


Abstract
Recent publications described many discrepant findings about thyroid “stunning” after the administration of 131I diagnostic activities to patients with differentiated thyroid carcinoma. Stunning may play a major role in reducing the therapeutic efficacy of high 131I activities given for ablation therapy. Methods: Participation in a multicenter study to investigate differences in iodine biokinetics in the hypothyroid state and after the application of recombinant human thyroid-stimulating hormone enabled us to study quantitative changes in thyroid iodine biokinetics after the administration of 74 MBq of 131I twice within 6 wk and an ablation activity of 3–4 GBq 7–12 d after the second diagnostic administration of 131I in 6 patients. Results: The uptake and half-life of the first 74 MBq of 131I were significantly reduced to a mean of 44% and a mean of 51%, respectively, after the second diagnostic administration and further reduced to a mean of 40% and a mean of 30%, respectively, during ablation therapy. The residence times were reduced to 25% in the second dosimetric assessment and to 10% during therapy compared with the value in the first assessment. For one patient, an estimated absorbed dose as high as 38 Gy was found in the first diagnostic study. The mean dose for all patients after the first assessment was 15 Gy; after each further assessment, the dose was reduced according to the decrease in residence time. Conclusion: This study shows a severe impact of 74 MBq of 131I on the biokinetics of thyroid remnants during subsequent radioiodine therapy.
- differentiated thyroid cancer
- radioiodine therapy
- recombinant human thyroid-stimulating hormone
- dosimetry
- stunning
It is well known that the administration of diagnostic activities of radioiodine may influence iodine biokinetics in the thyroid during subsequent radioiodine ablation therapy for differentiated thyroid carcinoma (DTC). The phenomenon usually is called “stunning,” as it is assumed to be a temporary malfunction of the thyroid tissue attributable to moderate nonablative radiation doses in the range of a few Gy to some 10 Gy. The importance of the effect is that it may influence the rate of success of consecutive radioiodine treatments for the ablation of DTC.
The topic has been discussed in many publications (1–20). Some groups described an impact on the visibility of lesions in posttherapeutic scans (9–11,19), disregarding the fact that it depends on a variety of factors, such as γ-camera sensitivity, time after radioiodine administration, or thyroid-stimulating hormone (TSH) level. Some authors focused on the effect of diagnostic activity on the results of posttherapeutic scanning (2–5) or on the remnant ablation dose (3–6). Others investigated the outcome, defined as the thyroid remnant ablation rate, showing different percentages of ablation failures (12,17,19). Hilditch et al. (20) showed that there is a reduced uptake of therapeutic radioiodine in the thyroid bed after the administration of 120 MBq of 131I for diagnostic scans compared with the results for a group of patients who received 123I for diagnostic scans.
To our knowledge, nobody has yet provided evidence that the impact of moderate doses really is temporary or has suggested a time frame for full regeneration. The underlying mechanisms at the cellular level are not fully understood, and it has not yet been proven whether the concern is temporary stunning or nonreversible destruction. However, care must be taken not to reduce the chances of success of radioiodine ablation treatments because of unconsidered dose reductions attributable to moderate pretherapeutic doses.
Participation in an international multicenter dosimetry study (21) and a follow-up study enabled us to investigate quantitative changes in thyroid iodine biokinetics after the administration of 74 MBq of 131I twice within 6 wk and an ablation activity of 3–4 GBq 7–12 d after the second diagnostic administration of 131I in 6 patients.
Originally, the first study was performed to determine the correction factor to be applied to the 131I activity for DTC remnant ablation therapy with recombinant human TSH (rhTSH) in euthyroid patients versus conventional subsequent hypothyroid conditions after thyroid hormone withdrawal (21). Because the findings of the study (21) showed evidence of reduced remnant residence times in hypothyroidism, we analyzed data for a subset of 5 patients investigated at our site in more detail. In addition, a further study was initiated with dose assessments in reverse order (conventional hypothyroid conditions versus euthyroid conditions first and rhTSH administration second).
The objectives of this work were to verify whether the reduced residence times were attributable to an effect of rhTSH and to quantify the potential contribution of stunning. Furthermore, the effect of the 2 preceding diagnostic procedures on the biokinetics of therapeutic 131I activities for thyroid remnants was analyzed.
MATERIALS AND METHODS
Patients
Both studies were approved by the local ethics committee and by German radiation protection authorities. Six patients (2 male and 4 female) who had DTC and who were referred to our center shortly after surgery were enrolled in the studies. Five patients (P1–P5) initially received a diagnostic activity of 74 MBq of 131I under euthyroid conditions after 2 or 3 injections of rhTSH (Thyrogen; Genzyme); this step was followed by a dosimetric study. After the first dosimetric study, thyroid hormone suppressive therapy was discontinued to achieve a TSH level of higher than 30 mU/L. At 4–6 wk after administration of the first diagnostic activity of 74 MBq of 131I, the patients received a second diagnostic activity of 74 MBq of 131I; this step was followed by a second dosimetric assessment. After 7–9 d, 3–4 GBq of 131I were administered for remnant ablation, according to our local standard operational procedures. All 131I activities (capsules) were given orally. A schematic representation of the time lines for the studies is shown in Figure 1.

Time lines for studies. THST = thyroid hormone suppressive therapy.
One patient (P6) participated in the second study with diagnostic assessments in reverse order (first hypothyroid and then euthyroid). For this patient, an ablation activity of 3.85 GBq of 131I was administered 12 d after the second dosimetric assessment. The time interval was longer because another course of exogenous TSH stimulation was needed.
We had planned to enroll another 2 patients but, after finalizing the assessment of patient P6, we discontinued the second study for ethical reasons, as potentially insufficient ablation doses were expected.
A complete set of patient data, including demographics and data on TNM stage, rhTSH regimen, TSH and thyroglobulin levels, and study time intervals, is shown in Table 1. Five of the patients had more than 1 lesion after surgery.
Patient Data
Imaging
Spot images of the neck were acquired to determine biokinetics. For the diagnostic assessments, measurements were obtained at nominal time points of 6, 24, 48, and 120–144 h after administration. After therapy, at least 3 scintigrams were acquired starting at 48 h after 131I administration and ending at 6–14 d after 131I administration.
The γ-camera used was a standard dual-head camera (Bodyscan; Siemens) equipped with a high-energy general-purpose collimator. The acquisition time was 300 s (128 × 128 matrix), with a 15% window centered on the 364-keV peak of 131I. The pixel size of the camera for a 128 × 128 matrix was 4 mm. For quality control purposes, a 133Ba source with an activity of 1.85 MBq was scanned together with the patient. Additionally, an acrylic calibration phantom (150 × 50 × 50 mm) containing 2 separate flat 131I sources (source diameter, 25 mm; source distance, 100 mm; thickness, <1 mm; attenuation layer on the top and on the bottom of the sources, 25 mm; activities, 1.85 and 5.55 MBq) was placed on the patient bed and scanned with the same parameters as the patient.
The geometric mean net counts were 5.8 counts of 131I per kilobecquerel in the lesion for a 5-min scan, corresponding to 430 net counts for an uptake of 0.1% in the diagnostic assessments.
Dosimetry
The computer code NUCLIDOSE (22) was used to draw regions of interest (ROIs) around the remnant and the sources and to copy them identically to subsequent images. Representative ROIs adjacent to the respective remnant regions were used for background correction. The counts used for the dosimetric calculations were the geometric means of anterior and posterior counts in the remnant regions corrected for the background counts per pixel as calculated from the background region.
Uptake was calculated by use of the camera efficiency obtained from the phantom measurements by taking into account the attenuation in the phantom. A transmission factor of 0.3 was applied to correct for the attenuation in the neck at an 11-cm neck thickness. Deviations from that “standard” neck thickness resulted in errors of 5% per centimeter only and were neglected.
The effective half-lives were evaluated by linear regression to the logarithms of the uptake values at nominal times 24 h after administration or later. The remnant residence times for the dosimetric assessments were calculated as the sum of the integrals of trapezoidal functions up to 24 h and the exponential decay function obtained from the regression after 24 h.
For therapeutic assessment, the 24-h uptake was determined by extrapolation of the deduced decay function. The residence time for the therapeutic course was calculated as the residence time of the first diagnostic course multiplied by the ratios of the therapeutic 24-h uptake to the 24-h uptake of the first diagnostic scan and the therapeutic half-life to the half-life of the first diagnostic scan.
To calculate the order of magnitude of the radiation doses applied to the thyroid remnants, it was necessary to estimate the remnant masses. At present, there is no validated method for determining the masses of thyroid remnants after surgery exactly. We adopted a previously described method (7,23) to estimate the mass from the number of pixels significantly above the background level in the scintigraphic image and the pixel size by assuming a mean thickness of the remnant of 2 mm. For determination of the number of pixels, a ROI was drawn around the lesion. A second ROI representing the background was drawn adjacent to the lesion ROI to determine the average background counts. From the lesion ROI, the number of pixels with the number of counts exceeding the maximum of either twice the background or the sum of the background plus 3 times the square root of the background was determined.
An analysis of the remnant regions for all patients and all time points for all scans showed systematically smaller lesion areas in the second dosimetric assessment. At only a few days after the second assessment, however, the lesion area values during therapy were almost identical to the values in the first assessment. Because this effect is not considered to be a real change in mass from course to course but may be dependent on specific lesion uptake and on the total amount of the administered activity, we decided to calculate the lesion mass values from the average of the lesion area values of the 48-h scans, which were the only scans obtained at identical time points for the 2 diagnostic courses and the therapy course.
The doses delivered to the lesions were calculated from the average mass values, the corresponding residence times, and the S factors, as published by the MIRD Committee of the Society of Nuclear Medicine (24).
The reductions in uptake, half-life, and residence time observed during the second diagnostic assessment and during the therapeutic assessment were calculated as the ratios of the values for those parameters during those assessments to the values during the first diagnostic assessment.
RESULTS
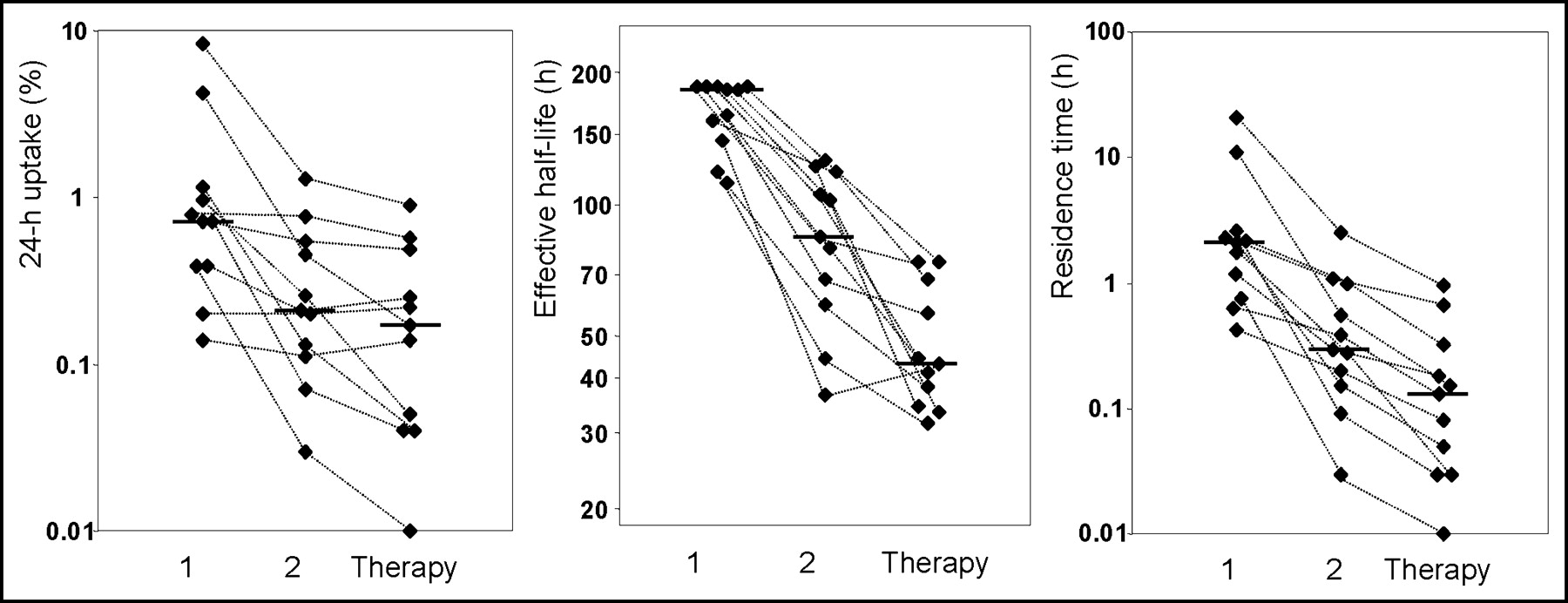
The results of the scan assessment are shown in Table 2. The iodine kinetics in the remnants (lesion 1 [L1] or lesion 2 [L2]) in the 2 diagnostic courses and the therapeutic course are shown for patients P1–P6. Uptake and half-life were reduced to 44% (mean; range, 8%–98%; P < 0.001, as determined by the Wilcoxon test) and 51% (mean; range, 26%–76%; P < 0.001), respectively, in the second diagnostic assessment and to 40% (mean; range, 3%–107%; P < 0.001) and 30% (mean; range, 18%–43%; P < 0.001), respectively, during therapy.
Uptake at 24 Hours and Effective Half-Life of 131I
Table 3 shows the residence times calculated from the data obtained. The residence times were reduced to 25% (mean; range, 4%–63%; P < 0.001) in the second course and to 10% (mean; range, 1%–29%; P < 0.001) during therapy. The lesion masses shown in Table 3 are the average values for the therapeutic course and the 2 diagnostic courses at 48 h.
Lesion Residence Times, Estimated Masses, and Doses
The doses delivered to the thyroid remnants during the diagnostic procedures reached a maximum of 38 Gy for 1 patient (P5, L1) in the first diagnostic assessment. The resulting dose after 2 courses of 74 MBq of 131I diagnostic imaging for this patient was about 43 Gy. The mean value for all patients in the first assessment was 15 Gy, with a minimum of 4 Gy.
Figure 2 shows the 24-h uptake, the effective half-life, and the residence time for the 11 lesions during the 2 diagnostic courses and during therapy. The dotted lines connect the data points for each lesion. The horizontal bars indicate the median for each data set.
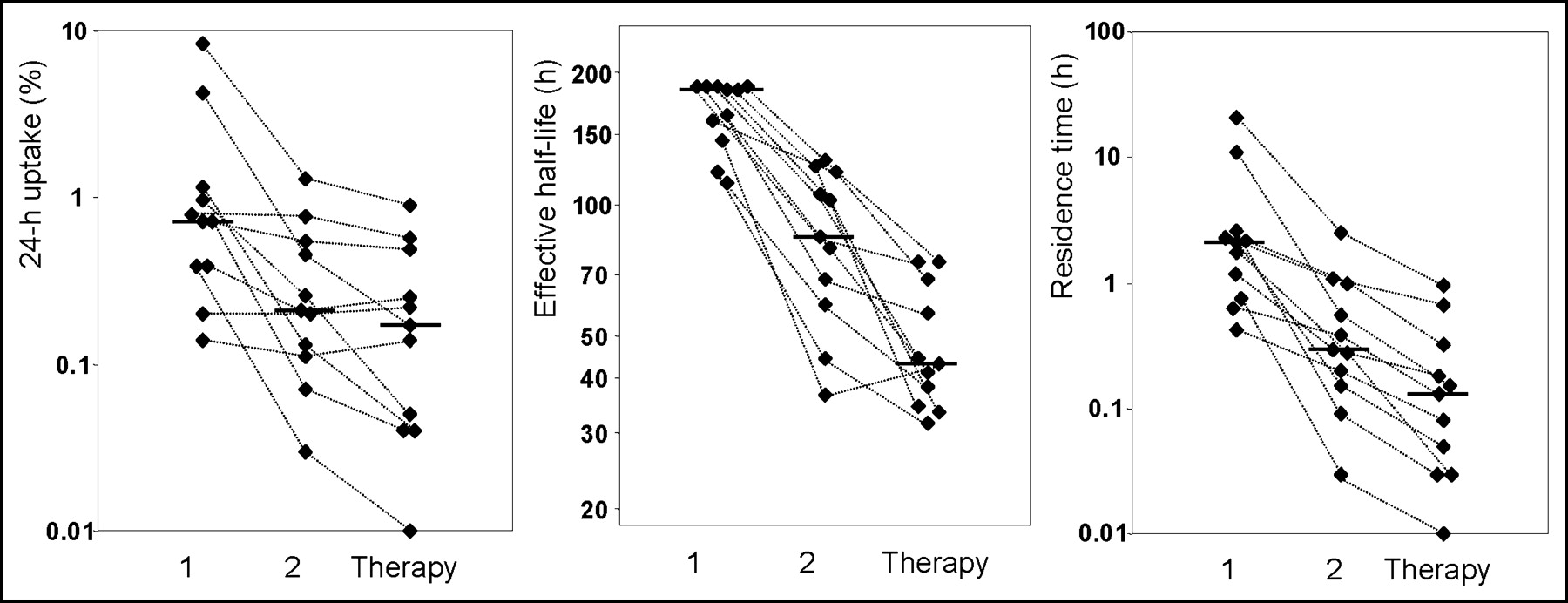
Uptake at 24 h, effective half-life, and residence time for 11 lesions during diagnostic courses 1 and 2 and during therapy. The dotted lines connect the data points for each lesion; the horizontal bars indicate the medians.
Figure 3 shows an example (patient P6) of the decrease in the 48-h uptake in the first (Fig. 3A) and second (Fig. 3B) diagnostic assessments and at 48 h after the administration of therapeutic activity (Fig. 3C). The gray scale of the therapeutic image (Fig. 3C) was adjusted to the administered activity.
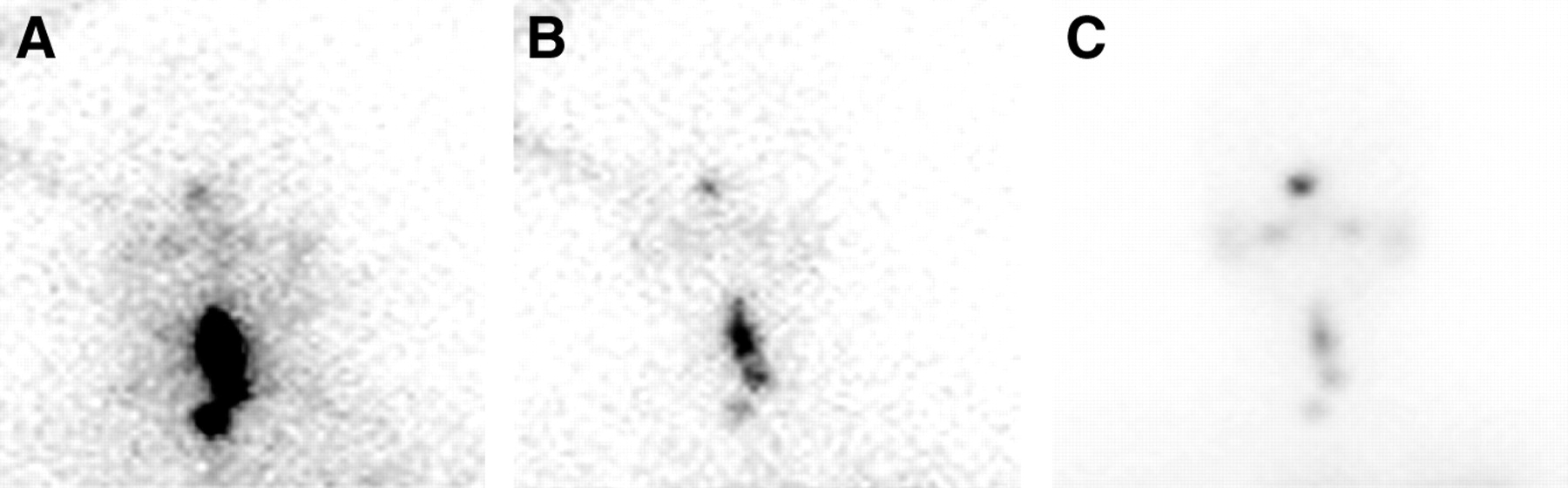
Neck scans for patient P6 at 48 h during diagnostic course 1 (A), diagnostic course 2 (B), and therapy (C). For the therapy scan, the gray scale was adjusted to the diagnostic activity. The increased number of counts in the upper left corner in panels A and B is an artifact caused by septal penetration of the photons emitted by the 133Ba quality control phantom, which was scanned together with the patient.
The results of the study show clear differences in iodine kinetics between the first and second diagnostic imaging procedures and a further reduction in the ability of remnants to take up and store iodine during the therapy course.
Patients P1, P3, P4, and P5 showed complete remission after ablation (thyroglobulin level, less than 0.2 ng/mL; no evidence of pathologic 131I uptake in subsequent diagnostic scans). Patients P2 and P6 had positive follow-up scans, with 290 MBq of 131I after 6 mo (uptake limited to the thyroid bed in lesions L1 and L2 in both patients was still visible), resulting in the need for a second course of therapy with 131I.
DISCUSSION
In vitro experiments showed that stunning of iodide transport occurs after 131I irradiation of cultured thyroid cells (25). The results of patient studies investigating the impact of diagnostic activity on iodine kinetics in thyroid remnants range from the absence of any effect to the observation of reduced uptake comparable to that found in this study (4,6,14). The decrease in therapeutic uptake is expected to depend on the timing of the diagnostic administration. Some authors (14,16,17) have focused on the influence on thyroid lesion uptake during therapy a few days after diagnostic dosimetry, when about one-third of the dose from the tracer already has been deposited. After some weeks, the dose and the impact may be higher. On the other hand, the tissue may recover.
The special design of the present study enabled us to show for the first time significant effects on both uptake and effective half-life in thyroid tissue 4–6 wk after a diagnostic scan in the absence of any impact of therapeutic activities on iodine kinetics. This means that at least up to 4 wk after the administration of a diagnostic activity even as low as 74 MBq, the dose delivered to a thyroid remnant for ablation therapy may be reduced. This time interval appears to be long for an acute transient effect of moderate doses. Furthermore, the reduction in residence time attributable to diagnostic activity was confirmed by the results of the iodine kinetic measurements obtained during therapy after the second diagnostic assessment.
The masses (shown in Table 3) and, as a consequence, the calculated absolute radiation doses must be considered less accurate than the uptake values and the corresponding effective half-lives. For patients with a mean remnant thickness exceeding the presumed value of 2 mm, masses are underestimated and doses are overestimated. If the mean remnant thickness is smaller, then the masses are smaller. The doses, however, are not correspondingly higher, because an increasing fraction of the dose is deposited outside the thyroid tissue, as the mean range of the radiation exceeds the dimensions of the residual tissue (26). Therefore, it is very unlikely that doses are significantly underestimated.
For one patient, a dose estimate as high as 38 Gy was found in the first diagnostic study. The mean dose for all patients after the first assessment was 15 Gy; after each further assessment, the dose was reduced according to the decrease in residence time. We suspect that reduced uptake values and half-lives are manifestations of permanent destruction of tissue and not of stunning.
In all likelihood, this effect will occur for any tissue of thyroid origin, although our results do not prove that the same results can be found for metastatic tissue. As a consequence, further studies are warranted to determine whether the administration of 131I for diagnostic applications degrades the probability of total ablation during subsequent radioiodine ablation therapy. A shortened time interval between diagnostic procedures and therapy may decrease the rate of stunning.
The sharp decrease in the residence times from course to course raises suspicion that, in particular, well-differentiated tissues are affected. This situation may result in potential negative selection of susceptible cells, possibly leading to dedifferentiation of benign thyroid or tumor tissue attributable to radiation damage during the course of the disease. There is proof, however, that in a mixed population of thyroid cells, there are a variety of levels of expression of the sodium iodide symporter, resulting in different radioiodine uptake levels in the same patient or lesion (27–29).
As the study originally was set up to analyze the difference in therapeutic activities to be administered to euthyroid and hypothyroid patients after a diagnostic scan, we could not rule out a direct effect of the use of rhTSH after evaluation of the first 5 patients. These patients were scanned after the administration of rhTSH first and were withdrawn from thyroid hormones for the second course of diagnostic scanning. Therefore, for patient P6, the order was reversed (withdrawal first and rhTSH second). This patient (P6) showed the same trend as the other 5 patients, as shown in Table 2.
Originally, we had planned to enroll 3 patients in the reverse-order study. However, there seemed to be a very high probability that additional patients to be recruited would show the same unfavorable results, leading to potentially insufficient ablation doses; therefore, no further patients were included for ethical reasons.
With only 1 patient in the second study and with the observed high variability in the residence time reduction for the first group of patients (patients P1–P5), it was not possible to deduce statistically significant differences between the studies. The effect of stunning is dominant and masks a potential influence of rhTSH on iodine kinetics. An ongoing multicenter trial comparing conventional ablation therapy to ablation therapy with rhTSH may provide further data on the influence of rhTSH on iodine kinetics.
CONCLUSION
Even diagnostic activities as low as 74 MBq may deliver radiation doses to thyroid remnants that are not negligible compared with the target dose of 300 Gy (30,000 rads), which is believed to be crucial for successful ablation after thyroidectomy. A significant reduction in the ability of the tissue to take up and store iodine is the most obvious adverse effect of the radiation damage. In the light of our findings, preablation diagnostic scanning with 131I can no longer be recommended.
Alternatively, 123I could be used for investigations to rule out any radiation-induced effect because of its much lower radiation dose to thyroid tissue. A prospective study comparing diagnostic 123I scanning with rhTSH versus conventional 131I scintigraphy under hypothyroid conditions is under way.
Acknowledgments
We thank Stephen Thomas, University of Cincinnati, for his review of the calculations and his valuable support for thyroid dosimetry and Cornelia Schmutzler, Universitätsklinikum Charité, Berlin, Germany, for giving us more insight into iodide transport mechanisms at the cellular level.
Footnotes
Received Sep. 3, 2003; revision accepted Dec. 8, 2003.
For correspondence or reprints contact: Michael Lassmann, PhD, Klinik und Poliklinik für Nuklearmedizin der Universität Würzburg, Josef-Schneider-Str. 2, D-97080 Würzburg, Germany.
E-mail: lassmann{at}nuklearmedizin.uni-wuerzburg.de
REFERENCES
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- The Role of Pretherapy Quantitative Imaging and Dosimetry in Radioiodine Therapy for Advanced Thyroid Cancer
- Analysis of Residence Time, Effective Half-Life, and Internal Dosimetry Before Radioiodine Therapy
- Dosimetry and thyroid cancer: the individual dosage of radioiodine
- Radiation-Induced Thyroid Stunning: Differential Effects of 123I, 131I, 99mTc, and 211At on Iodide Transport and NIS mRNA Expression in Cultured Thyroid Cells
- The success rate of I-131 ablation in differentiated thyroid cancer: comparison of uptake-related and fixed-dose strategies
- Role of Radioactive Iodine for Adjuvant Therapy and Treatment of Metastases
- Reduced Iodide Transport (Stunning) and DNA Synthesis in Thyrocytes Exposed to Low Absorbed Doses from 131I In Vitro
- A new functional parameter measured at the time of ablation that can be used to predict differentiated thyroid cancer recurrence during follow-up
- The So-Called Stunning of Thyroid Tissue
- European consensus for the management of patients with differentiated thyroid carcinoma of the follicular epithelium.
- Juvenile differentiated thyroid carcinoma and the role of radioiodine in its treatment: a qualitative review
- The Evolving Role of 131I for the Treatment of Differentiated Thyroid Carcinoma