


Abstract
The purpose of this retrospective analysis was to evaluate the prognostic significance of both initial glucose metabolism as measured by 18F-FDG PET and osteoblastic activity as measured by 99mTc-methylene diphosphonate (MDP) bone scintigraphy in osteosarcoma. Methods: In 29 patients (18 male, 11 female; age range, 5–41 y) with primary osteosarcoma, 18F-FDG uptake and 99mTc-MDP uptake were measured semiquantitatively (average and maximum tumor-to-nontumor ratios [T/NTav and T/NTmax, respectively]) using PET and bone scintigraphy at the time of diagnosis. After chemotherapy, the patients underwent surgery for their primary tumor, and the response was determined histologically. Cumulative overall survival and event-free survival were determined by clinical and imaging follow-up of 7–72 mo (median, 28 mo). Results: Clinical and imaging follow-up revealed that the disease relapsed or failed to achieve complete remission in 9 patients and that 6 patients died of the disease. Both overall and event-free survival were significantly better in patients with a low 18F-FDG T/NTmax (less than the median) than in patients with a high 18F-FDG T/NTmax (at least the median). The negative relationship of 18F-FDG T/NTav, 99mTc-MDP T/NTmax, and 99mTc-MDP T/NTav with overall and event-free survival did not reach a level of significance. 18F-FDG uptake values correlated moderately and positively with 99mTc-MDP uptake values, but a level of significance was reached only between 18F-FDG T/NTmax and 99mTc-MDP T/NTav. Conclusion: The initial glucose metabolism of primary osteosarcoma as measured by 18F-FDG PET using T/NTmax provides prognostic information. High 18F-FDG uptake correlates with poor outcome. Thus, 18F-FDG uptake may be complementary to other well-known factors in judging the prognosis in osteosarcoma.
Musculoskeletal malignancies usually metabolize glucose at an increased rate, and 18F-FDG PET can thus be used for grading and characterizing their biologic aggressiveness (1,2). In osteosarcoma, measurement of changes in glucose metabolism using 18F-FDG PET appears to be a good noninvasive way to determine the response to neoadjuvant chemotherapy (3,4). More recently, glucose metabolism at the time of diagnosis has been shown to predict prognosis in some types of solid tumors, such as lung cancer and pancreatic carcinoma (5–9). A systematic evaluation of the prognostic value of initial glucose metabolism in osteosarcoma has not yet been reported. Furthermore, for tumor cells in other malignancies, specific capabilities such as uptake of 131I indicate differentiation and imply a good prognosis (10). In the case of osteosarcoma, the production of primitive osseous matrix is a specific capability of the tumor cells. The aim of this retrospective analysis of osteosarcoma patients was to evaluate the prognostic importance of initial glucose metabolism as measured by 18F-FDG PET and of osteoblastic activity as measured by 99mTc-methylene diphosphonate (MDP) bone scintigraphy.
MATERIALS AND METHODS
Patient Population
Primary osteosarcoma was diagnosed in all patients, and all underwent both 18F-FDG PET and bone scintigraphy at the time of the initial diagnosis, before beginning chemotherapy. The exclusion criteria were surgery before the nuclear medicine examinations or a pathologic fracture of the primary tumor site. Patients with primary metastatic disease were not excluded. Within a 5 -y period, 29 consecutive patients fulfilled these criteria (18 males, 11 females; age range, 5–41 y; median age, 14 y). All patients had high-grade osteosarcoma. Further detailed clinical information is given in Table 1. The size of the primary tumor was determined by morphologic imaging (MRI or CT). After biopsy and histologic confirmation, all patients underwent neoadjuvant chemotherapy with doxorubicin, high-dose methotrexate, cisplatin, and ifosfamide according to the respective Cooperative Osteosarcoma Study (COSS) protocols (COSS-86c, n = 7; COSS-96, n = 22), followed by surgical resection of the primary tumor site. Response was assessed histologically according to the classification of Salzer-Kuntschik et al. (11). A good response was assumed when tumor viability was <10%. Cumulative overall survival and event-free survival were determined by clinical and imaging follow-up of 7–72 mo (median, 28 mo).
-y period, 29 consecutive patients fulfilled these criteria (18 males, 11 females; age range, 5–41 y; median age, 14 y). All patients had high-grade osteosarcoma. Further detailed clinical information is given in Table 1. The size of the primary tumor was determined by morphologic imaging (MRI or CT). After biopsy and histologic confirmation, all patients underwent neoadjuvant chemotherapy with doxorubicin, high-dose methotrexate, cisplatin, and ifosfamide according to the respective Cooperative Osteosarcoma Study (COSS) protocols (COSS-86c, n = 7; COSS-96, n = 22), followed by surgical resection of the primary tumor site. Response was assessed histologically according to the classification of Salzer-Kuntschik et al. (11). A good response was assumed when tumor viability was <10%. Cumulative overall survival and event-free survival were determined by clinical and imaging follow-up of 7–72 mo (median, 28 mo).
Clinical, Imaging, and Follow-Up Patient Data
Imaging Techniques
18F-FDG PET scans were acquired as previously described (12). The patients had been fasting for at least 5 h before the 18F-FDG injection. No patient was known to have diabetes mellitus or a pathologic glucose tolerance. Blood glucose levels at the time of injection were <6.66 mmol/L in all patients. The first 20 18F-FDG PET examinations were done without attenuation correction. For the remaining 9 examinations, whole-body emission- transmission scanning was performed.
The procedure for planar 3-phase 99mTc-MDP bone scintigraphy has been described in detail (3). Total body imaging (anterior and posterior views) was performed 3–4 h after the injection using a Bodyscan (Siemens, Erlangen, Germany) at a speed of 15 cm/min. Additionally, static planar images of the primary tumor site in 2 planes were acquired. Low-energy, high-resolution collimators were used.
All patients, or the parents or legal guardians of minors, gave informed consent to all 18F-FDG PET and bone scintigraphy examinations, to participation in the COSS therapy studies, and to all surgical interventions.
Imaging Analysis
The images were analyzed by observers who were unaware of the clinical and histopathologic data. Only the primary tumor site and the age and sex of the patients were known by the observers.
On the 18F-FDG PET coronal slice expressing the highest uptake of the primary tumor site, rectangular regions of interest (ROIs) were manually defined using a 3-dimensional display technique (MPI-Tool; Advanced Tomo Vision, Erfstadt, Germany) (13). The boundaries of the ROIs were just within the apparent hypermetabolic zone of the tumor. ROIs of identical configuration were placed on the analogous site of the contralateral extremity. Tumor-to-nontumor ratios (T/NT) were calculated using the average (T/NTav) and maximum (T/NTmax) values within each tumor ROI and the average value within the nontumor ROI (2–4,14).
On bone scintigrams, identical rectangular ROIs were manually placed around clearly visible tumor activity and on the analogous site of the contralateral extremity. Epiphyseal plate activity was omitted. T/NTav was calculated in the usual way for all patients, and T/NTmax was calculated additionally for 23 patients (3,15,16).
Statistical Analysis
For each parameter, the median, 25th, and 75th percentiles are given. The significance of the difference in medians between 2 groups was tested using the 2-tailed Mann-Whitney test (17). The significance of the correlation between 2 parameters was assessed using Spearman rank correlation (18). Probability values < 0.05 were considered significant. The follow-up period was calculated from the time of diagnosis. An event was defined as local or distant relapse of disease or failure to achieve complete remission. Survival was analyzed using the Kaplan-Meier method (19). The log-rank test was used to compare actuarial survival probabilities (20). The median value was chosen as the cutoff level for all parameters to establish a low-uptake group and a high-uptake group (21).
RESULTS
18F-FDG and 99mTc-MDP Uptake
All primary osteosarcomas were clearly visible on both the 18F-FDG PET images and the bone scintigrams. The individual 18F-FDG and 99mTc-MDP uptake values are given in Table 1.
The median 18F-FDG T/NTs for the whole patient group were 4.5 for T/NTav (25th percentile, 3.7; 75th percentile, 6.8) and 12.6 for T/NTmax (25th percentile, 8.3; 75th percentile, 23.3) (r = 0.80; P < 0.001).
The median 99mTc-MDP T/NTs were 6.6 for T/NTav (25th percentile, 3.2; 75th percentile, 9.0) and 15.5 for T/NTmax (25th percentile, 12.8; 75th percentile, 28.9). A significant positive correlation was found between 99mTc-MDP T/NTav and 18F-FDG T/NTmax (r = 0.50; P = 0.005), but only a tendency toward a positive correlation was found between 99mTc-MDP T/NTav and 18F-FDG T/NTav (r = 0.36; P > 0.05), between 99mTc-MDP T/NTmax and 18F-FDG T/ NTav (r = 0.21; P > 0.05), and between 99mTc-MDP T/NTmax and 18F-FDG T/ NTmax (r = 0.33; P > 0.05). These 3 correlations did not reach statistical significance.
Histology, Regression Grade, and Size
Histologically, the response to chemotherapy was good in 20 patients and poor in 9 patients. No significant difference in 18F-FDG T/ NTav, 18F-FDG T/NTmax, 99mTc-MDP T/NTav, or 99mTc-MDP T/NTmax median values was found between the various osteosarcoma histology subtypes or the different regression grades. Additionally, no significant correlation was found between the size of the primary tumor and any of the semiquantitative uptake values (18F-FDG T/NTav, 18F-FDG T/ NTmax, 99mTc-MDP T/NTav, or 99mTc-MDP T/NTmax).
Survival
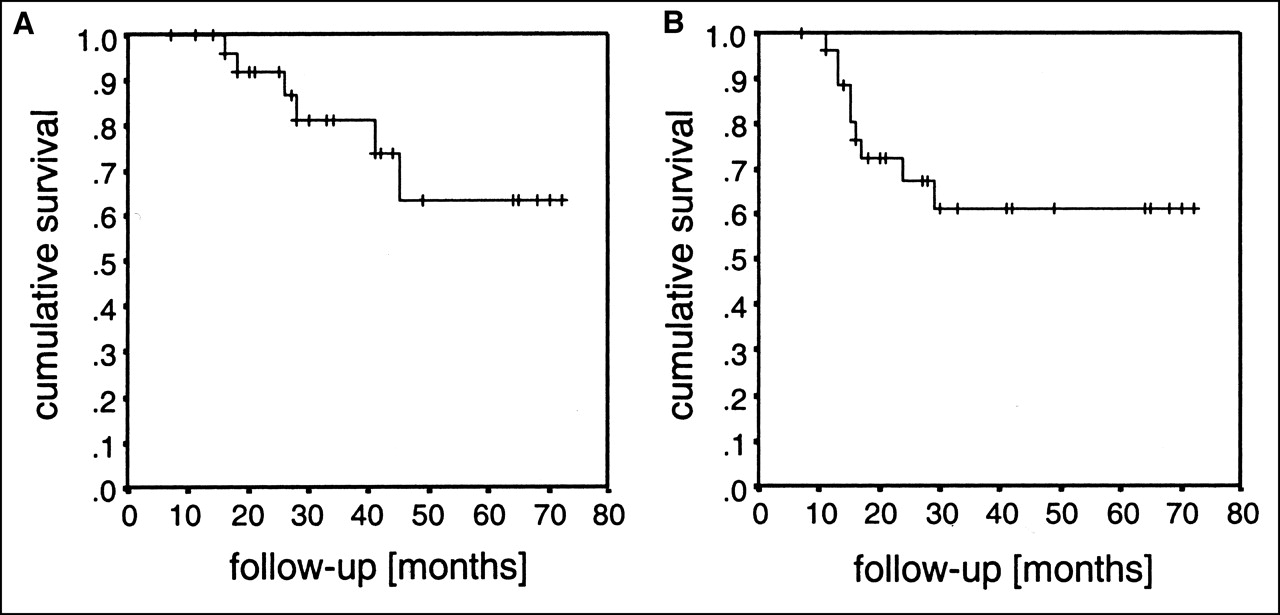
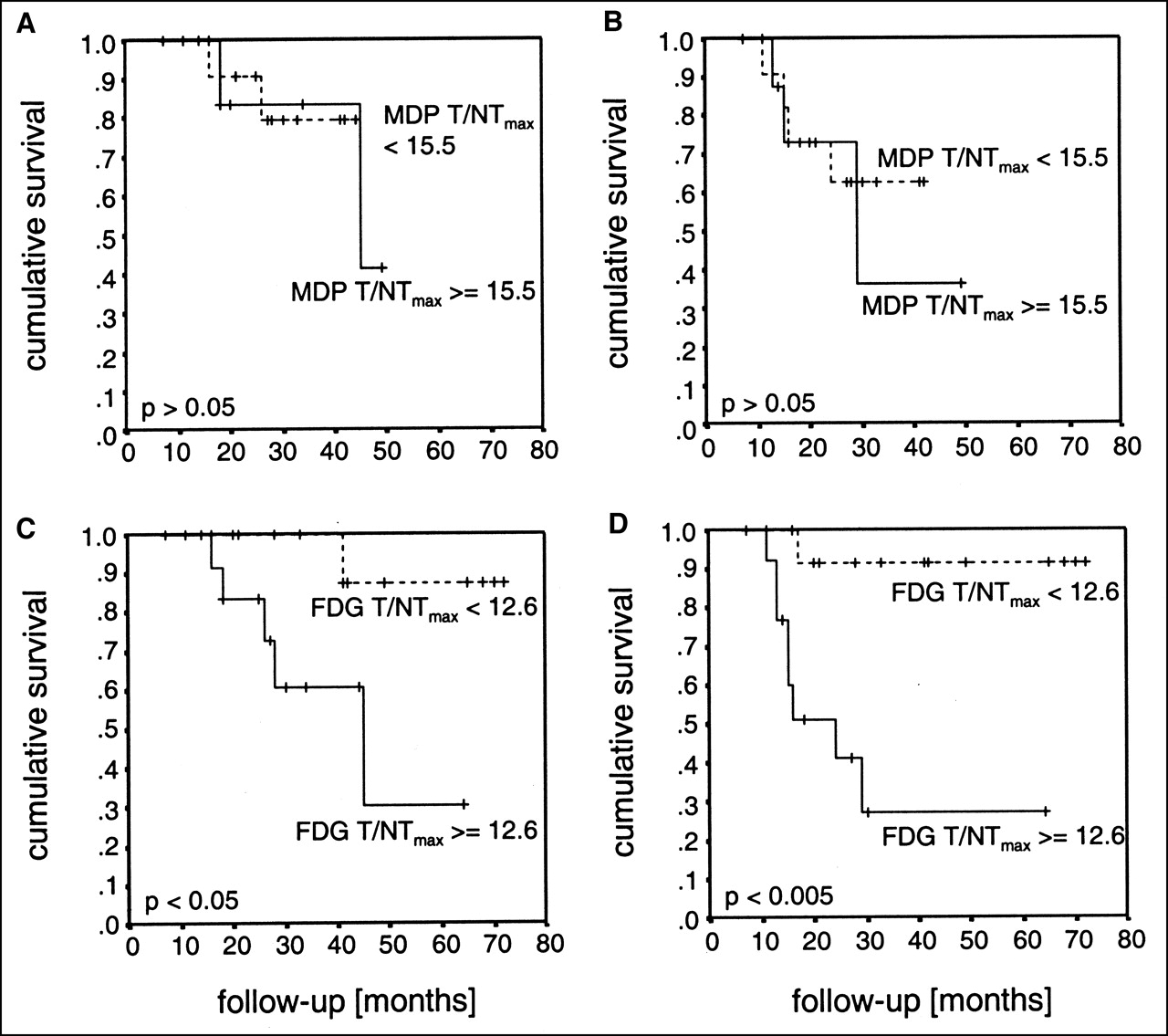
Clinical and imaging follow-up revealed an event in 9 patients (relapse of disease in 8 patients, failure to achieve complete remission in 1 patient). Six patients died of their disease (Table 1). For the whole patient group, actuarial overall survival and event-free survival at 72 mo were 0.63 and 0.61, respectively (Figs. 1A and 1B). Only 18F-FDG T/NTmax (18F-FDG T/NTmax ≥ median vs. 18F-FDG T/NTmax < median) correlated significantly with both overall survival (P < 0.05) and event-free survival (P < 0.005) (Figs. 2C and 2D). The influence of tumor 18F-FDG uptake was explored for various T/NTmax cutoff values. Using 18F-FDG T/NTmax, dichotomization with a broad range of T/ NTmax values gave significantly discriminative log-rank probability values for both overall survival (30th percentile to 50th percentile of 18F-FDG T/NTmax) and event-free survival (30th percentile to 60th percentile of 18F-FDG T/NTmax) (Figs. 3A and 3B). Using the other semiquantitative uptake values (18F-FDG T/NTav, 99mTc-MDP T/NTav, and 99mTc-MDP T/ NTmax), there was the tendency toward a worse prognosis with higher uptake rates, but the level of significance was reached neither with the median cutoff (Figs. 2A and 2B) nor with any other cutoff (10th percentile to 90th percentile of uptake values).
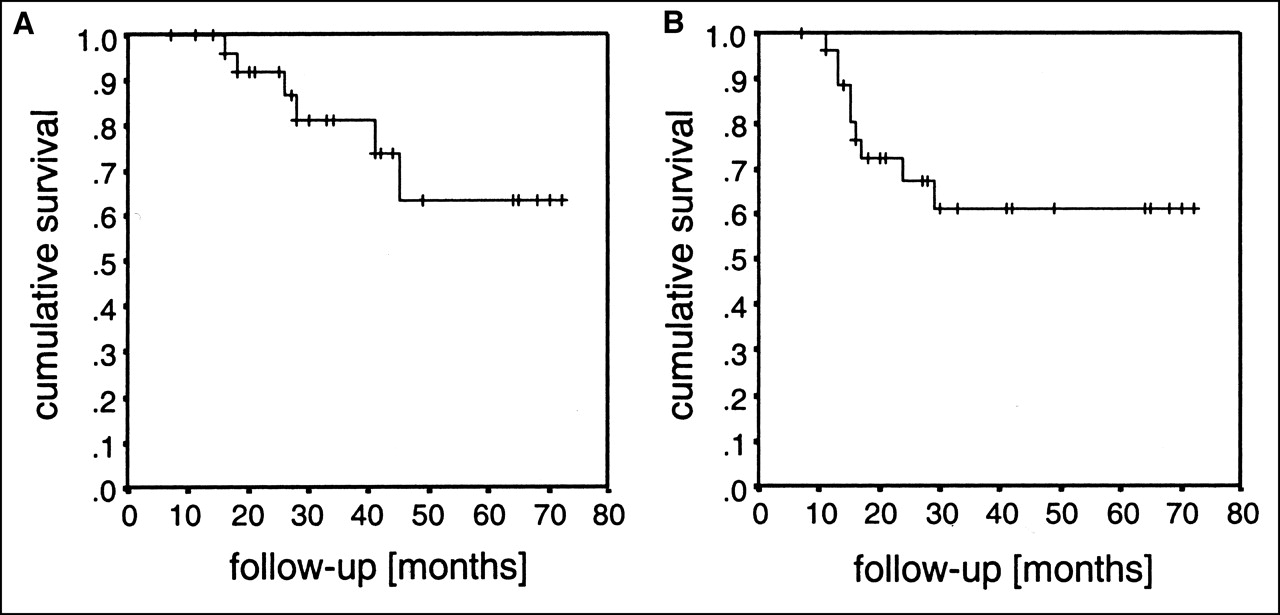
Disease outcome for whole patient group as determined by Kaplan-Meier analyses using overall survival (A) and event-free survival (B). Tick marks indicate individual follow-up period.

Disease outcome for 99mTc-MDP T/NTmax (overall survival [A] and event-free survival [B]) and 18F-FDG T/NTmax (overall survival [C] and event-free survival [D]) as determined by Kaplan-Meier analyses. Median levels were used as cutoff values. Tick marks indicate individual follow-up period.

Relationship between various 18F-FDG T/NTmax cutoff values and their discriminative value for both overall survival (A) and event-free survival (B) as assessed by log-rank test. Broad range of 18F-FDG T/NTmax ratios gave significant log-rank probability values (P < 0.05).
DISCUSSION
This study showed that initial 18F-FDG T/NTmax values clearly discriminated between osteosarcoma patients with a high probability of overall and event-free survival and osteosarcoma patients with a poor prognosis.
Previous studies have shown that pretreatment 18F-FDG PET can predict tumor behavior and prognosis for a variety of other tumor types (5–9,22). However, some of these studies are hindered by the heterogeneity of their treatment options. In a retrospective study by Ahuja et al. (6) of patients with non-small cell lung cancer, patients with stages I-IIIA underwent complete tumor resection whereas patients with stages IIIB-IV received chemotherapy or radiation. In a series of primary breast cancer patients, mastectomy was performed on some patients whereas others had breast-conserving therapy (22). The different therapeutic regimens, chosen because there were tumors in different stages, might have caused a bias in those studies. In this study, all patients received the same treatment: neoadjuvant chemotherapy followed by surgical removal of the primary tumor. Furthermore, knowledge of the 18F-FDG uptake of the primary tumor site is not likely to have influenced the choice of therapeutic management, because all 18F-FDG PET examinations were performed for the purpose of individual staging.
In recent studies, a positive correlation between 18F-FDG uptake and grading has been shown for the heterogeneous group of bone tumors. Although definite differentiation between benign and malignant bone tumors and between the different grades is not possible using 18F-FDG PET, high 18F-FDG uptake values measured either semiquantitatively (standardized uptake value or T/NT) or absolutely (metabolic rate of glucose consumption) indicate biologically aggressive lesions (1,2,23). In the current analysis, all patients had high-grade osteosarcoma. The 18F-FDG uptake values varied within a wide range, and some were even very low, as is concordant with those studies (1,2,23). 18F-FDG uptake not only reflects the biologic characteristics of bone tumors but also was found to be of prognostic significance in osteosarcoma. It is not surprising that prognostic discrimination is best when the peak values (18F-FDG T/ NTmax) within the tumor ROIs are used, because the cellular composition of sarcomas is frequently heterogeneous and the most aggressive sarcoma cells seem to determine the outcome of the patient. The prognostic impact of standardized uptake value could not be evaluated in this study because 18F-FDG PET was performed with transmission scanning for only a few patients. Because most of the primary osteosarcoma tumors were in the extremities (n = 28), with the exception of 1 pelvic primary tumor, attenuation was not expected to play a major role.
Additionally, the results of this study showed a trend toward an association between low 99mTc-MDP uptake and good prognosis. However, levels of significance were not reached. This trend fits in with the moderately positive correlation between 18F-FDG and 99mTc-MDP uptake values. The production of primitive osseous matrix is a specific capability of osteosarcoma cells. In some solid tumor types, such as differentiated thyroid cancer, the specific capabilities of the tumor cells are a sign of cellular differentiation (10,24,25) and correlate positively with prognosis (10). In contrast, in some other tumor types, high 18F-FDG uptake indicates dedifferentiation and is associated with poor outcome (10). In cases of osteosarcoma, a negative association between the production of primitive osseous matrix as measured by 99mTc-MDP bone scintigraphy and glucose metabolism as measured by 18F-FDG PET was not found. One reason might be that 99mTc-MDP uptake depicts both components: the osteoblastic activity of the osteosarcoma cells themselves and the osteoblastic reaction of normal bone tissue surrounding the osteosarcoma (3). The second component is probably more prominent in more aggressively growing tumors. Furthermore, fast tumor growth implies neoangiogenesis with increased perfusion, which may also lead to higher 99mTc-MDP uptake in biologically highly aggressive tumors (4). The same reasons seem to contribute to the similarity in 99mTc-MDP uptake in various histologic subtypes of osteosarcoma. In contrast to 99mTc-MDP bone scintigraphy, 18F-FDG PET directly assesses the cellular level of tumor metabolism, with only marginal influence from surrounding tissue.
The lack of correlation between 18F-FDG uptake and either the size or the histologic type of the primary lesion agrees with the findings of other studies—for instance, studies of patients with soft-tissue sarcoma (26)—and further underlines the fact that 18F-FDG uptake reflects an inherent biologic characteristic and does not relate to simply the morphologic parameters of the tumor. However, the lack of correlation between initial 18F-FDG uptake and grade of response is striking in the context of the significant correlation between 18F-FDG T/NTmax and outcome. The response to neoadjuvant chemotherapy has been characterized as one of the most important prognostic factors (27,28). By measuring the change in 18F-FDG uptake during neoadjuvant chemotherapy, PET seems able to discriminate between good and poor responders, as assessed histologically (3,4,29). 18F-FDG uptake was not compared with individual outcome in those studies. The clinical impact of the combination of both the initial and the follow-up 18F-FDG uptake after neoadjuvant chemotherapy has to be evaluated prospectively with respect to patient outcome. Because of the relatively small population in the current study, a meaningful multivariate analysis was not feasible. Therefore, we could not establish whether 18F-FDG contributes as an additional independent prognostic factor, as has been proven in the case of pancreatic carcinoma and lung cancer (5,6,9). This issue should be addressed in further studies with larger, multicentric patient groups.
CONCLUSION
18F-FDG uptake as measured by T/NTmax using PET is predictive of outcome in osteosarcoma. Initial 18F-FDG uptake may add information useful for therapeutic decision making. There was a moderately positive relationship between 18F-FDG uptake and 99mTc-MDP uptake.
Acknowledgments
The authors gratefully acknowledge Silke Steinhoff and Anika Brunegraf for their help with the 18F-FDG PET and bone scintigraphy quantifications; Matthias Kevric for his support with data collection; and all involved physicians, nurses, technicians, and members of the supporting services of the Department of Pediatric Hematology and Oncology and the Department of Nuclear Medicine.
Footnotes
Received Nov. 26, 2001; revision accepted Mar. 27, 2002.
For correspondence or reprints contact: Christiane Franzius, MD, Department of Nuclear Medicine, Münster University Hospital, Albert-Schweitzer-Strasse 33, 48149 Münster, Germany.
E-mail: franziu{at}uni-muenster.de
REFERENCES
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- SNMMI Procedure Standard/EANM Practice Guideline on Pediatric 18F-FDG PET/CT for Oncology 1.0
- Value of 18F-FDG PET and PET/CT for Evaluation of Pediatric Malignancies
- Relationship Between 18F-FDG Accumulation and Lactate Dehydrogenase A Expression in Lung Adenocarcinomas
- Characterization of Different Osteosarcoma Phenotypes by PET Imaging in Preclinical Animal Models
- Contribution of PET/CT to Prediction of Outcome in Children and Young Adults with Rhabdomyosarcoma
- Contemporary Imaging in Sarcoma
- Prediction Model of Chemotherapy Response in Osteosarcoma by 18F-FDG PET and MRI
- 18F-FDG PET/CT as an Indicator of Progression-Free and Overall Survival in Osteosarcoma
- Positron Emission Tomography for Staging of Pediatric Sarcoma Patients: Results of a Prospective Multicenter Trial
- Microvessel Density: Correlation with 18F-FDG Uptake and Prognostic Impact in Lung Adenocarcinomas
- Expression Profiles of Osteosarcoma That Can Predict Response to Chemotherapy
- In Vitro Proton Magnetic Resonance Spectroscopic Lactate and Choline Measurements, 18F-FDG Uptake, and Prognosis in Patients with Lung Adenocarcinoma
- Quantification of 18F-FDG Uptake in Non-Small Cell Lung Cancer: A Feasible Prognostic Marker?
- PET Imaging of Osteosarcoma
- Prognosis of Primary Osteosarcoma