


Abstract
The current major limitation to development of electrocardiographically (ECG) gated blood-pool SPECT (GBPS) for measurement of the left ventricular (LV) ejection fraction (LVEF) and volumes is the lack of availability of clinically validated automatic processing software. Recently, 2 processing software methods for quantification of the LV function have been described. Their LVEFs have been validated separately, but no validation of the LV volume measurement has been reported. Methods: We compared 3 processing methods for evaluation of the LVEF (n = 29) and volumes (n = 58) in 29 patients: automatic geometric method (GBPSG), semiautomatic activity method (GBPSM), and 35% maximal activity manual method (GBPS35%). The LVEF provided by the ECG gated equilibrium planar left anterior oblique view (planarLAO) and the LV volumes provided by LV digital angiography (Rx) were used as gold standards. Results: Whereas the GBPSG and GBPSM methods present similar low percentage variabilities, the GBPS35% method provided the lowest percentage variabilities for the LVEF and volume measurements (P < 0.04 and P < 0.02, respectively). The LVEF and volume provided by the 3 methods were highly correlated with the gold standard methods (r > 0.98 and r > 0.83, respectively). The LVEFs provided by the GBPS35% and GBPSM methods are similar and higher than those of the GBPSG method and planarLAO method, respectively (P < 0.0001). For the LVEF, there is no correlation between the average and paired absolute difference for the 3 GBPS methods against the planarLAO method, and the limits of agreement are relatively large. LV volumes are lower when calculated with the GBPSM, GBPSG, and Rx methods (P < 0.0001). However, the GBPS35% and Rx methods provide LV volumes that are similar. There is no linear correlation between the average and the paired absolute difference of volumes calculated with the GBPSG and GBPS35% methods against Rx LV volumes. However, a moderate linear correlation was found with the GBPSM method (r = 0.6; P = 0.0001). The 95% limits of agreement between the Rx LV volumes and the 3 GBPS methods are relatively large. Conclusion: GBPS is a simple, highly reproducible, and accurate technique for the LVEF and volume measurement. The reported findings should be considered when comparing results of different methods (GBPS vs. planarLAO LVEF; GBPS vs. Rx volume) and results of different GBPS processing methods.
- left ventricular ejection fraction
- cardiac radionuclide angiography
- gated SPECT
- left ventricular volume
- left ventricular function
Electrocardiographically (ECG) gated planar radionuclide angiography is the gold standard for left ventricular (LV) ejection fraction (LVEF) assessment in the clinical setting. This method has withstood the test of time not only because of its simplicity and excellent reproducibility but also because it provides much quantitative or semiquantitative information needed for clinical management of patients’ LV and right ventricular function.
However, besides LVEF evaluation, measurement of LV volumes has important clinical implications for the diagnosis, management, and prognosis of patients with cardiac disease (1–4). Planar radionuclide angiography can provide information about the LV volume but this is done at the expense of the simplicity of the planar technique, therefore limiting its use for LV volume measurement. The use of ECG gated blood-pool SPECT (GBPS) can provide simultaneously accurate LV and right ventricular ejection fraction (EF) and volumes with a simple technique. However, since its first description by Strauss et al. (5) in 1971 and many subsequent clinical validation studies, the GBPS acquisition technique has not met the success it was expected to have (5–8), mainly because of the long processing time it requires for the operator to isolate the left ventricle using manually or semiautomatically drawn regions of interest (ROIs) over a large number of reconstructed slices. Currently, the major limitation to its current development is the commercial availability of automatic processing software and the wide clinical validation. Recently, 2 processing software programs for the segmentation of the left ventricle have been developed and validated clinically: completely automatic processing software developed by the group of Germano as described in Kriekinge et al. (9) (geometric method [GBPSG]) and semiautomatic processing software developed by Mariano-Goulart et al. (10) (activity method [GBPSM]). In our department, we use time-consuming software (with manual segmentation of the left ventricle) for the processing of GBPS based on the maximal activity threshold volume method as described (11–14).
The aim of this study was to evaluate the accuracy of the LVEF and LV volume calculated with the above 3 GBPS processing methods, in comparison with the planar radionuclide angiography LVEF and radiologic angiography LV volumes taken as the gold standards.
MATERIALS AND METHODS
The study population included 29 male patients (mean age, 58 ± 14 y) referred for equilibrium radionuclide angiography having LV radiologic angiography within a 1-wk period without any intervening cardiac event or modification in therapy between the 2 studies (1 ± 3 d). Twenty-three patients (79%) had a previously known myocardial infarction (13 patients with an anterior myocardial infarction). Twenty-five patients had coronary artery disease (8 patients with 3-vessel, 4 patients with 2-vessel, and 13 patients with 1-vessel disease), 1 patient had cardiomyopathy associated with mitral regurgitation, and 3 patients had idiopathic dilated cardiomyopathy. Exclusion criteria included patients with frequent arrhythmias, acute cardiac event, or hemodynamic instability.
LV end-diastolic volume (EDV) and end-systolic volume (ESV) were calculated by a single observer with contrast radiologic LV digital cardioangiography (Rx) using the single-plane area–length Sandler–Dodge method in the 30° right anterior oblique (RAO) projection, as validated (15). After normalization for magnification, the following RAO ventriculogram correction factor was applied: V = 0.693 × V′ + 8.65, where V is the corrected volume and V′ is the measured LV volume as calculated with the RAO single-plane Sandler–Dodge method. End-diastolic and end-systolic projections were obtained by selecting the largest and smallest contours, respectively. Ventriculograms were traced manually by a single observer, who took care to avoid postectopic beats.
Acquisition
After in vivo labeling of red blood cells with 1.110 MBq (30 mCi) 99mTc, planar equilibrium ECG gated radionuclide angiography in the left anterior oblique view (planarLAO) followed immediately by GBPS radionuclide angiography were performed. All acquisitions were done on a dual-head DST-XL gamma camera (SMVi, Buc, France) using a low-energy, high-resolution collimator.
PlanarLAO Acquisition.
Conventional ECG gated planar equilibrium radionuclide angiography studies were realized in the best septal LAO projection with a caudal tilt for 400 kilocounts per frame, 16 frames per cardiac cycle, 64 × 64 matrix, a ±10% R–R acceptance window, image magnification of 2.67, and an energy window of 20% centered on 140 keV. The size of 1 pixel after magnification was 3.38 mm.
GBPS Acquisition.
For GBPS studies, acquisition parameters consisted of 32 steps per 180°, 90 s per step, 16 frames per cardiac cycle, 64 × 64 matrix, body contour, an energy window of 15% centered on 140 keV, a ±10% R–R acceptance window, and image magnification of 1.3. At acquisition, the size of 1 pixel after magnification was 6.77 mm. The full width at half maximum was 14.6 mm.
Processing
Planar Processing.
The data were processed on a dedicated computer (NXT; SMVi), and the LVEF was obtained with a previously validated algorithm included in the standard software package. End-diastolic and end-systolic ROIs were computed automatically but could be partially or totally redrawn manually with the help of phase, amplitude, and Laplacian functional images (16).
GBPS Processing.
GBPS studies were reconstructed by ramp-filtered backprojection after prefiltering the projection data with a 2-dimensional Butterworth filter (order, 5; cutoff, 0.25 pixel−1; pixel size, 6.7 mm). Four-cavity horizontal and short-axis datasets were generated by manual reorientation.
GBPS was processed using 3 methods:
GBPS automatic software (β version) developed by the group of Germano (9) (GBPSG). This method is based on activity and temporal gradients (geometric method). The algorithm determines an ellipsoid coordinate system for the left ventricle and then computes a statistic estimate of the endocardial surface by use of counts and count gradients. A dynamic surface representing the endocardium is computed for each interval of the cardiac cycle by use of additional information from the temporal Fourier transform of the image datasets. The algorithm then calculates the LV volume for each interval. It provides estimates of the LV EDV and ESV as calculated from the number of LV voxels. Then, the LVEF is derived from the calculated LV volumes as follows: LVEF = ([LV EDV − LV ESV] × 100/LV EDV).
GBPS semiautomatic software (β version) developed by the group of Mariano-Goulart et al. (10) (GBPSM). It consists of a semiautomatic segmentation of ventricular activities based on the watershed algorithm. This watershed segmentation method determines the borderlines dividing adjacent catchment basins—that is, the whole set of points of a surface whose steepest slope paths reach a given minimum (i.e., LV cavity). Over- and undersegmentation of the LV cavity can result, but the software provides the operator with the possibility of correcting manually the automatic software proposed segmentation. It allows estimation of the LV EDV and ESV based on the normalization of the LV activities calculated within the defined LV borders (at end diastole and end systole) to the maximal pixel activity in the reconstructed cardiac slices (activity method). This provides the number of voxels constituting the LV cavity that is then normalized to volume measurement. The LVEF was calculated as ([LV ED activity − LV ES activity] × 100/LV ED activity) without background correction.
GBPS manual software used routinely in our department, which is based on the maximal activity threshold LV volume method as described (11–13). In this method, the operator isolates the left ventricle from all other cardiac, vascular, and background structures by manually drawing an irregular ROI. This is done on each slice of the 4-cavity horizontal end-diastolic and end-systolic reconstructed projections. Then, a 35% maximal activity threshold was used to provide estimates of the number of voxels included in the LV cavity as validated by our group on phantom studies (14). The calculated LV number of voxels is then normalized to the LV volume measurement. The LVEF is then calculated as ([LV EDV − LV ESV] × 100/LV EDV).
Statistical Analysis
Statistical calculation was performed using Prophet 5.0 (BBN Systems and Technologies). Data are expressed as mean ± SD. The LV EDV and ESV measurements provided by each GBPS method were combined. The LVEF and volumes calculated with the 3 GBPS methods, planarLAO method (LVEF; n = 29), and Rx (LV volumes; n = 58) were compared using Friedman’s test. Comparison of the mean of the paired absolute difference between 2 methods to the zero value was done with the 1-sample t test.
The linear regression analysis and paired absolute differences between GBPS values and the reference methods (planarLAO for LVEF and Rx for LV volumes) were studied, and Bland–Altman analysis was also performed. In case of linear correlation between the difference of 2 methods and their average, a logarithmic transformation was used for calculation of the limits of agreement. Otherwise, these values were considered to be the mean ± SD of the difference.
The accuracy of each method (random error [RE]) was compared after adjustment for systematic error by applying a correction factor based on its linear regression with planarLAO LVEF reference values and Rx LV EDV and LV ESV reference values, used as the gold standards. The variances of the calculated RE were compared using Levene’s test.
The interobserver variability between 2 observers was measured on 10 patients for the 3 GBPS methods. It was calculated as the difference between the 2 calculated measurements normalized to their average and expressed as a percentage. The variances of the interobserver variability of the 3 GBPS methods were compared using Levene’s test.
P < 0.05 was considered significant.
RESULTS
LVEF
Interobserver variability and paired absolute difference results of LVEF calculated with the GBPS methods are reported in Table 1. The variance of interobserver paired absolute difference and paired variability were lower with the GBPS35% method than with the GBPSG and GBPSM methods (P < 0.04 and P < 0.03).
Interobserver Variability and Paired Absolute Difference of LV Volumes and LVEF Calculated with 3 GBPS Methods
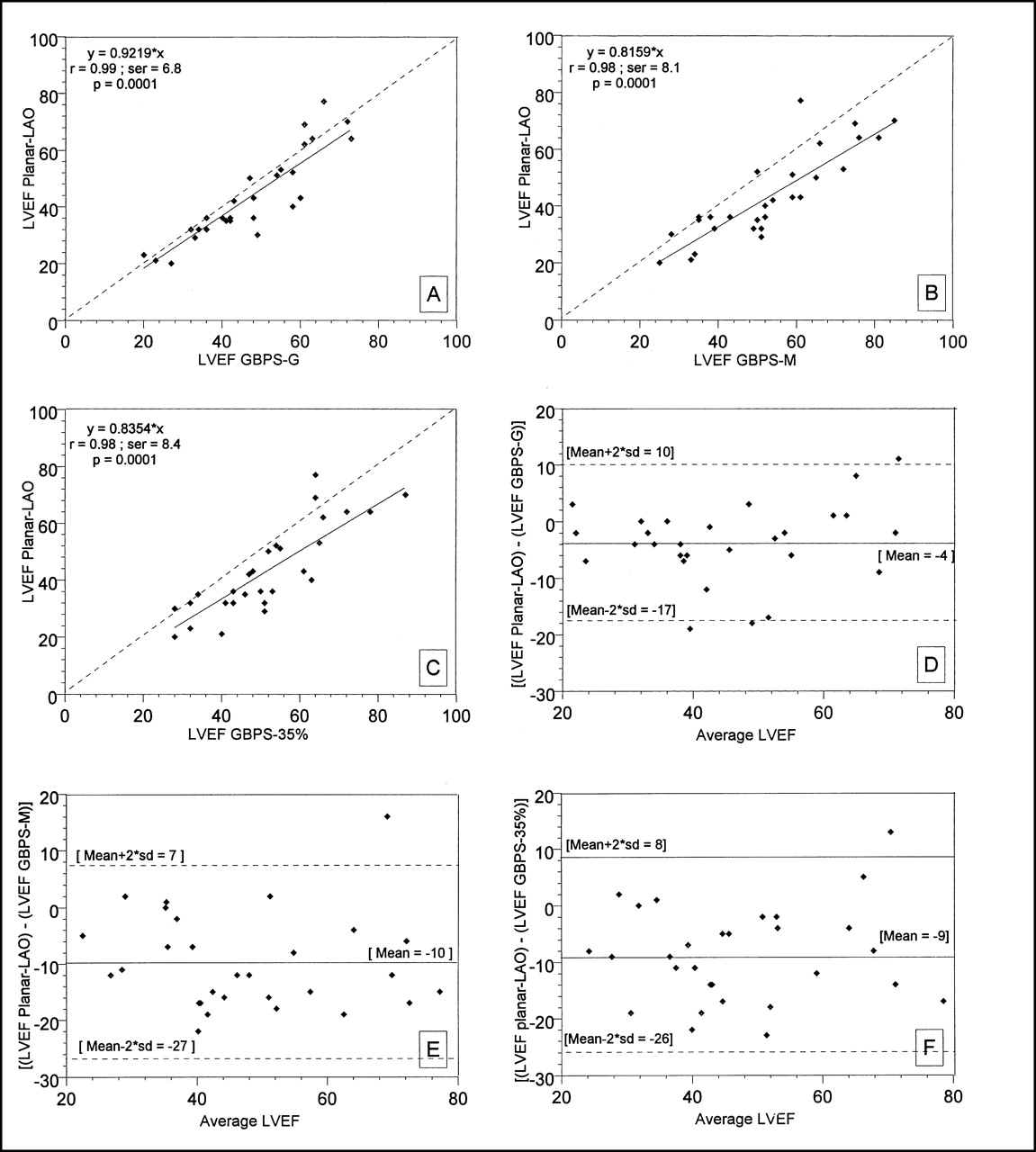
LVEFs calculated with the GBPSG, GBPSM, and GBPS35% methods are linearly correlated with planarLAO LVEF with high r values: 0.99, 0.98, and 0.98, respectively (P < 0.0001) (Figs. 1A–1C).
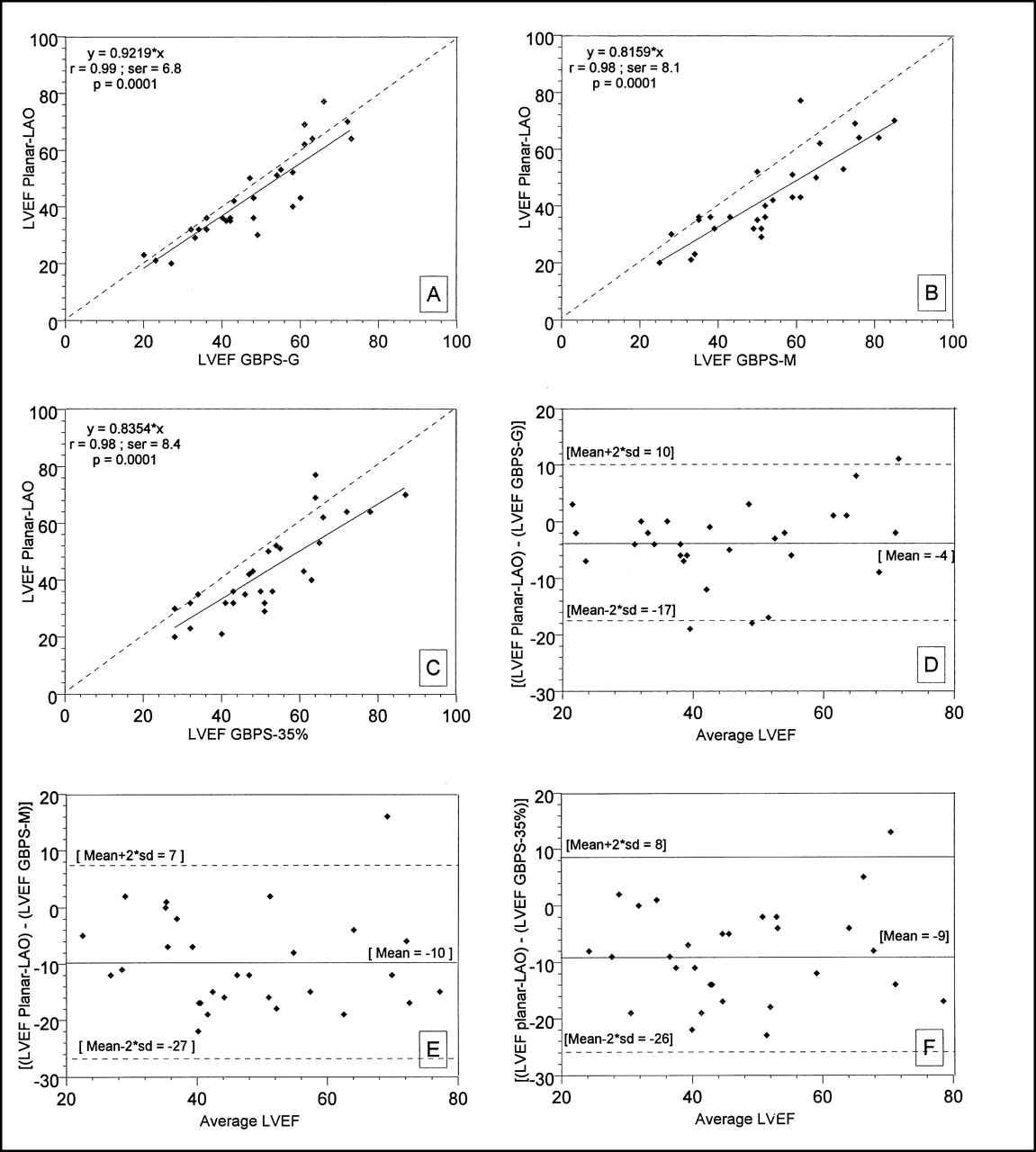
Linear correlation (A–C) and Bland–Altman analysis (D–F) of equilibrium radionuclide angiography GBPS processing methods vs. planarLAO method for LVEF calculation. ser = SE of the regression.
The LVEFs calculated with the GBPSM and GBPS35% methods are similar, with a mean ± SD of paired absolute difference of 1 ± 8 (mean not significantly different from zero). They are higher than with the GBPSG and planarLAO methods, respectively (P < 0.0001) (Table 2).
Comparison of LVEF Calculated with 3 GBPS Methods and Equilibrium PlanarLAO Method
The mean ± SD of paired absolute difference between the LVEF calculated with the GBPSG and GBPSM methods is −5.9 ± 9.4 (mean significantly different from zero; P = 0.0023).
Agreement, as measured with the Bland–Altman method, indicates a constant overestimation of the LVEF with the GBPSG, GBPSM, and GBPS35% methods compared with the planarLAO method over the wide range of the LVEFs evaluated. The means ± SD of paired absolute difference values of GBPS methods are reported in Table 2 with the mean values significantly different from zero (P < 0.005). No correlation was found between the average and the paired absolute difference values for the 3 GBPS methods. The calculated 95% limits of agreement are relatively large (Figs. 1D–1F).
No difference of the variance of the RE between LVEF GBPSG, GBPSM, and GBPS35% methods was found.
LV Volumes
Interobserver variability and paired absolute difference results of LV volumes calculated with the GBPS methods are reported in Table 1. The variance of interobserver paired absolute difference and paired variability of LV volumes were lower with the GBPS35% method than with the GBPSG and GBPSM methods (P < 0.02 and P < 0.0004).
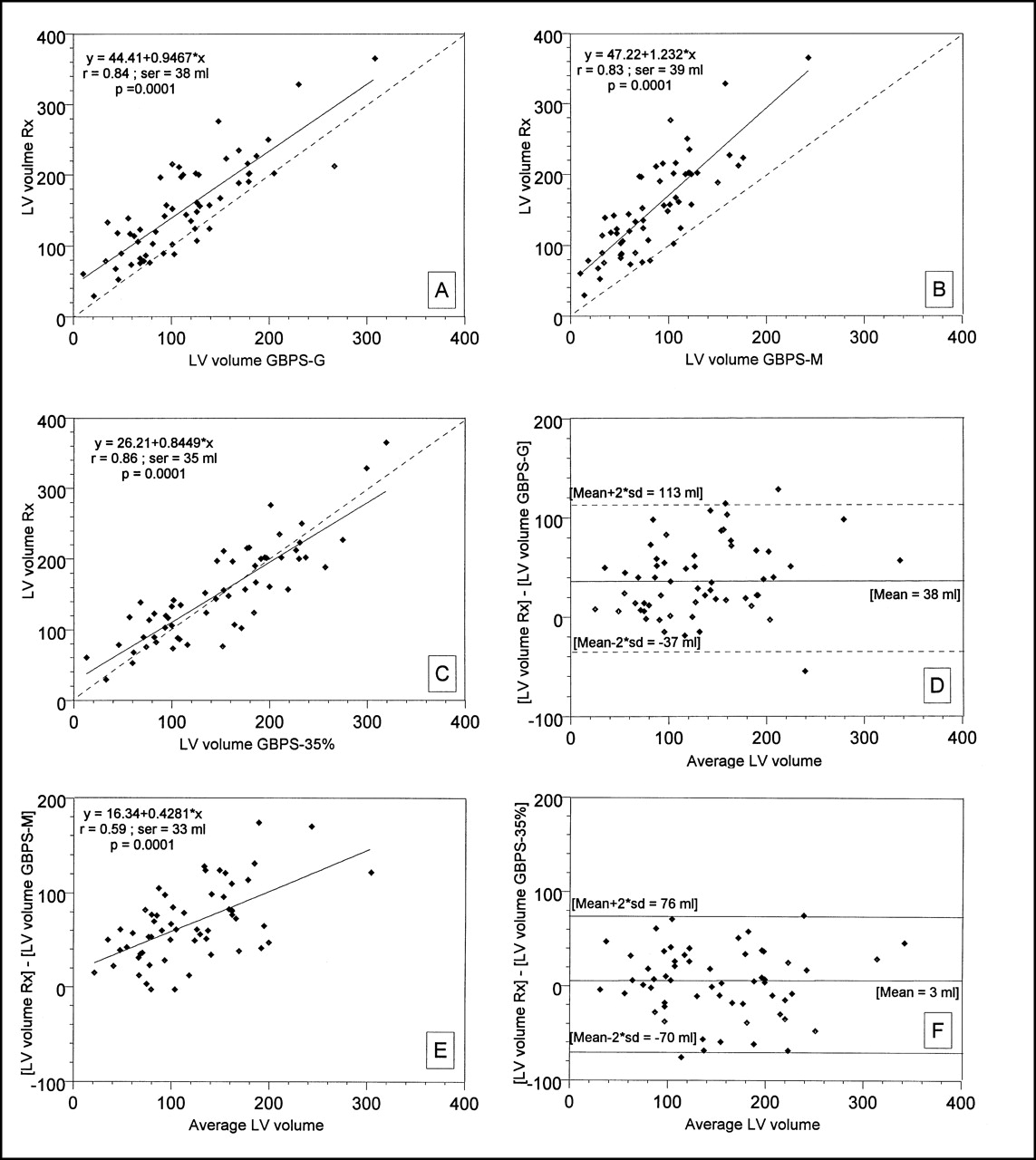
Good linear correlations were found between volumes calculated with the GBPS methods versus the Rx method, with r values of 0.84, 0.83, and 0.86, respectively, with GBPS35%, GBPSG, and GBPSM (P < 0.0001) (Figs. 2A–2C).
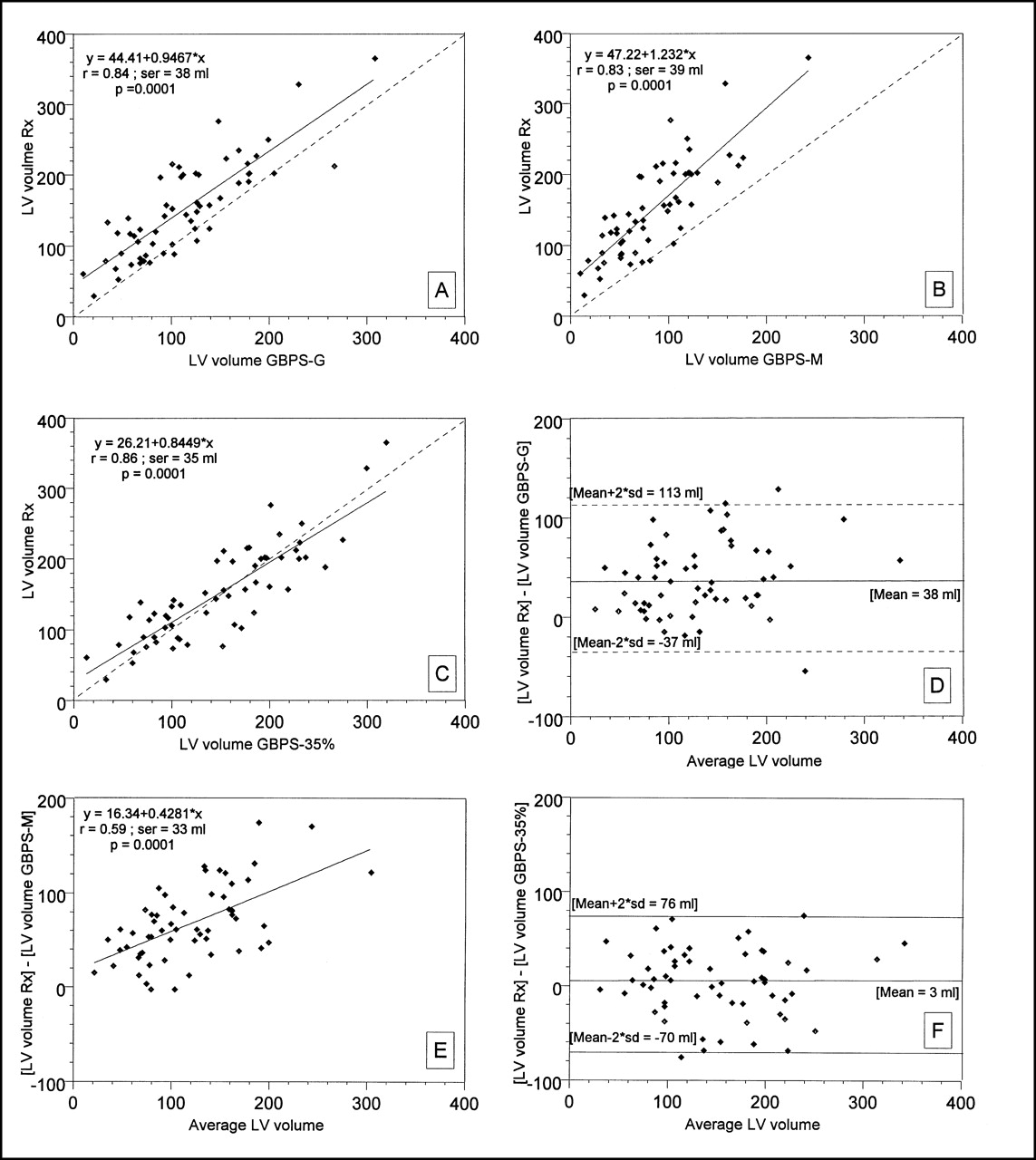
Linear correlation (A–C) and Bland–Altman analysis (D–F) of equilibrium radionuclide GBPS processing methods vs. LV Rx angiography for LV volume calculation. ser = SE of the regression.
LV volumes are lower when calculated with the GBPSM, GBPSG, and Rx methods (P < 0.0001). However, the GBPS35% and Rx methods provide similar values of LV volumes (Table 3).
Comparison of LV Volumes Calculated with 3 GBPS Methods and Rx Method
Agreement, as measured with the Bland–Altman method, indicates no tendency for under- or overestimation as calculated with the GBPS35% method over the wide range of LV volumes evaluated: paired absolute difference of 3 ± 36 mL (mean ± SD; mean not different from zero) (Figs. 2D–2F). However, the GBPSG and GBPSM methods significantly underestimate the Rx LV volumes: paired absolute differences of 38 ± 37 mL and 67 ± 40 mL, respectively, are significantly different from zero (P = 0.0001) (Table 3). No linear correlation was found between the paired absolute difference and the average values of volumes calculated with the GBPSG and GBPS35% methods compared with the Rx LV volumes. However, a moderate but significant linear correlation was found using the GBPSM method (r = 0.6; P = 0.0001). The 95% limits of agreement between the Rx LV volumes and those calculated with the GBPSG and GBPS35% methods are relatively large. After correction with logarithmic transformation for this linear correlation, the GBPSM method underestimated the LV volume by 77% or overestimated the LV volume by 53% compared with the Rx LV volume (Figs. 2D–2F).
No difference of the variance of the RE between LV volumes was calculated with the GBPSG, GBPSM, and GBPS35% methods.
DISCUSSION
This study shows that estimation of the LVEF and volumes is feasible with a simple acquisition technique using GBPS. The estimated values using any of the 3 processing methods (GBPSG, GBPSM, and GBPS35%) are highly correlated with the planarLAO LVEF and Rx LV volumes, and the 3 methods present similar accuracy for LVEF and LV volume estimation.
Planar equilibrium radionuclide angiography withstood the test of time primarily because of the simplicity of its acquisition and processing as well as its great reproducibility. It provides much quantitative or semiquantitative information needed for the clinical management of patients’ LV function. However, progressively, clinicians have had a greater interest in the absolute accurate quantification of the LV and right ventricular volumes and EF as well as regional wall motion. Compared with planar equilibrium radionuclide angiography, the use of GBPS may provide an answer to these clinical interests. First, GBPS is expected to provide all of the clinically useful, well-documented information provided by planar equilibrium radionuclide angiography. Second, GBPS is expected to provide more accurate and precise clinical information with a simple technique (i.e., volumes). The theoretic advantage of GBPS compared with planar equilibrium radionuclide angiography includes the assessment of wall motion without superimposition of the heart structures (17); 3-dimensional regional wall motion quantitative analysis (18,19); assessment of chamber volumes without the complicating effects of attenuation, background correction methods, camera detection efficiency, and blood sampling; assessment of LV and right ventricular volumes and EF; calculation of the regurgitant fraction (20); greater accuracy of the LVEF in the presence of an inferior or anterior myocardial infarction; and regional phase analysis (atrioventricular nodal bypass tracts, arrhythmogenic right ventricular cardiomyopathy) (21).
Until recently, the widespread use of GBPS has been hampered mainly by the lack of availability of automatic processing software. Now that these software programs are being developed, especially with the availability of powerful computers, we are in need of clinical validation studies. Moreover, the limitations and advantages of the different GBPS processing methods should be defined to standardize the processing methods before the development and widespread use of different GBPS processing software. Hopefully, this may obviate the need to confront the harmful reality we are still facing with planar radionuclide angiography—that is, the use of different commercially available processing software programs that raise questions relating to agreement between the results of different processing methods.
In our study, the 3 GBPS processing methods (GBPSG, GBPSM, and GBPS35%) overestimate the LVEF estimated with the planarLAO method (4%, 10%, and 9%, respectively) with relatively large limits of agreement. However, the GBPSM and GBPS35% methods provide similar LVEF values. These findings should be considered when comparing not only the LVEF calculated with different acquisition techniques (GBPS and planarLAO) but also the results of different GBPS processing methods.
Previous studies have shown that LVEFs calculated with the GBPS methods overestimate LVEFs calculated with the planarLAO method, probably because of atrial overlap (22).
In the validation study of LVEF measurements with the GBPSG software, Germano’s group (9) found r = 0.89, an average paired absolute difference of −2.8%, and wide limits of agreement of [−19;13]. These findings are concordant with our study findings: r = 0.9, an average paired absolute difference of −3.9%, and limits of agreement of [−17;10]. We note that Germano’s group used a temporal sampling of 8 frames per cardiac cycle for GBPS and 16 frames for planarLAO, whereas a similar temporal sampling (16 frames) was used in our study. This difference may explain why we did not find any underestimation of the LVEF with the GBPSG method compared with the planarLAO method in patients with a high LVEF (9).
Mariano-Goulart et al. (10) reported a high correlation between the LVEF measured with the GBPSM and planarLAO methods: r = 0.93, SE of the regression = 5.93%, P < 0.0001. Globally, this finding compares favorably with our results: r = 0.85, SE of the regression = 8.45%, and P = 0.0001 (10).
Compared with the Rx LV volume, the GBPSG and GBPSM processing methods underestimate the LV volume, whereas the GBPS35% method provides similar LV volumes. Underestimation of the LV volume with the GBPSG method compared with the Rx volume remained constant over the wide range of LV volumes studied. However, underestimation of the LV volume using the GBPSM method increased linearly with the range of the studied LV volume. These results should be considered when comparing results of different GBPS processing methods. To our knowledge, no previous clinical validation has been reported for LV volumes with either the GBPSG or the GBPSM processing software.
In this study, we found good interobserver reproducibility for the LVEF and LV volumes for the 3 GBPS processing methods. This finding is in agreement with the good interobserver reproducibility reported for the LVEF with the GBPSM processing method: 4.6% variability (10). However, no reproducibility for LVEF measurement was reported for the GBPSG method (9). Moreover, in previous LVEF validation studies for the GBPSG and GBPSM methods, LV volumes were not validated, and reproducibility was not evaluated for LV volume measurement (9,10). We found that the reproducibility of the LVEF and LV volume was best with the GBPS35% manual method; this is intriguing because GBPS35% as a manual method is supposed to give a lower reproducibility in the segmentation of the left ventricle (and, therefore, in estimation of the LVEF and LV volumes) than the GBPSM semiautomatic and GBPSG automatic LV segmentation methods. The significantly higher reproducibility with the GBPS35% manual segmentation method indicates that further gain in reproducibility may be possible by ameliorating these clinically useful automatic segmentation methods.
The GBPSG software presents the advantage of being completely automatic, favoring its widespread clinical use, compared with the semiautomatic GBPSM method and with our time-consuming manual GBPS35% method. One important limitation of the GBPSG software, which must be addressed in the future, is the possibility that the operator can modify the automatically drawn LV ROI. For the GBPSM software, efforts should be made to reduce the operator intervention required to correct the automatic LV segmentation, and it may be useful to address the question of the augmentation in underestimation of the LV volume with the increase in the Rx LV volume.
It would be useful to verify if our results still apply when the recommended acquisition parameters used for clinical validation of the GBPSG and GBPSM software (60 s per stop, 8 frames per cardiac cycle) and the clinically interesting acquisition parameters of 60 s per stop with 16 frames per cardiac cycle are used (providing higher and lower frame count statistics, respectively, than in our study).
We used the LVEF calculated with the planarLAO method and LV volumes calculated with Rx LV angiography as the gold standards. These methods present some well-known limitations: underestimation of the LVEF in the presence of an anterior LV aneurysm and its overestimation in the presence of an inferior myocardial infarction; and overestimation of LV volumes with Rx angiography, particularly in the presence of akinesis, dyskinesis, or aneurysm. In our study, these limitations should have decreased the correlation and the agreement between the evaluated GBPS methods and the gold standard methods. Future studies should address this aspect using different gold standards (i.e., ultrafast CT and MRI).
The ultimate goal of GBPS is to provide reconstructed images in which each voxel represents accurately the absolute activity concentration. For this, we need to minimize the effects of various degrading factors without introducing image distortions and artifacts. This might be achieved with implementation of different compensation methods (motion, detector response, attenuation, scatter, and iterative reconstruction), which should have beneficial effects on GBPS quantification. However, we should not wait until this technical perfection is achieved because GBPS in its current state is a robust technique, even without application of these sophisticated quantification compensation methods.
CONCLUSION
GBPS is a simple, highly reproducible, and accurate technique for LVEF and volume measurement. Complete automation of the GBPS processing software, as with the GBPSG software, is an important step toward its widespread clinical application. Optimization of these automatic processing methods to further improve their performances is desirable.
Findings relating to the reproducibility and accuracy of GBPS for measurement of the LVEF and volumes should be considered when comparing results of different methods (GBPS vs. planarLAO LVEF and GBPS vs. Rx volume) and results of different GBPS processing methods.
Footnotes
Received Jul. 19, 2000; revision accepted Nov. 10, 2000.
For correspondence or reprints contact: Doumit Daou, MD, Department of Nuclear Medicine, Bichat Hospital, AP-HP, 46 rue Henri Huchard, 75877 Paris Cedex 18, France.
REFERENCES
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Diagnosis of Diffuse and Localized Arrhythmogenic Right Ventricular Dysplasia by Gated Blood-Pool SPECT
- Mechanisms of Sudden Cardiac Death in Myocardial Infarction Survivors: Insights From the Randomized Trials of Implantable Cardioverter-Defibrillators
- Quantitative Evaluation of Myocardial Blood Flow and Ejection Fraction with a Single Dose of 13NH3 and Gated PET
- Gated Cardiac SPECT: Has the Addition of Function to Perfusion Strengthened the Value of Myocardial Perfusion Imaging?