


Abstract
Hürthle cell carcinoma is an uncommon differentiated thyroid cancer characterized by an aggressive clinical course and low avidity for 131I. Treatment usually involves an aggressive surgical approach often combined with 131I. 18F-FDG PET has been helpful in the staging and evaluation of many types of aggressive malignancy. No reports to date have described the utility of PET in a series of patients with Hürthle cell cancer. We reviewed our experience with 18F-FDG PET in the care of patients with Hürthle cell carcinoma to determine the likelihood of uptake in these cancers and the effect of 18F-FDG PET on patient care. Methods: Patients with Hürthle cell cancer who were seen between June 2000 and April 2002 and were imaged with 18F-FDG PET were included. Imaging and clinical data were reviewed. PET results were compared with the results of anatomic imaging (CT, sonography, or MRI) and 131I imaging when performed. Patient charts were reviewed to identify any change in management that resulted from the 18F-FDG PET findings. Results: Fourteen 18F-FDG PET scans of 12 patients were obtained in the time frame indicated. All patients had documented Hürthle cell carcinoma. PET showed intense 18F-FDG uptake in all known Hürthle cell cancer lesions but one. PET showed disease not identified by other imaging methods in 7 of the 14 PET scans. PET identified distant metastatic disease (5) or local disease (2) that was more extensive than otherwise demonstrated. In 7 of the 14 scans, the information provided by PET was used to guide or change therapy. Conclusion: Hürthle cell carcinoma demonstrates intense uptake on 18F-FDG PET images. PET improves disease detection and disease management in patients with Hürthle cell carcinoma relative to anatomic or iodine imaging. 18F-FDG PET should be recommended for the evaluation and clinical management of patients with Hürthle cell carcinoma.
Hürthle cell carcinoma is an aggressive, follicular thyroid cancer variant that is infrequent relative to papillary or follicular thyroid malignancy. The tumor is derived from follicular cells and is composed mostly of oxyphilic follicular cells (1). Hürthle cell cancer has a 33% risk of metastasizing distantly, compared with 22% for follicular and 10% for papillary cancer. Survival at 5 and 20 y is poorer for patients with Hürthle cell cancer. Papillary and follicular cancer patients have survivals of 94% and 87%, respectively, at 5 y and 87% and 81%, respectively, at 20 y, whereas Hürthle cell cancer patients have survivals of 81% and 65% at 5 and 20 y, respectively (2).
The diagnosis of Hürthle cell carcinoma, as with all follicular cancers, requires histologic identification of malignant characteristics to separate adenomas from carcinomas. Ideally, an initial complete resection with preservation of laryngopharyngeal function is combined with appropriate adjuvant therapy. Unfortunately, Hürthle cell neoplasms have poor iodine accumulation, and therefore, 131I therapy is not often a good therapeutic option (3). Local recurrence requires a careful balance of revision surgery and, potentially, external-beam radiation therapy. External-beam radiation therapy has also benefited nonpulmonary distant metastasis. Complete resection of the primary and any cervical disease, thorough evaluation for distant metastasis, and close follow-up for local or distant recurrence would be prudent.
Several functional imaging modalities have been proposed for imaging Hürthle cell cancer (3–5). Imaging with 99mTc-sestamibi, 99mTc-dimercaptosuccinic acid, and 111In-diethylenetriaminepentaacetic acid-d-Phe1-octreotide has shown encouraging results. 18F-FDG PET can identify high-grade cancer because of the high glucose uptake in aggressive, poorly differentiated malignancy. Although 18F-FDG PET has reduced sensitivity for early-stage, well-differentiated thyroid malignancy (6), improved sensitivity is seen in aggressive, dedifferentiated, 131I-negative thyroid malignancy with 18F-FDG PET. The highly aggressive nature of Hürthle cell cancer may provide an opportunity to image this malignancy with improved sensitivity using PET. Indeed, reports of 18F-FDG PET in patients with Hürthle cell cancer have supported this notion (7–11). We reviewed our data of patients with 18F-FDG PET scans and Hürthle cell cancer of the thyroid to determine the sensitivity of PET in these patients and its contribution to their overall care.
MATERIALS AND METHODS
Patients
Patients with Hürthle cell cancer seen between June 2000 and April 2002 who were imaged with 18F-FDG PET were included. The study was approved by the Mayo Clinic institutional review board, and clinical data were reviewed. All imaging results as indicated in the medical record were used as the imaging results for the study. Experts on each modality (131I/123I, CT, PET, or sonography) interpreted the imaging data. PET results were compared with the findings of other types of imaging (131I/123I, CT, or sonography), when performed. Imaging with 131I/123I (7 patients) was performed on average within 7 d (range, 23 d before to 6 d after) of the PET scan. CT (10 patients) was performed on average within 1.8 d (range, 2 d before to 7 d after) of the PET scan. MRI (2 patients) was performed on average within 1.8 d (range, 7 d before to 2 d after) of the PET scan. Sonography (7 patients) was performed on average within 2.1 d (range, 8 d before to 5 d after) of the PET scan. CT was performed on a HiSpeed CT/i tomograph (General Electric Medical Systems) and included the area from the zygoma to the aortic arch when neck scans were obtained. Generally, sonography was the primary anatomic imaging technique used for the neck. CT of the chest was performed on all but 3 patients as well. Contrast (100 mL of Omnipaque 350; Amersham Health) was injected intravenously, and helical imaging was started 30 s afterward using 5-mm collimation. Scans of more superior regions, to include the skull base, were obtained when indicated. MR images were obtained on a limited basis. 131I imaging was performed 24 h after the administration of 111–148 MBq (3–4 mCi) of orally administered 131I. Whole-body images and dedicated neck views were obtained. Imaging was performed on a Bodyscan tomograph (Siemens Medical Systems, Inc.).
Patient charts were reviewed to identify any change in management that resulted from the 18F-FDG PET findings indicated by the physician. Disease limited to the thyroid gland was treated with a near-total or total thyroidectomy. Suggestive lymph nodes identified either radiologically or clinically were addressed with regional lymphadenectomy. Extrathyroidal extension required frozen-section control of margins to guide resection of tumor invasion of the larynx, trachea, esophagus, or other vital neck structures.
PET
18F-FDG PET was performed on an Advance tomograph (General Electric Medical Systems). This tomograph has an axial field of view of 15 cm and an axial resolution of 5.4 mm from a point source at a 10.0-cm radius.
The 18F-fluoride was produced by a Trace cyclotron (General Electric Medical Systems) that is on site. 18F-FDG was synthesized by the Hamacher method. 18F-FDG was tested for sterility, pyrogenicity, and radiochemical purity on each production run.
PET emission images of the body, to include the head, neck, chest, and abdomen, were obtained 50 min after intravenous injection of 370–740 MBq of 18F-FDG. After the patients had been allowed to void, they were positioned on the tomographic gantry and a series of body images was obtained. This set of image data spanned at least from the upper orbit to the iliac crests.
Emission images were reconstructed using filtered backprojection with a Hann window of 5.0-mm width and iterative reconstruction. Attenuation correction was used. Emission data were corrected for scatter, random events, and dead-time losses using the manufacturer’s software. Image pixel size was 4.25 mm, and the image was displayed in a 128 by 128 matrix. Standard tomographic views and a maximum-intensity projection were reviewed during scan interpretation.
Data Analysis
Results from PET and other imaging methods were tabulated. The results of the imaging tests were compared, and differences in disease distribution observed in the different imaging studies were noted. The imaging results were compared with pathologic sampling of regions of concern. The sensitivity of 18F-FDG PET was determined through histologic confirmation or through clinical consensus on disease status based on the medical record.
RESULTS
Fourteen 18F-FDG PET scans of 12 patients were obtained in the time frame indicated. Ten of the PET scans were for evaluation of morphologic abnormalities found by other imaging techniques. Of the other 4 patients, 2 were imaged without any other suspected abnormalities, 1 for a positive finding on physical examinations, and 1 for an elevated thyroglobulin level. The patient group included 7 men and 5 women with an average age of 47 y (range, 38–78 y). All patients had previous biopsy-proven Hürthle cell carcinoma. Eleven of the 12 patients were being evaluated for recurrent Hürthle cell carcinoma, and 1 patient was undergoing disease staging for the planning of initial therapy. In patients with previous disease, the mean time from diagnosis to the time of evaluation was 4.4 y (range, 5 mo to 15 y). At the time of evaluation, Hürthle cell carcinoma was shown to be present in 13 patients, as confirmed by pathology in 10 and by clinical follow-up in 3. One patient (patient 7), who had undergone subtotal thyroidectomy 1 mo before, was shown to be disease free on all imaging tests except iodine imaging, which was equivocal; was biopsy negative in the neck by fine-needle aspiration; and was disease free 1 y later on follow-up. PET findings were positive, with intense 18F-FDG uptake, in all but 1 of these 13 patients with known disease (92% sensitivity).
Disease not identified by other imaging methods was shown in 7 of the 14 PET scans obtained (Table 1). PET identified distant metastatic disease (6) or local disease (2) that was more extensive than otherwise demonstrated (1 patient had both more extensive local disease and distant disease shown by PET). Of these 8 areas of disease, 5 were proven by biopsy, 2 were confirmed by other imaging methods, and 1 was considered positive on the basis of other clinical data (Figs. 1 and 2). For 7 of 14 scans, the information provided by PET was used to guide or change therapy. Of 7 patients who had iodine scans, 6 had negative findings and 1 scan was read as questionable. In the 1 PET scan that was read as negative, there was substantial nonspecific neck uptake, probably because of muscle or fat uptake, that may have obscured the 1 focal site of disease then thought to exist (Fig. 3). The focus as seen on sonography was 1.8 × 1.1 × 0.9 cm. Three months later, this site was resected and proven to be grade 2/4 Hürthle cell recurrence. On retrospective review of the PET data, the area in question did show moderate metabolism, but the finding was not obvious.
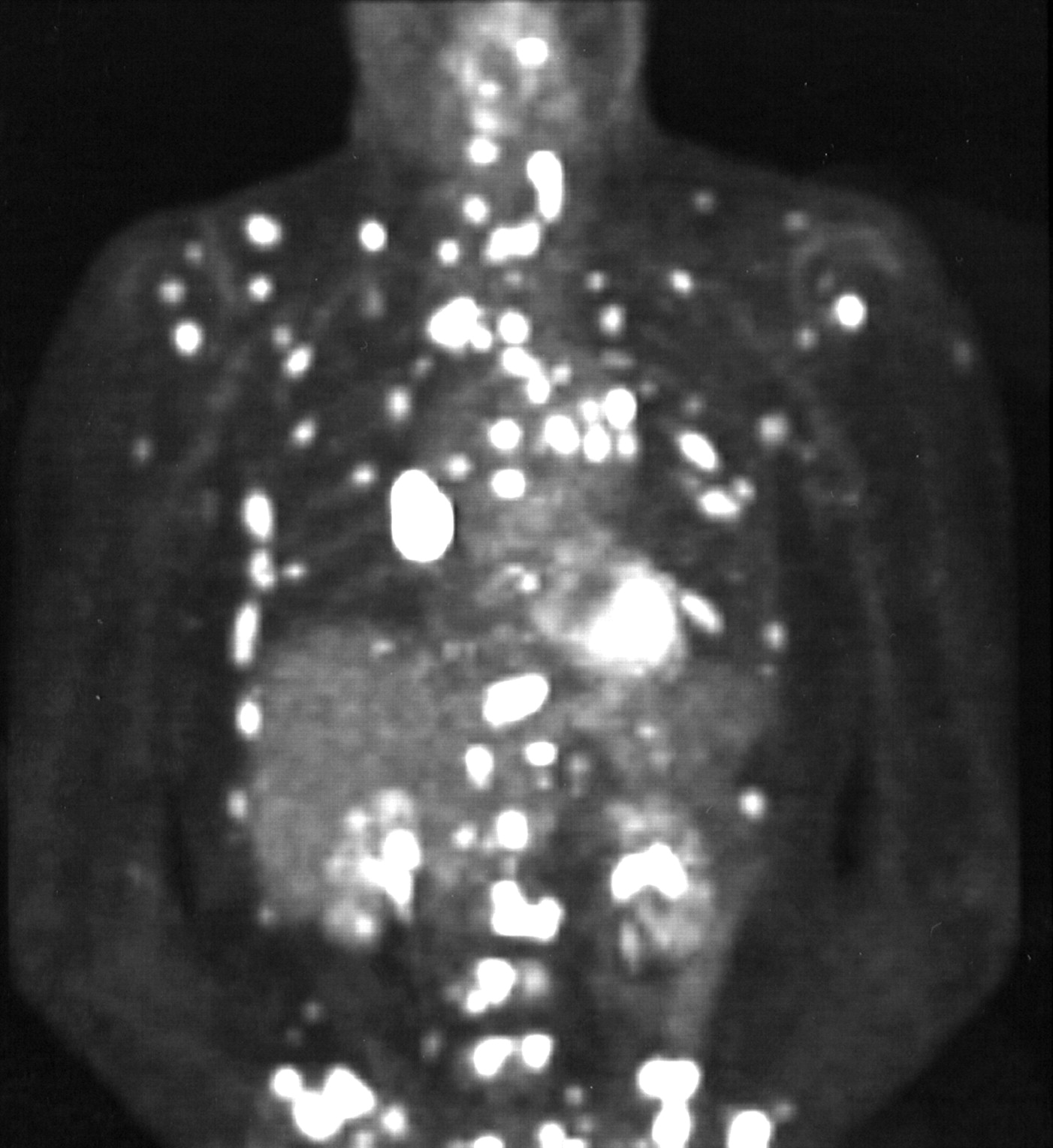
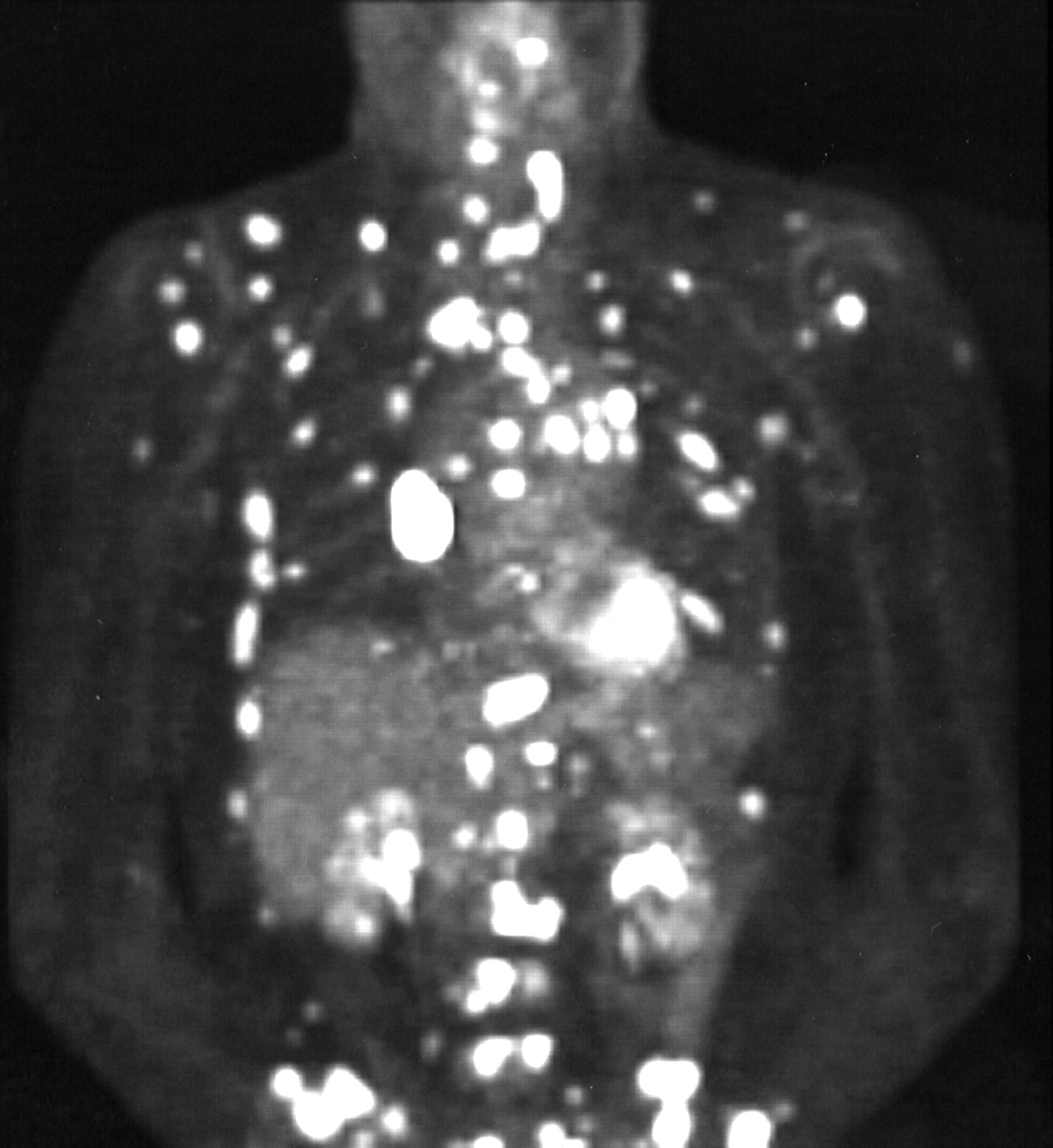
PET image of patient 2, who had history of Hürthle cell cancer and returned with complaint of diffuse aches. Single indeterminate lung nodule with some mediastinal adenopathy was seen on CT. Sonography and 131I scans had negative findings. PET image showed widespread bone and lung metastases, which were confirmed with right hilar biopsy.
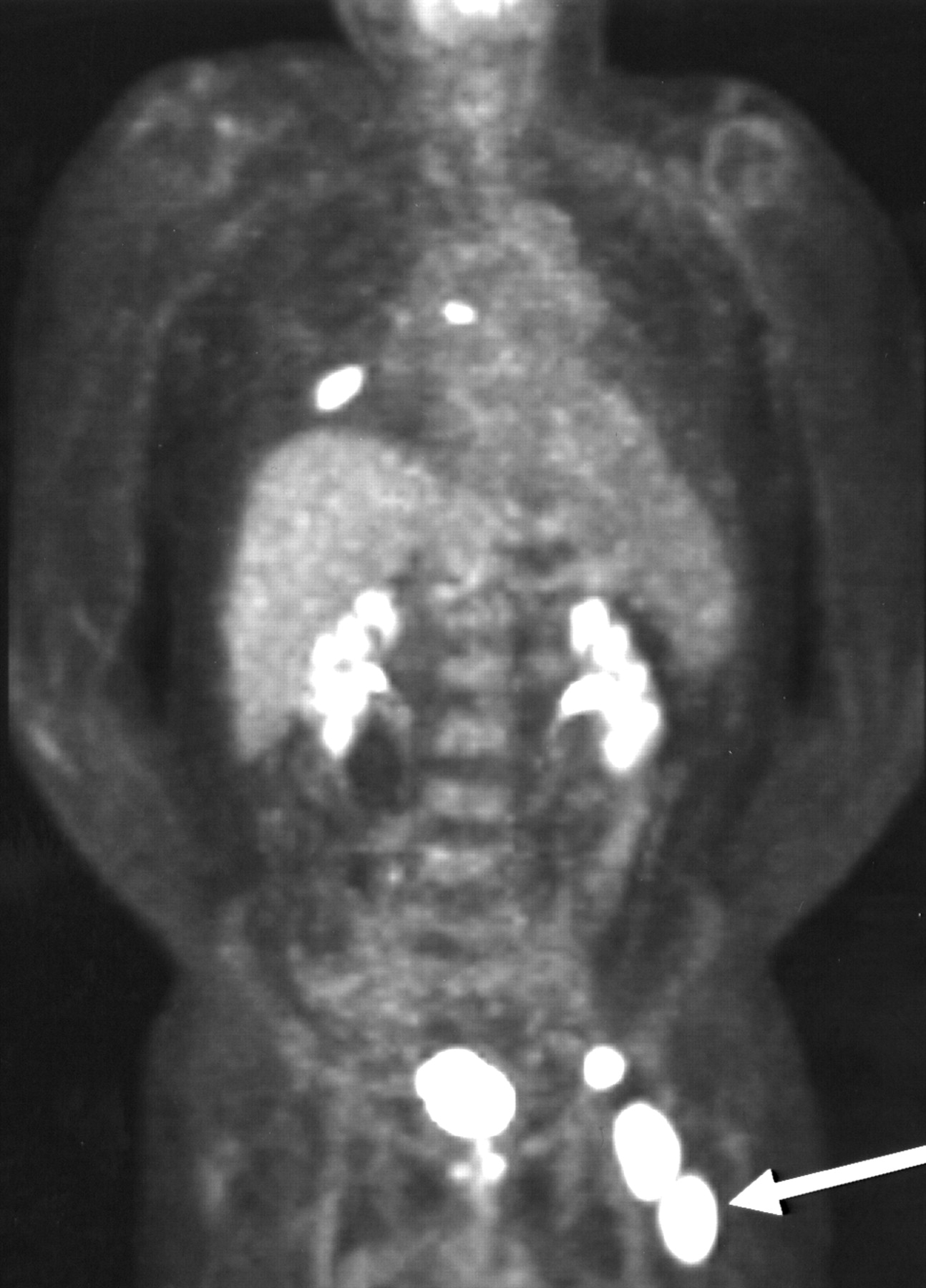
PET image of patient 8, who had Hürthle cell cancer previously treated and who returned with elevated thyroglobulin level (800 ng/mL) for evaluation. Neck sonography and 131I scan had negative findings. PET image showed lung, vertebral body, and pelvis/femur (arrow) metastases. Biopsy of pelvis confirmed metastatic disease.

PET image of patient 9, who had Hürthle cell cancer previously treated and who returned for follow-up evaluation. Neck sonography showed 1-cm right-neck lymph node suggestive of Hürthle cell cancer. PET image showed variable nonspecific uptake in neck and chest, and no definite tumor was believed to be present. Biopsy 2 mo later of region seen on sonography confirmed disease (2/4 grade Hürthle cell cancer), which was also likely near right-lower-neck uptake seen on PET (arrow).
Patient Data
DISCUSSION
Hürthle cell carcinoma is an aggressive thyroid cancer that may require more aggressive locoregional therapy than other thyroid malignancies. This tumor is more commonly metastatic, and a thorough evaluation for distant metastasis is recommended. Hürthle cell carcinoma is also quite rare, with little published on imaging of this malignancy with PET.
In this review, we have shown that 18F-FDG PET is likely to show regions of active involvement by Hürthle cell cancer. Most areas of tumor demonstrated intense 18F-FDG uptake that was similar in intensity to that seen in other highly metabolically active malignancies. In the 1 case that was falsely negative on PET, other confounding uptake of 18F-FDG in the neck may have hampered the detection of a small focus (1 cm) of disease. The disease in this case was also of low grade (2/4), possibly reducing 18F-FDG uptake. Retrospective review of this case showed that moderate uptake was present in the region of the disease but was difficult to detect. New advances such as PET/CT fusion may improve the accuracy of PET in such cases.
PET provided additional information on disease extent that led to a change in patient care for 50% (7/14) of the scans obtained. The change in care was due to better characterization of indeterminate abnormalities on CT or sonography for 3 scans and to detection of unsuspected disease for 4 scans. The contribution of PET in the patient group was dramatic and certainly comparable with other data reporting clinical management changes resulting from PET in other 18F-FDG–avid malignancies such as colorectal and lung cancer (12). Our data support the results of Plotkin et al. (11), who described accurate identification of Hürthle cell carcinoma by 18F-FDG PET in a group of 17 patients with indications of recurrent disease.
Our data are limited in that the number of patients in our study was low. However, considering that this malignancy is uncommon, larger groups of patients will be difficult to obtain. Another limitation is that this study was a retrospective review, with all the inherent biases of such. Referral of these study patients for PET may well have been prompted by existing clinical dilemmas. The high rate with which PET affected management could thereby be somewhat exaggerated and might not be seen in a group of patients who are referred prospectively.
CONCLUSION
Hürthle cell carcinoma demonstrates intense uptake on 18F-FDG PET. Relative to anatomic or iodine imaging, PET improved staging and disease management in patients with Hürthle cell carcinoma. 18F-FDG PET should be recommended for the evaluation and clinical management of patients with Hürthle cell carcinoma.
Footnotes
Received Oct. 15, 2002; revision accepted May 15, 2003.
For correspondence or reprints contact: Val J. Lowe, MD, PET Imaging, Section of Nuclear Medicine, Charlton 1N-215, Mayo Clinic, Rochester, MN 55905.
E-mail: vlowe{at}mayo.edu
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Effectors enabling adaptation to mitochondrial complex I loss in Hürthle cell carcinoma
- IMAGING IN ENDOCRINOLOGY: 2-[18F]-fluoro-2-deoxy-D-glucose positron emission tomography/computed tomography in differentiated thyroid carcinoma: clinical indications and controversies in diagnosis and follow-up
- NCCN Task Force: Clinical Utility of PET in a Variety of Tumor Types
- The role of F-18-fluorodeoxyglucose positron emission tomography in the postoperative evaluation of differentiated thyroid cancer
- Diagnostic Accuracy and Prognostic Value of 18F-FDG PET in Hurthle Cell Thyroid Cancer Patients
- Empirically Treating High Serum Thyroglobulin Levels