


Abstract
Hepatic resection is the therapy of choice for malignant and symptomatic benign hepatobiliary tumors. The concept of remnant liver volume (RLV) has been introduced and can be assessed with CT. However, inhomogeneous liver function distribution and a lack of correlation between morphologic hypertrophy and functional recovery fuelled the enthusiasm for functional imaging. The aim of the present study was to assess liver function reserve (LFR) and remnant liver function (RLF) before and after major liver surgery with hepatobiliary scintigraphy (HBS) and to compare scintigraphic results with volumetric CT data and indocyanine-green (ICG) clearance test results. Furthermore, HBS was used to assess functional recovery of liver function, and results were compared with volumetric data. Methods: Fifteen patients with a partial liver resection were included. HBS was performed before, 1 d after, and 3 mo after surgery. ICG clearance and CT were performed before and 3 mo after surgery. Liver function determined with HBS was compared with ICG and volumetric data. Results: Liver function determination using HBS was highly reproducible. A strong positive association (r = 0.84) was found between LFR determined with HBS and ICG clearance. Little or no association (r = 0.27) was found between CT volumetric analysis and corresponding ICG clearance. A strong positive association (r = 0.95) was found between the RLF determined preoperatively on HBS and the actually measured value postoperatively. A weak positive association (r = 0.61) was found between functional liver regeneration and liver volume regeneration in the 3 mo after partial liver resection. Conclusion: HBS offers a unique combination of functional liver uptake and excretion with the ability to assess the preoperative LFR and to estimate the RLF preoperatively. Determination of the RLF instead of the RLV might clarify some of the discrepancies observed in the literature between RLV and clinical outcome in patients with an inhomogeneous liver function. Finally, liver function regeneration can be monitored using HBS.
Hepatic resection is the therapy of choice for malignant and symptomatic benign hepatobiliary tumors. Recent improvement in the safety of liver surgery has resulted in more extended hepatic resections (1,2). The improvement of results is largely due to better techniques and selection of patients (3).
The maximum extent of resection compatible with a safe postoperative outcome remains unknown, but the risk for perioperative complications is generally believed to increase when the remnant liver volume (RLV) is too small (4). Therefore, preoperative assessment of hepatic function and RLV is advocated (3). Preoperative liver volume and RLV can accurately be estimated by CT (5,6). However, most strategies evaluating preoperative hepatic function reserve and estimating the RLV rely on a homogeneous liver function (7). Unlike patients undergoing liver resection for metastatic cancer or benign liver conditions, patients with hepatocellular carcinoma or obstructing tumors such as cholangiocarcinoma may have underlying chronic liver disease or cholestasis with primary or secondary impaired total or segmental liver function (8–10).
Hepatobiliary scintigraphy (HBS) using 99mTc-labeled iminodiacetic acid (IDA) analogues has been proposed as a liver function test (11). Liver uptake function can be measured by first-pass hepatocyte extraction fraction or the IDA liver uptake rate (12,13). The rate of preoperative 99mTc-mebrofenin liver uptake correlates well with the indocyanine-green (ICG) clearance test in patients scheduled for major liver surgery (14). Because IDA scintigraphy is commonly used for the evaluation of hepatobiliary function (15), HBS might be interesting for evaluation of both total and regional hepatocyte uptake function as well as excretory kinetics for risk assessment before major liver surgery.
Therefore, the aim of this study was to validate total and regional HBS as a tool to measure total and regional liver function before and after major liver surgery and to compare scintigraphic results with volumetric data and ICG clearance test results. Furthermore, the correlation between the immediate postoperative remnant liver function (RLF) predicted on preoperative scintigraphy and the RLF scintigraphically measured 24 h after surgery was assessed. Finally, the relationship between liver function regeneration determined with HBS and volumetric analysis was assessed.
MATERIALS AND METHODS
Patients
During a period of 2 y, 55 patients for whom partial liver resection for hepatobiliary tumors was being considered presented at our medical center and were asked to participate in a trial assessing the metabolic effects of major liver resection. Eight patients refused to participate. In 6 patients, concurrent volumetric data were not available. Sixteen patients had an unresectable tumor. Three patients had a severe peroperative complication (blood loss > 2 L), excluding them from further participation in the primary trial. Seven patients had severe perioperative complications (sepsis, n = 4; abdominal bleeding, n = 1; or lethal hepatic insufficiency, n = 2). We included 15 consecutive patients (7 men, 8 women; mean age, 60.8 y; range, 37–77 y) with a perioperative uncomplicated partial liver resection. No patients had biliary obstruction at the time of inclusion. Six patients were treated for cholangiocarcinoma, 7 patients had a solitary metastasis of a colon carcinoma, and 2 patients had a hepatocellular carcinoma without liver cirrhosis. Five patients had a right hemihepatectomy, 4 patients had an extended right hemihepatectomy, 3 patients had a left hemihepatectomy, and 3 patients had only 1 or 2 liver segments removed. All patients underwent an ICG clearance test 1 d before and 3 mo after surgery. Immediate postoperative ICG clearance was not measured. All patients underwent hepatic CT volumetric analysis and HBS performed a maximum of 2 wk before and 3 mo after surgery. All patients underwent HBS 24 h after surgery. The volume of the resected liver was measured by immersing the specimen in water. The postoperative liver volume was calculated by subtracting the volume of the resected specimen from the preoperatively measured CT liver volume. The study was approved by the Medical Ethics Committee of the Academic Medical Center of the University of Amsterdam. Each patient gave written informed consent before participating in the study.
ICG Clearance Test
On every occasion, bilateral intravenous lines were placed in the antecubital veins. After the patient had fasted overnight, 25 mg of ICG (Infracyanine; Laboratoires Pharmaceutiques) were dissolved in 10 mL of 5% dextrose solution and injected rapidly into the antecubital vein. The clearance tests were performed after overnight fasting because food consumption stimulates hepatic function and bile flow. Blood samples were drawn contralateral to the side of injection before administration of ICG (blank) and at 5, 10, 15, and 20 min after ICG injection. Plasma samples were read against the plasma blank at 805 nm by photospectrometry to determine the concentration of ICG. The theoretic maximum concentration at zero minutes was estimated using the least-squares method (16). Results were expressed as the percentage ICG cleared at 15 min.
CT Volumetric Analysis
CT volumetric analysis was performed as described by Vauthey et al. (6). Patients underwent diagnostic CT of the abdomen with and without intravenous contrast medium before and 3 mo after surgery. All CT examinations were performed with a helical scanner (Philips). CT of the abdomen was performed to include the whole liver in a single breath-hold, using 5-mm collimation. Liver volumes were calculated by integrated software techniques that use density threshold seeding. With this technique, the level of density desired for inclusion in the dataset was selected. Regions that were of the selected density but should not be included in the dataset—such as inferior vena cava, gallbladder, and abdominal and chest wall muscles—were excluded. Liver volumes were calculated before and 3 mo after surgery. Liver volume recovery was calculated by subtraction of the liver volume measured immediately after surgery from the liver volume measured after 3 mo. CT volumetric analysis was compared with ICG clearance, as the gold standard, before and 3 mo after surgery. Finally, the relationship between liver function regeneration determined with HBS and volumetric analysis was assessed.
Scintigraphic Test
Patients underwent HBS using the radiopharmaceutical agent 99mTc-labeled mebrofenin. After intravenous administration of 85 MBq of 99mTc-mebrofenin, a dynamic image acquisition was performed with a γ-camera (Diacam; Siemens) with the liver and heart in the field of view, using a 128 × 128 matrix. Dynamic acquisition was performed in 1 h at 10 s per frame for 60 frames (liver uptake sequence), followed by 50 frames of 1 min each (bile excretion sequence). The liver uptake rate was calculated as described by Ekman et al. (13). Regions of interest (ROIs) were drawn around the liver, heart, and large vessels within the mediastinum (serving as blood pool) and around the total hepatocellular carcinoma (indicative of total activity). The liver ROI was drawn automatically on a threshold-based algorithm using 20% of the maximum liver value on a summed image of the first 10 min of the acquisition as the cutoff. Three different time–activity curves based on the liver, blood pool, and total hepatocellular carcinoma were generated. Liver uptake based on these 3 parameters was calculated in %/min. Furthermore, an ROI could be drawn around parts of the liver to calculate regional differences in 99mTc-mebrofenin uptake. Hepatic 99mTc-mebrofenin uptake was calculated using scanned radioactivity values acquired between 150 and 350 s after injection, to ensure that the calculations were made during a phase of homogeneous distribution of the agent in the blood pool and before the rapid phase of hepatic excretion (13).
All studies were processed twice by the same operator to assess the reproducibility of the hepatic uptake calculations. Scintigraphic liver uptake was correlated with ICG clearance, as the gold standard, before and 3 mo after surgery.
Regional liver function was calculated in retrospect, after completion of the trial. The regional uptake of the future remnant liver on the preoperative HBS was calculated by manual division of the global liver ROI into 2 parts. The surgeon who performed the hemihepatectomy guided the drawing of the remnant liver ROI. In this remnant liver ROI, the estimated RLF was calculated. Furthermore, the remnant liver ROI of the immediate postoperative HBS was copied on the preoperative HBS dataset to recalculate the RLF. Subsequently, the preoperative estimated RLF was compared with the actually measured immediate postoperative RLF. Functional hepatic recovery was calculated by subtraction of the scintigraphic liver function measured immediately after surgery from the liver function measured after 3 mo. Three months after surgery, functional scintigraphic liver regeneration was compared with CT volumetric regeneration.
Statistical Analysis
A commercial computer package (SPSS Inc.) was used to analyze the data. The relationship between ICG clearance, liver uptake of 99mTc-mebrofenin, and CT volumetric analysis was tested using the standard Pearson correlation coefficient. All results are expressed as mean ± SEM. All statistical tests were 2-tailed, and differences were evaluated at the 5% level of significance.
RESULTS
Patient volumetric and functional data are summarized in Table 1. A total of 45 HBS examinations were performed on 15 patients (Fig. 1). For every scintigraphic examination, the hepatic uptake rate of 99mTc-mebrofenin was calculated twice, once on the day the scintigraphy was performed and once in a batch after completion of the trial by the same operator. An excellent correlation (r = 0.99; R2 = 0.98; P < 0.001) was found between the 2 calculations (Fig. 2A). Bland–Altman statistics are shown in Figure 3A. For 27 HBS examinations (preoperative and 3 mo after surgery), a corresponding ICG clearance test was performed. A strong positive association (r = 0.84; R2 = 0.71; P < 0.001) was found between the liver function reserve (LFR) determined with HBS and ICG clearance (Fig. 2B).

Preoperative HBS in patient 13, with a proximal cholangiocarcinoma. (A) Reframed images of the dynamic acquisition. Homogeneous liver uptake with moderate cholestasis is seen in the left side, without functional repercussion. (B) A summed image from 150 to 350 s after intravenous injection of 80 MBq of 99mTc-mebrofenin, with an ROI drawn semiautomatically (threshold, 20%) around the entire liver and a second ROI drawn in the mediastinum (blood pool). (C) A blood-pool–corrected liver-uptake time–activity curve. Liver uptake (d) is calculated as the increase in specific (corrected for blood pool) 99mTc-mebrofenin uptake (y-axis) per minute over a period of 200 s (x-axis).
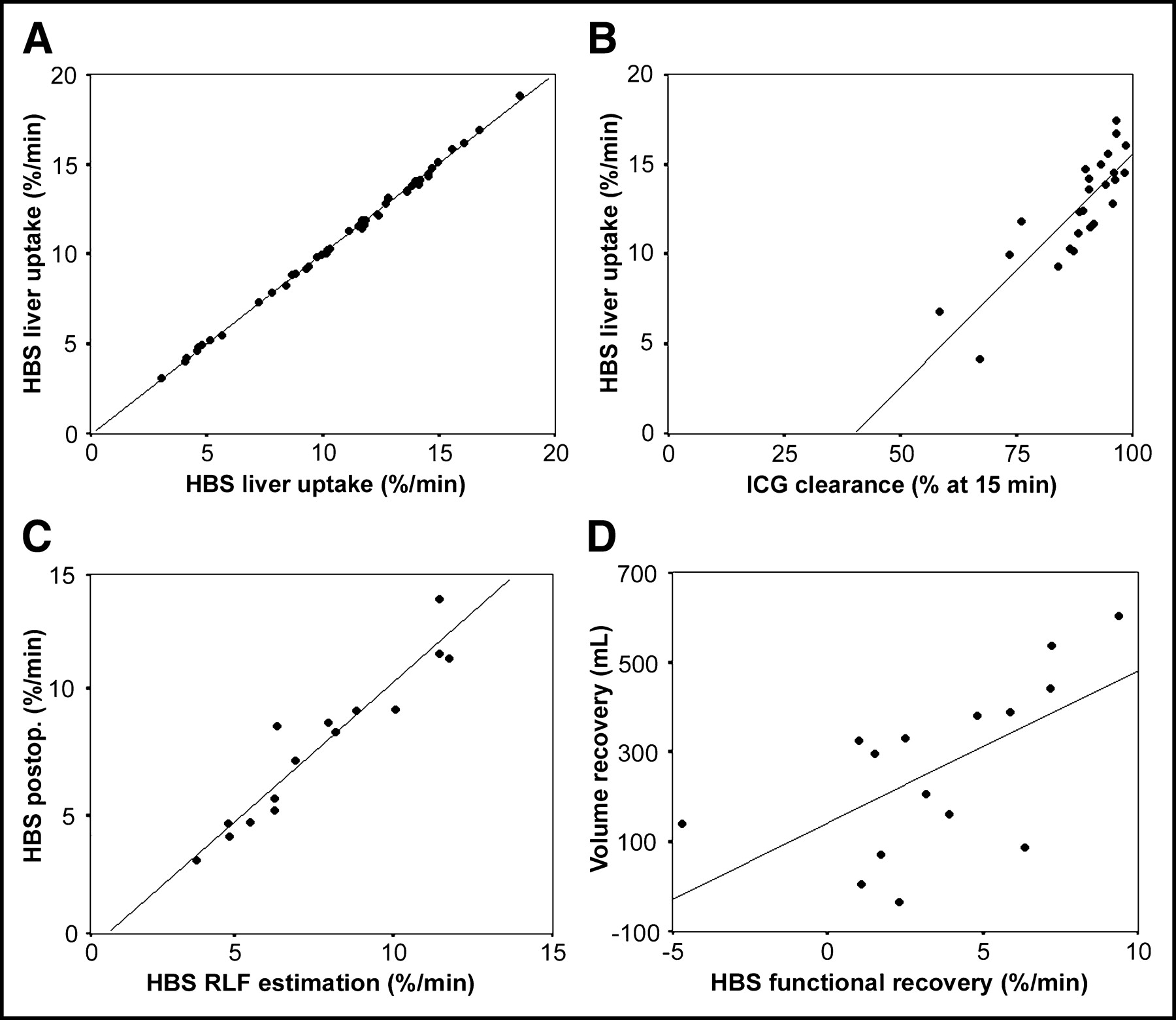
Scatter plots with linear regression line of HBS liver function calculation reproducibility (A), HBS and ICG clearance LFR assessment (B), HBS preoperative and postoperative (postop.) RLF measurement (C), and liver volume and function recovery (D).

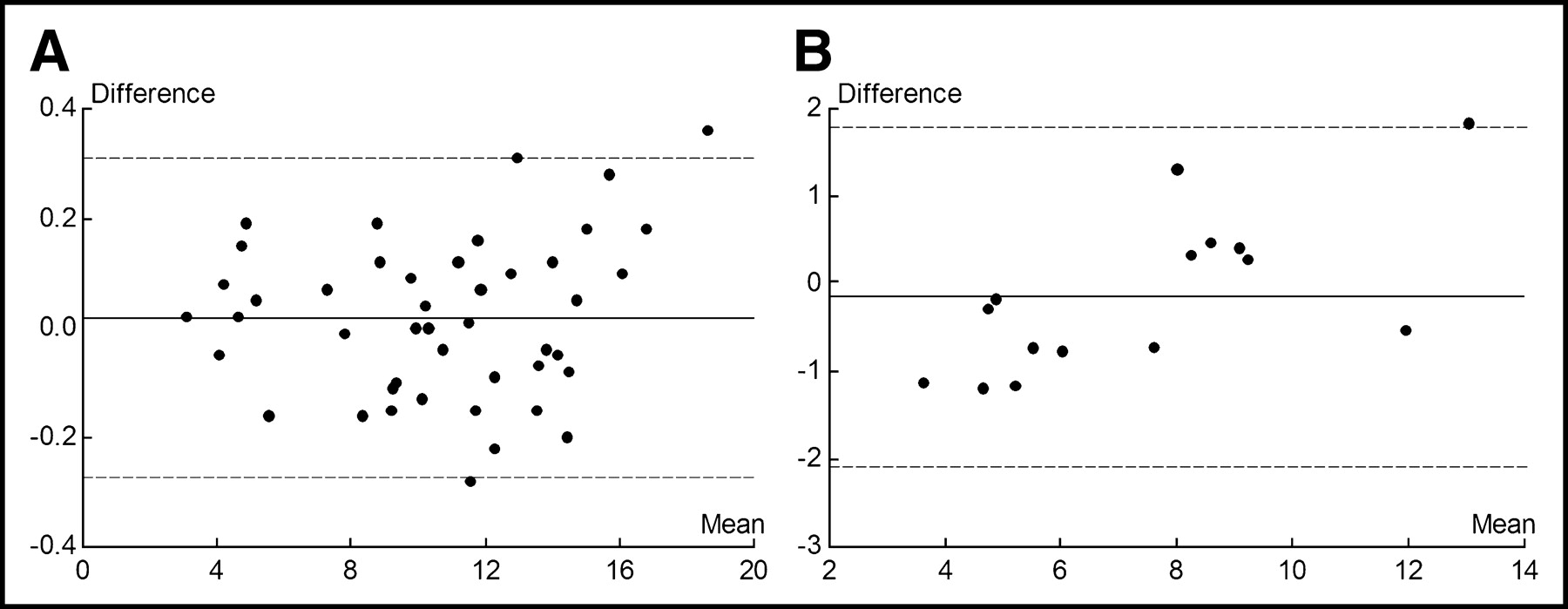
Bland–Altman plots of hepatic 99mTc-mebrofenin uptake, expressed as percentage uptake per minute. (A) A plot of the mean of the repeated liver uptake function calculation on HBS in 45 studies (horizontal axis) vs. the differences in the repeated calculations (vertical axis). (B) A plot of the mean of FLR determination on HBS before and after surgery in 15 studies (horizontal axis) vs. the differences in the repeated measurements (vertical axis). The horizontal solid lines indicate the mean difference between the 2 calculations. The horizontal dashed lines indicate the 95% limits of agreement (mean ± 1.96 SD).
Patient Volumetric and Functional Data
Upon guidance of the surgeon, an ROI encompassing the future remnant liver was drawn on the preoperative HBS image (Figs. 4A and 5A). The scintigraphic RLF within this ROI was assessed and compared with the scintigraphic liver uptake 1 d after surgery (Figs. 4B and 5B). A strong positive association (n = 15; r = 0.95; R2 = 0.90; P < 0.001) was found between these measurements (Fig. 2C). Bland–Altman statistics are shown in Figure 3B. When the ROI of the remnant liver on the immediate postoperative HBS image was copied onto the baseline preoperative scintigram to calculate the RLF, the correlation (n = 15; r = 0.97; R2 = 0.94; P < 0.001) was slightly better.

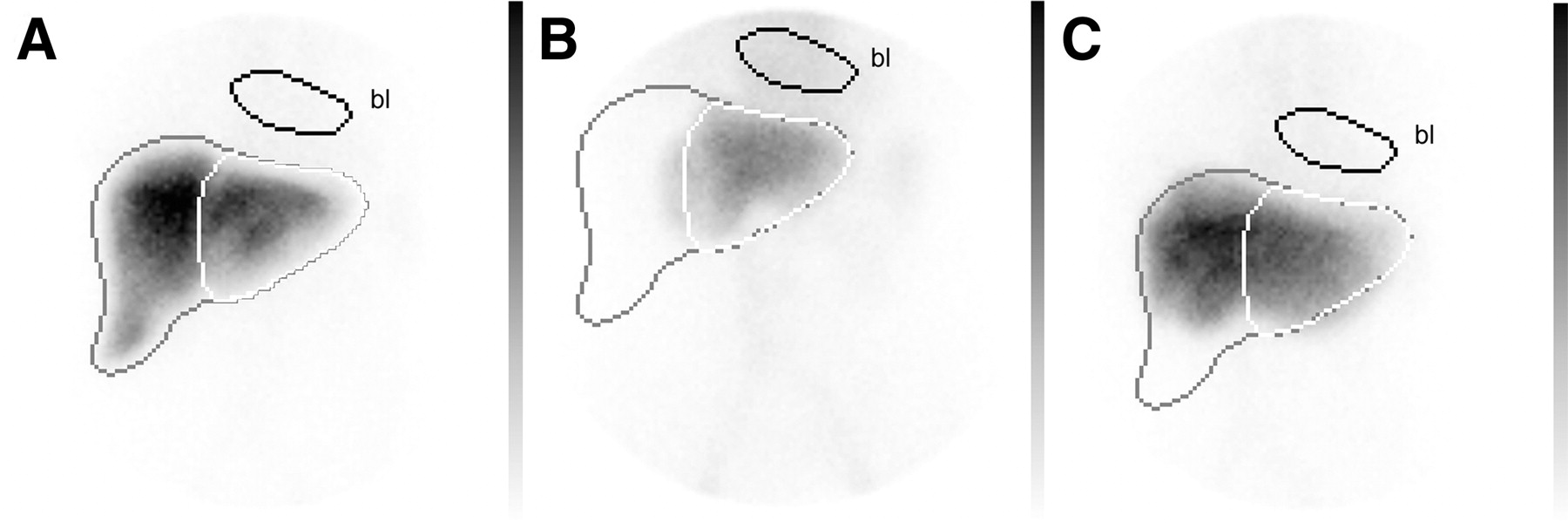
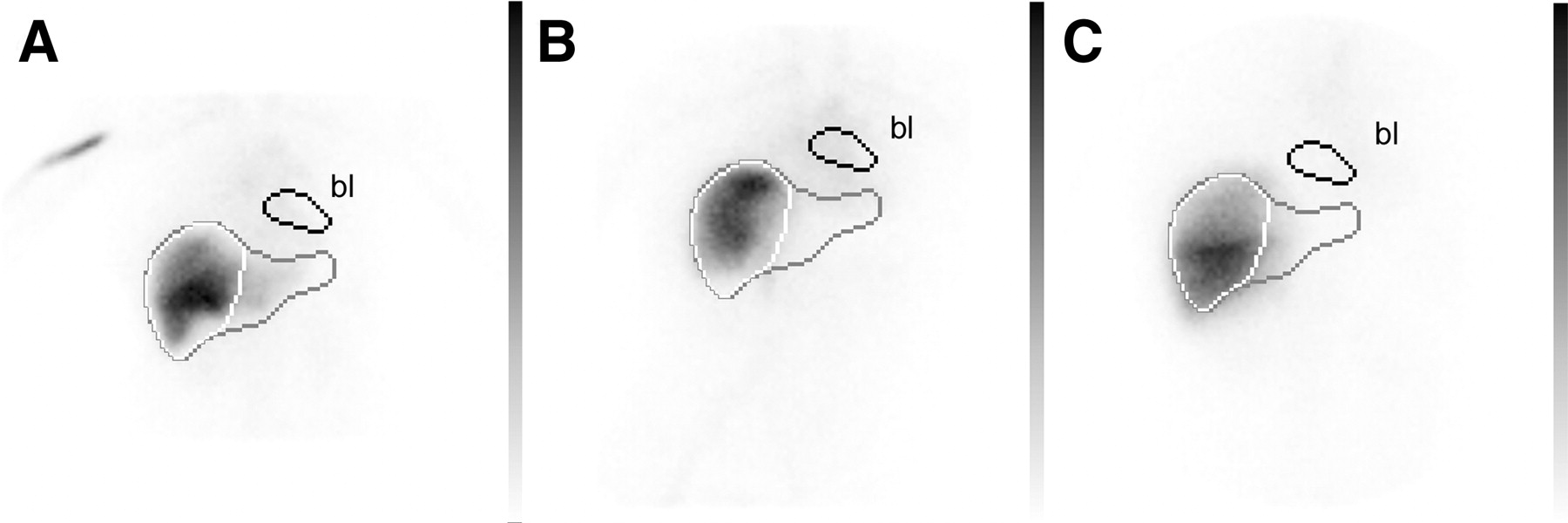
Summed images of patient 3 from 150 to 350 s after intravenous injection of 80 MBq of 99mTc-mebrofenin preoperatively (A), 1 d postoperatively after right-sided hemihepatectomy (B), and 3 mo postoperatively (C). Images are normalized to the preoperative HBS. In A, an ROI is drawn over the entire liver (black), the future remnant liver (white), and the mediastinal blood pool (bl). The ROIs were copied on the HBS performed 1 d and 3 mo postoperatively. The total liver function was 16.05%/min, and the RLF was estimated at 5.88%/min on preoperative HBS. The measured RLF 1 d postoperatively was 5.15%/min. After 3 mo, liver function recovered to 12.80%/min, with hypertrophy visible on HBS.
Liver volumes were assessed with CT preoperatively and 3 mo after surgery. In 27 CT volumetric analysis assessments (preoperative and 3 mo after surgery), a corresponding ICG clearance test was performed. Little or no association (r = 0.27) was found between the measured liver volume and function, determined with CT and ICG clearance, respectively.
Finally, functional liver regeneration was assessed with HBS and compared with volume regeneration assessed with CT volumetric analysis (Table 2). A strong positive association (n = 10; r = 0.81; R2 = 0.66; P < 0.01) was found between liver function assessed with HBS and ICG clearance 3 mo after surgery. A weak association (n = 15; r = 0.61; R2 = 0.37; P = 0.16) was found between functional liver regeneration and liver volume regeneration in the 3 mo after partial liver resection (Fig. 2D). An example of HBS in a patient with a right-sided hemihepatectomy is shown in Figure 4. An example of HBS in a patient with a left-sided hemihepatectomy is shown in Figure 5.
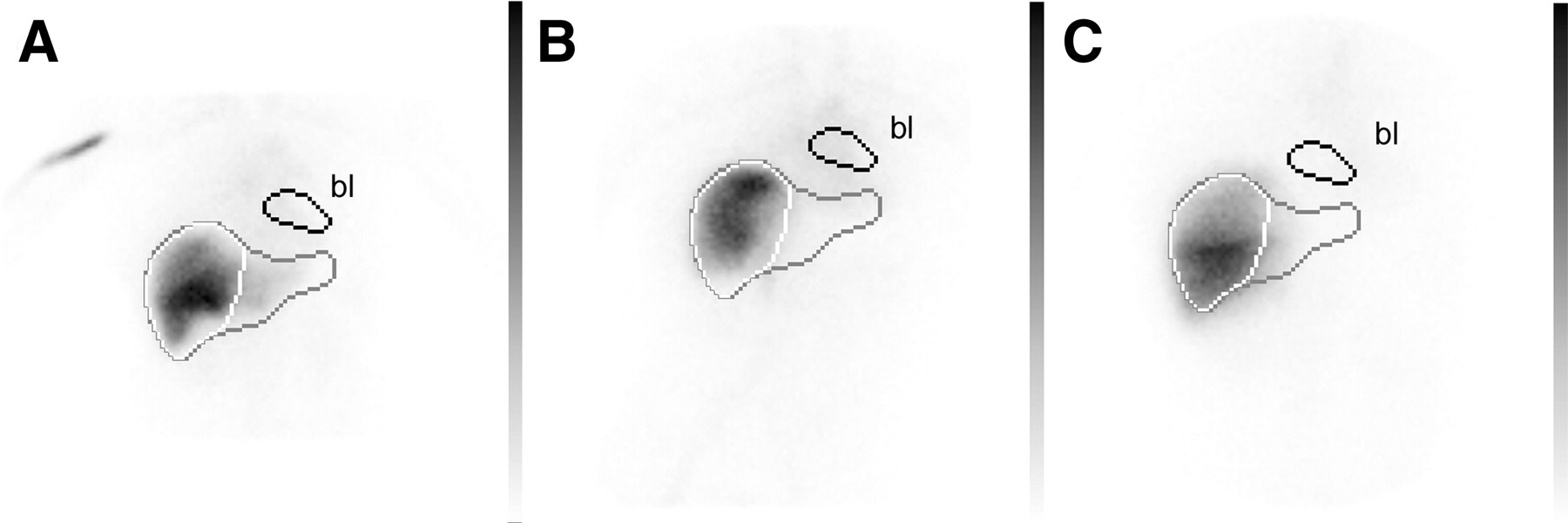
Summed images of patient 15 from 150 to 350 s after intravenous injection of 80 MBq of 99mTc-mebrofenin preoperatively (A), 1 d postoperatively after left-sided hemihepatectomy (B), and 3 mo postoperatively (C). Images are normalized to the preoperative HBS. In A, an ROI is drawn over the entire liver (black), the future remnant liver (white), and the mediastinal blood pool (bl). The ROIs were copied on the HBS performed 1 d and 3 mo postoperatively. The total liver function was 10.30%/min, and the RLF was estimated at 8.99%/min on preoperative HBS. The measured RLF 1 d postoperatively was 9.30%/min. After 3 mo, liver function recovered to 11.79%/min, with hypertrophy visible on HBS.
Liver Recovery Data
DISCUSSION
Improvements in the safety of liver surgery have resulted in more extended hepatic resections (1,2). The improvement of results is largely due to better techniques, resulting in reduction of blood loss (3). However, better selection of patients and exclusion of high-risk patients seems to be another important contributor (3). Furthermore, preoperative (selective) portal vein embolization is used in patients with and without underlying liver disease to increase the safety of and tolerance to major hepatectomy with a small liver remnant (4).
Important parameters in risk assessment for major hepatectomy are the preoperative LFR and the RLV (3,4). Several methods of liver function assessment have been used, including liver biochemistry, Child classification, and quantitative liver function tests (3). The ICG clearance test is regarded as the most accurate test for the evaluation of preoperative hepatic function reserve and for predicting postoperative mortality (17,18). However, test results reflect total liver function but cannot provide information on the distribution of liver function among liver segments.
Preoperative liver volume and RLV can accurately be assessed with CT (6). The combination of functional data with morphology is able to predict hepatic dysfunction in patients with normal liver parenchyma undergoing major liver resection (19). However, many patients undergoing partial hepatectomy for hepatocellular carcinoma have associated liver cirrhosis (8). Furthermore, patients with obstructing biliary tumors such as cholangiocarcinoma may have cholestasis with secondary impaired total or segmental liver function (9). Therefore, 99mDTPA-galactosyl human serum albumin (99mTc-GSA) scintigraphy was previously tested (20) and refined for hepatic function testing and risk assessment for safe partial hepatectomy (21,22). Major limitations are the availability of 99mTc-GSA and the fact that 99mTc-GSA is not excreted into the bile, making it impossible to study liver uptake and excretory function within a single test—a capability that can be useful in tumors or pathology with the possibility of obstruction (23).
HBS has been performed on liver transplant patients to assess the functional and morphologic status of the graft, including structural complications such as bile leakage or bile duct obstruction (24,25). The uptake mechanism of IDA analogues by the hepatocyte is similar to the uptake mechanisms of other anorganic anions (15). Both ICG and IDA analogues are excreted in the bile by hepatocytes by the ATP-dependent export pump multidrug-resistance–associated protein 2, without undergoing biotransformation during transit through the hepatocyte (26–28). Measurement of liver uptake function by iodide clearance rate was described by Ekman et al. (13). We adopted this technique but used 99mTc-mebrofenin as the radiopharmaceutical. 99mTc-Mebrofenin shows a high liver uptake and minimal urinary excretion and strongly resists displacement by a high bilirubin level (15).
In our study, a strong positive association was found between the LFR measured with ICG and HBS, confirming earlier observations (14). Furthermore, the reproducibility of the liver function calculation based on HBS was high. However, reproducibility depends largely on the level of automatic and systematic ROI drawing, which is subject to a learning curve. Therefore, only 1 operator performed calculations in this phase of the trial program.
One can argue that diseased regions are difficult to localize on planar registration and that differences in volumes of liver ROIs might influence the findings (23). Therefore, SPECT techniques offer potential advantages in localization (23,29,30). However, quantitative or semiquantitative analysis in SPECT has limitations of its own, and implementation of attenuation and scatter correction should be considered (31,32). Furthermore, the LFR determined with planar dynamic HBS correlated well with ICG clearance, and the RLF assessed preoperatively correlated well with the value measured postoperatively. Therefore, we feel confident about using planar HBS for the assessment of LFR and RLF. The asymmetric liver shape can produce over- or underestimation of uptake on planar anterior dynamic scintigraphy. Although such estimation errors did not significantly affect data in this study, dual-head dynamic acquisition with geometric mean value calculation could improve the reliability of RLF and will be evaluated in the future.
CT has been shown to assess liver volumes accurately (6). However, the question remains whether volume and function can be related in any given situation. When a small tumor has to be resected from a homogeneous and normally functioning liver, volume and function can be related (19). For these patients, restricted surgery is needed and the significance of RLF determination is questionable (4). For multiple resectable or large tumors, liver function distribution is not homogeneous. Furthermore, patients with hepatocellular carcinoma frequently present with an associated underlying disease such as cirrhosis or cholestasis, induced by obstructing biliary tumors, that affects total or segmental liver function. In these patients, morphologic volumetric analysis may not reflect functional volumetric analysis, possibly explaining the reported lack of association between the volume of the remaining liver and the postoperative course (4,19).
In assessments of functional recovery of the liver after hemihepatectomy, our results showed only a weak association between functional liver regeneration and liver volume regeneration in the 3 mo after partial liver resection. This finding emphasizes the importance of functional imaging and might play an important role in patients subject to preoperative techniques, such as portal embolization, to enhance liver function (33).
Finally, HBS offers the ability to assess both liver uptake and excretory function. Besides preoperative assessment of the functional consequences of possible cholestasis, postoperative assessment of RLF can be combined with biliary function and bile leak assessment. This combination of investigations is not possible with laboratory (ICG), morphologic (CT), or other scintigraphic techniques (23,29,30).
CONCLUSION
HBS offers the unique combination of functional liver uptake and excretion evaluations with the ability to assess LFR preoperatively and to estimate RLF preoperatively. Determination of the RLF instead of the RLV might clarify some of the discrepancies observed in the literature between RLV and clinical outcome in patients with inhomogeneous liver function.
Footnotes
Received Nov. 7, 2003; revision accepted Dec. 29, 2003.
For correspondence or reprints contact: Roelof J. Bennink, MD, Department of Nuclear Medicine, Academic Medical Centre, P.O. Box 22700, 1100 DE Amsterdam, The Netherlands.
E-mail: r.bennink{at}amc.uva.nl
REFERENCES
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Liver Intrinsic Function Evaluation (LIFE): Multi-parametric Liver Function Profiles of Patients Undergoing Hepatectomy
- A Pilot Study on Hepatobiliary Scintigraphy to Monitor Regional Liver Function in 90Y Radioembolization
- Evaluation of liver regeneration and post-hepatectomy liver failure after hemihepatectomy in patients with hepatocellular carcinoma
- The Role of Organic Anion Transporters in Diagnosing Liver Diseases by Magnetic Resonance Imaging
- Quantitative Assessment of Hepatic Function During Liver Regeneration in a Standardized Rat Model
- Nuclear Imaging Techniques for the Assessment of Hepatic Function in Liver Surgery and Transplantation
- Comparison Between the Values of the Hepatic Uptake Rate Obtained by 2 Methods, Using Hepatobiliary Scintigraphy in Patients with Nonalcoholic Steatohepatitis
- 99mTc-Mebrofenin Hepatobiliary Scintigraphy with SPECT for the Assessment of Hepatic Function and Liver Functional Volume Before Partial Hepatectomy
- 99mTc-GSA Scintigraphy with SPECT for Assessment of Hepatic Function and Functional Volume During Liver Regeneration in a Rat Model of Partial Hepatectomy
- Risk Assessment of Posthepatectomy Liver Failure Using Hepatobiliary Scintigraphy and CT Volumetry