


Abstract
This prospective study aimed to confirm, in a clinical setting, the benefits suggested by earlier retrospective studies of 18F-FDG PET scanning for the evaluation of patients with suspected recurrence of colorectal cancer. Methods: The referring oncologist was asked to prospectively assign a treatment plan for 102 consecutive patients being evaluated by 18F-FDG PET for suspected or confirmed recurrence of colorectal cancer and without evidence of unresectable disease on conventional staging investigations, including CT. This treatment plan was then compared with that based on incremental information supplied by PET. Management changes were validated by follow-up. Results: For 6 patients, the oncologist would not commit to a management plan without access to PET information, and for all these patients, PET correctly guided management. Of the remaining 96 patients, the management plan for 54 (56%) was altered as a direct result of unexpected PET findings. Thus, PET directly influenced management in 60 (59%) of 102 patients. The discrepant PET results could be validated in 57 patients and were correct for both the presence and the extent of malignant disease in 52 (91%) of these patients but were false-positive in 1 patient because of a pelvic abscess and underestimated the extent of metastatic disease in 4 (7%). Relapse was confirmed in 49 (98%) of 50 evaluable patients with positive PET findings. Significantly, planned surgery was abandoned in 26 (60%) of 43 patients because of incremental PET findings. Of the 42 patients for whom management was not changed by PET findings, false-negative PET findings were documented for 5 (4 with metastases < 1 cm), and the PET findings for 1 were presumed to be false-positive because of sarcoidosis. Conclusion: This prospective study confirms the high impact, suggested by previous retrospective analyses, of 18F-FDG PET on management of patients with suspected recurrent colorectal cancer. The major benefit of PET is avoidance of inappropriate local therapies by documentation of widespread disease.
Recurrence of colorectal cancer after apparently curative resection remains alarmingly common, with reported relapse rates of up to 40% (1). Because complete resection of solitary metastases or local recurrence may improve long-term survival (2,3), surgical management of such cases has become increasingly aggressive but has led to only modest survival benefit. The limitations of current approaches based on structural imaging are well documented (3–5), with over half of the patients who are thought suitable for curative surgery being found to have unresectable disease at operation. Better preoperative assessment is clearly needed.
The increasing use of 18F-FDG PET as an oncologic staging investigation (6) has significantly improved the assessment of patients with suspected colorectal cancer recurrence (7–11). Formal comparison studies (12–16) have uniformly shown its superiority over conventional staging procedures, including CT, particularly for the detection of extrahepatic disease. Several studies (14,15,17–19) have retrospectively examined the impact of PET on patient management. These show that substantial and largely appropriate changes in patient management occur, often sparing patients the significant morbidity and mortality associated with aggressive but futile therapies while also saving scarce community resources. Nevertheless, the clinical relevance of these findings has still been questioned (20).
Because of its availability and relatively low cost, CT is generally performed as the primary investigation of patients with suspected colorectal cancer relapse. Thus, the utility of PET in routine clinical practice will likely depend on its ability to provide incremental information compared with CT in selected patients rather than to serve as a replacement for CT. Accordingly, this study excluded patients with confirmed disseminated metastases on conventional staging because we believed that PET was unlikely to alter management in these patients even if additional disease sites were detected. The current study builds on the foundation of earlier studies by prospectively examining the clinical impact of 18F-FDG PET on the management of recurrent colorectal cancer in routine oncologic practice and also assessing the validity of PET-induced management changes by outcome analysis.
MATERIALS AND METHODS
Patient Population
Between February 15, 1998, and November 13, 1999, 106 consecutive patients who had been referred to our tertiary oncology center for a clinically indicated 18F-FDG PET scan to evaluate suspected or confirmed regional recurrence of colorectal cancer were prospectively entered into a database. None had confirmed disseminated metastases, and all were potential candidates for aggressive therapy if localized disease were confirmed. In cases of equivocal structural imaging results, patients were included if their referring clinician indicated that aggressive local therapy remained appropriate. The PET facility had been operational for 6 mo before the study began, and the reporting physician had significant PET experience. Patients entered into clinical trials gave written informed consent, and the protocol was approved by the institutional ethics committee.
On the routine clinical request form, the referring specialist oncologists were required to state the indication for the PET scan, the histology of the tumor, the clinical stage, and the results of the most recent structural imaging tests. The referring physicians were also required to state what their proposed management plan would be in view of all available clinical information and investigations up to the time of referral. These investigations routinely included CT and any other imaging or biochemical studies that had previously been undertaken to address specific clinical issues. The treatment options available were not restricted to any single modality so that physicians were able to choose combinations of therapy that they thought appropriate to their individual patient.
Four patients, for whom the physicians had not prospectively entered their management plan before dispatch of the PET result, were excluded. The remaining 102 patients (65 men, 37 women; age range, 28–88 y; mean age, 62 ± 12 y) formed the study population. Prospective management plans were supplied for 96, whereas for 6 the referring clinician refused to commit to a treatment plan without access to the PET information. The original tumor locations were the rectum in 36%, the rectosigmoid colon in 22%, the sigmoid colon in 6%, the descending colon in 4%, the transverse colon in 9%, the ascending colon in 9%, the cecum in 12%, and unspecified in 2%. These patients were studied between 6 wk and 12 y after their initial, potentially curative treatment of colorectal cancer. The median time from treatment to the PET study was 2 y.
Review of Conventional Staging Investigations
Most but not all patients had undergone helical CT with both oral and intravenous contrast media unless contraindicated. Whenever possible, the results of imaging not performed by our institution were evaluated by specialist radiologists at our site for the technical adequacy of the scan and the accuracy of the report. Any imaging studies deemed to be of suboptimal quality were repeated before the PET scan, and the results were provided to the referring clinician. CT was performed within 2 mo of PET in 91 (89%) of 102 patients, and all imaging was performed within 5 mo. The median time between CT and PET was 25 d. In some cases, sonography or MRI had been performed, and its results were used in determining the disease status by conventional evaluation. The results of imaging studies were presented at a weekly multidisciplinary colorectal unit meeting attended by specialist oncologic radiologists, medical and radiation oncologists, and surgeons in determining the management options for patients of this institution and were generally discussed before a PET scan was ordered.
Classification of Referral Indication and Management Plan
From the clinical request provided, the patients’ referral indications were subdivided into the following diagnostic subgroups: limited (solitary or adjacent) metastases amenable to aggressive local therapy (usually surgical resection but including regional chemotherapy, cryoablation, or local radiotherapy), rising carcinoembryonic antigen (CEA) levels with either normal or equivocal structural imaging findings, increasing local symptoms without definite structural abnormalities, known recurrence but extent characterization needed for treatment planning, and new mass or residual mass suggestive of recurrence but unconfirmed by biopsy.
For purposes of analysis, patient management definitions were defined as follows. Active treatment was when any combination of surgery, radiotherapy, or chemotherapy was delivered to patients considered to have recurrence. Supportive treatment was when recurrence was considered proven but no active treatment was given. Observation was when no objective evidence of disease was present and routine surveillance was planned. Treatment planning was when the referring clinicians refused to commit to a treatment plan without access to the PET information.
PET Scan Procedure
All patients were asked to fast for 6 h before the study (21) but were encouraged to drink water. To reduce the confounding effects of changing bladder activity on assessment of the pelvis and to reduce out-of-field scatter in 3-dimensional scanning mode, patients were catheterized when possible and given 10–20 mg furosemide 30 min before imaging. In the later part of the study, patients also received bowel preparation on the day before scanning (22). This was not, however, used in patients with prior colostomy. Imaging was performed using a GE QUEST 300H scanner (UGM Medical Systems, Inc., Philadelphia, PA) at least 1 h after intravenous injection of 18F-FDG. This scanner is a dedicated 3-dimensional PET scanner that uses NaI detectors (23). Consistent with the restricted count-rate capacity of the NaI detectors on this scanner, patients were administered 70–120 MBq to achieve an estimated singles count rate of <3 million counts per second. Whenever possible, transmission and emission scans were obtained from the neck to the upper femurs to include the lower neck, lung, liver, and adrenal glands in the field of view. Total imaging time was approximately 45 min, and patients were scanned with their arms raised unless unable to tolerate this position. Some patients with claustrophobia were scanned only to the mid thoracic level.
Image datasets were obtained using iterative reconstruction (ordered-subset expectation maximization method) (24). Attenuation correction was performed using previously described methods (25). Datasets with and without measured attenuation correction were reported from the screen using an interactive display program that allows multiple orthogonal images to be displayed simultaneously. Rotating count-rendered images were also reviewed, particularly to clarify the relationship between suspected abnormalities and physiologic radiotracer accumulation in the colon.
PET Scan Interpretation
The PET stage was determined by incorporating the PET findings with all other staging information and was abstracted from the clinical report issued thereafter. In almost all cases, the previous CT findings were directly correlated with the PET findings, but in occasional cases, the images were not available and the CT report was relied on. As a general rule, 18F-FDG PET abnormalities less intense than physiologic uptake in the liver were not considered to be positive unless there was a small corresponding structural imaging abnormality. This is consistent with the concept of compensation for partial-volume limitations of the PET scanner (26). Significant structural imaging abnormalities did not influence the PET result if there was no associated 18F-FDG PET abnormality.
Evaluation of Impact of PET Scan and Outcome
All referring physicians were contacted within 1 mo of the scan. Each physician provided information on how patients were managed after their PET scans and when surgical interventions such as laparotomy were performed, operative findings were obtained, and pathology reports were obtained. At least 6 mo and approximately 12 mo after the PET scan report was issued, information on clinical outcome and subsequent imaging or pathologic findings was obtained from the referring clinicians or medical records.
The PET study was classified as true-positive if recurrent disease was confirmed at surgery or on subsequent follow-up, usually including confirmation by structural imaging. The criterion for imaging confirmation was increasing or new abnormalities in the region of PET-defined abnormalities compatible with tumor and sufficient to justify a management change. This criterion did not require biopsy confirmation of every site of PET abnormality. True-positive PET scans were considered to have underestimated the extent of disease if additional sites of involvement were found at subsequent surgery or were confirmed on imaging within l y of the PET scan. A false-positive PET scan was defined as either misclassification of a subsequently proven benign abnormality as malignant or PET abnormalities that showed no progression after at least 2 y of follow-up. PET was considered true-negative if the patient was free of disease progression at least 1 y after the scan. PET was considered false-negative if no abnormality was seen on PET but malignancy was subsequently found at surgery or if progressive abnormalities developed on structural imaging within 1 y of follow-up in patients with durable disease control locally or at the site of subsequent surgery.
Statistics
When appropriate, 95% confidence intervals (CI) calculated using StatXact software (version 4.0.1; CYTEL Software Corp., Cambridge, MA) are reported.
RESULTS
Overall Clinical Impact of 18F-FDG PET on Management
The impact of PET is shown in Table 1. In the 6 patients for whom the referring clinician was not prepared to commit to a treatment plan without access to the PET information, PET correctly guided management in all patients, with 2 confirmed true-negative studies and 4 validated true-positive results. Of the remaining 96 patients with prospectively defined treatment plans, incremental information provided by 18F-FDG PET directly changed the management of 54 (56%). Thus, overall, PET directly influenced management decisions in 60 (59%) of 102 patients.
Management Changes Influenced by PET by Clinical Indication
There were 2 patients with positive PET findings that altered management but who died within 3 mo of the PET study without definite confirmation of the incremental findings and 1 other patient who was lost to follow-up. Of the remaining 57 patients, the correct disease status, and therefore appropriate information to guide management change, was validated by clinical follow-up in 52 (91%). These included 7 with true-negative and 45 with true-positive PET results. One patient had a false-positive result relating to a pelvic abscess but was appropriately managed by surgery, whereas in the other 4 patients (7%), the PET result was true-positive but underestimated the extent of disease subsequently confirmed. These included 3 patients with additional small peritoneal metastases (all <1 cm) found at laparotomy and 1 patient with early relapse of extrahepatic disease after resection of a hepatic metastasis. Thus, 49 (98%) of 50 evaluable patients with positive PET findings had confirmation of relapse.
Evaluation of Clinical Indication Subgroups
The patient referral indications and associated changes in management induced by incremental PET findings are presented in Table 1. The largest group consisted of 34 patients with apparently limited metastases thought to be amenable to aggressive local therapy. Substantial changes in management were observed for every diagnostic subgroup.
The most frequent change in management was to vary the active treatment planned. In 26 patients, the PET results directly influenced the changes made, representing 25% (95% CI, 17%–34%) of the entire patient population. Similarly, PET influenced a change from observation to active therapy in 12 patients (12%; 95% CI, 5%–19%) and from active to supportive palliative therapy after showing more extensive disease than previously suspected in 11 patients (11%; 95% CI, 4%–17%). In 5 patients for whom active treatment was changed to observation only, abnormal findings on conventional imaging were thought to be most likely caused by a recurrence, but subsequent PET findings were normal. In 6 further patients, the clinician refused to commit to a treatment plan before availability of the PET result, and PET was therefore deemed to have changed management.
A high impact was found on the delivery of aggressive local therapies, including surgery and local radiotherapy (Table 2). These therapies were correctly prevented by incremental PET findings in 31 patients but initiated in 18 patients. Overall, for 26 (60%) of 43 patients for whom surgical intervention had prospectively been planned, this was abandoned as a direct result of the PET findings. The high impact of PET was particularly evident in the group of patients with apparently limited metastases for whom surgical resection was planned. In this group, only 10 came to operation, including 2 for whom the PET findings of inoperability were confirmed. One patient was recognized at the time of reporting to have false-negative PET findings in relationship to a small (<1 cm) but biopsy-proven hepatic metastasis. This patient underwent limited hepatic resection because there was no evidence of extrahepatic disease on PET, and there was no evidence of progressive extrahepatic disease during more than 12 mo of follow-up. Seven other patients were judged to have potentially operable disease on the basis of concordant CT and PET findings. In 1 of these patients, both CT and PET underestimated the extent of disease found at surgery and curative resection was not attempted, whereas 6 underwent curative surgery and the surgical findings were consistent with the imaging results. Of these, 3 remained free of disease at >1 y, 1 had late recurrence (19 mo), and 2 had early recurrences (6 and 9 mo). All patients with relapsing disease presumably had microscopic disease undetected by CT, 18F-FDG PET, or diagnostic laparotomy. Of the 19 patients with apparently solitary liver metastases on CT, PET found additional hepatic metastases in 2, extrahepatic disease in 8, and more extensive intrahepatic spread and extrahepatic disease in 3.
Summary of Impact of PET on Aggressive Local Therapies by Clinical Indication
In 13 (65%) of 20 patients with a rising CEA level, true-positive incremental PET findings suggested a recurrence site and altered management. In 4 further patients, the PET findings were abnormal but did not alter management: In 1 of these patients, who was described earlier, the findings were misinterpreted through lack of direct correlation with structural imaging; in 3, true-positive PET findings did not induce a management change. Despite the high sensitivity of PET in this patient subgroup, PET underestimated the extent of disease in 4 of these 16 true-positive cases: 2 patients with additional peritoneal metastases (<1 cm) documented at surgery and 2 patients with relapse at additional sites after 4 and 9 mo of further observation. On clinical follow-up, 2 of the 3 PET-negative patients in this subgroup are free from disease at >1.5 y, both with falling CEA levels, but 1 was found to have small-volume peritoneal disease at laparoscopy. In all but 1 patient for whom PET altered management and follow-up was available, the PET result was correct for the relapse status (Table 3), but in several patients detailed above, all imaging techniques underestimated the extent of disease.
Validation of PET Results in 60 Patients for Whom PET Altered Management
Outcomes in Which 18F-FDG PET Findings Were Inconsistent with Final Management
Of the entire study group, the final management for 18 patients was not consistent with the disease status reported on PET, including 6 patients for whom management was changed from the prospectively assigned treatment plan. The details of these patients are shown in Table 4. In summary, PET was clearly correct for both the presence and the extent of relapse in 9 patients but was inappropriately ignored. In 2 patients, PET correctly identified relapse but underestimated the extent of disease. Nevertheless, inappropriate hepatic resection was avoided in both patients by subsequent evaluation. In another patient, an interpretative false-negative study was recognized by direct correlation of the CT and PET images, emphasizing the limitations of relying on clinical CT reports alone when reporting PET results. In 4 patients, the PET findings were false-negative, but in 2 of these patients the false negativity was prospectively recognized on the basis of knowledge of the presence of a biopsy-confirmed, <l-cm hepatic metastasis on CT. For these 2 patients, correct exclusion of extrahepatic disease allowed surgery to proceed. The other 2 patients had small peritoneal deposits that were missed by PET and CT but were directly visualized by invasive procedures. One patient who was thought to have relapse on PET refused further investigation and has been lost to follow-up, whereas the remaining patient was reported to have probable granulomatous disease as the cause of additional 18F-FDG PET abnormalities in the mediastinum. These findings were not further evaluated by the treating clinician and therefore did not adversely affect management. On the basis of these findings, the incorporation of PET into clinical decision making leads to appropriate management in most patients. Figures 1 and 2 are 2 representative examples of this.
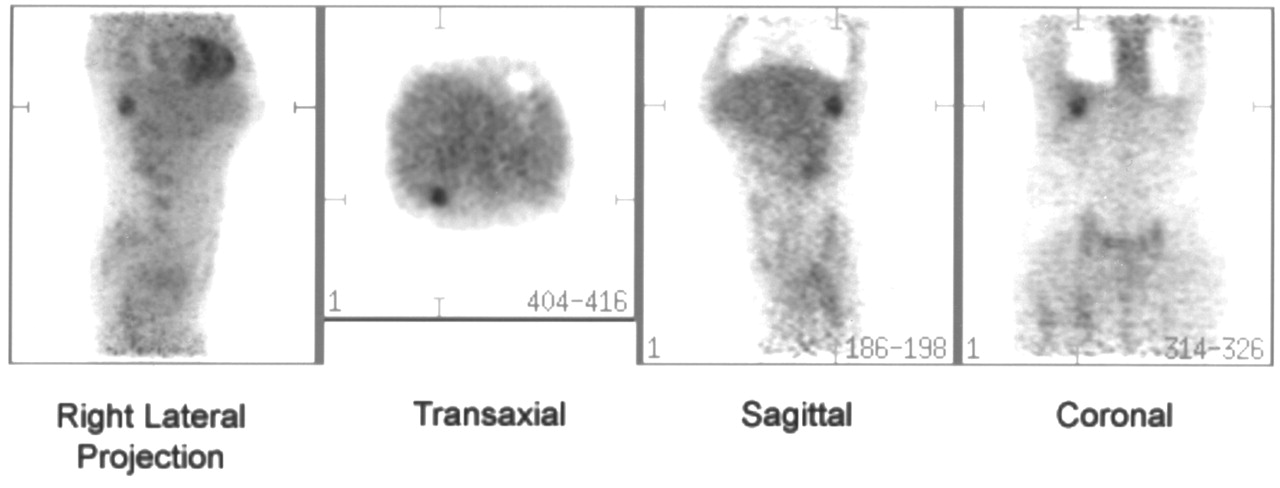
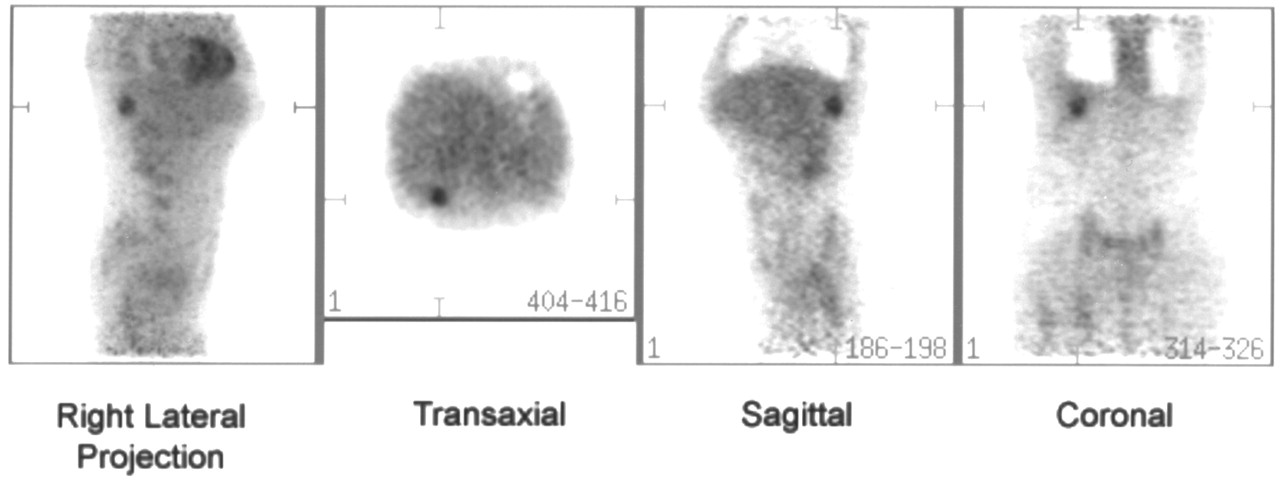
Both CT and 18F-FDG PET suggested presence of single hepatic metastasis. At laparotomy, additional small (<1 cm) metastases were found and hepatic resection was abandoned.
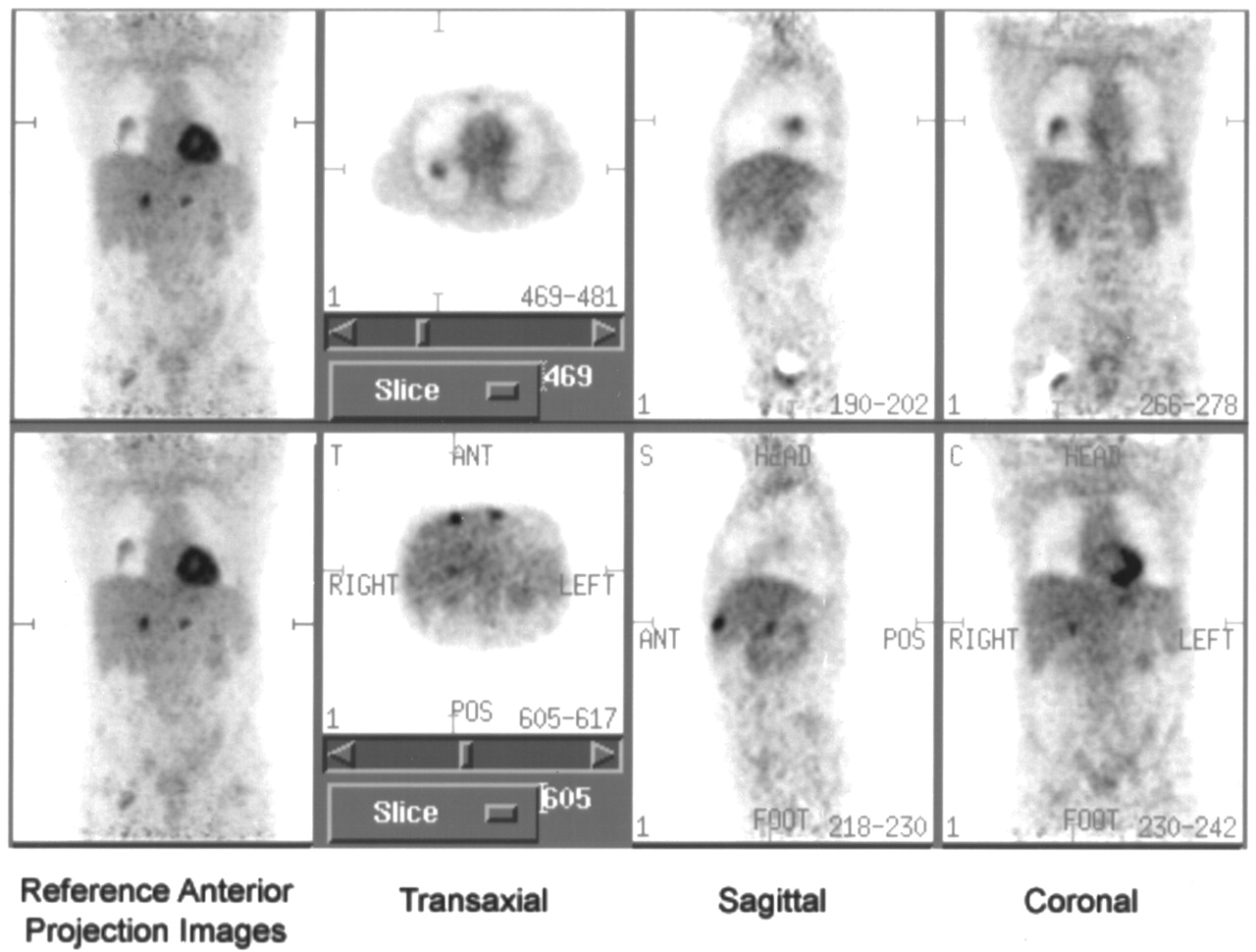
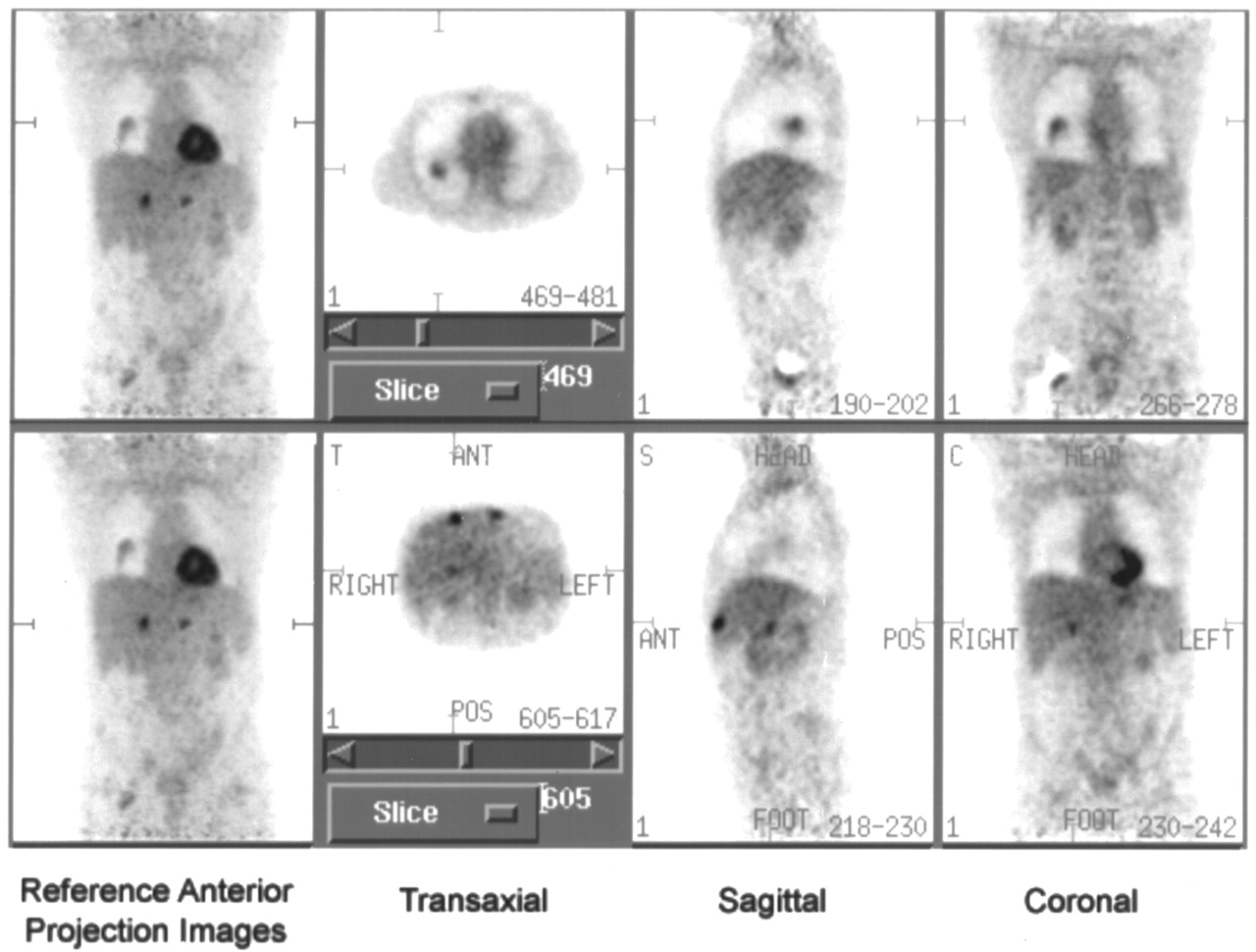
This patient was being considered for resection of an apparently isolated lung metastasis. In addition to lung lesion shown in upper panel, PET found additional multiple liver metastases not apparent on CT, as shown in lower panel. Surgery was avoided, and abdominal metastases were subsequently confirmed by serial imaging.
Outcomes in Patients for Whom Discrepant PET Findings Were Inconsistent with Final Management
Effect of CT Timing Relative to PET
Although nearly all patients underwent CT shortly before PET, 5 patients experienced a delay of >3 mo. It is thus possible that these 5 patients may have skewed the overall findings of this study in favor of PET because of the natural progression of the disease rather than increased sensitivity of PET. This subgroup included 3 patients with ongoing symptoms suspected to be caused by recurrence and previously unhelpful structural imaging and for whom the referring clinician elected to use PET as the sole restaging technique. Two had their most recent CT performed 103 and 134 d before a negative PET scan. Both continued with observation without evidence of recurrent disease. A further patient with negative findings on CT performed 154 d before PET was found to have widespread metastatic disease, and adjuvant chemotherapy was therefore stopped. Two patients with apparently isolated metastasis on CT performed 111 and 99 d before PET were found to have disseminated disease. The management of the first was changed from surgery to chemotherapy, and the management of the second was changed from intraarterial chemotherapy to palliative care. Thus, progressive disease between the CT and PET scans could have accounted for the discrepant results in 3 patients, all of whom had their management changed.
DISCUSSION
This prospective study confirms the usefulness of PET in the evaluation of a clinically selected spectrum of patients with a history of treated colorectal cancer, which was suspected or confirmed to have recurred. The substantial impact on management (59%) is likely to reflect, in part, the high pretest likelihood of recurrent cancer in this patient population but nevertheless indicates that PET is substantially more sensitive than conventional imaging in this clinically relevant patient population. Although PET appears to have accurately characterized both the presence and the extent of relapse in most evaluable patients, underestimation of disease extent is not uncommon and negative results need ongoing surveillance as a minimum. Most false-negative sites were related to lesions < 1 cm that were documented by invasive procedures or subsequent relapse at additional sites many months after the PET scan, also suggesting that these lesions were small at the time of imaging. Limited detection of low-bulk disease is a recognized limitation (16) of PET but is also a failing of all imaging approaches.
The frequency of change of patient management attributable to PET in this study was high (59%; 95% CI, 49%–69%), with only 3 of 60 cases potentially influenced by a delay between CT and PET. The incidence of management alterations in this study was similar to that in a recent study (16) but was somewhat higher than found in a recent metaanalysis (6), in which changes occurred in 20%–45% of cases. Some discrepancy may reflect the prospective design of this study, which enabled better evaluation of changes in therapeutic delivery than is possible in retrospective studies (6). These changes in therapeutic delivery accounted for 47% (28/60 patients) of the changes that were attributable to PET findings and would be difficult to fully document in retrospective studies.
For a high percentage (60%; 95% CI, 45%–76%) of patients (26/43), surgery was cancelled because of the PET findings, with most of these patients included with the group being considered for resection of limited disease. This cancellation rate was again greater than the 20%–43% rate found by the metaanalysis study (13,14,18,27,28) but was similar to that of a large, more recent series of 100 patient studies (29), in which PET affected the surgical management of 61% of patients. Our findings also cannot be explained by the delay between CT and PET, because delays of >50 d occurred in only 2 of these 26 patients. We are encouraged that most of the management changes induced by PET appeared to be appropriate to the clinical outcomes. Clearly, differences in local surgical practices and philosophies are likely to influence both the selection of patients for PET scans and the rate at which PET findings affect the treatment delivered, and our results will therefore need to be confirmed by further prospective studies.
In contrast, the overall frequency of conversion of patients from active treatment to supportive therapy after demonstration of occult disseminated disease by PET in this study (11%) and from active treatment to observation because of negative PET findings (5%) is similar to that in other large series (14,19). This was also seen in the ability of PET to detect occult relapse in 65% of patients with rising CEA levels but no obvious site of tumor recurrence—a finding that is consistent with published data (14,30). Finally, the frequency of underestimation of tumor extent at surgery or on follow-up—7% of patients for whom PET altered management—was again similar to that found by other studies (14).
The study was designed to replicate as closely as possible the likely niche of PET in a clinical setting as an investigation performed after structural imaging. Thus, patients with disseminated disease that had already been identified definitively on structural imaging were not included, thereby biasing any direct comparison between PET and CT. For similar reasons, CT at the time of PET was not an absolute requirement for study eligibility. Accordingly, the interval between CT and PET (median, 25 d) may in part explain some of the differences in accuracy. Our study assessed the incremental rather than the independent diagnostic information provided by PET, and we therefore believe it appropriate that best clinical practice was followed with PET and routinely reviewed with CT (26) and all of the clinical findings. It is possible that a comparison with spiral CT performed and interpreted exclusively in facilities with special expertise in this field could lessen the impact of PET (20), but in the context of this study, such a comparison would probably do so mainly by reducing the overall number of patients coming for a PET scan rather than by reducing the frequency of change induced by PET scan findings.
Many of our patients did not undergo extensive invasive procedures to definitively confirm or deny the presence of all apparent disease found by PET. Although such confirmation is desirable (6), it is often clinically impractical or impossible (14,20). Nevertheless, with the use of clinical and multimodality imaging evidence, confirmation or denial of the presence of discordant PET-defined disease was usually quite a straightforward process and was sufficient to justify the appropriateness of the change in management. However, problems arise in patients with negative scan findings who appear free of disease at >1 y, because they may still harbor small-volume disease.
The limitations of PET in abdominal imaging have been well described (19). Respiratory movement and normal physiologic uptake of 18F-FDG into the liver and the colon (19) reduce the contrast resolution of PET; thus, liver lesions < 1 cm often are not detected (18). This has lead to controversy about whether PET is equivalent (18,27) or superior (14,28) to CT, including spiral CT (17), in assessing the liver. This study had examples to support both assertions: PET studies had false-negative findings for which CT-defined lesions were <1 cm, but PET also showed liver metastases not seen on CT, further supporting the use of CT and PET as complementary rather than competing modalities. Improvement in PET instrumentation, including devices with higher spatial and contrast resolution, will likely further increase the clinical value of this technology, as will the ability to accurately coregister 18F-FDG PET and CT data through hybrid scanner technology (31).
The difficulty 18F-FDG PET has in distinguishing between abscesses and tumor recurrence is also well documented (19). In our patient population, this problem affected only 1 patient, and although the finding was false-positive for the purposes of this study, the condition still required aggressive treatment in its own right. Granulomatous disease poses an interpretive problem in the thorax but is relatively uncommon in the abdomen. There was 1 case of apparently false-positive mediastinal abnormalities on PET, but this case was reported as likely to reflect sarcoidosis, and management was not affected.
CONCLUSION
This prospective study confirmed the importance of 18F-FDG PET in the management of patients with colorectal cancer recurrence. Positive PET findings reliably enable patients to be directed to nonsurgical therapy if a disseminated disease pattern is obtained. However, this study also places a caveat on the limitations of this technique: When there is a solitary PET 18F-FDG–positive lesion thought suitable for surgery, or there are structural lesions < 1 cm that are PET negative, the rate of underestimation of disease extent is not negligible and further work-up would be recommended.
Acknowledgments
The authors thank Anne Thompson, PhD, the referring clinicians and their secretarial staffs, and the staff of the Medical Records Department of the Peter MacCallum Cancer Institute for help in providing and obtaining follow-up information; Robert Thomas, MD, for thoughtful comments during manuscript preparation and help with clinical follow-up; and the radiochemistry staff and technologists of the PET center of the Peter MacCallum Cancer Institute for technical contributions. This study was supported by a grant from the Consultative Committee on Diagnostic Imaging, under the auspices of the Australian Government Department of Health and Aged Care. Sabbatical leave was supported by the Whole-Time Medical Specialist Private Practice funds of the Alfred Hospital, Prahran, Victoria, Australia.
Footnotes
Received Apr. 6, 2001; revision accepted Dec. 19, 2001.
For correspondence or reprints contact: Rodney J. Hicks, MD, Centre for PET, Peter MacCallum Cancer Institute, 12 Cathedral Pl., East Melbourne, Victoria 3002, Australia.
E-mail: rhicks{at}petermac.unimelb.edu.au
REFERENCES
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- The Injustice of Being Judged by the Errors of Others: The Tragic Tale of the Battle for PET Reimbursement
- Effect of PET/CT on Management of Patients with Non-Small Cell Lung Cancer: Results of a Prospective Study with 5-Year Survival Data
- Doing More Harm than Good? Do Systematic Reviews of PET by Health Technology Assessment Agencies Provide an Appraisal of the Evidence That Is Closer to the Truth than the Primary Data Supporting Its Use?
- Are Health Economics Making Us Sick?
- PET Changes Management and Improves Prognostic Stratification in Patients with Recurrent Colorectal Cancer: Results of a Multicenter Prospective Study
- Impact of Positron Emission Tomography/Computed Tomography and Positron Emission Tomography (PET) Alone on Expected Management of Patients With Cancer: Initial Results From the National Oncologic PET Registry
- Impact of [18F]-fluorodeoxyglucose ([18F]-FDG) imaging in sarcoidosis: unsuspected neurosarcoidosis discovered by [18F]-FDG PET and early metabolic response to corticosteroid therapy
- Early Detection of Cancer Recurrence: 18F-FDG PET/CT Can Make a Difference in Diagnosis and Patient Care
- "Flying Through" and "Flying Around" a PET/CT Scan: Pilot Study and Development of 3D Integrated 18F-FDG PET/CT for Virtual Bronchoscopy and Colonoscopy
- Findings on 18F-FDG PET Scans After Neoadjuvant Chemoradiation Provides Prognostic Stratification in Patients with Locally Advanced Rectal Carcinoma Subsequently Treated by Radical Surgery
- Whole body positron emission tomography/computed tomography (PET/CT) tumour staging with integrated PET/CT colonography: technical feasibility and first experiences in patients with colorectal cancer
- 18F-FDG PET for Evaluation of Bone Marrow Infiltration in Staging of Lymphoma: A Meta-Analysis
- Benign Lesions in Cancer Patients: CASE 1. Sarcoidosis After Chemoradiation for Head and Neck Cancer
- Is 18F-FDG PET/CT Useful for Imaging and Management of Patients with Suspected Occult Recurrence of Cancer?
- 18F-FDG PET in Evaluating Patients Treated for Metastatic Colorectal Cancer: Can We Predict Prognosis?
- Comparison of 2-Dimensional and 3-Dimensional 82Rb Myocardial Perfusion PET Imaging
- Imaging of Gynecologic Tumors: Comparison of 11C-Choline PET with 18F-FDG PET
- 18F-Fluoro-2-deoxyglucose positron emission tomography in the evaluation of gastrointestinal malignancies
- Utility of PET Scanning for Evaluation of Recurrent Colorectal Cancer