


Abstract
The purpose of this study was to describe the clinical presentation of bone metastases in patients with carcinoid tumors and to determine the diagnostic value of imaging techniques and markers of bone metabolism. Methods: This retrospective study was performed on the entire group of patients with carcinoid tumors treated in our hospital from January 1992 to May 1999. Only patients with metastasized tumors were included. Results: Eleven of 90 patients (12%) (95% confidence interval [CI], 5%–19%) with a metastasized carcinoid tumor had symptomatic bone metastases. All bone metastases occurred in 55 patients with midgut carcinoids (20%; 95% CI, 9%–31%). Plain radiography had a sensitivity of 44% (95% CI, 12%–76%); MRI, 100% (95% CI, 61%–100%); bone scintigraphy, 90% (95% CI, 72%–100%); and octreotide scintigraphy, 60% (95% CI, 35%–93%). In 9 patients, both octreotide scintigraphy and bone scintigraphy were performed. Of 45 bone lesions, 22 (49%) were visualized by both modalities, 13 (29%) were visualized with octreotide scintigraphy but not with bone scintigraphy, and 10 (22%) were visualized with bone scintigraphy but not with octreotide scintigraphy. In 2 patients, octreotide scintigraphy and bone scintigraphy provided complementary results. Markers of bone metabolism could not discriminate carcinoid patients from those without bone metastases. The markers of bone metabolism did not reflect the osteolytic or osteoblastic appearance of metastases. Conclusion: Pain is the principal symptom of bone metastases in patients with carcinoid tumors. Plain radiography and markers of bone metabolism do not contribute to the diagnosis of bone metastases. MRI has a high sensitivity for bone metastases. Both bone scintigraphy and octreotide scintigraphy have acceptable sensitivity and can provide complementary results.
The clinical presentation of carcinoid tumors is dominated by symptoms caused by amines secreted by the tumor. The classical carcinoid syndrome with diarrhea, flushing, bronchial obstruction, and carcinoid heart disease correlates with the serotonin-secreting activity of the tumor (1,2). Recently, improved control of the carcinoid syndrome with somatostatin analogs (3,4) and interferon-α (5,6) has changed the clinical presentation of carcinoid tumors. However, these agents failed to reduce the rate of tumor progression (3,7,8). As a result, symptoms related to tumor growth can prevail over metabolic symptoms. Consequently, a precise staging is of increasing importance for optimal management of carcinoid patients. The availability of partial liver resections and, in selected cases, liver transplantation (9–11) emphasizes the need for a thorough staging procedure (9).
Despite the increasing need for precise staging, bone metastases may frequently remain undetected. This is suggested by the discrepancy observed between clinically detected bone metastases and postmortem findings. Bone metastases were clinically detected in 11 of 274 patients with advanced carcinoid tumors (4%) (95% confidence interval [CI], 2%–6%) (12). In contrast to this relatively low rate, autopsy revealed a higher rate (42%) (95% CI, 26%–58%) of bone metastases in 36 patients with advanced carcinoid tumors (13).
In noncarcinoid tumors the diagnosis of bone metastases is established by plain radiography, bone scintigraphy, and MRI (14–16). Although markers of bone metabolism have a limited role in the diagnosis and follow-up of bone metastases, these markers may provide insight in their osteolytic or osteoblastic nature (17–20). Octreotide scintigraphy is used as a sensitive first step in the staging of carcinoid tumors (21). However, the sensitivity of octreotide scintigraphy for bone metastases remains to be determined.
In this retrospective study we describe the clinical presentation of bone metastases in patients with carcinoid tumors. Furthermore, we compare the sensitivity of plain radiography, MRI, bone scintigraphy, and octreotide scintigraphy for the detection of bone metastases. Finally, we evaluate the osteolytic or osteoblastic nature of bone metastases using markers of bone metabolism.
MATERIALS AND METHODS
Patients
Patients with bone metastases were identified among 90 carcinoid patients with metastases who were treated in the University Hospital Groningen during the period from January 1992 to May 1999. Assessment for the presence of bone metastases was initiated in patients having clinical symptoms suggestive for bone metastases. These symptoms comprised pain, fractures, or hypercalcemia that was not otherwise explained. The presence of bone metastases was confirmed by plain radiography, MRI, bone scintigraphy, or octreotide scintigraphy. We used the combination of these imaging procedures as an integrated standard for the presence of bone metastases because obtaining histologic proof was impractical. Because reference ranges for markers of bone metabolism are not available, each patient with bone metastases was matched with 1 control carcinoid patient without bone metastases. Matching was achieved for sex, age, and primary site of the carcinoid tumor (22).
Imaging Procedures
Plain skeletal radiography of sites with clinically suspected bone metastases was performed in 2 perpendicular directions according to standard procedures.
MRI was performed with a 1.0-T unit (Magnetom Impact; Siemens, Erlangen, Germany). Sites with suspected bone metastases were investigated with adjacent slices of 6- to 10-mm thickness, using the turbo inversion recovery modulus.
Whole-body bone scintigraphy was performed 3–4 h after intravenous injection of 600–700 MBq 99mTc-methylenediphosphonate, using a large field-of-view double-head gamma camera (Multispect 2; Siemens Inc, Hoffman Estates, IL), together with a low-energy, high-resolution collimator.
For octreotide scintigraphy, planar images were acquired 24 h after intravenous administration of 200 MBq 111In-octreotide (Octreoscan; Mallinckrodt, Petten, The Netherlands). For acquisition, the same camera system as that used for bone scintigraphy was used, but with a medium-energy, all-purpose collimator. SPECT was performed when planar images were equivocal.
All imaging procedures were serially evaluated by investigators experienced in radiology or nuclear medicine. The sites of bone metastases were described in detail and the osteolytic or osteoblastic appearance on plain radiography was specified. An analysis was performed on a patient-by-patient basis to enable comparison between the respective imaging procedures. Because bone scintigraphy and octreotide scintigraphy both visualize the whole body, a lesion-by-lesion analysis could be used to compare the sensitivity of these techniques.
Markers of Serotonin Metabolism
Urinary 5-hydroxyindoleacetic acid (5-HIAA) concentration and platelet serotonin content were determined in a 24-h urine collection and in platelet-rich plasma by high-performance liquid chromatography with fluorometric detection. The reference interval for urinary 5-HIAA ranges from 0.8 to 3.8 mmol/mol creatinine. Platelet serotonin content, expressed as nanomoles per 109 platelets, was calculated by dividing the serotonin concentration in platelet-rich plasma by the concentration of platelets. The reference interval for platelet serotonin content ranges from 2.8 to 5.4 nmol per 109 platelets. A detailed description of the sampling procedures and analytic methods for urinary 5-HIAA and platelet serotonin has been published (23).
Markers of Bone Metabolism
In the patients with bone metastases, and in the control carcinoid patients without bone metastases, markers of bone metabolism were determined retrospectively in serum. The samples had been stored at −20°C until analysis. We preferred the measurement of recently developed, more specific markers (17,20) of bone metabolism. The serum bone-specific alkaline phosphatase (BSAP) activity and the amino-terminal propeptide of type I procollagen (PINP) concentration in serum were determined as markers of osteoblastic activity or bone formation. The serum concentration of the cross-linked amino-terminal telopeptide of type I collagen (NTx) was determined as a marker of osteoclastic activity or bone resorption. The serum BSAP activity was measured with the Metra-Biosystems immunoassay (Mountain View, CA). The BSAP assay has a reference range of 9–23 U/L and intra- and interassay coefficients of variance of 4.9% and 5.5%, respectively. The PINP concentration in serum was measured using a radioimmunoassay (Orion Diagnostica, Espoo, Finland). The reference range of the PINP assay is 20–70 μg/L; the intra- and interassay coefficients of variance are 8.4% and 9.0%, respectively. The NTx serum concentration was measured using the Osteomark NTx Serum immunoassay (Ostex International, Seattle, WA). This NTx assay has a reference range of 5–24 nmol/L bone collagen equivalents per liter and has intra- and interassay coefficients of variance of 7.3% and 6.9%, respectively.
Statistics
Differences in the number of bone metastases in midgut versus foregut carcinoids were evaluated using χ2 statistics. To compare the respective imaging modalities, we used the McNemar test together with the Fisher exact test.
To compare markers of bone metabolism between patients with bone metastases and the matched control patients, the Wilcoxon signed-rank test was used. Correlations between the respective markers of serotonin and bone metabolism were calculated with the Pearson correlation for markers with a normal distribution and the Spearman rank correlation for markers with a non-normal distribution. P < 0.05 was considered statistically significant.
RESULTS
Table 1 presents the frequency of bone metastases in relation to the primary site of the tumor. Of the 90 patients at risk, 24 were evaluated for suspected bone metastases. Eleven patients with bone metastases were identified within the 90 patients at risk (12%) (95% CI, 5%–19%). All patients with bone metastases had tumors originating from the midgut region. Ten of the 11 patients with bone metastases had skeletal pain; 1 of these 10 patients also had a pathologic fracture. In 1 asymptomatic patient, bone metastases were detected with octreotide scintigraphy performed as a staging procedure. No hypercalcemic episodes were observed. Table 2 summarizes the clinical and biochemical characteristics of the patients with bone metastases.
Patients with Bone Metastases in Relation to Primary Site of Tumor
Clinical and Biochemical Characteristics of Carcinoid Patients With and Without Bone Metastases
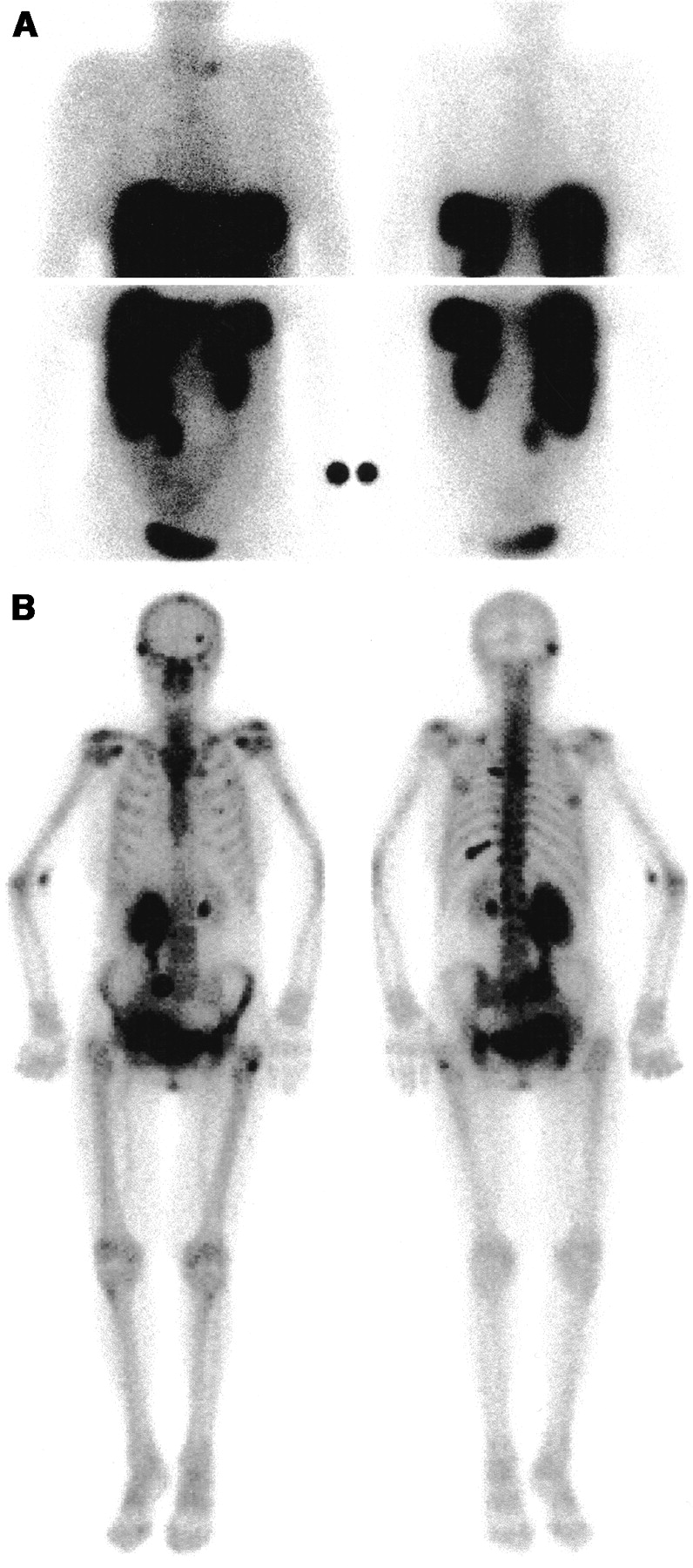
The outcomes of the imaging procedures are specified in Table 3. To enable comparison between local techniques (plain radiography and MRI) and whole-body imaging techniques (octreotide scintigraphy and bone scintigraphy), sensitivity was calculated on a patient-by-patient basis. Plain radiography showed osteolytic bone metastases in patients 3 and 11, whereas an osteoblastic appearance was found in patients 4 and 8. Because of the small number of patients with bone metastases, no differences between the sensitivity of the respective imaging modalities were detectable. The numbers of bone lesions visualized with bone scintigraphy and octreotide scintigraphy were compared on a lesion-by-lesion basis in 9 patients who underwent both procedures (Table 4). The interval between both scintigraphic procedures ranged from 0 to 9 mo (median, 3 mo). In the 11 patients with bone metastases, 45 bone lesions were visualized (Table 4). Twenty-two lesions were visible with both octreotide scintigraphy and bone scintigraphy (49%) (95% CI, 34%–64%). Octreotide scintigraphy but not bone scintigraphy revealed 13 bone lesions (29%) (95% CI, 16%–42%). The remaining 10 bone lesions were visualized with bone scintigraphy but not octreotide scintigraphy (22%) (95% CI, 10%–34%). In 3 patients (patients 4, 9, and 11), bone scintigraphy showed lesions not detected with octreotide scintigraphy (Fig. 1). One patient (patient 10) had a bone lesion visualized with octreotide scintigraphy but not with bone scintigraphy. In the remaining patients, octreotide scintigraphy and bone scintigraphy provided complementary results (Fig. 2).
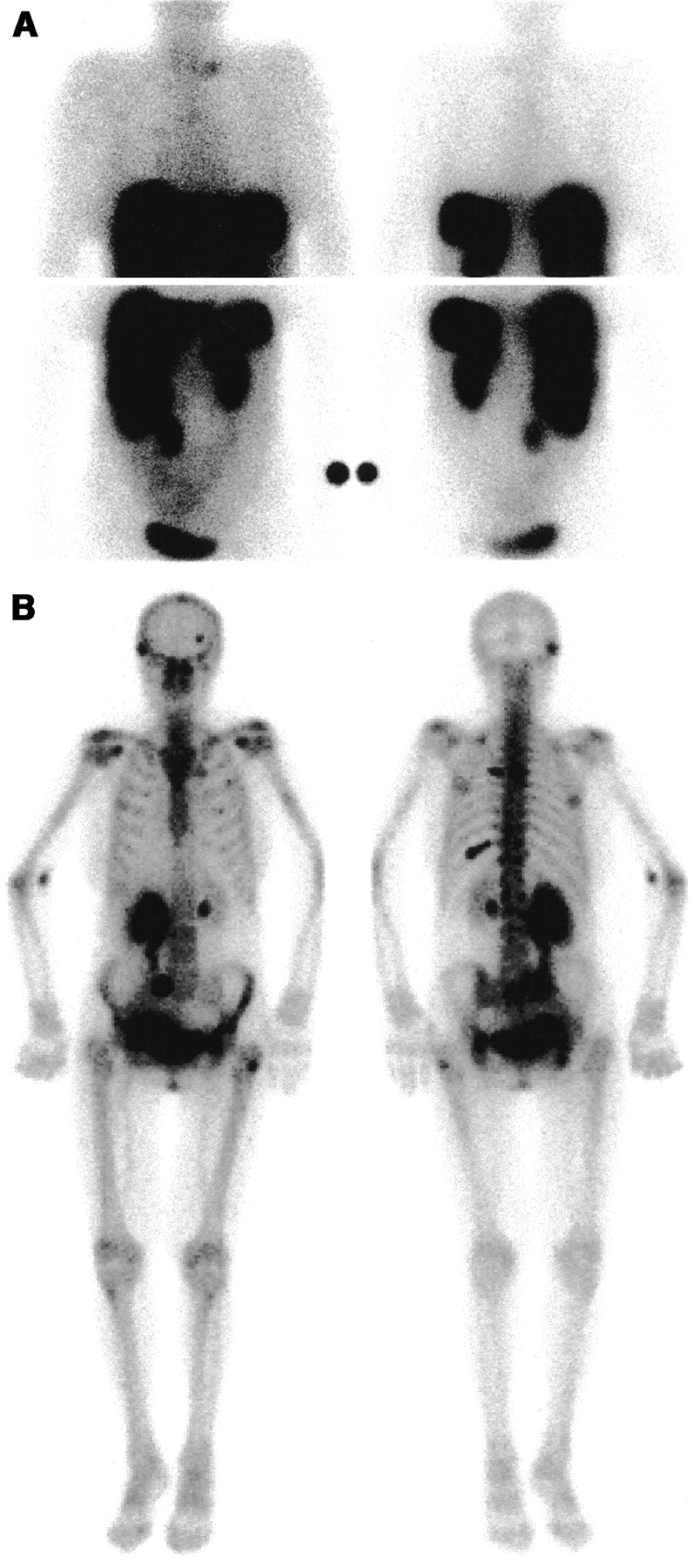
Visualization of bone metastases by bone scintigraphy (B) but not by octreotide scintigraphy (A) in 70-y-old female midgut carcinoid patient (patient 9). Upper panel (A) and left panel (B) represent anterior images. Bone lesions are present in vertebral body thoracic 5, dorsal part of left costa 5 and costa 10. Lesions located in skull and left femur are not accurately visualized with octreotide scintigraphy. Note hydronephrosis of right kidney.
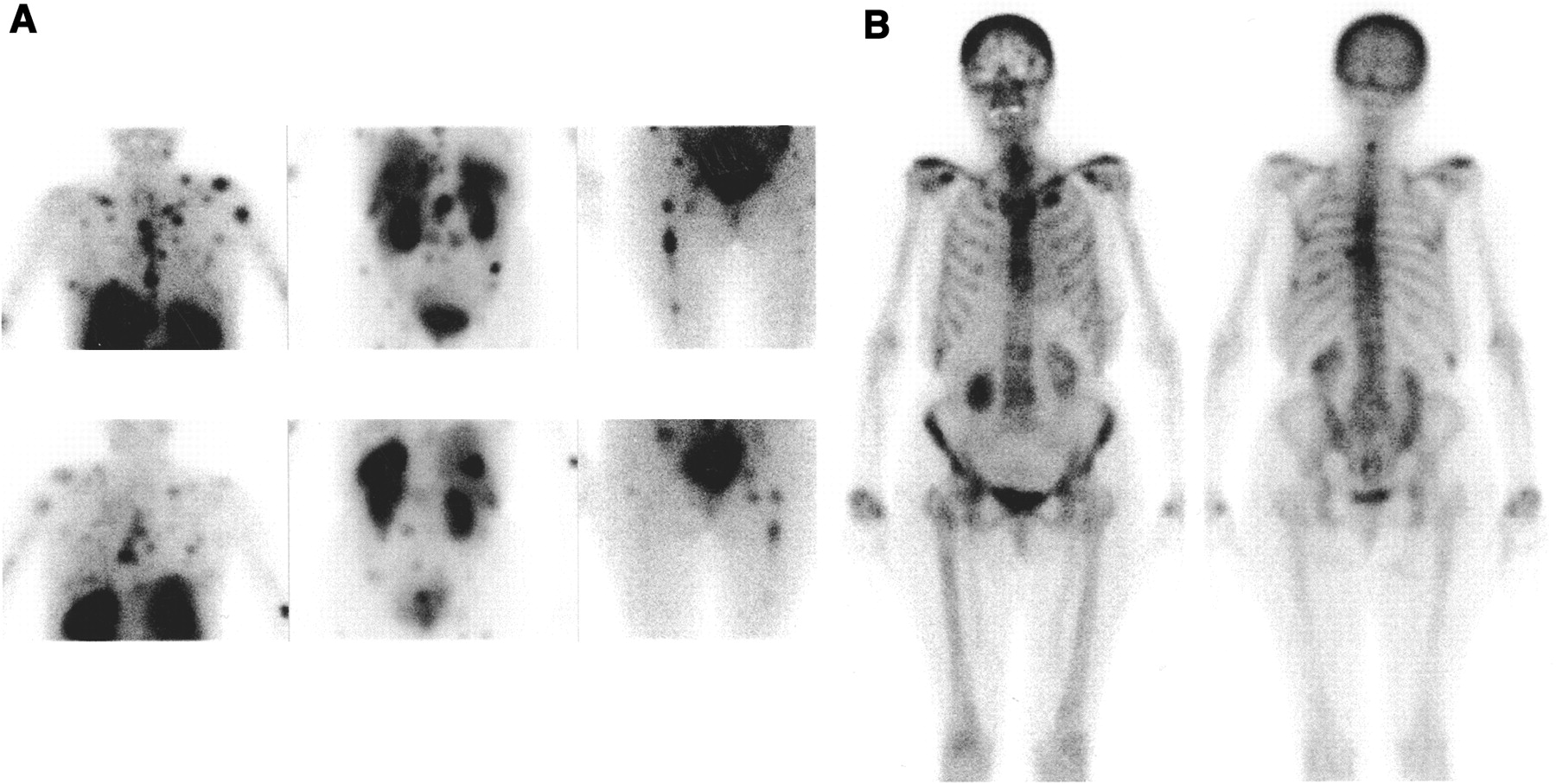
Complementary visualization of bone metastases by octreotide scintigraphy (A) and bone scintigraphy (B) in 63-y-old female midgut carcinoid patient (patient 6). Octreotide scintigraphy visualizes bone metastases in left humerus, pelvis, and bilateral femur. Cervical vertebral hot spot is visualized by bone scintigraphy but not by octreotide scintigraphy. Hot spots located in thoracic skeleton and lumbar spine are visible with both investigations.
Clinical Characteristics and Outcome of Imaging Techniques in Patients with Bone Metastases of Carcinoid Tumors
Visualization of Bone Metastases: Bone Scintigraphy Compared with Octreotide Scintigraphy
Markers of bone metabolism were determined in all patients with bone metastases and in 11 control carcinoid patients without bone metastases (Table 1). The measurements of BSAP, PINP, and NTx did not distinguish patients with bone metastases from those without bone metastases (Fig. 3). Furthermore, the number of patients with markers of bone metabolism exceeding the upper reference limit was equally distributed over the patients with and without bone metastases (Fig. 3). One of the 2 patients with osteolytic metastases (patient 3) on plain radiography showed an elevated concentration of NTx. One of the 2 patients with osteoblastic metastases (patient 8) had an elevated PINP concentration. PINP correlated with NTx within the total group of 22 patients (Pearson r = 0.65; P < 0.001) but not with BSAP. The markers of bone metabolism did not correlate with urinary 5-HIAA excretion, somatostatin analog treatment, age, or time from diagnosis.
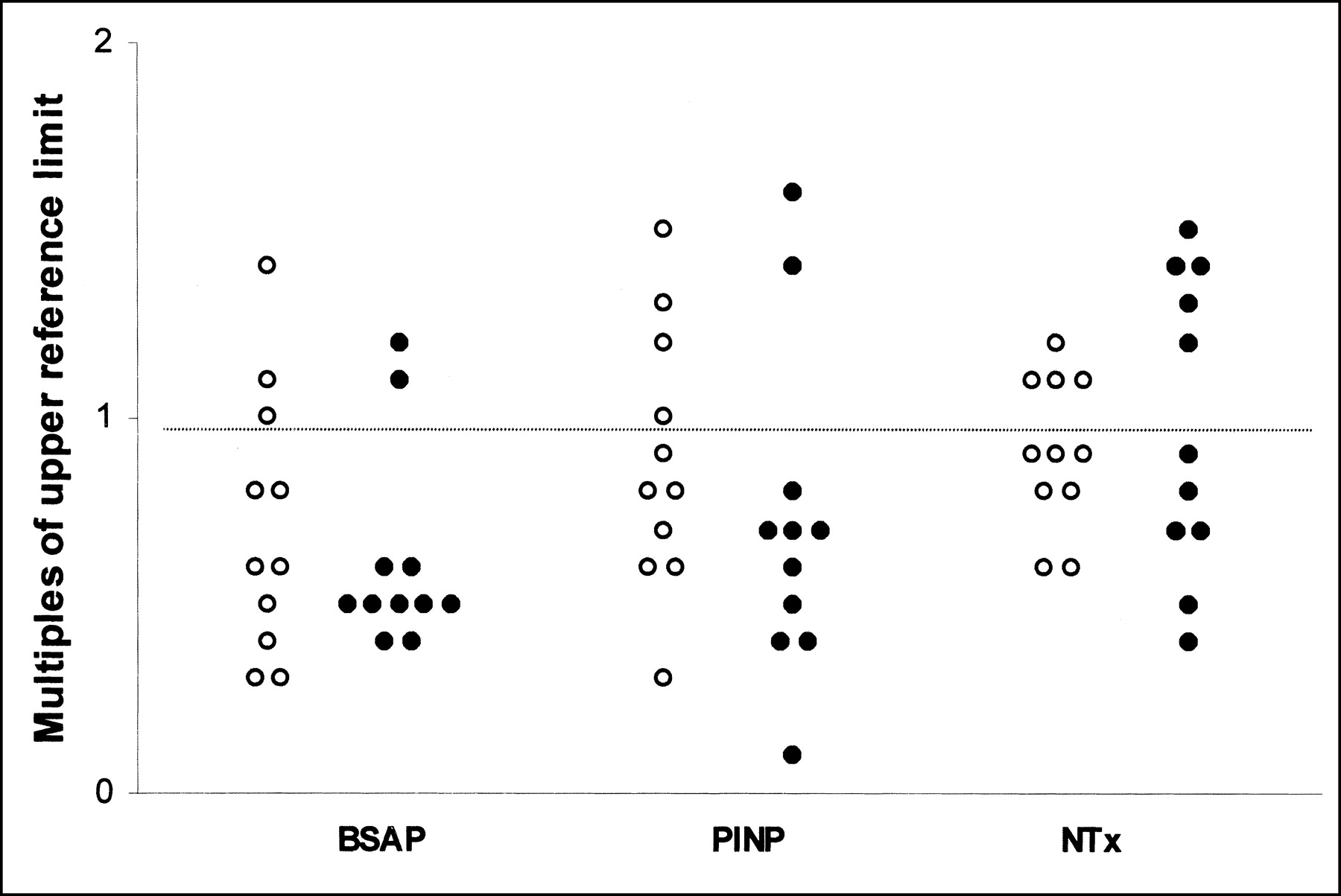
Multiples of upper reference limits of BSAP, PINP, and NTx. (○), Patients without bone metastases; (•), patients with bone metastases. Horizontal dotted line represents upper reference limit.
DISCUSSION
In this retrospective study we found bone metastases in 12% of 90 carcinoid patients with metastases. The frequency of bone metastases in our patients is higher than that in the study by Janson et al. (12), who described 11 patients with bone metastases among 301 carcinoid patients, of whom 274 had metastasized tumors (12% vs. 4%; P = 0.01). More recent studies (9,24–26), evaluating the use of octreotide scintigraphy in carcinoid tumors, describe a rate of bone metastases between 7% and 15%. These rates are in agreement with our study.
A possible explanation for the high rate of bone metastases in the later studies could arise from the therapeutic use of somatostatin analogs and interferon-α. These agents relieve symptoms mediated by amines secreted by the tumor (1,3,6,27) but have only a limited effect on tumor growth (3,7). As a result, these agents can lead to a prolonged survival and a greater impact of symptoms related to tumor growth. In this situation, bone metastases, associated with advanced disease, may increasingly cause symptoms in carcinoid patients. An additional explanation for the high rate of bone metastases could be that the use of octreotide scintigraphy also reveals asymptomatic bone metastases, leading to a higher rate of bone metastases. However, only 1 of our patients had asymptomatic bone metastases detected by octreotide scintigraphy.
All of our patients with bone metastases had a carcinoid tumor from midgut origin. However, because of the small numbers of patients with bone metastases, we could not recognize a difference between midgut and foregut carcinoid patients. In contrast to our results, an earlier study (12) described a higher rate of bone metastases in 39 patients with foregut carcinoids (23%) (95% CI, 10%–36%) than in patients with midgut carcinoids (1%) (95% CI, 0%–2%). Accordingly, the patients with bone metastases described in several case reports (28–30) had predominantly tumors from foregut origin.
Although our study is limited by its retrospective character, some clinical features deserve attention. All patients with bone metastases in our study had advanced disease, characterized by widespread metastases, elevated markers of serotonin metabolism, and the carcinoid syndrome. This could indicate that bone metastases occur in long-lasting disease.
The interval between diagnosis of a carcinoid tumor and the appearance of bone metastases shows a wide range within our patients. This is probably related to the indolent course of the disease and its difficult diagnosis. Although 2 patients had bone metastases at the time of diagnosis of the carcinoid tumor, all patients had bone metastases together with widespread extraosseous metastases (Table 2). Bone metastases were located predominantly in the axial skeleton; this distribution is comparable to that found in noncarcinoid tumors (31). Pain was the principal symptom in our patients. Bone metastases seem to follow a relatively uncomplicated course, which possibly results from the slow rate of growth that is characteristic of carcinoid tumors.
In our study the sensitivity for bone metastases ranged from 44% for plain radiography, 70% for octreotide scintigraphy, and 90% for bone scintigraphy to 100% for MRI. The small number of patients with bone metastases resulted in wide confidence intervals (Table 3). As a consequence, no significant differences between the sensitivity of the respective techniques were found. Only a limited number of previous studies address the imaging of bone metastases in patients with carcinoids and related neuroendocrine tumors. These studies describe small numbers of patients, comparable with our study. In a study of patients with gastrinoma (32), bone scintigraphy correctly diagnosed 5 of 8 patients with bone metastases. In their study, octreotide scintigraphy and MRI identified 6 and 7, respectively, of the 8 patients with bone metastases. The authors advocate the use of octreotide scintigraphy as a first step in the diagnosis of bone metastases. A second study (33), performed on patients with neuroendocrine tumors, compared octreotide scintigraphy with MRI. Octreotide scintigraphy showed bone metastases in 3 of 10 patients, whereas MRI identified all 10 patients with bone metastases. In another study (34) of 145 patients with gastroenteropancreatic neuroendocrine tumors, 19 (13%) were identified as having bone metastases. Octreotide scintigraphy showed bone metastases in all 19 patients, whereas bone scintigraphy showed bone metastases in 17 of 19 patients. Four of the 30 carcinoid patients included in this study (34) had bone metastases. In a recent study (35), octreotide scintigraphy showed bone lesions in 23 of 26 carcinoid patients with bone metastases (88%).
MRI appeared to be the most sensitive imaging technique in our study. This finding agrees with studies on noncarcinoid bone metastases (15,16,36,37). In these studies, MRI had a slightly higher sensitivity and specificity for bone metastases than bone scintigraphy. A disadvantage of MRI is that only a restricted part of the skeleton can be visualized in 1 investigation. Both bone scintigraphy and octreotide scintigraphy have the advantage of imaging the whole body.
Octreotide scintigraphy has a prominent role in the detection of tumor deposits in carcinoid tumors (21). However, our results suggest that the sensitivity for bone metastases is higher for bone scintigraphy than for octreotide scintigraphy. Bone scintigraphy identified more patients with bone metastases than octreotide scintigraphy. Furthermore, the number of lesions visualized with bone scintigraphy was higher than that with octreotide scintigraphy. Nevertheless, both scintigraphic procedures showed bone lesions not detected by the other scintigraphic techniques (Table 4; Fig. 2). Therefore, bone scintigraphy and octreotide scintigraphy can provide complementary information about the presence of bone metastases. The combination of bone scintigraphy and octreotide scintigraphy identified all patients with bone metastases in our study. Probably, there are 2 factors determining whether a bone lesion can be visualized by 1 or both scintigraphic procedures. Visualization by bone scintigraphy identifies those metastases that induce an osteoblastic reaction. On the other hand, visualization by octreotide scintigraphy requires the presence of octreotide receptors. The complementary imaging of bone metastases suggests that bone metastases can show different imaging characteristics in 1 patient.
To our knowledge, the role of markers of bone metabolism in carcinoid patients has not been investigated previously. In our study, the measurement of BSAP, PINP, and NTx did not distinguish patients with bone metastases. Furthermore, formation markers were not preferentially elevated compared with resorption markers (Fig. 3) and, therefore, failed to reflect the predominantly osteoblastic appearance that is described for bone metastases from carcinoid tumors (28,29). The low sensitivity of the markers of bone metabolism is possibly explained by one of the following mechanisms. Because carcinoids are slowly growing tumors, bone metastases may have only limited impact on the metabolism of the surrounding normal bone. These minor changes in bone metabolism are not easily detected. Furthermore, somatostatin analogs inhibit the pituitary secretion of growth hormone, resulting in low levels of insulin-like growth factor I (38). This inhibition possibly affects bone metabolism and can, therefore, influence markers of bone metabolism. Finally, serotonin exerts a stimulating effect on collagen formation, mediated by transforming growth factor-β (39,40). Because carcinoids produce excessive amounts of serotonin, a stimulated collagen formation may obscure small changes in bone collagen metabolism. Possibly because of these interfering mechanisms, markers of bone metabolism are not sensitive enough to detect the predominantly osteolytic or osteoblastic behavior of bone metastases.
CONCLUSION
Our study shows that bone metastases have a high rate (20%) in patients with disseminated midgut carcinoids. This contrasts with previous studies describing bone metastases predominantly in patients with foregut carcinoids. Octreotide scintigraphy is recommended as an initial staging procedure in carcinoid patients. Those patients with symptoms suggesting bone metastases or suspected bone metastases on octreotide scintigraphy need additional imaging with bone scintigraphy or MRI. Bone scintigraphy and octreotide scintigraphy can provide complementary information on the presence of bone metastases. Markers of bone metabolism do not contribute to the diagnosis of bone metastases in carcinoid patients.
Footnotes
Received Jan. 17, 2002; revision accepted Aug. 23, 2002.
For correspondence or reprints contact: Elisabeth G.E. de Vries, MD, PhD, Department of Medical Oncology, University Hospital Groningen, P.O. Box 30.001, 9700 RB Groningen, The Netherlands.
E-mail: e.g.e.de.vries{at}int.azg.nl
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Bone metastases and skeletal-related events from neuroendocrine tumors
- Tumor Response Assessment to Treatment with [177Lu-DOTA0,Tyr3]Octreotate in Patients with Gastroenteropancreatic and Bronchial Neuroendocrine Tumors: Differential Response of Bone Versus Soft-Tissue Lesions
- Response and Long-Term Control of Bone Metastases After Peptide Receptor Radionuclide Therapy with 177Lu-Octreotate
- Bone Metastases in Patients with Neuroendocrine Tumor: 68Ga-DOTA-Tyr3-Octreotide PET in Comparison to CT and Bone Scintigraphy
- Metastatic Carcinoid Tumors: A Clinical Review