation. In the present study, 18F-FDG PET correctly identified 93% of all infected sites. However, PET alone could not exactly localize these infectious foci because of the proximity of bone and soft tissues in the foot. Pinpointing the focus of abnormal uptake detected by PET to bone or soft tissue is key for differentiating between osteomyelitis and soft-tissue involvement. PET/CT correctly diagnosed osteomyelitis versus soft-tissue involvement in all 13 infection sites. Eight foci of 18F-FDG uptake were localized by PET/CT to bone structures, consistent with the diagnosis of osteomyelitis (Fig. 1). Five sites of abnormal 18F-FDG uptake were localized by PET/CT only to soft tissues, thus excluding bone involvement (Fig. 2). 18F-FDG may accumulate in nonspecific inflammatory processes, common in diabetic patients. PET/CT correctly localized 1 focus of mildly increased 18F-FDG uptake to neuropathic osteoarthritic changes demonstrated on CT, with no further evidence of infection in this patient. Overall, PET/CT allowed accurate diagnosis of all sites of abnormal 18F-FDG uptake detected by PET.
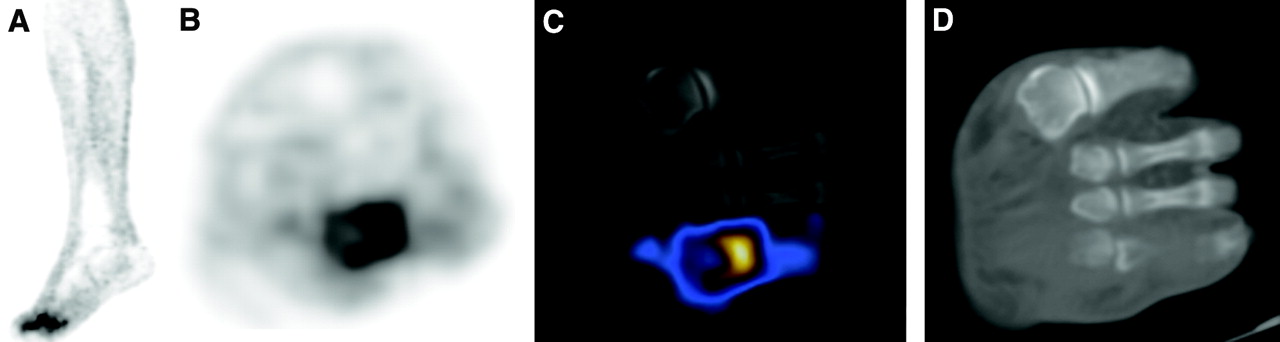
PET/CT-based diagnosis of osteomyelitis complicating diabetic foot in 50-y-old man with nonhealing wound in right forefoot. (A and B) 18F-FDG PET coronal (A) and transaxial (B) images show area of increased 18F-FDG uptake in lateral aspect of forefoot. (C) PET/CT localizes abnormal 18F-FDG uptake to head of fourth metatarsus. (D) CT shows normal bone structure in corresponding area. Osteomyelitis was further confirmed by histopathologic examination of tissue samples obtained at surgery.

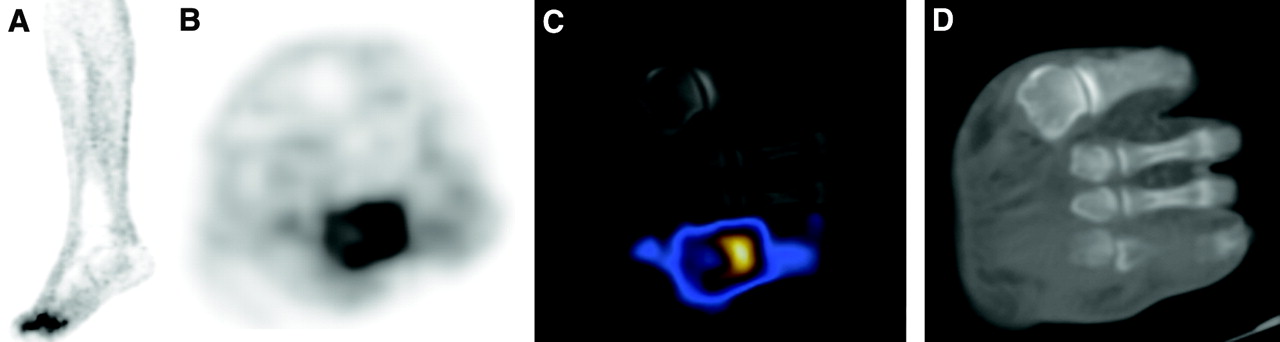
PET/CT-based exclusion of osteomyelitis and localization of infection to soft-tissue abscess in 43-y-old woman with nonhealing ulcer and cellulitis in lateral aspect of right foot. (A and B) 18F-FDG PET coronal (A) and transaxial (B) images show area of increased 18F-FDG uptake in lateral aspect of mid foot. (C) PET/CT localizes abnormal 18F-FDG uptake to soft tissues. (D) CT shows soft-tissue swelling in same area. Patient underwent local drainage and short course of antimicrobial therapy with good clinical response. No evidence of osteomyelitis was found during a clinical and imaging follow-up of 12 mo.
The CT component of the hybrid imaging studies showed skeletal changes consistent with or suggestive of osteomyelitis in 7 of 8 sites with confirmed bone infection, but also in 4 of 5 sites with an infectious process confined only to soft tissues (Table 2). These results confirm previous studies showing that CT is less accurate in diagnosing diabetic foot osteomyelitis because it is unable to distinguish between infection, reactive granulomatous tissue, edema, and fibrosis (15).
A limitation of the present study lies in the availability of a histopathologic diagnosis for only 2 of the 4 patients with osteomyelitis, in addition to surgical observation for a third patient. Previous publications have shown, however, that diagnosing osteomyelitis complicating foot infections is often done by observing clinical response to treatment or performing imaging follow-up studies (20).
Software coregistration of PET with high-resolution anatomic imaging modalities may solve the clinical problem of the diabetic foot (21). Small variations in limb positioning between separate studies may lead, however, to a faulty localization of infectious foci, in particular where different structures are close to each other. Based on these initial results, hybrid PET/CT, combining 18F-FDG assessment of infection and CT structural data of the skeleton, is likely to be a better, more accurate, and certainly simpler procedure for diagnosing osteomyelitis in this patient population. Limited-field-of-view 18F-FDG PET/CT could be the single-step imaging procedure of choice in diagnosing diabetic foot disease, if further confirmed by studies including large clinical series, mandatory for defining a diagnostic algorithm.
The effect of elevated glucose serum levels on PET sensitivity is a controversial issue (22,23). Although extensively assessed in patients with malignancies, the effect of hyperglycemia on 18F-FDG uptake by inflammatory and infectious processes is not well documented. Scarce data suggest that elevated blood glucose levels may not impair 18F-FDG uptake in infection (24). Although elevated glucose serum values were found in half the present study population at the time of 18F-FDG injection, this did not lead to false-negative studies. There was no relationship between the glycemic state and the presence or absence of abnormal 18F-FDG uptake in the present study.
The degree of 18F-FDG uptake, as measured by maximum SUVs, was assessed for all suggestive foci showing abnormal tracer activity. The mean measured value in the infectious foci was 5.7, with variations between 1.7 and 11.1 for both osseous and soft-tissue infectious sites. Although the clinical value of SUV in oncologic diseases has been assessed (25,26), use of SUV in infectious processes needs additional investigation.
This study showed the feasibility of hybrid imaging using PET/CT in evaluating diabetic foot infection. Studies on a larger number of patients and comparing the results of concurrent combined bone and white blood cell scintigraphy are needed to validate and establish the role and diagnostic performance of PET/CT in evaluating diabetic foot infection.
CONCLUSION
The initial experience with PET/CT demonstrates the potential value of hybrid imaging in diabetic patients with suspected foot infections. PET/CT allowed precise diagnosis of osteomyelitis versus soft-tissue infection through better anatomic localization of abnormal PET findings. This single-step, noninvasive imaging modality, combining functional and anatomic data, can facilitate diagnosing and defining diabetic foot infection, help guide further invasive tissue-sampling procedures, and improve treatment planning.
Acknowledgments
This study was supported in part by a grant from the Fund for the Promotion of Research at the Technion–Israel Institute of Technology.
Footnotes
Received Jul. 27, 2004; revision accepted Oct. 8, 2004.
For correspondence or reprints contact: Zohar Keidar, MD, PhD, Department of Nuclear Medicine, Rambam Medical Center, Haifa, Israel.
E-mail: zohar{at}keidar.net
REFERENCES
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Imaging Diverse Pathogenic Bacteria In Vivo with 18F-Fluoromannitol PET
- Detection of Osteomyelitis in the Diabetic Foot by Imaging Techniques: A Systematic Review and Meta-analysis Comparing MRI, White Blood Cell Scintigraphy, and FDG-PET
- Radionuclide Imaging of Musculoskeletal Infection: A Review
- EANM/SNMMI Guideline for 18F-FDG Use in Inflammation and Infection
- Indexing Severity of Diabetic Foot Infection With 99mTc-WBC SPECT/CT Hybrid Imaging
- The Charcot Foot in Diabetes
- Can Sequential 18F-FDG PET/CT Replace WBC Imaging in the Diabetic Foot?
- 18F-FDG and Diabetic Foot Infections: The Verdict Is...
- Investigating suspected bone infection in the diabetic foot
- Diabetic Foot Infection: Usefulness of SPECT/CT for 99mTc-HMPAO-Labeled Leukocyte Imaging
- Fever of Unknown Origin: The Role of 18F-FDG PET/CT
- Role of Modern Imaging Techniques for Diagnosis of Infection in the Era of 18F-Fluorodeoxyglucose Positron Emission Tomography
- Prosthetic Vascular Graft Infection: The Role of 18F-FDG PET/CT
- Imaging Infection with 18F-FDG-Labeled Leukocyte PET/CT: Initial Experience in 21 Patients