


Abstract
The aims of this study were to determine whether responses in myocardial blood flow (MBF) to the cold pressor testing (CPT) method noninvasively with PET correlate with an established and validated index of flow-dependent coronary vasomotion on quantitative angiography. Methods: Fifty-six patients (57 ± 6 y; 16 with hypertension, 10 with hypercholesterolemia, 8 smokers, and 22 without coronary risk factors) with normal coronary angiograms were studied. Biplanar end-diastolic images of a selected proximal segment of the left anterior descending artery (LAD) (n = 27) or left circumflex artery (LCx) (n = 29) were evaluated with quantitative coronary angiography in order to determine the CPT-induced changes of epicardial luminal area (LA, mm2). Within 20 d of coronary angiography, MBF in the LAD, LCx, and right coronary artery territory was measured with 13N-ammonia and PET at baseline and during CPT. Results: CPT induced on both study days comparable percent changes in the rate × pressure product (%ΔRPP, 37% ± 13% and 40% ± 17%; P = not significant [NS]). For the entire study group, the epicardial LA decreased from 5.07 ± 1.02 to 4.88 ± 1.04 mm2 (ΔLA, −0.20 ± 0.89 mm2) or by −2.19% ± 17%, while MBF in the corresponding epicardial vessel segment increased from 0.76 ± 0.16 to 1.03 ± 0.33 mL · min−1 · g−1 (ΔMBF, 0.27 ± 0.25 mL · min−1 · g−1) or 36% ± 31% (P ≤ 0.0001). However, in normal controls without coronary risk factors (n = 22), the epicardial LA increased from 5.01 ± 1.07 to 5.88 ± 0.89 mm2 (19.06% ± 8.9%) and MBF increased from 0.77 ± 0.16 to 1.34 ± 0.34 mL · min−1 · g−1 (74.08% ± 23.5%) during CPT, whereas patients with coronary risk factors (n = 34) revealed a decrease of epicardial LA from 5.13 ± 1.48 to 4.24 ± 1.12 mm2 (−15.94% ± 12.2%) and a diminished MBF increase (from 0.76 ± 0.20 to 0.83 ± 0.25 mL · min−1 · g−1 or 10.91% ± 19.8%) as compared with controls (P < 0.0001, respectively), despite comparable changes in the RPP (P = NS). In addition, there was a significant correlation (r = 0.87; P ≤ 0.0001) between CPT-related percent changes in LA on quantitative angiography and in MBF as measured with PET. Conclusion: The observed close correlation between an angiographically established parameter of flow-dependent and, most likely, endothelium-mediated coronary vasomotion and PET-measured MBF further supports the validity and value of MBF responses to CPT as a noninvasively available index of coronary circulatory function.
The vascular endothelium plays an important role in the regulation of coronary circulatory function and in preserving the structural and functional integrity of the vascular wall (1). The antithrombotic and antiatherosclerotic effect of the endothelium is essential for normal function (1,2). An abnormal endothelium-dependent coronary vasomotion has therefore been found to be an independent predictor of coronary artery disease (CAD) and of coronary events (3–5). Several invasive approaches for the evaluation of endothelial function are available (1). They require quantitative angiography and intracoronary flow velocity probes for measuring changes in coronary flow in response to acetylcholine-stimulated endothelial release of nitric oxide (NO) or flow-dependent changes of the lumen of the epicardial conduit vessels (1,6). For the latter approach, changes in coronary blood flow are induced either by intracoronary administration of papavarine or adenosine or by sympathetic stimulation with cold pressor testing (CPT) (1–4,6).
Changes in the luminal area (LA) of the epicardial vessels during CPT were found to significantly correlate with changes in coronary blood flow, suggesting that information on flow-dependent endothelium-mediated coronary vasomotor function can be derived from measurements of coronary blood flow (6–8). However, the invasive nature of the measurements precludes a more widespread clinical use (7–10). Measurements of myocardial blood flow (MBF) and its response to sympathetic stimulation with CPT are now possible with PET and may offer a noninvasive means of probing endothelium-dependent coronary vasomotion and thus provide important diagnostic and prognostic information (6,11,12).
The aims of this study were to define (a) the relationship between hemodynamic responses to CPT and LA changes of the epicardial conduit vessels; (b) responses of MBF to increases in the rate × pressure product (RPP); and (c) the correlation between responses of the epicardial conduit vessel LA, as a measure of flow-dependent vasomotion, and the responses of MBF as determined with PET.
MATERIALS AND METHODS
Study Population and Study Design
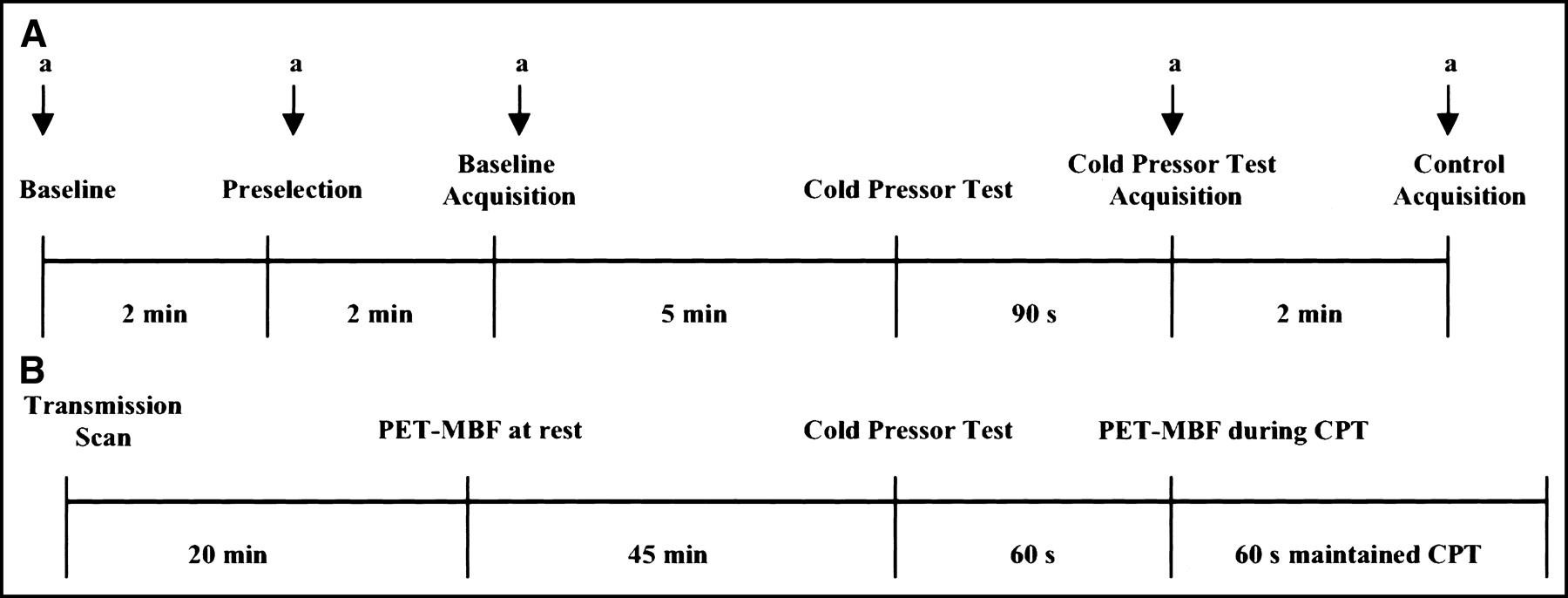
Fifty-six patients (mean age, 57 ± 6 y; 33 men, 23 women) referred for diagnostic cardiac catheterization for evaluation of atypical chest pain and with normal coronary angiograms, as defined by the absence of angiographic evidence for CAD, were studied. Each patient underwent quantitative coronary angiography (QCA) at baseline and during CPT for measurement of the epicardial LA (9,10,13) and, within 20 d (mean 11 ± 6 d), PET measurements of MBF at baseline and during CPT (14,15) (Fig. 1). All patients had normal wall motion on left ventriculography (n = 45) or on echocardiography (n = 11). None had a history of acute coronary syndrome including myocardial infarction or lead hypertrophic obstructive and nonobstructive cardiomyopathy, congestive heart failure, malignant hypertension, valvular heart disease, or significant endocrine, hepatic, renal, or inflammatory disease. Four of 16 hypertensive patients required antihypertensive therapy and none of the hypercholesterolemic patients was on HMG-CoA reductase inhibitor treatment at the time of the study. The study was approved by the Ethics Committee of the University of Freiburg. All participants gave written informed consent.
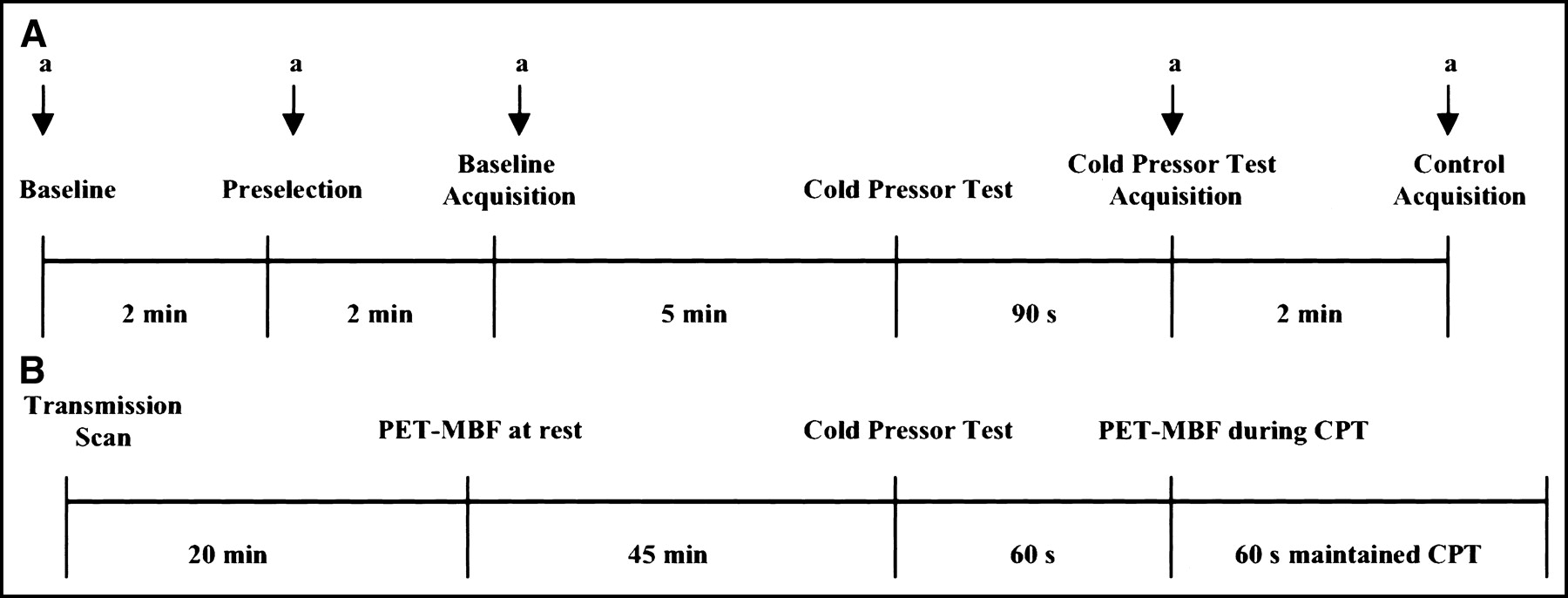
Study protocol. (A) Study inclusion at coronary angiography and quantitative assessment of epicardial vasoreactivity during CPT. a = angiogram. (B) Within 20 d of study inclusion MBF assessment with PET at rest and during CPT.
Patient Subgroups
Based on changes in epicardial LA with CPT, the study participants were grouped into normal controls and at-risk patients.
Control Group.
Twenty-two patients (14 men, 8 women; 37–65 y; mean age, 56 ± 9 y) without coronary risk factors including history of hypertension (≥140/90 mm Hg), smoking, diabetes, or hypercholesterolemia (total serum cholesterol values, ≥240 mg/dL) and all with CPT-induced dilation of the epicardial vessels (percent change of LA [ΔLA] > 0%) on angiography were defined as normal (9,10). None had a family history for CAD defined by evidence for CAD in a parent or sibling <60 y of age at the time of diagnosis.
At-Risk Group.
Thirty-four patients (19 men, 15 woman; mean age, 56 ± 10 y) with coronary risk factors and with a decrease in LA during CPT (ΔLA ≤ 0%) on angiography were defined as abnormal responders (9,10). Sixteen had hypertension (systolic blood pressure, ≥145 mm Hg), 10 had hypercholesterolemia (cholesterol, ≥263 ± 10 mg/dL), and 8 were long-term smokers (33 ± 8 pack-years). A family history for CAD was present in 5 patients with hypertension, 3 patients with hypercholesterolemia, and 2 chronic smokers.
Study Protocol
All patients were studied first with quantitative angiography and within 20 d with PET. Each patient was carefully screened by obtaining a complete history and by physical examination and laboratory analyses. Vasoactive medications including calcium-channel blockers, angiotensin-converting enzyme inhibitors, long-acting nitrates, and β-blockers were withheld for at least 24 h before the QCA and the PET study.
QCA
All patients underwent routine diagnostic catheterization for evaluation of chest pain using a biplanar, isocentric multidirectional digital angiographic system (BICOR-HICOR; Siemens) (13) (Fig. 1). A prerequisite for inclusion in the study was the absence of angiographically significant CAD, as indicated by smooth coronary vessels without evidence of luminal wall irregularities or diffuse caliber reduction and stenosis. After routine coronary angiography, a control angiogram was performed to select the best acquisition angulation for coronary angiography at baseline and during CPT for measurements of the LA of the selected epicardial vessel segment (Fig. 1). The coronary arteries studied were positioned near the isocenter. Care was taken to avoid overlapping of coronary segments. Thus, a relatively straight 4- to 8-mm-long segment of the left anterior descending artery (LAD) (27 patients) or left circumflex coronary artery (LCx) (29 patients) was preselected and a coronary angiogram was obtained at baseline. For the CPT, the patient immersed the left hand in ice water for 90 s when a second angiogram was acquired while—as described previously (3,9,16,17)—the CPT was continued for another 10 s. End-diastolic images of coronary arteries on biplanar views at baseline and after CPT were analyzed quantitatively (13). An automatic contour detection of the coronary artery segment was used using a geometric edge differentiation technique. Tapered or tortuous segments were not used. The LA of the coronary segment of interest was measured in both views of the images using the take-off of side branches as anatomic landmarks for identification of corresponding vessel segments. Estimation of the LA assumed an elliptic shape at baseline and after CPT (7,9,13). Calculation of the radiologic magnification factor of the measured segment was used for scaling of the data from pixels to millimeters (13). Thus, the epicardial LA as an endpoint of the measurements was determined at baseline and during CPT and the epicardial vasomotor response was quantified (Fig. 1). Accuracy, reproducibility, and inter- and intraobserver variability of the measurements have been reported previously (6,9,13).
PET Study Protocol
Regional MBF was measured with intravenous 13N-ammonia and serial image acquisition by PET (951 ECAT-HR; Siemens) (14,15). Measurements were performed first at baseline and then during CPT (Fig. 1). For the CPT, study participants immersed the left hand in ice water for 60 s, and 13N-ammonia was injected again while CPT was continued for another 60 s to permit trapping of 13N-ammonia in the myocardium (18). Beginning with each 13N-ammonia administration (555–740 MBq [15–20 mCi]), serial transaxial emission images were acquired (12 frames of 10 s each, 2 frames of 30 s each, and 1-frame of 900 s) (14,15). The serially acquired transaxial image data were then reoriented into short-axis slices. The 900-s short-axis cuts were examined visually on the last frame for the regional myocardial tracer activity concentrations at baseline and during CPT. Time–activity curves were generated from the first 12 serially acquired short-axis slices after assigning, on 3 midventricular slices, myocardial regions of interest to the territories of the LAD and LCx and of the right coronary artery (14,15). A small, 25-mm2 region of interest was assigned to the left ventricular blood pool. The myocardial and blood-pool time–activity curves were fitted with a previously validated 2-compartment tracer kinetic model and estimates of MBF (in mL · min−1 · g−1) were obtained (14,15). Heart rate, blood pressure, and a 12-lead electrocardiogram were recorded continuously. From the average of heart rate and blood pressure during the first 2 min of each image acquisition, the RPP was determined as an index of cardiac work. An index of coronary vascular resistance was calculated as the ratio of mean arterial blood pressure (mm Hg) to MBF (mL · min−1 · g−1).
Statistical Analysis
Data are presented as mean ± SD for quantitative and absolute frequencies for qualitative variables. For comparison of differences, appropriate Wilcoxon rank sum tests for independent or paired samples were used (SAS Institute). The Pearson correlation coefficient (r), assuming a linear regression, was calculated to investigate the associations between CPT-induced changes of epicardial LA and MBF responses. Differences of P < 0.05 were considered significant.
RESULTS
Patient Characteristics
Table 1 summarizes the baseline characteristics of the 2 study groups and lists hemodynamic parameters and findings on quantitative angiography and on MBF at baseline and during CPT. Of the 56 patients, 18 (32%) experienced chest pain during CPT at the time of cardiac catheterization, whereas 14 patients (25%) reported atypical chest pain during CPT at the time of the PET MBF study.
Characteristics of Study Population
Hemodynamics
Hemodynamic parameters during angiographic assessment of epicardial coronary vasomotion, during PET measurements of MBF at baseline, and during CPT are listed in Table 2. The RPP was used as an index of cardiac work and as a measure of the effectiveness of sympathetic stimulation with CPT. Heart rate and blood pressure were similar at baseline and during CPT on the 2 study days (P = not significant [NS]). During CPT, heart rate and systolic and diastolic blood pressure significantly increased (both P < 0.05) so that the RPP was significantly higher during CPT than at baseline. Importantly, the RPP at the time of the angiographic study and of the PET study was similar both at baseline (6,674 ± 995 vs. 6,636 ± 1,221) and during CPT (9,146 ± 1,431 vs. 9,199 ± 1,634; P = NS, respectively). In addition, there were no significant differences in the percent change of the RPP (%ΔRPP) in response to CPT during coronary angiography and MBF evaluation with PET (%ΔRPP, 37% ± 17% vs. 40% ± 21%; P = NS), indicating comparable myocardial workload on both study days.
Hemodynamics in QCA and PET Studies at Rest and During CPT
Findings on Quantitative Angiography
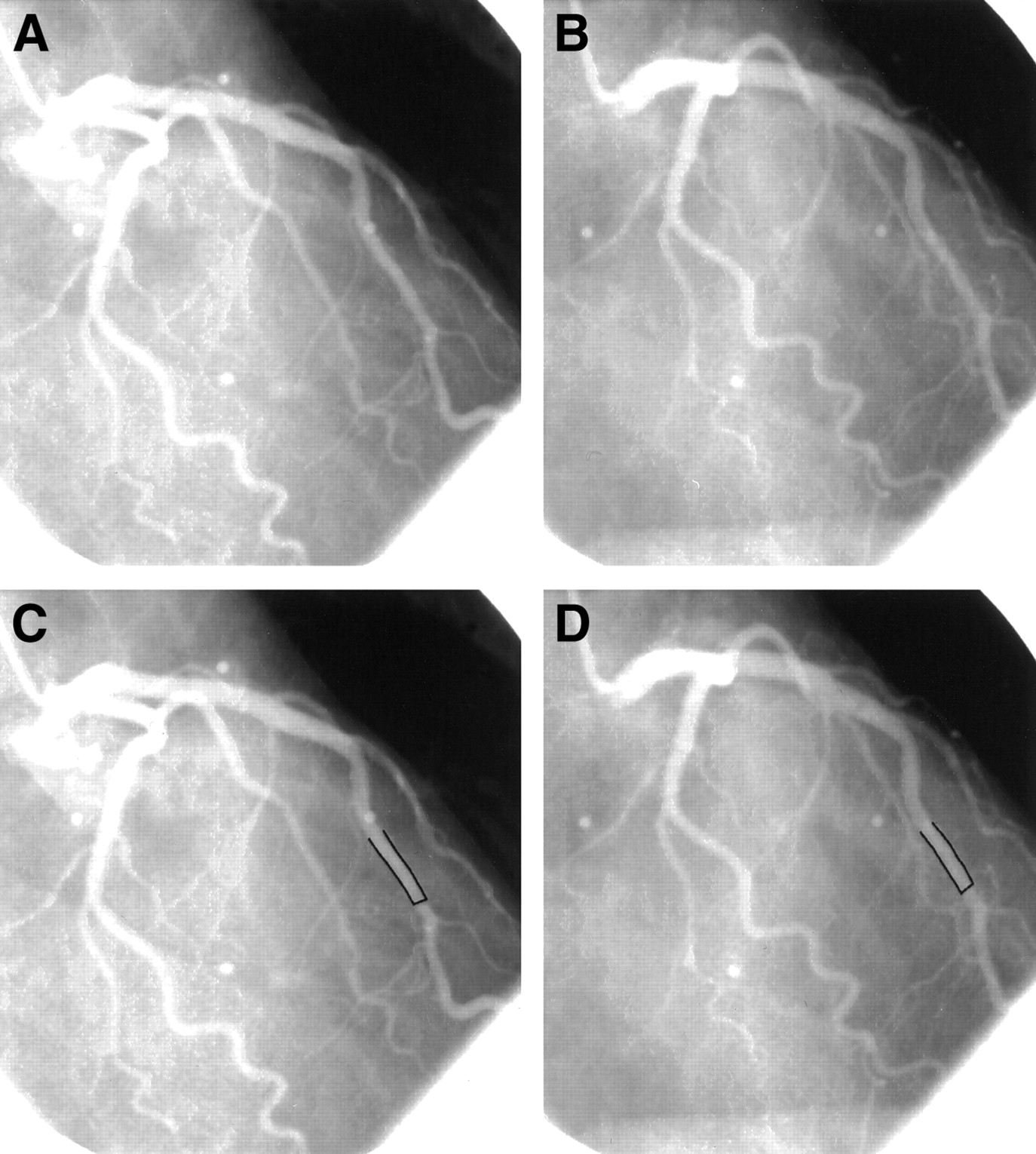
Figure 2 illustrates an example of a normal angiographic response to CPT in a normal control. The panel depicts a normal angiogram in the right anterior oblique (RAO) projection at baseline and during CPT. The epicardial vessel diameter has increased during CPT as compared with baseline. QCA of the LAD segment demonstrates an increase in luminal vessel diameter from 2.0 to 2.5 mm. The corresponding PET measurements demonstrated an increase in MBF from 0.78 to 1.36 mL · min−1 · g−1 during CPT. Figure 3 depicts an abnormal angiographic response to CPT in a long-term smoker. Again, the upper panel depicts the coronary angiogram in the left anterior oblique (LAO) projection at baseline and during CPT. However, the epicardial vessel diameter is seen to decrease from baseline to CPT, indicating an abnormal endothelium-dependent epicardial vascular response to CPT. QCA of the LAD segment reveals a decrease of the luminal vessel diameter from 1.89 to 1.57 mm (Figs. 3C and 3D). The corresponding PET measurements revealed a markedly attenuated MBF response to CPT; MBF was 0.51 mL · min−1 · g−1 at baseline and 0.61 mL · min−1 · g−1 during CPT and, therefore, increased by only 20%, implying that the abnormal endothelium-dependent vasomotion in this patient was not confined to the epicardial vessels but extended into the microcirculation.
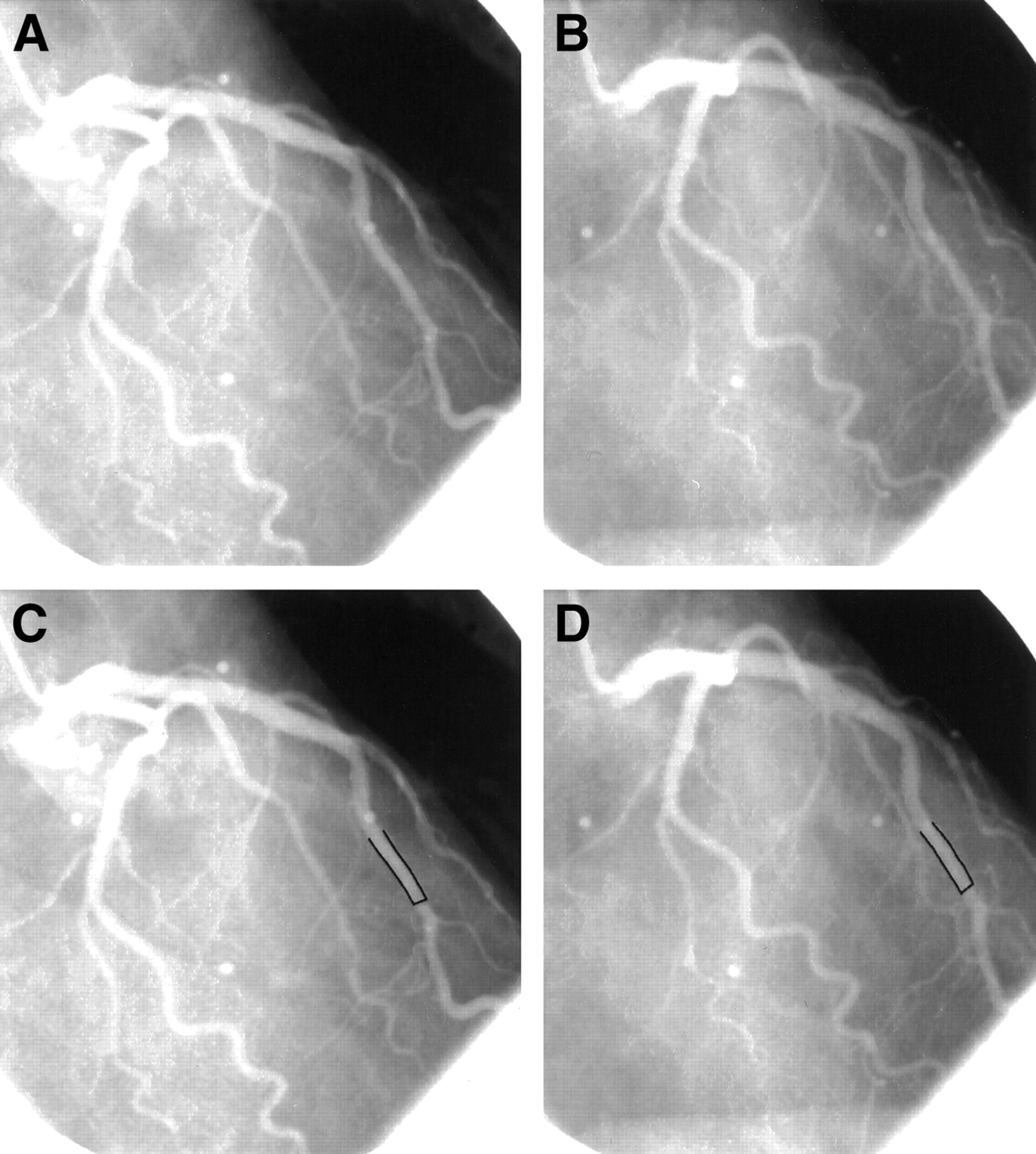
(A) Normal coronary angiogram of the left coronary tree in the RAO view of a control patient. (B) Corresponding coronary angiogram during sympathetic activation by CPT. (C and D) Quantitative coronary angiographic evaluation of the proximal-mid LAD segment at rest (mean diameter, 2.0 mm) (C) and during CPT (mean diameter, 2.5 mm) (D).
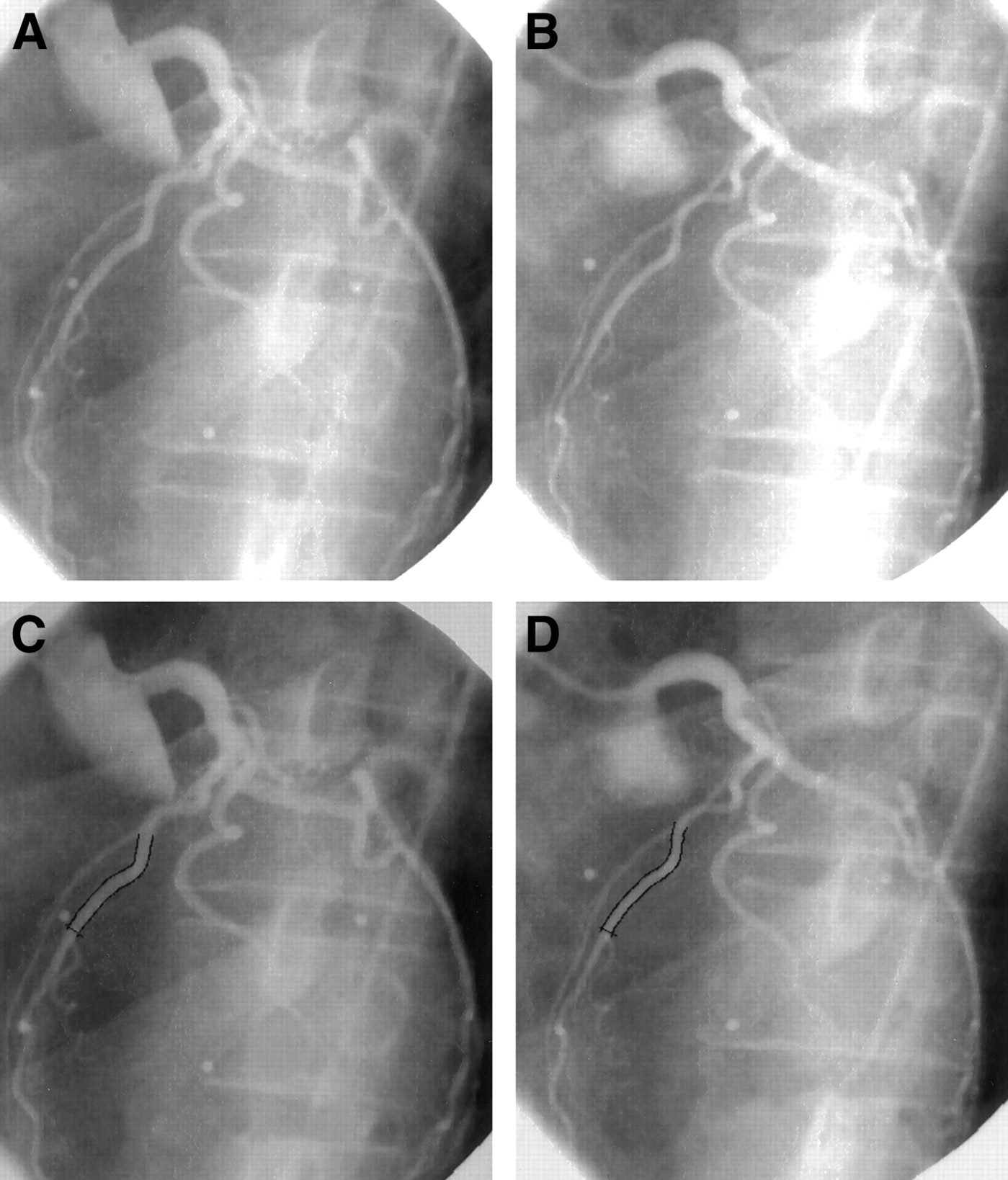
(A) Normal coronary angiogram of the left coronary artery tree in the LAO view in a chronic smoker at baseline. (B) Corresponding coronary angiogram during sympathetic activation by CPT. (C and D) Quantitative coronary angiographic evaluation of the proximal-mid LAD segment at rest (mean diameter, 1.89 mm) (C) and during CPT (mean diameter, 1.57 mm) (D).
Table 1 summarizes the findings on QCA. At baseline, the average epicardial LA was similar in normal controls and in at-risk patients (P = NS). During CPT however, the epicardial LA had decreased in the at-risk patients from 5.13 ± 1.49 to 4.24 ± 1.12 mm2 (P < 0.0001), representing an average −16% ± 12% decrease. The normal controls, however, demonstrated a flow-mediated increase of the average LA from 5.01 ± 1.07 to 5.88 ± 0.89 mm2 (P < 0.0001), representing a 19% ± 9% increase. During CPT, the LA change in the at-risk group differed significantly from that in the control subjects (P < 0.0001).
The abnormal flow-mediated epicardial vascular response to an increase in myocardial demand during CPT in the at-risk patients was also evident when the data were plotted so that changes in epicardial LA were compared with increases in the RPP. Figure 4 depicts a significant correlation between percent changes in epicardial LA and the percent change in the RPP during CPT for the normal controls (r = 0.82; P < 0.0001); no such correlation was observed in the at-risk patients (r = 0.08; P = NS), implying an uncoupling of the epicardial vascular response from an increase in demand during stimulation.

Correlation of CPT-induced change in RPP and epicardial LA in normal control patients (○) and in the group at risk for CAD (•), demonstrating a significant correlation in normal patients but no relation for patients at risk for CAD.
MBF Responses to CPT
Visual inspection and polar map analysis of the 13N-ammonia distribution at baseline and during CPT revealed homogeneous tracer uptake in all study participants. There were no CPT-induced regional myocardial perfusion defects. PET-measured MBFs in the coronary artery territory supplied by the epicardial vessel analyzed on angiography were at baseline similar for at-risk and normal control patients (0.76 ± 0.20 mL · min−1 · g−1 vs. 0.77 ± 0.16 mL · min−1 · g−1; P = 0.76; Table 1). However, MBF during CPT was lower in the at-risk patients than in the control subjects (0.76 ± 0.20 to 0.83 ± 0.25 mL · min−1 · g−1 vs. 0.77 ± 0.16 to 1.34 ± 0.34 mL · min−1 · g−1; P ≤ 0.0001; Table 1). MBF during CPT was thus significantly higher than baseline in the normal control but not in the at-risk patients. Moreover, average MBFs in the 2 coronary territories supplied by vessels not evaluated on quantitative angiograpphy were similar to MBFs in coronary territories subtended by coronary vessels submitted to quantitative analysis. No significant differences were noted during CPT (at-risk patients, 0.76 ± 0.17 to 0.83 ± 0.20 mL · min−1 · g−1 vs. 0.76 ± 0.20 to 0.83 ± 0.25 mL · min−1 · g−1; controls, 0.75 ± 0.20 to 1.32 ± 0.31 mL · min−1 · g−1 vs. 0.77 ± 0.16 to 1.34 ± 0.34 mL · min−1 · g−1, respectively; P = NS), suggesting that the vasomotor abnormality in the at-risk patients affected the coronary circulation homogenously.
MBF responses relative to the CPT-induced changes in the RPP greatly differed between the 2 study groups. This difference is illustrated in Figure 5, where the CPT-induced increase in the RPP is associated with a proportionate increase in MBF in the normal controls (r = 0.87; P < 0.0001), whereas changes in the RPP no longer correlate with changes in MBF (r = 0.26; P = 0.13) in at-risk patients, implying an uncoupling of abnormal endothelium-dependent coronary vasomotion from the CPT-induced metabolic demand.
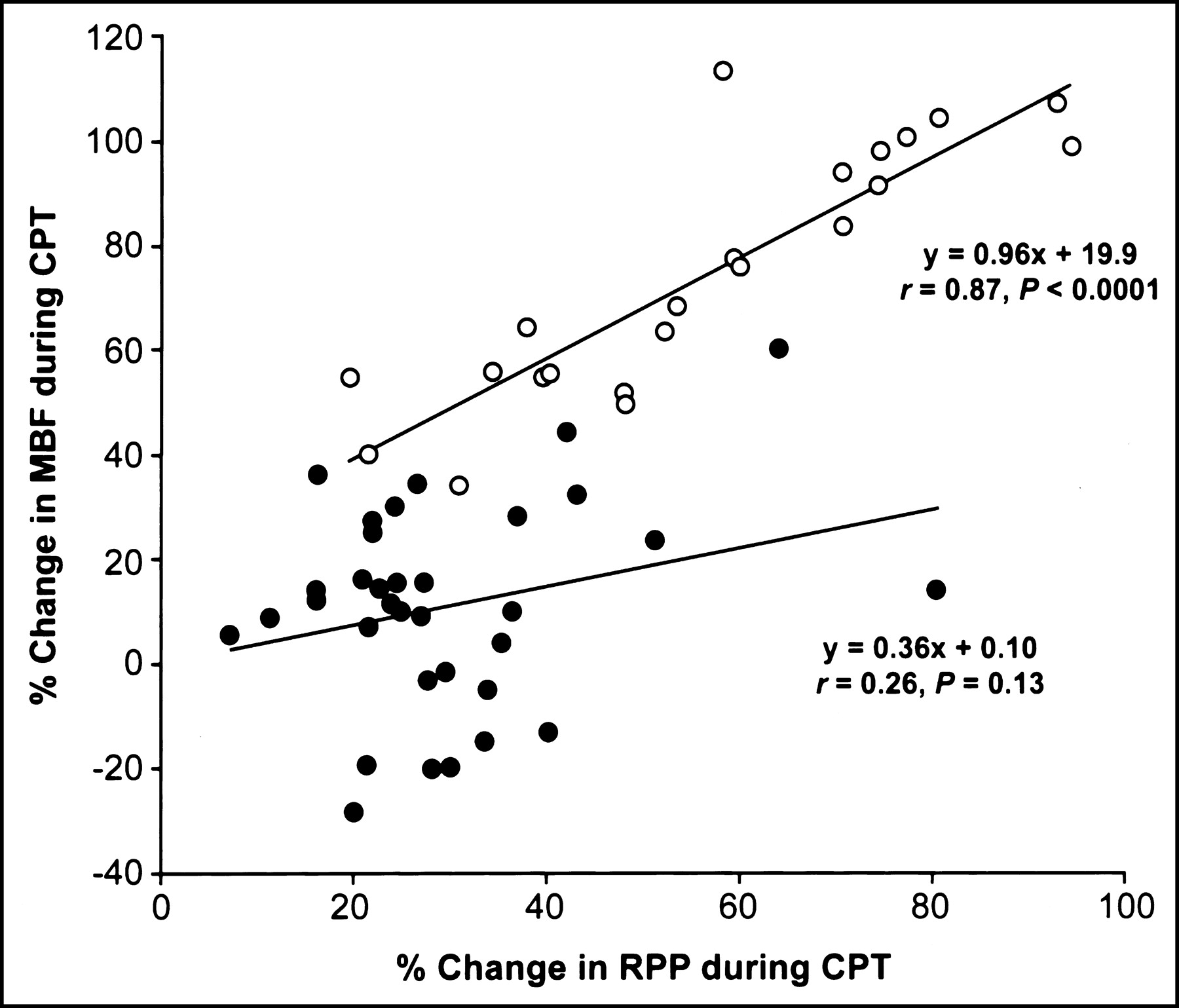
Correlation of CPT-induced change in RPP and regional MBF in normal control patients (○) and in the group at risk for CAD (•), revealing a significant correlation in normal patients but no relation for patients at risk for CAD.
In order to account for interindividual variations in the coronary driving pressure, an index of coronary vascular resistance was calculated as the ratio of mean arterial blood pressure to MBF. At baseline, the index was similar for controls and patients at-risk (114 ± 23 vs. 122 ± 26 mm Hg/mL · min−1 · g−1; P = 0.61; Table 1). During CPT, coronary vascular resistance consistently declined in the normal controls, which was different from the responses in at-risk patients; they were highly variable and paradoxically increased in some patients. Mean values of the resistance index in the normal controls and the at-risk patients were 114 ± 23 to 80 ± 14 mm Hg/mL · min−1 · g−1 and 122 ± 26 to 128 ± 32 mm Hg/mL · min−1 · g−1; P < 0.001; Table 1). Figure 6 illustrates the percent change of coronary vascular resistance (CVR) for each patient during CPT.
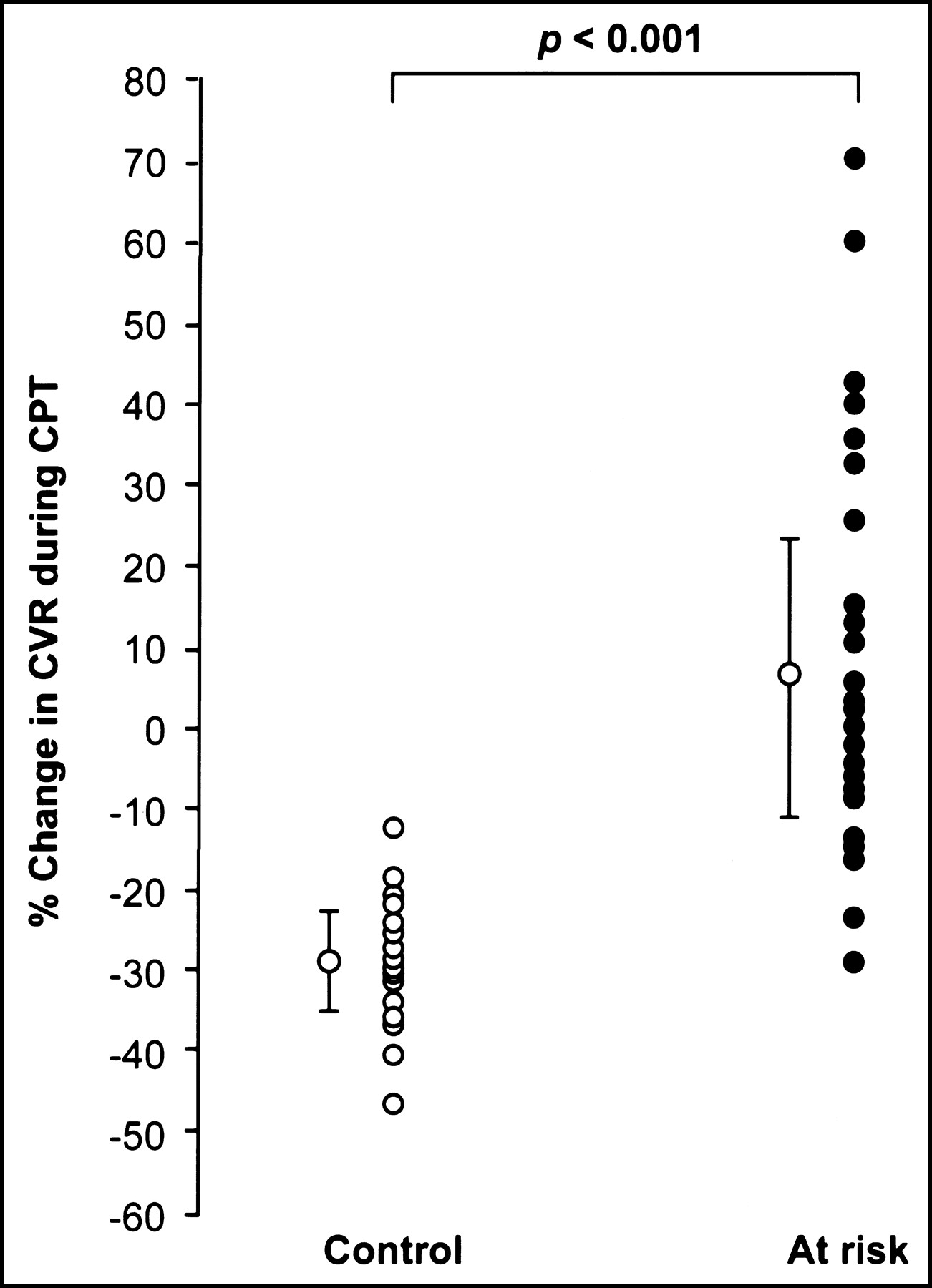
Percent change of CVR in the control group and in patients at risk for CAD.
Correlation Between Coronary Angiographic and PET Measurements
For the entire study group, the epicardial LA decreased from 5.07 ± 1.02 to 4.88 ± 1.04 mm2 (ΔLA, −0.20 ± 0.89 mm2) or by −2.19% ± 17% (P = 0.19), whereas MBF increased from 0.76 ± 0.16 to 1.03 ± 0.33 mL · min−1 · g−1 (ΔMBF, 0.27 ± 0.25 mL · min−1 · g−1) or by 36% ± 31% (P ≤ 0.0001). In order to examine a possible relationship between CPT-induced epicardial and arteriolar vasomotion, the change in epicardial LA was compared with the CPT-induced change of MBF. As Figure 7 illustrates, the CPT-induced percent change in the LA of the epicardial coronary segment and the percent change of MBF response were significantly correlated (r = 0.87; P = 0.0001), suggesting that the CPT-induced change of the epicardial LA was associated with a corresponding change in MBF.

Percent change of epicardial LA and MBF to CPT of the study population.
DISCUSSION
To our knowledge, this study is first to demonstrate a significant correlation between CPT-induced changes of the epicardial LA and MBF in patients with normal coronary angiograms, indicating that flow-dependent changes of epicardial LA indeed correlate with flow-dependent changes in the coronary resistance vessels. These observations are in keeping with previous studies (6,7,12) but extend these findings to a correlation between changes of the epicardial LA and of MBFs in response to sympathetic activation. Thus, the results of the study provide evidence that myocardial flow responses to sympathetic activation as assessed noninvasively by PET may serve as a useful tool for probing predominantly endothelium-dependent coronary vasomotion.
Heart rate and blood pressure at baseline and during CPT were similar at the time of the 2 study sessions, suggesting comparable hemodynamic conditions during QCA and during the PET measurements. Comparable mean values of MBF both at baseline and during CPT on repeated PET studies, as reported previously (12,18,19), suggest the reproducibility of the PET measurements and MBF responses to CPT. The present investigation demonstrates that in the absence of angiographic evidence of CAD, the paradoxical vasoconstrictor response of epicardial coronary arteries is associated with an impaired vasodilator function of the coronary arteriolar vessels in response to sympathetic stimulation. The functional impairment was noted in patients with coronary risk factors, whereas control subjects without such risk factors revealed preserved endothelium-dependent coronary vasomotion of both coronary conductance and resistance vessels. However, it should be emphasized that participants in this study were grouped according to a normal or abnormal epicardial coronary vasomotor response to CPT. Thus, patients with coronary risk factors but a possibly preserved vasomotor response were not included in this study, thereby avoiding possibly confounding effects of variabilities of coronary vasomotion (1,19).
Of particular interest, as also described previously (7,8), there was a significant positive correlation between CPT-induced changes in the RPP and changes of epicardial LA as well as PET-measured MBF responses in control subjects. Patients with coronary risk factor states no longer revealed such correlation, indicating an uncoupling of the normal endothelium-dependent coronary vasomotion from the metabolic demand during sympathetic activation. Thus, despite angiographically normal coronary arteries, the diminished or even paradoxical endothelium-dependent myocardial flow response may result in a mismatch between an increase in demand and supply that has been related to myocardial ischemia during daily life (20) and during exercise (21,22). Consistent with previous reports (7,8), the observed association between increases in MBF and increases in the RPP and thus in cardiac work in our normal controls implicates about a 30%–40% increase in MBF as a normal response to CPT. While the flow response to cold was on average markedly attenuated in the patients at risk, individual flow responses to sympathetic stimulation considerably varied, suggesting that flow responses to sympathetic stimulation in some patients with coronary risk factors such as hypertension or hypercholesterolemia may remain fully preserved. Thus, additional still undefined mechanisms such as genetic and environmental factors may be needed for an abnormal endothelium-dependent vasomotor response (1,2). In this regard, it is of interest to note that approximately only 50% of the total attributable risk burden for CAD can be related to conventional risk factor states (23,24), warranting identification of alternate determinants of risk with mechanistic rationale. Although genetic variations have been realized as an important determinant of both the development of coronary atherosclerosis and the subsequent cardiovascular events, there are still some controversies of the impact of gene polymorphisms on late cardiovascular outcome (24). The latter controversies may be explained at least in part by modification of a genetic effect by environmental factors. For example, the carriage of the eNOS Asp298 allele alone may be insufficient to account for enhanced susceptibility to vascular disease or dysfunction. Rather, it requires other risk factors such as smoking to increase the likelihood of impaired endothelial-dependent vasomotion (25). Therefore, interactions of environmental factors with the eNOS Glu298Asp polymorphism appear to be necessary to produce the disease phenotype resulting in abnormal, endothelial-dependent vascular function. More exciting, dietary intervention to increase n-3 fatty acid levels resulted in a positive effect of vascular function in healthy young subjects with the eNOS Glu298Asp polymorphism (25), suggesting that medical interventions tailored to enhance endogenous NO production and bioavailability may prove beneficial in individuals with eNOS polymorphisms that limit the generation of bioactive and atheroprotective NO.
Moreover, it should be kept in mind that coronary risk factors per se may not always be associated with abnormal coronary vasomotion (1,2,26). For example, recent studies suggest that hypertension alone is not a stimulus for increased production of reactive oxygen species (ROS) but that conditions in which elevated circulating or local concentrations of angiotensin II induce an increase in superoxide production via stimulation of the membrane-bound NADH oxidase may result in detrimental effects on the vascular endothelium independent of elevating blood pressures (26). Thus, it appears that hypertension not associated with increases in angiotensin II and not associated with the activation of NADH oxidases may be less prone to manifest in abnormal endothelial-dependent vasomotion (27).
The correlation between LA changes of the large-conduit vessels and changes in MBF in response to CPT as found for the entire study population argues in favor of a close functional association between flow-dependent regulatory mechanisms at the level of the epicardial conduit and of the coronary resistance vessels. Functional alterations associated with coronary risk factors are therefore likely to affect both the conduit and the resistance vessels. Because alterations in flow responses to CPT were not confined to the territory of the coronary artery analyzed by quantitative angiography but were distributed homogenously throughout the entire myocardium, disturbances of endothelium-dependent vasomotion appear to homogenously affect the entire coronary circulation. Further, because of the previously observed close correlation between LA changes of the epicardial conduit vessels and changes in coronary flow velocity, changes in shear stress are major contributors to flow-mediated vasodilator responses (6,7). It is therefore conceivable that metabolically mediated increases in blood flow during sympathetic stimulation with CPT led, under normal conditions, to shear stress–mediated increases of the diameter of the conduit vessels (7). MBF responses to adenosine or dipyridamole are predominantly vascular smooth muscle dependent. However, shear-sensitive components of the endothelium are likely to participate and contribute through flow-dependent mechanisms so that the hyperemic MBF serves as a measure of the integrated coronary circulatory function (28). In contrast, MBF responses to CPT provide more selective information on the endothelium-dependent coronary vasomotor function (1,7,12,16,17). This has been shown previously through highly invasive investigations in which the responses to direct intracoronary acetylcholine stimulation of the coronary endothelium were found to correlate closely with responses of the coronary flow velocity and of the coronary vessel diameter to CPT (7,9).
The cause of abnormal endothelium-dependent coronary vasoregulation in patients with various coronary risk factor states in this study and observed in previous investigations has yet to be defined. Abnormal coronary vasoreactivity to sympathetic stimulation is certainly multifactorial in etiology but may include diminished production or release of NO, destruction of NO, and concomitant release of constricting factors (1,2). Traditional risk factors for CAD have been shown to be associated with increased amounts of ROS and through interaction with NO reduce the bioavailability of endothelium-derived NO and promote vascular injury (1,2). Increased oxidative stress also may induce an array of inflammatory genes involved in the pathogenesis of atherosclerosis (1,2). Thus, increased generation of vascular ROS from sources such as NAD(P)H oxidase, xanthine oxidase, and uncoupled NO synthase in patients with coronary risk factors is considered to be a major common pathway leading to abnormal endothelium-dependent coronary vasomotion.
During sympathetic stimulation with CPT, the α-adrenergically mediated vasoconstriction of the vascular smooth muscle cell is, under normal conditions, offset by flow-mediated response and, possibly, by a direct adrenergically induced endothelium-dependent vasodilator response (29). However, the vasoconstrictor effect may remain largely unopposed in the presence of endothelial dysfunction or atherosclerosis (30). Thus, the cold-induced response of MBF represents the net effect of endothelium-related vasodilator effects and vasoconstrictor responses of epicardial and arteriolar vascular smooth muscle cells (29,30,31), supporting the notion that coronary vasomotor responses to sympathetic activation may accurately reflect the functional integrity of the vascular wall (1,9).
The clinical implications of this study are considerable. Endothelial dysfunction of both the conduit and the coronary resistance vessels has been shown to precede and accompany the development and progression of atherosclerosis, implicating the endothelium as both the target and the mediator of the atherosclerotic process with substantial diagnostic and prognostic implications (3–5,23,32,33). However, established coronary risk factors may not be the sole determinants of abnormal endothelium-dependent coronary vasomotion. As recent observations indicate, individuals with normal endothelial function and patients with various stages of endothelial dysfunction may not necessarily differ in their risk factor profiles (23,32,33). Consistent with this possibility is the recently reported dissociation between endothelial vasomotor responses to acetylcholine and coronary atherosclerosis by intravascular ultrasound (IVUS), further suggesting that findings on intracoronary ultrasound alone may be limited in value for predicting coronary events (32).
In this regard, the findings of the current study indicate that PET measurements of MBF combined with CPT correlate with well-established indices of coronary vasomotion on quantitative angiography and support the validity and value of MBF responses to sympathetic activation as a noninvasive measure of coronary circulatory function. Hence, this noninvasive assay approach could serve as a surrogate for predicting the development of coronary atherosclerosis in humans (4). In addition, it is of great interest to ascertain whether a preventive medical intervention may be successfully guided according to the findings of abnormal coronary circulatory function in response to sympathetic activation as assessed by PET imaging.
There are limitations worth consideration in interpreting our data. One important drawback was that we did not perform IVUS to assess the vascular wall structure for an accurate classification of patients with normal coronary angiograms (34). Hence, as reported previously (35), early signs of atherosclerosis not detected by coronary angiography may have been present in the actual study population. Furthermore, because changes of epicardial LA and MBF responses to CPT were determined on different study days, differences in the hemodynamic state could have influenced the results of epicardial and arteriolar vascular responses. However, as shown, there were no significant differences in hemodynamic parameters and in hemodynamic responses to CPT between the angiographic and PET studies, indicating that both measurements were performed under comparable study conditions.
CONCLUSION
The observed close correlation between an angiographically established parameter of flow-dependent, and most likely endothelium-mediated, coronary vasomotion and PET-measured MBFs further supports the validity and value of MBF responses to sympathetic activation as a noninvasive index of coronary circulatory function. Thus, PET perfusion imaging with CPT appears to be a promising tool to probe noninvasively flow-dependent, and most likely endothelium-dependent, coronary vasomotion.
Acknowledgments
The authors are indebted to the nurses of the Cardiac Catheterization and PET-Cyclotron Unit of the Albert Ludwigs University, Freiburg, for their invaluable support. This work was supported in part by a grant from the government of Baden-Württemberg to the Center of Clinical Research II: Cardiovascular Diseases: Analysis and Integration of Form and Function of the Albert Ludwigs University, Freiburg (project THS- and EUN-A1/A2), and by grant HL 33177 from the National Heart, Lung and Blood Institute.
Footnotes
Received Jun. 19, 2003; revision accepted Oct. 29, 2003.
For correspondence or reprints contact: Heinrich R. Schelbert, MD, PhD, Department of Molecular and Medical Pharmacology, David Geffen School of Medicine at UCLA, B2-085J CHS: Box 95648, Los Angeles, CA 90095-6948.
E-mail: hschelbert{at}mednet.ucla.edu
REFERENCES
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Total-Body Perfusion Imaging with [11C]-Butanol
- Coronary Microvascular Dysfunction: Clinical Considerations and Noninvasive Diagnosis
- Myocardial Blood Flow and Coronary Flow Reserve During 3 Years Following Bioresorbable Vascular Scaffold Versus Metallic Drug-Eluting Stent Implantation: The VANISH Trial
- Clinical Quantification of Myocardial Blood Flow Using PET: Joint Position Paper of the SNMMI Cardiovascular Council and the ASNC
- Atherosclerotic Plaque Characteristics by CT Angiography Identify Coronary Lesions That Cause Ischemia: A Direct Comparison to Fractional Flow Reserve
- Structural Abnormalities of the Coronary Arterial Wall--in Addition to Luminal Narrowing--Affect Myocardial Blood Flow Reserve
- Cardiac PET Imaging for the Detection and Monitoring of Coronary Artery Disease and Microvascular Health
- Coronary Circulatory Function Abnormalities in Insulin Resistance: Insights From Positron Emission Tomography
- Improvement in coronary vascular dysfunction produced with euglycaemic control in patients with type 2 diabetes
- Smoking Cessation Normalizes Coronary Endothelial Vasomotor Response Assessed with 15O-Water and PET in Healthy Young Smokers
- Repeatability of Cold Pressor Test-Induced Flow Increase Assessed with H215O and PET
- Relationship Between Increasing Body Weight, Insulin Resistance, Inflammation, Adipocytokine Leptin, and Coronary Circulatory Function
- Coronary Circulatory Dysfunction in Insulin Resistance, Impaired Glucose Tolerance, and Type 2 Diabetes Mellitus
- Positron Emission Tomography-Measured Abnormal Responses of Myocardial Blood Flow to Sympathetic Stimulation Are Associated With the Risk of Developing Cardiovascular Events