


Abstract
This review describes the application of 2 nuclear imaging techniques for assessment of hepatic function in the setting of liver surgery and transplantation. The biochemical and technical background, as well as the clinical applications, of 99mTc-labeled diethylenetriaminepentaacetic acid galactosyl human serum albumin (GSA) scintigraphy and hepatobiliary scintigraphy (HBS) with 99mTc-labeled iminodiacetic acid derivates is discussed. 99mTc-mebrofenin is considered the most suitable iminodiacetic acid agent for 99mTc-HBS. 99mTc-GSA scintigraphy and 99mTc-mebrofenin HBS are based on 2 different principles. 99mTc-GSA scintigraphy is a receptor-mediated technique whereas HBS represents hepatic uptake and excretion function. Both techniques are noninvasive and provide visual and quantitative information on both total and regional liver function. They can be used for preoperative assessment of future remnant liver function, follow-up after preoperative portal vein embolization, and evaluation of postoperative liver regeneration. In liver transplantation, these methods are used to assess graft function and biliary complications.
Surgical resection is still the most effective treatment for patients with hepatic malignancies. Because of improved surgical techniques and perioperative care, extended resections are performed with greater frequency. Extended resections can, however, result in a small postoperative remnant liver with increased risk of postoperative liver failure, especially in patients whose liver parenchyma is compromised because of steatosis, cholestasis, or fibrosis (1,2). Treatment of posthepatectomy liver failure remains difficult, and mortality is substantial. Preoperative evaluation of future remnant liver (FRL) function is therefore important to determine whether a patient can safely undergo an extended liver resection. The availability of preoperative portal vein embolization (PVE) has increased the importance of preoperative assessment of regional hepatic function (3). PVE induces atrophy of the embolized, tumor-bearing liver segments with compensatory hypertrophy of the nonembolized lobe, thereby increasing FRL volume and function. PVE reduces the risk of postoperative liver insufficiency in patients with a marginal FRL (4). The individual hypertrophic response is variable (4,5), indicating the need to quantify the increase in FRL function after PVE.
The unique capacity of the liver to regenerate is important for the clinical outcome of donor and recipient after living donor liver transplantation, as well as for patients undergoing partial liver resection. Liver regeneration is influenced by many factors, including the presence of coexisting parenchymal liver diseases (6). Impaired liver regeneration can cause serious clinical problems such as delayed recovery of postoperative liver function and increased risk of postoperative liver failure. It is consequently imperative to evaluate the recovery of liver function after liver surgery.
The liver encompasses multiple functions, including metabolic, synthetic, and detoxifying functions. In recent decades, several liver function tests have been developed, each reflecting a separate component of the broad spectrum of liver function. 99mTc-labeled diethylenetriaminepentaacetic acid galactosyl human serum albumin (GSA) scintigraphy and hepatobiliary scintigraphy (HBS) with 99mTc-labeled iminodiacetic acid (IDA) derivates are 2 nuclear imaging techniques used for noninvasive evaluation of liver function. This review discusses the biochemical and technical background, as well as the clinical applications, of 99mTc-GSA scintigraphy and HBS for the assessment of hepatic function in liver surgery and transplantation.
THE DEVELOPMENT OF NEW TECHNIQUES FOR ASSESSMENT OF LIVER FUNCTION
The Child–Pugh score is a widely used clinical scoring system that includes biochemical parameters (plasma bilirubin albumin and prothrombin time) together with clinical parameters (presence of encephalopathy and ascites). The Child–Pugh scoring system is conventionally used in selecting patients with hepatocellular carcinoma and cirrhosis for resection or transplantation. It provides merely indirect information on FRL function and can be unreliable for predicting clinical outcome after liver resection, especially in noncirrhotic patients (7,8).
Indocyanine green (ICG) clearance and galactose elimination capacity are dynamic quantitative liver function tests. ICG is cleared from plasma by hepatocyte transporters located on the basolateral membrane and subsequently excreted into the bile (9). Galactose elimination capacity measures the rate of galactose elimination from the blood—a rate that depends mainly on phosphorylation of galactose by galactokinase (10). Although the ICG clearance test (11,12) and galactose elimination capacity (13) have the ability to preoperatively predict morbidity and mortality after partial hepatectomy, they can be unreliable (7,14) because they measure global liver function and not specific FRL function. The ICG clearance test is the most frequently used quantitative liver function test in liver surgery and transplantation (15). Other clinically applied liver function tests include the monoethylglycinexylidide test, which measures hepatic metabolism of lidocaine through the cytochrome p450 pathway (16,17), the caffeine clearance test, and the aminopyrine breath test (7), all of which provide information on total liver function only.
CT volumetry, in which liver volume is used as an indirect measurement of liver function, is currently the established method to determine whether a patient can safely undergo liver resection (15,18). Although there are no official guidelines, an FRL volume larger than 25% (15%–40%) of total liver volume is considered sufficient for a safe resection in patients with normal liver parenchyma, whereas in patients with a compromised liver (e.g., fibrosis, steatosis, or cholestasis), more than 40%–50% is preferred (15,19). These separate ranges of what is considered sufficient FRL volume necessitate the preoperative assessment of liver parenchyma quality by liver biopsy to identify patients with increased surgical risk. Preoperative liver biopsy is not routinely performed, because of the potentially unequal distribution of parenchymal damage (20) and the risk of complications (21,22). As a result, the quality of the liver parenchyma remains frequently uncertain, rendering preoperative risk analysis by CT volumetry unreliable.
In recent decades, several nuclear imaging techniques have been developed as noninvasive methods for evaluating liver function. 131I-rose bengal was one of the first agents used for HBS. 131I-rose bengal is taken up from the circulation by hepatocytes and excreted into the biliary system. Rose bengal fell in disfavor because of several disadvantages, including its slow hepatic clearance and significant β-radiation, which limits the dose that can safely be administered, thereby resulting in poor imaging characteristics. 99mTc proved a more suitable isotope for scintigraphy because of its excellent physical characteristics. Several 99mTc-labeled agents have been developed, including 99mTc-sulfur colloid, 99mTc-GSA, and 99mTc-IDA. The latter 2 radiopharmaceuticals can be used for assessment of hepatocyte function, whereas 99mTc-sulfur colloid scintigraphy is based on the principle of phagocytosis by the reticuloendothelial cells of the liver, thereby visualizing RE activity.
99MTC-GSA SCINTIGRAPHY
Background
The asialoglycoprotein receptor is present only in mammalian hepatocytes and is specific for asialoglycoproteins, which are formed after the removal of sialic acid from endogenous glycoproteins by sialidases. The asialoglycoprotein receptor consists of 2 subunits (human hepatic lectins 1 and 2) and is expressed on the hepatocyte sinusoidal surface adjoining the extracellular space of Disse (23). Asialoglycoproteins bind to asialoglycoprotein receptors and are subsequently taken up by receptor-mediated endocytosis and delivered to lysosomes for degradation. A significant decrease in asialoglycoprotein receptors together with accumulation of plasma asialoglycoproteins is seen in patients with chronic liver diseases (24,25). At first, 99mTc-labeled galactosylneoglycoalbumin was developed as a synthetic asialoglycoprotein to visualize and quantify its hepatic binding to the asialoglycoprotein receptor (26). For clinical use, 99mTc-GSA, which is commercially available in an instant labeling kit in Japan, was developed (27). The liver is the only uptake site for 99mTc-GSA, which is therefore an ideal agent for functional liver scintigraphy. The parameters obtained from planar 99mTc-GSA scintigraphy proved valuable for the assessment of liver function in cirrhotic patients and demonstrated a strong correlation with conventional liver function tests (i.e., antithrombin III, bilirubin, prothrombin time, ICG clearance, Child–Pugh classification, and histology [hepatic activity index score]) (28,29). A discrepancy between the ICG clearance test and 99mTc-GSA scintigraphy is described in 9%–20% of the patients in whom the histologic severity of disease is better reflected by 99mTc-GSA scintigraphy (30,31). 99mTc-GSA scintigraphy is also effective in assessing hepatic function in patients with hyperbilirubinemia (32–34).
Kinetics and Quantitative Measurement of Liver Function
After an intravenous bolus of 99mTc-GSA, dynamic 99mTc-GSA scintigraphy images are obtained by a γ-camera positioned over the heart and liver region. The blood clearance and hepatic uptake are obtained by generating regions of interest (ROIs) of the heart and liver, respectively. For actual kinetics of 99mTc-GSA receptor binding, 3 models are commonly applied.
Vera et al. developed a 3-compartment model of a bimolecular chemical reaction (35). Required for calculations in this model are time–activity curves of liver and heart; the patient's height, weight, and hematocrit level; and a portion of the injected dose from a blood sample. Five independent parameters are calculated: receptor concentration, receptor affinity (forward binding rate), hepatic plasma volume, extrahepatic plasma volume, and hepatic plasma flow. The receptor concentration is the most accurate index for hepatic function (36,37).
A 5-compartment model based on a Michaelis–Menten type of kinetics for receptor–ligand binding was introduced as a noninvasive approach, requiring no blood samples (38). Blood flow and maximal removal rate (Rmax) of 99mTc-GSA (mg/min) from plasma are calculated from time–activity curves of heart, liver, and lung (background). Miki et al. introduced a 7-compartment model that included receptor-mediated endocytosis and receptor recycling (39). The model permits quantitative measurement of total receptor amount (Rtot) and hepatic blood flow, without blood samples. Rtot correlates with the number of viable hepatocytes and can be used to assess functional liver mass (40).
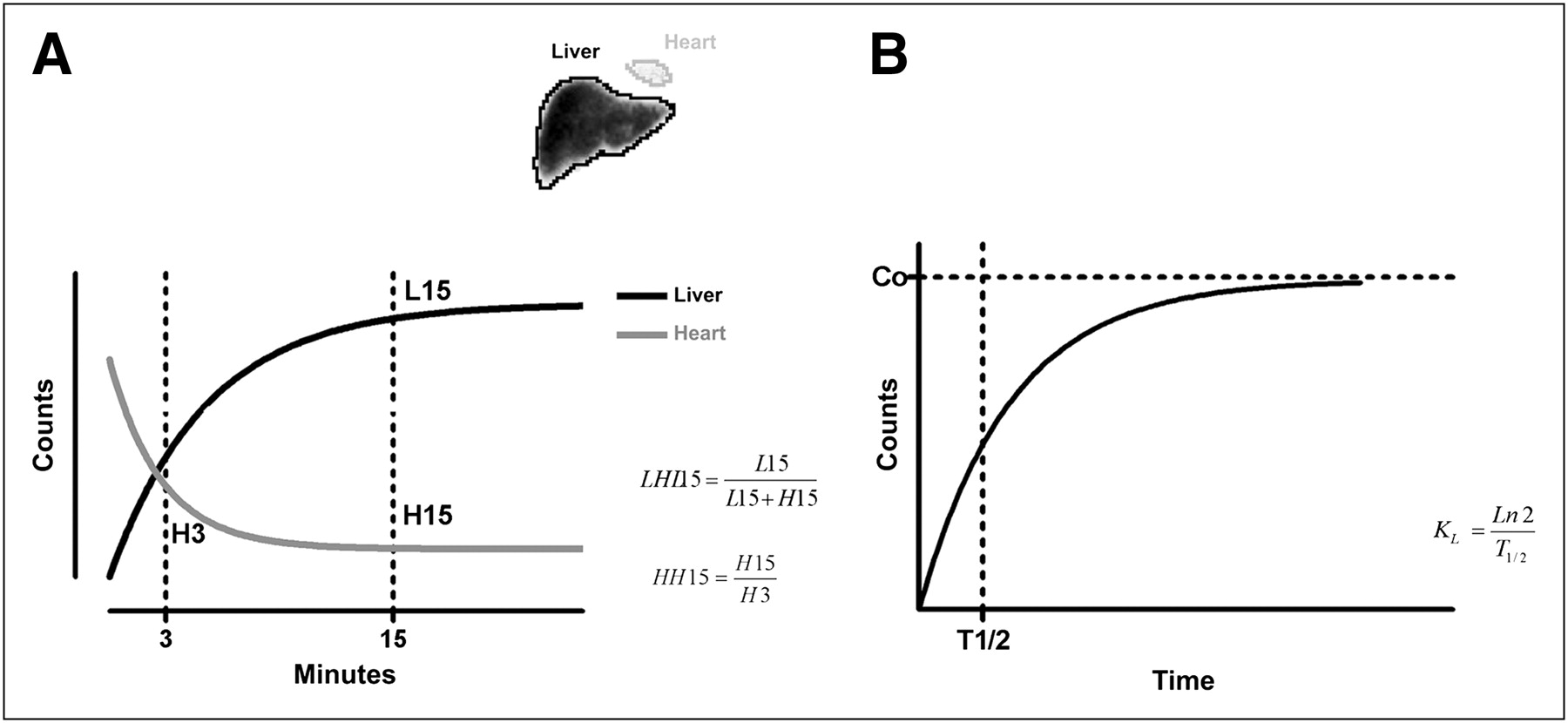
Although many different parameters can be calculated from the different kinetic models, they are highly complex and therefore not widely used in the context of liver surgery. Tables 1 and 2 provide an overview of frequently used parameters in this field. Hepatic uptake ratio and blood clearance ratio of 99mTc-GSA are the most commonly used parameters determined from planar dynamic 99mTc-GSA scintigraphy (Fig. 1). Blood clearance ratio is calculated by dividing the radioactivity of the heart ROI at 15 min after 99mTc-GSA injection by that at 3 min after injection (HH15). Hepatic uptake ratio is calculated by dividing the radioactivity of the liver ROI by the radioactivity of the liver-plus-heart ROIs at 15 min after injection (LHL15) (27,29,41). The modified receptor index is determined by dividing LHL15 by HH15 (29).
Commonly Used Parameters from Dynamic Planar 99mTc-GSA Scintigraphy
Commonly Used Parameters Derived from 99mTc-GSA SPECT
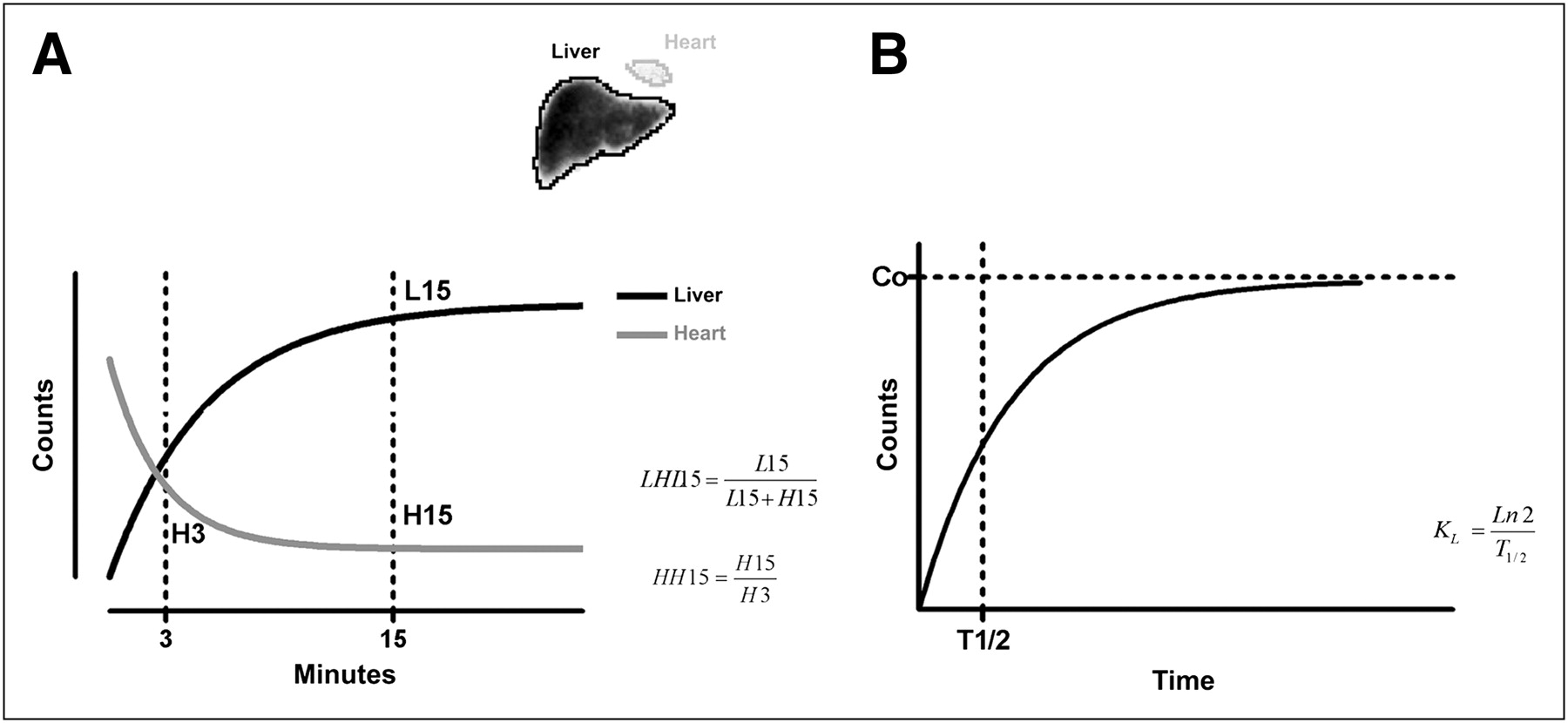
Planar dynamic 99mTc-GSA scintigraphy. (A) LHL15 and HH15 are calculated from 99mTc-GSA time–activity curves from heart (gray) and liver (black). (B) Blood clearance constant (KL) is calculated from liver uptake curve using clearance half-time (T1/2).
Static 99mTc-GSA SPECT has been introduced to improve the assessment of segmental liver function and to measure functional liver volume (33,42–44). The outline extraction method is a simple technique to calculate functional liver volume using a specific cutoff value to automatically outline the liver (33). However, it does not incorporate regional functional differences within the included volume. Therefore, Satoh et al. described a more precise method for calculating functional liver volume depending on the degree of 99mTc-GSA radioactivity in each voxel (43). First, the voxel with maximal counts was determined. Voxels with counts below 54% of the maximal counts were regarded as background. Voxels with counts above 80% of the maximum were considered fully functional, and their voxel thickness was counted as the maximal voxel thickness for the calculation of liver functional volume. For each voxel with counts between 54% and 80%, the voxel thickness was estimated according to the accumulated counts in that voxel.
In addition to static SPECT, dynamic SPECT has been applied. It requires a fast rotating multidetector γ-camera, which is not widely available. Liver uptake ratio and liver uptake density are calculated from dynamic SPECT acquisitions (45,46). Liver uptake ratio reflects the percentage of hepatic SPECT counts relative to the injected counts measured in the syringe, thereby calculating the dose that is incorporated in the liver. Liver uptake density is the liver uptake ratio divided by functional liver volume. In addition, the hepatic 99mTc-GSA clearance (Ku, mL/min) can be calculated using a Patlak plot analysis (42).
99mTc-GSA Liver Scintigraphy in Experimental Surgical Research
Small-animal models are commonly used to study the complex recovery mechanisms of liver function during liver regeneration. Recently, we studied the application of 99mTc-GSA scintigraphy with SPECT for the assessment of liver function and functional volume during liver regeneration in a rat model (47). In normal rat livers, as well as in regenerating livers, a strong correlation was found between functional liver volume and conventional liver volume, indicating the usefulness of 99mTc-GSA SPECT to measure functional liver volume in a noninvasive manner. The hepatic 99mTc-GSA uptake measured by dynamic scintigraphy, however, seemed to underestimate hepatic regeneration in comparison to liver volume.
Unlike ICG, 99mTc-GSA uptake is not directly inhibited by hyperbilirubinemia and can therefore be used to evaluate liver function during cholestasis. In a rat model of obstructive jaundice, hepatic 99mTc-GSA uptake decreased as the period of jaundice was prolonged, as is explained by a decrease in affinity of the asialoglycoprotein receptor for 99mTc-GSA (34).
Clinical Use of 99mTc-GSA Liver Scintigraphy in Liver Surgery
Preoperative Assessment of Liver Function
Multiple studies have described the application of preoperative planar dynamic 99mTc-GSA scintigraphy for predicting postoperative complications (31,48–50). Preoperative GSA Rmax and LHL15 proved to be reliable indicators for predicting postoperative complications in patients with hepatocellular carcinoma and chronic liver disease, because significantly lower values were found in patients with major postoperative complications (30,50). Specific cutoff values for LHL15 (i.e., 0.90 (48) and 0.875 (31)) have been described to select patients with a high risk for complications. Other cutoff values include LHL15/preoperative liver volume of 0.76 (32) and total asialoglycoprotein receptor concentration in the FRL of 0.05 μmol (31,49). Cutoff values, however, usually are not based on accurate risk analysis but rather are set arbitrarily. In patients with a discrepancy between ICG15 and LHL15, 99mTc-GSA scintigraphy was better in predicting postoperative complications (31). Multivariate analysis revealed that LHL15 was an independent preoperative predictor of postoperative complications in patients with chronic liver disease, whereas the ICG clearance test was not (48). Postoperative liver failure, however, was also observed in patients with relatively normal liver function (LHL15 > 0.875), as can be explained by the fact that LHL15 measures only preoperative total liver function and not FRL function.
Static 99mTc-GSA SPECT was introduced for measurement of functional volume and more accurate assessment of segmental liver function (33,42–44). Whereas functional volume measured by 99mTc-GSA SPECT reflects the functional hepatocyte mass (43,51), CT volumetry cannot distinguish between functional and nonfunctional liver tissue. This is especially of interest in cirrhotic patients, in whom advanced fibrosis is accompanied by a reduction of functional hepatocytes. In addition, tumor compression on surrounding liver tissue, bile ducts (33), or blood vessels (52) can affect regional liver function, whereas liver volume is maintained over a longer period. Preoperative functional volume measured by 99mTc-GSA SPECT proved more suitable for predicting remnant liver function than did CT volumetry in a study group with predominantly cirrhotic patients (33,44). Although the outline extraction method is regularly used to calculate functional hepatic volume (33,44,52–54), that method is based on the assumption that liver function is uniformly distributed in the tissue included within the cutoff value. Especially in tumor-bearing and compromised livers, function is not distributed homogeneously. Therefore, functional volume does not necessarily correlate with intrinsic liver function measured by dynamic planar 99mTc-GSA scintigraphy (41,43).
To overcome this problem, dynamic SPECT was introduced. A study by Sugahara et al. demonstrated the advantage of dynamic SPECT for assessment of regional liver function (55). Liver functional volume (by outline extraction method), liver uptake ratio, and liver uptake density were calculated in patients with different severities of parenchymal liver disease. Both liver uptake ratio and liver uptake density decreased with the severity of liver disease, whereas functional liver volume was significantly decreased only in patients classified as Child–Pugh C. The ratio of liver uptake (and liver uptake density) between the left liver lobe and right lobe changed with the progression of liver disease, confirming that liver function is not distributed homogeneously in patients with compromised livers. Dynamic SPECT was used to measure FRL function and preoperatively predict postoperative complications (42,43). Patients with postoperative liver insufficiency had significantly lower hepatic FRL 99mTc-GSA clearance (Ku, in mL/min) than did patients without complications (42). The predictive residual index was able to predict postoperative complications with a positive predictive value of 71% and negative predictive value of 100%, using a cutoff value of 0.38 (43). The conclusions in these studies, however, were based on a relatively small number of complications.
Increase of Liver Function After PVE
Several studies evaluated increased FRL function after PVE using 99mTc-GSA scintigraphy (46,53–57). In 2 studies, the increase in FRL function after PVE was measured by dynamic 99mTc-GSA SPECT and was compared with an increase in FRL volume, measured by CT volumetry, in cirrhotic and noncirrhotic patients (53,57). The increase in FRL function (expressed as liver uptake ratio, liver uptake density, residual functional liver volume, and predictive residual index) was more extensive than the increase in FRL volume, indicating that 99mTc-GSA scintigraphy has additional value over CT volumetry for evaluating the functional increase in FRL after PVE.
So far, no studies have been published on the use of 99mTc-GSA scintigraphy in selecting candidates for PVE. Therefore, further research in this field is recommended.
Postoperative Liver Regeneration
Postoperative liver regeneration is currently evaluated by CT volumetry. A discrepancy has been described between postoperative liver functional recovery and volumetric liver regeneration. Tanaka et al. reported that functional recovery was impaired after large resections, in comparison to volumetric regeneration (41). However, data presented in this study demonstrated that 4 wk after a resection, the average LHL15 recovered to 95% of the preoperatively measured value, whereas volume recovered to approximately 70% of initial values. This finding suggests that functional recovery was greater then volumetric recovery, indicating the opposite of the conclusions drawn by the authors. Kwon et al. described in 2 almost identical studies that functional regeneration was more rapid than volumetric regeneration measured by CT volumetry (44,54). Functional and volumetric liver regeneration was delayed in patients with underlying liver disease. Although no direct comparison was made between 99mTc-GSA SPECT and CT volumetry, it was concluded that functional recovery was more rapid in patients with injured livers. Again, in our view, the data presented in these studies do not support this conclusion. Although 99mTc-GSA scintigraphy is useful to assess liver regeneration, it is difficult to draw conclusions on the difference between functional and volumetric regeneration from the present evidence.
99mTc-GSA scintigraphy has also been used to preoperatively predict the rate of liver regeneration after partial hepatectomy in patients with liver fibrosis (58). 99mTc-GSA scintigraphy correlates with the severity of liver fibrosis, and impaired liver regeneration is also described in patients with an increased severity of liver fibrosis (59). Patients with a high preoperative HH15 (>0.52) that was due to fibrosis exhibited a worse regeneration of the remnant liver (58).
Clinical Use of 99mTc-GSA Scintigraphy in Liver Transplantation
After liver transplantation, graft function is affected by many factors, including acute and chronic rejection, indicating the necessity to evaluate posttransplantation graft function. In a study comprising 7 liver transplant patients, the total amount of asialoglycoprotein receptors (Rtot by the kinetic model of Miki et al. (39,40)) was used to evaluate liver allograft function (60). Histologic liver damage was evaluated from a biopsy sample and correlated with Rtot. Although cohort size was small, this study shows the potential of 99mTc-GSA scintigraphy to noninvasively evaluate graft function after transplantation.
In an auxiliary partial orthotopic liver transplantation, the native liver is left partially in place and the donor (partial) liver graft is positioned orthotopically. 99mTc-GSA scintigraphy can be used to monitor both graft and native liver function after auxiliary partial orthotopic liver transplantation (61). The uptake of 99mTc-GSA (calculated by Patlak plot analysis) proved a better predictor of actual graft function than did liver volume assessed by CT volumetry. Especially in patients with severely damaged liver grafts, 99mTc-GSA uptake corresponded better with histopathologic evaluation of liver biopsy than did CT volumetry.
In 2004, Kwon et al. addressed the need to accurately measure FRL function in donors participating in living donor liver transplantation (62). The authors concluded that the FRL function estimated by 99mTc-GSA SPECT is useful for selecting the hepatectomy procedure in the setting of living donor liver transplantation. However, that study was performed on 152 patients resected predominantly for malignant tumors and not for living donor liver transplantation. Eighty-three percent of the patients were resected for hepatocellular carcinoma, which is frequently associated with liver cirrhosis. Therefore, it is highly questionable if the patients included in this study are representative of living donors.
HBS WITH IDA DERIVATES
Background
99mTc-IDA agents were introduced in 1976 by Loberg et al. (63). These lidocaine analogs are transported to the liver predominantly bound to albumin (64). Dissociation between albumin and the 99mTc-IDA agents occurs in the hepatic space of Disse, after which the 99mTc-IDA agents is taken up by the hepatocytes. Although IDA agents are not metabolized, they follow the path of intracellular transit similar to various endogenous and foreign substances, including bilirubin, hormones, drugs, and toxins, thus representing an important function of the liver (64,65). Organic anion transporter polypeptides, expressed in the basolateral plasma membrane of hepatocytes, are involved in the uptake of organic anions. Organic anion transporter polypeptides 1B1 and 1B3 are able to transport 99mTc-mebrofenin, which is an IDA derivate (66). IDA agents are excreted in the bile canaliculi similarly to ICG without undergoing biotransformation during their transport through the hepatocyte and, therefore, are ideal tracers for the biliary tract (63,67). The suggested bile canalicular transporters include multidrug resistance protein 2 (66,68).
99mTc-labeled IDA agents were first used in cholescintigraphy for the diagnosis of various biliary diseases (64,69). More recently, the application of HBS has been proposed for assessment of liver function (70). Liver uptake of IDA agents can be affected by high plasma levels of bilirubin (69). Of all IDA analogs, 99mTc-mebrofenin shows the highest hepatic uptake, minimal urinary excretion, and strong resistance to displacement by high plasma bilirubin concentrations (69,71). Therefore, 99mTc-mebrofenin is considered the most suitable agent for hepatic and biliary diagnostic procedures. 99mTc-mebrofenin uptake can be hindered by hypoalbuminemia, as albumin is the main plasma carrier of 99mTc-mebrofenin (69). Hypoalbuminemia consequently decreases hepatic delivery of 99mTc-mebrofenin and increases renal excretion. Conversely, hypoalbuminemia in liver disease is a sign of impaired liver function and therefore decreased mebrofenin uptake in patients with hypoalbuminemia still reflects liver function.
The Kinetics and Quantitative Measurement of Liver Function
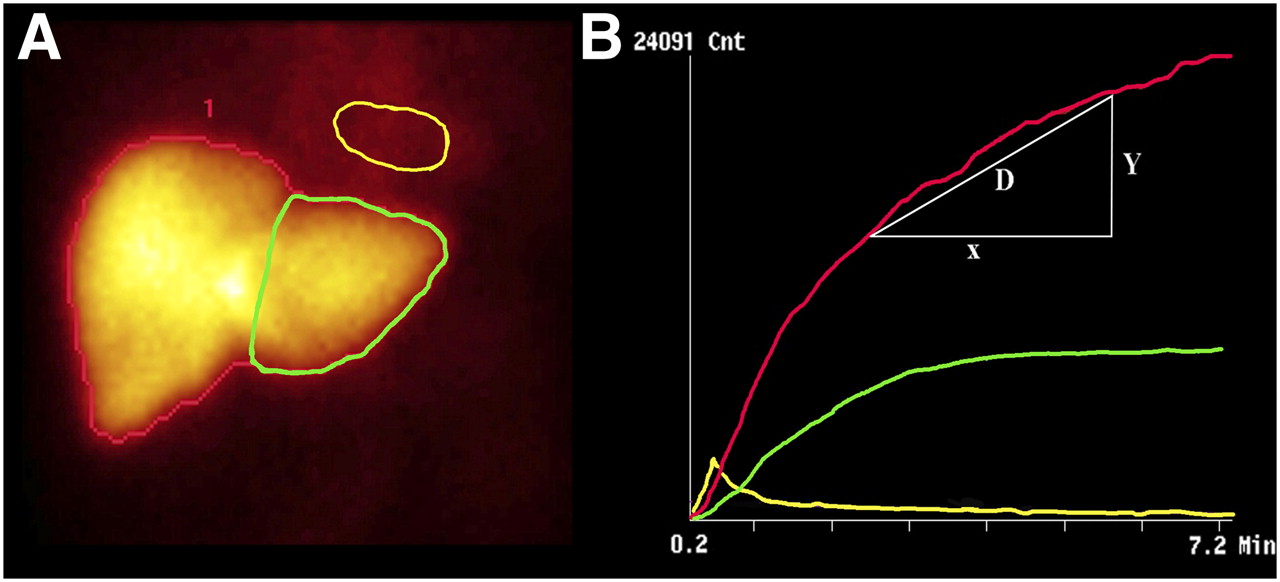
Measurement of hepatic uptake function by the clearance rate of iodide (an IDA analog) was first described by Ekman et al. (72). The hepatic uptake of 99mTc-mebrofenin is calculated similarly to iodide (73). After intravenous injection of 99mTc-mebrofenin, dynamic scintigraphy is performed with a γ-camera. The hepatic uptake of 99mTc-mebrofenin is determined by drawing an ROI around the liver, the heart (serving as blood pool), and the total field of view (Fig. 2). Three different time–activity curves based on these ROIs are generated. With these 3 parameters, the hepatic 99mTc-mebrofenin uptake rate (%/min) can be calculated. Radioactivity values acquired between 150 and 350 s after injection are used to ensure that the calculations are made during a phase of homogeneous distribution of the agent in the blood pool, before biliary excretion takes place (73,74). To compensate for differences in individual metabolic requirements, hepatic 99mTc-mebrofenin uptake rate (%/min) is divided by body surface area and expressed as %/min/m2. ROIs can be drawn around specific parts of the liver to calculate regional differences in 99mTc-mebrofenin uptake (Fig. 2). FRL uptake function is calculated by dividing counts within the ROI of the FRL by the total liver counts and multiplying this factor by total liver 99mTc-mebrofenin uptake and is expressed as %/min/m2. Regional uptake and FRL uptake of 99mTc-mebrofenin can be assessed with little intra- and interobserver variation (74,75). Single-head γ-cameras permit anterior or posterior projections of the liver only. Dual-head γ-cameras enable simultaneous data acquisition of the anterior and posterior projections, from which a geometric mean dataset can be calculated, thereby reducing the attenuation bias (76).
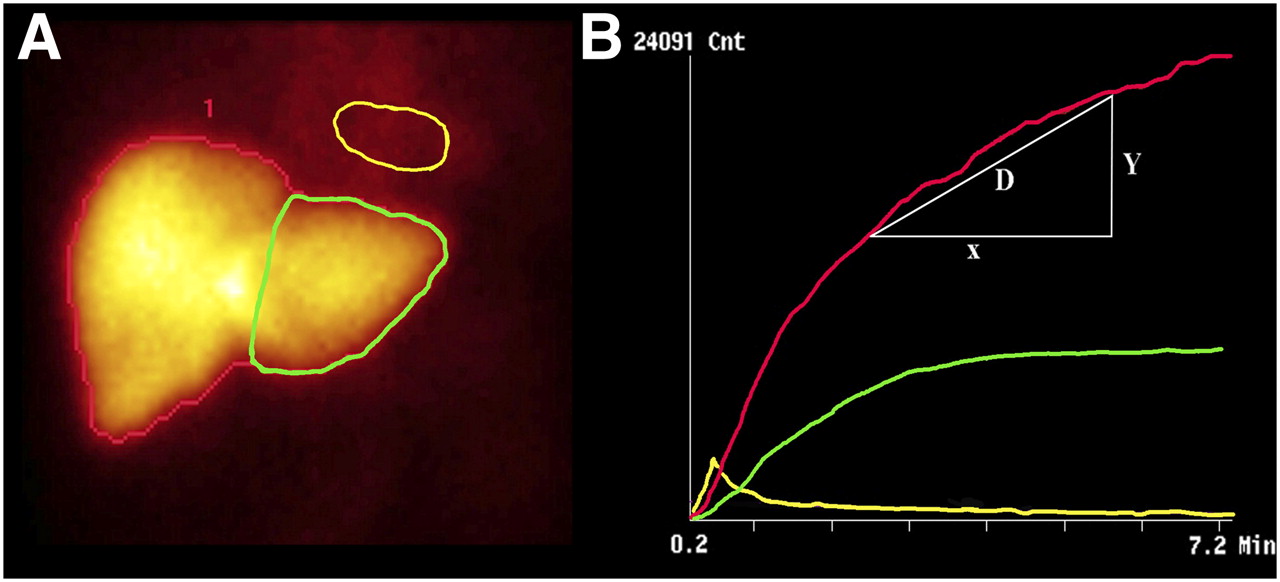
Dynamic image of planar HBS. (A) Example of summed HBS images from 150 to 350 s after intravenous injection of 99mTc-mebrofenin. ROI is drawn around entire liver (red line), mediastinum (blood pool; yellow line), and FRL (green line). (B) Blood-pool–corrected liver uptake time–activity curve. Liver uptake of mebrofenin is calculated as increase of blood-pool–corrected 99mTc-mebrofenin uptake (y-axis) per minute over a period of 200 s.
Alternative methods for determining liver function include hepatic extraction fraction, the time at which maximal hepatic radioactivity occurs (Tpeak), and the time required for peak activity to decrease by 50% (T1/2 peak) (77–79). The hepatic extraction fraction is calculated from the time–activity curves of the heart and liver by a deconvulsion analysis using a (modified) Fourier transform method (80).
Recently, application of 99mTc-mebrofenin SPECT for the assessment of regional liver function and functional liver volume has been described (76). The timing of the SPECT is a challenge when a dynamic tracer is used, which is taken up by the liver and subsequently excreted in the bile. The SPECT acquisition is therefore centered on the peak of the hepatic time–activity curve, when the amount of radioactivity within the liver is relatively stable. In patients with fast hepatic uptake, biliary excretion is already visible during the SPECT phase, disturbing the calculation of total and regional liver function and volume. Activity within the extrahepatic bile ducts is therefore removed, and activity in the intrahepatic bile ducts is replaced by the average count density of normal liver tissue. Functional liver volume is calculated by the outline extraction method (with a threshold of 30% of the maximal voxel count value). The FRL can be outlined manually on a low-dose CT scan linked to the SPECT images, with a contrast-enhanced CT scan used as a reference. The percentage of counts within the FRL is calculated by dividing counts within the FRL by the total counts within the entire liver. For calculation of actual FRL function, this percentage is multiplied by the total liver 99mTc-mebrofenin uptake rate as measured by the geometric mean dataset of the dynamic HBS.
HBS in Experimental Surgical Research
Measurement of liver function in small animals remains a challenge because many quantitative liver function tests require repetitive blood samples. Hepatic extraction fraction and T1/2 peak, measured by HBS, were used as a noninvasive method of evaluating hepatic function after ischemia–reperfusion injury to quantify the protective effect of new interventions on ischemia–reperfusion injury (81–83).
For the evaluation of functional regeneration in small animals, serial measurements over a relatively long time period are preferred. The use of the hepatic 99mTc-mebrofenin uptake rate measured by dedicated pinhole HBS has recently been validated in different rat models of liver regeneration (77). 99mTc-mebrofenin HBS proved to be an accurate, noninvasive tool for the measurement of liver function in the rat and enabled serial measurements within the same animal (77).
Clinical Use of HBS in Liver Surgery
Preoperative Assessment of Liver Function
The use of 99mTc-mebrofenin HBS for preoperative assessment of liver function in patients undergoing liver surgery was first described by Erdogan et al. (73). In 54 patients scheduled for liver resection, 99mTc-mebrofenin uptake measured by HBS strongly correlated with the ICG clearance test. Besides quantitative information, HBS provides visual information about the localization of liver segments with inferior function. Biliary excretion of 99mTc-mebrofenin is useful for preoperatively determining segmental cholestasis and for diagnosing postoperative biliary complications, such as bile leakage and biliary obstructions. Because of the possibility of determining regional liver function, HBS was validated as a preoperative method for estimating FRL function (74). In this relatively small patient study, preoperatively estimated FRL function correlated well with actual remnant liver function 1 d after resection.
Dinant et al. investigated the value of preoperative FRL function, measured by 99mTc-mebrofenin HBS, in predicting short-term outcome after partial liver resection (75). Forty-six patients with and without parenchymal disease were included in this study. Preoperative measurement of FRL function was more accurate than liver volume in predicting postoperative liver failure and liver failure–related mortality. A safe resection could be performed in patients with FRL uptake above 2.5%/min/m2 of body surface area, with a 3% chance of developing postoperative liver failure and liver failure–related mortality. However, in patients with FRL uptake below 2.5%/min/m2, the risk of postoperative liver failure increased to 56%. In high-risk patients undergoing major liver resection, receiver-operating-characteristic curve analysis yielded a similar FRL function cutoff of 2.69%/min/m2 (84). HBS takes into account the presence of underlying parenchymal liver disease, with compromised livers having significantly less liver function. Therefore, a single cutoff value for the prediction of liver failure suffices for both patients with a compromised liver and patients with a normal liver. In patients with an unknown quality of liver parenchyma, preoperative dynamic HBS proved more valuable then CT volumetry for the prediction of postoperative liver failure (75, 84).
In the 2 abovementioned studies published by Erdogan and Dinant, HBS parameters have been derived from a single-head γ-camera using only the anterior projection (75,84). Because of the anatomic position of the liver, the left hemiliver is situated more anteriorly, leading to an overestimation of segmental left liver function in the anterior projection. The increasing availability of dual-head rotating γ-cameras enables the calculation of a geometric mean dataset of the anterior and posterior projections, which is recommended for dynamic HBS in the future.
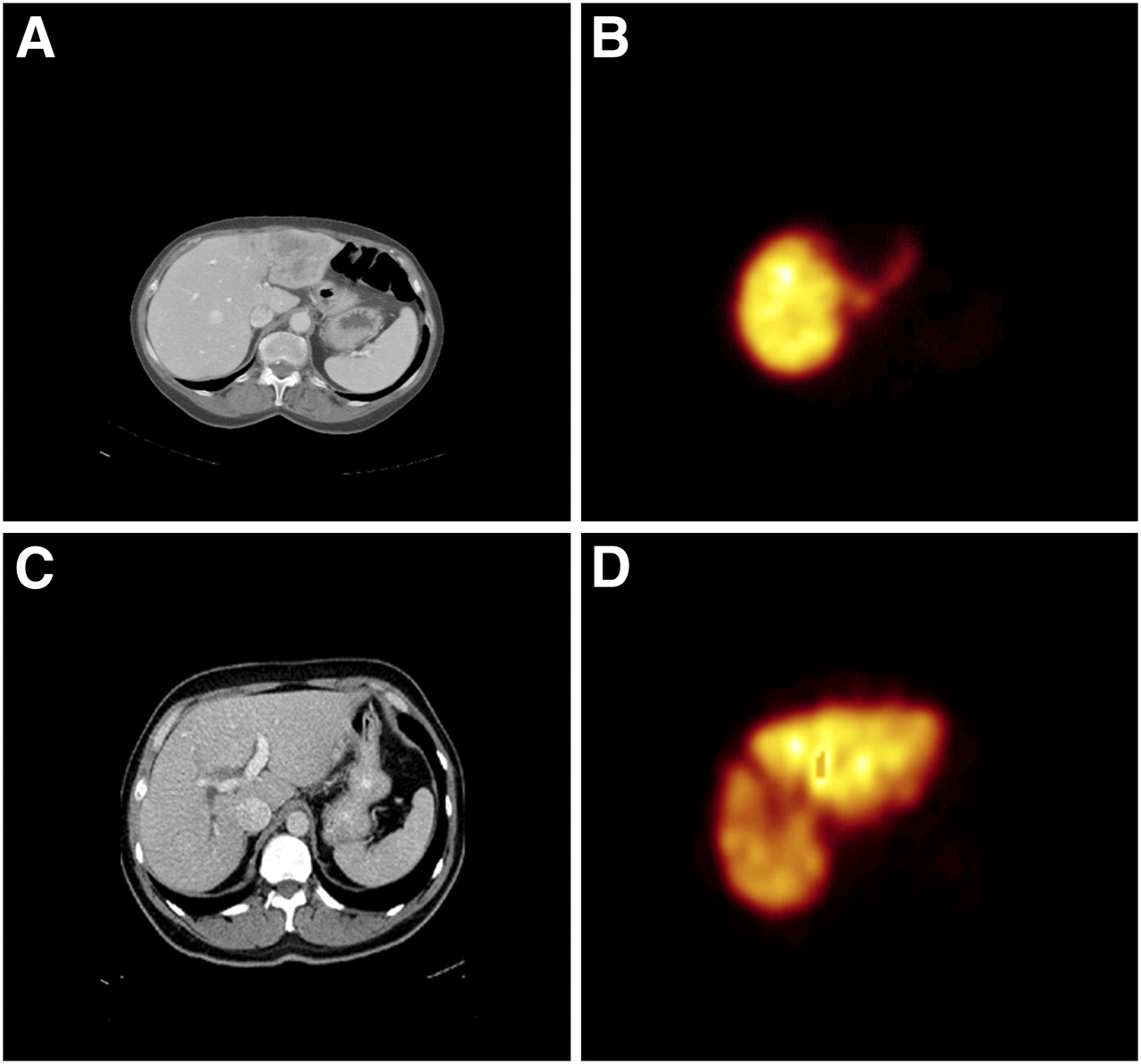
Although dynamic 99mTc-mebrofenin HBS has the possibility of measuring regional liver function, the 2-dimensional planar images lack the ability to assess detailed liver function on a segmental level. Modern SPECT/CT cameras combine dynamic 99mTc-mebrofenin HBS with additional SPECT and the anatomic information of the CT scan, thereby enabling measurement of segmental liver function and functional liver volume. A recent study including 36 patients demonstrated that 99mTc-mebrofenin SPECT provided valuable visible information on the distribution of liver function (Fig. 3.) (76) The results of functional liver volume measured by SPECT and morphologic volume measured by CT volumetry indicated that SPECT was an accurate method of measuring hepatic volume. FRL function measured by the combination of SPECT and dynamic HBS was able to accurately predict the actual function of the postoperative remnant liver.
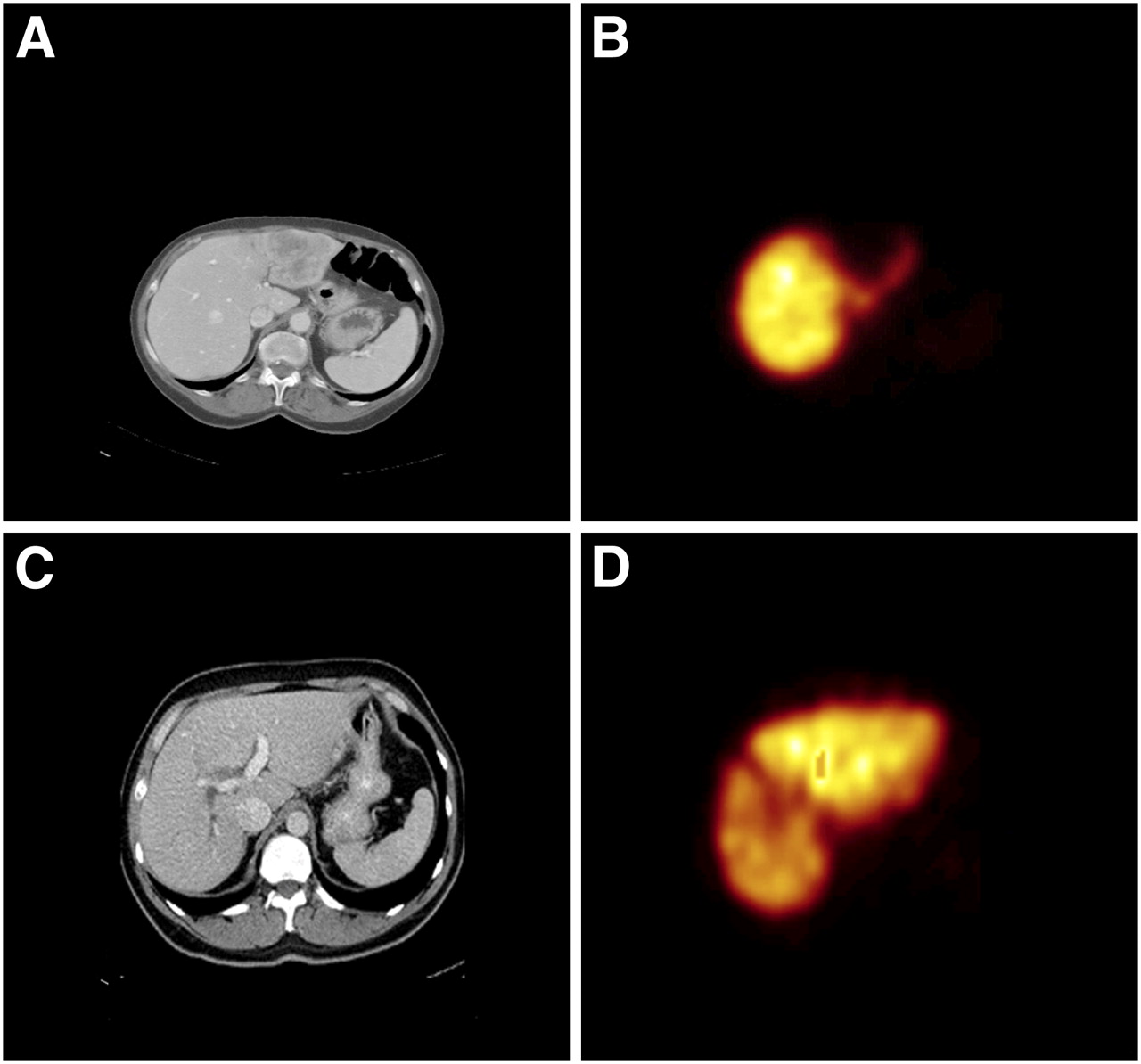
Two examples of 99mTc-mebrofenin SPECT, with CT scans on left and matching SPECT images on right. (A and B) Patient with large colorectal metastasis in left liver segments, visible on CT scan. SPECT image shows inhomogeneous distribution of mebrofenin, with decreased uptake in liver segments 2–4. (C and D) Patient with colorectal metastasis (not visible on this CT slide) in which tumor is compressing surrounding vessels and bile ducts, resulting in impaired liver function in segments 5–8.
Increase of Liver Function After PVE
The application of 99mTc-mebrofenin HBS after PVE is currently under investigation. HBS is one of the few quantitative liver function tests that has the ability to measure regional liver function and is therefore ideal for evaluating the functional increase in FRL after PVE. In addition, HBS could potentially be used to decide on candidates for PVE because of the ability to select patients with an increased risk of postoperative liver failure (75).
Postoperative Liver Regeneration
Bennink et al. compared the volumetric regeneration 3 mo after partial liver resection with the functional regeneration measured by HBS and ICG15 (74). There was a significant correlation between the ICG clearance and HBS. However, a weak association between functional recovery (HBS and ICG) and volumetric regeneration (CT volumetry) was observed. This discrepancy confirms that the mechanisms of functional recovery may be independent of those controlling volumetric regeneration.
Clinical Use of HBS in Liver Transplantation
Biliary complications and hepatic dysfunction due to graft rejection are major causes of postoperative morbidity and mortality in liver transplant recipients. Many studies have shown that HBS is an accurate, noninvasive technique for the diagnosis of biliary complications, including segmental and total biliary obstruction, as well as bile leakage in adult and pediatric transplantation patients (85–88). The efficacy of HBS for detection of graft dysfunction because of rejection is unclear. Graft rejection is usually diagnosed by liver biopsy. Brunot et al. demonstrated a close relation between early biopsy results and liver uptake function measured by HBS, implying that HBS is valuable in distinguishing graft rejection from cholestasis (89). In contrast, others reported that HBS can distinguish between normal grafts and those experiencing rejection or cholestasis but not between biliary complications and rejection (85,90).
In heterotopic auxiliary liver transplantation, the native liver is left in situ and a partial liver graft is transplanted elsewhere in the abdominal cavity. It has occasionally been applied in patients with fulminant liver failure, in whom the native liver is expected to recover and regain function. Individual assessment of graft and native liver is difficult because most function tests measure total liver function. HBS has the unique ability to perform functional assessment of graft and native liver separately (91,92).
Because of an increased shortage of cadaveric liver grafts, living donor liver transplantation is used to expand the organ pool. In living donor liver transplantation, a left or right hepatectomy is performed on a living donor. The regeneration capacity in donors after living donor liver transplantation was investigated using HBS (93). As described by others, that study indicated that accelerated recovery of organ function is an early compensatory mechanism after reduction of organ volume (93). To date, no studies have been published using HBS for the preoperative assessment of liver function in the donor in living donor liver transplantation.
DISCUSSION
99mTc-GSA scintigraphy and 99mTc-mebrofenin HBS are simple techniques that can be implemented in every hospital with a nuclear medicine department. Both methods are applicable in patients with parenchymal liver disease, which is of increasing importance in view of the increasing number of patients presenting with parenchymal liver disease due to neoadjuvant chemotherapy or aspects of Western lifestyle such as obesity, alcohol consumption, and sexually transmitted diseases.
99mTc-GSA scintigraphy and 99mTc-mebrofenin HBS are based on 2 different principles. 99mTc-GSA scintigraphy measures the binding of 99mTc-GSA to its receptor expressed on hepatocytes. A decreased hepatic 99mTc-GSA uptake can be caused by a reduction in the 99mTc-GSA binding affinity (as seen in cholestasis (34)), a reduction in the amount of asialoglycoprotein receptors per hepatocyte, or a decrease in the number of hepatocytes (as seen in cirrhosis (94)). Because 99mTc-GSA is not excreted into the bile, 99mTc-GSA scintigraphy cannot be used to diagnose biliary complications after liver surgery or transplantation. HBS measures the hepatic uptake and excretion of 99mTc-mebrofenin and therefore has the ability to also visualize the biliary system. Uptake of 99mTc-mebrofenin can be influenced by hepatic blood flow, hypoalbuminemia, and high concentrations of bilirubin (69). Because the hepatic uptake of many substances is influenced by the same factors, it still reflects liver function under these conditions.
Compared with other dynamic quantitative liver function tests such as the ICG clearance test, 99mTc-GSA scintigraphy and 99mTc-mebrofenin HBS have the advantage of being able to measure both total and regional liver function, enabling functional assessment of specifically the FRL. For this reason, preoperative 99mTc-GSA scintigraphy and HBS are accurate methods for preoperative prediction of postoperative complications (31,42,48,75,84) and for follow-up of FRL function after PVE.
Although both nuclear imaging techniques are applicable for the assessment of liver function in small laboratory animals, 99mTc-GSA SPECT is preferred for the noninvasive assessment of liver functional volume. Dynamic SPECT acquisitions with 99mTc-mebrofenin are difficult using dedicated animal pinhole γ-cameras because of the longer acquisition time per frame and faster hepatic uptake of 99mTc-mebrofenin in rats.
Although many studies have proven the value of nuclear imaging in liver surgery and transplantation, these techniques are not widely used. 99mTc-GSA scintigraphy is mainly used in Japan, whereas its use is not approved in Europe and the United States. In addition, 99mTc-GSA scintigraphy uses many different, sometimes complex, parameters (Tables 1 and 2), making comparison of studies difficult. The application of 99mTc-mebrofenin HBS in liver surgery is relatively new, and only a few clinical trials have been performed. Clinical trials on larger patient populations are required to confirm the value of 99mTc-mebrofenin HBS for the preoperative assessment of liver function and the postoperative evaluation of complications and liver regeneration.
CONCLUSION
Both 99mTc-GSA scintigraphy and 99mTc-mebrofenin HBS are noninvasive, reliable techniques that provide visual and quantitative information on both total and regional liver function. Both tests are applicable in patients with normal livers and patients with compromised livers. These features render both 99mTc-GSA scintigraphy and 99mTc-mebrofenin HBS useful tests for the assessment of liver function in liver surgery and liver transplantation.
Footnotes
-
COPYRIGHT © 2010 by the Society of Nuclear Medicine, Inc.
-
Learning Objectives: On successful completion of this activity, participants should be able to describe (1) the relevance of assessment of liver function in liver surgery and transplantation; (2) the technical background of 99mTc-GSA scintigraphy and 99mTc-mebrofenin hepatobiliary scintigraphy; and (3) the role of 99mTc-GSA scintigraphy and 99mTc-mebrofenin hepatobiliary scintigraphy for preoperative assessment of future remnant liver function, follow-up after preoperative portal vein embolization, and evaluation of postoperative liver regeneration.
-
Financial Disclosure: The authors of this article have indicated no relevant relationships that could be perceived as a real or apparent conflict of interest.
-
CME Credit: SNM is accredited by the Accreditation Council for Continuing Medical Education (ACCME) to sponsor continuing education for physicians. SNM designates each JNM continuing education article for a maximum of 1.0 AMA PRA Category 1 Credit. Physicians should claim only credit commensurate with the extent of their participation in the activity.
-
For CE credit, participants can access this activity through the SNM Web site (http://www.snm.org/ce_online) through May 2011.
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.
- 79.↵
- 80.↵
- 81.↵
- 82.
- 83.↵
- 84.↵
- 85.↵
- 86.
- 87.
- 88.↵
- 89.↵
- 90.↵
- 91.↵
- 92.↵
- 93.↵
- 94.↵
- Received for publication August 24, 2009.
- Accepted for publication December 4, 2009.





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Repurposing 99mTc-Mebrofenin as a Probe for Molecular Imaging of Hepatocyte Transporters
- Accurate Estimation of Functional Liver Volume Using Gd-EOB-DTPA MRI Compared to MDCT/99mTc-SPECT Fusion Imaging
- The Role of Organic Anion Transporters in Diagnosing Liver Diseases by Magnetic Resonance Imaging
- MRI: the new reference standard in quantifying hepatic steatosis?
- Copolymer-Based Hepatocyte Asialoglycoprotein Receptor Targeting Agent for SPECT
- Quantitative Assessment of Hepatic Function During Liver Regeneration in a Standardized Rat Model