


Abstract
The identification of severely dysfunctional but viable myocardium is of particular importance for the selection of patients with depressed left ventricular function who will benefit from coronary revascularization. Assessment of inotropic reserve with dobutamine has recently been used for this purpose. This study compared the accuracy of low-dose dobutamine stress gated myocardial SPECT (DS SPECT) with the accuracy of dobutamine stress echocardiography (DSE) and resting perfusion SPECT for the identification of viable myocardium in patients with previous myocardial infarction. Methods: Resting and low-dose dobutamine (7.5 μg/kg/min) gated 99mTc-tetrofosmin SPECT and echocardiography and resting 18F-FDG PET were prospectively studied in 23 patients with previous myocardial infarction and severely depressed regional function. Twenty-one of them were successfully studied with each technique. The left ventricular wall was divided into 14 segments to assess wall motion using a 5-point scale. PET viability was defined as FDG uptake ≥ 50% of the maximum uptake in a region with normal wall motion. For DS SPECT and DSE studies, viable myocardium was defined as hypokinetic areas with ≥1 point improvement in wall motion. For resting perfusion SPECT, viable myocardium was defined as hypokinetic areas with a relative uptake ≥ 50% of the maximum uptake. Results: Of a total of 294 segments, 55 had severe resting dyskinesis. Thirty-four segments were identified as viable on FDG PET, and 21 segments were identified as nonviable. Eleven segments were inadequately visualized with DSE, including 5 segments in the apex. Sensitivities (78% vs. 76%) and specificities (94% vs. 100%) were similar for DSE and DS SPECT, with a concordance of 86% (κ = 0.72). DS SPECT and perfusion SPECT did not significantly differ with respect to sensitivities (76% vs. 85%, respectively). However, specificity was significantly higher for DS SPECT than for perfusion SPECT (100% vs. 52%, respectively, P < 0.05). Conclusion: This study indicated that DS SPECT correlates well with DSE in the assessment of viability. In addition, gated SPECT can evaluate regional wall motion, even in areas inadequately assessed by echocardiography. DS SPECT may also provide additional information for identifying viable myocardium, which is often overestimated by routine perfusion scans.
In patients with chronic myocardial infarction and impaired left ventricular function, differentiation of dysfunctional but viable myocardium from irreversibly damaged scar tissue has important clinical implications (1,2). Several imaging techniques that evaluate different aspects of myocardial viability are used to identify viable myocardial regions with severely depressed function (3–5). Among these, PET using 18F-FDG is the accepted gold standard for differentiating viable myocardial tissue from scar tissue (6–9). However, this technique can be used only in centers that have a PET camera.
Low-dose dobutamine echocardiography is widely used to assess the inotropic reserve of severely dysfunctional myocardium (10). It is generally accepted that myocardial regions in which contractile function improves after inotropic stimulation will recover function spontaneously or after coronary revascularization (11). Gated myocardial SPECT has been widely used for the simultaneous assessment of perfusion and function. In addition, gated myocardial SPECT permits objective assessment of regional function. Everaert et al. (12) reported that low-dose dobutamine gated SPECT agreed well with dobutamine stress echocardiography (DSE) for the identification of inotropic reserve in infarcted areas. However, those authors did not correlate their findings with other imaging results.
The purpose of this study was to compare the accuracy of low-dose dobutamine stress gated myocardial SPECT (DS SPECT) and resting perfusion SPECT with DSE for the identification of viable myocardium in patients with previous myocardial infarction.
MATERIALS AND METHODS
Study Patients
Twenty-three sequential patients with previous myocardial infarction were prospectively studied from August 1999 to July 2000 (18 men, 5 women; mean age ± SD, 66.5 ± 7.8 y). These patients met the following criteria: the presence of a Q wave infarction caused by total or subtotal occlusion of a coronary artery, the presence of asynergy (severe hypokinesis, akinesis, or dyskinesis) on resting echocardiography, the presence of a normal sinus rhythm, and no concomitant cardiopulmonary or severe valvular diseases or evidence of left ventricular aneurysm. Two patients (8.7%) were excluded from the final evaluation, one patient because of inadequate FDG uptake caused by severe diabetes, and the other because of the development of paroxysmal atrial fibrillation during DSE. Table 1 summarizes the clinical characteristics of the 21 patients. Mean left ventricular ejection fraction was 47.8% ± 11.3% as determined by quantitative gated SPECT images using the fully automatic algorithm developed at Cedars-Sinai Medical Center (Los Angeles, CA) (13). β-adrenergic blocking agents were withdrawn 48 h before the study. The study was approved by the ethics committee of Hokkaido University Hospital. Written informed consent was obtained from each patient.
Clinical Characteristics of the 21 Patients
SPECT Protocol
Perfusion imaging was performed with a 1-d protocol after either maximal treadmill exercise using the Bruce protocol (n = 8) or pharmacologic vasodilation (n = 9). The remaining 4 patients underwent only resting perfusion imaging. Two of these 4 patients took an additional exercise stress test, which had positive findings for one patient, who underwent revascularization, and negative findings for the other patient, who did not undergo revascularization. Patients who underwent exercise treadmill testing received 300 MBq 99mTc-tetrofosmin (Nihon Mediphysics, Hyougo, Japan) at peak exercise and exercised at the same level for an additional minute. Stress imaging was performed 30 min after injection. Patients undergoing pharmacologic testing received an infusion of 0.16 mg/kg/min of adenosine triphosphate for 5 min. Three minutes after completion of the infusion, 300 MBq tetrofosmin were injected. The stress imaging did not use dobutamine studies. Five hours later, 600 MBq tetrofosmin were injected at rest, and imaging was performed 30 min later. After the resting images were obtained, dobutamine stress electrocardiograph- (ECG-) gated acquisition was performed. Uptake was sufficient in almost all segments to perform wall motion analysis, and no difference was observed between resting and dobutamine studies. One patient showed severe reduction of regional uptake. The SPECT window levels were changed for the analysis in this patient.
SPECT Acquisition and Processing
SPECT images were acquired using a rotating dual-detector gamma camera with the detectors mounted at right angles and fitted with high-resolution collimators (VXHR, Vertex; ADAC Laboratories, Milpitas, CA). The image acquisition variables included a 140-keV photopeak with a 20% window, 64 projections at 40 s per projection over a 180° (90° per detector) elliptic orbit, a 38-cm roving detector mask, and a matrix size of 64 × 64. Acquisitions were gated for 8 frames per cardiac cycle, with 100% beat acceptance.
The 8-interval projection datasets were prefiltered with a 2-dimensional Butterworth filter (order, 2.5; critical frequency, 0.22 cycles per pixel; pixel size, 0.64 cm) and reconstructed with filtered backprojection (ramp filter) and no attenuation correction. The resulting transaxial image sets were reoriented into short-axis sets that were then processed in batch mode using a stand-alone workstation (Sun Microsystems, Palo Alto, CA) running software to automatically quantify left ventricular ejection fraction.
The projection datasets were also summed and were prefiltered with a 2-dimensional Butterworth filter (order, 2.5; critical frequency, 0.33 cycles per pixel; pixel size, 0.64 cm), producing high-count short, vertical, and horizontal long-axis images for qualitative interpretation and for polar plot and circumferential count displays.
DS SPECT
A low-dose, graded infusion of dobutamine was administered intravenously at a starting dose of 5 μg/kg/min and increased by 2.5 μg/kg/min at 3-min intervals. ECG-gated SPECT was then performed during the dobutamine infusion at a dose of 7.5 μg/kg/min. The patients underwent continuous ECG monitoring, and blood pressure was recorded at 1-min intervals using an automated cuff.
SPECT Image Interpretation
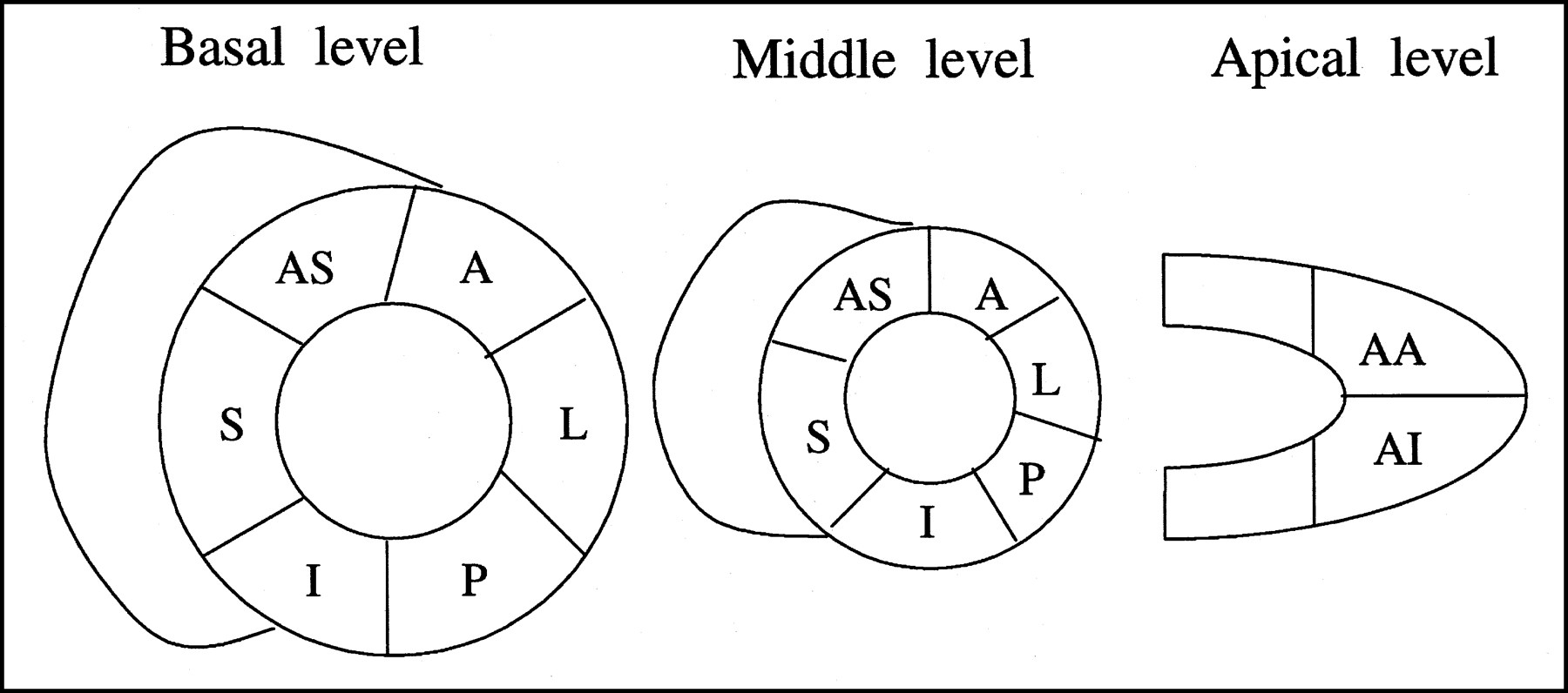
For the analysis of wall motion, the left ventricle was divided into 14 segments (Fig. 1). These segments included the anterior, septal, inferior, posterior, anterolateral, and lateral walls, each subdivided into a basal and mid portion, and the anterior apex and inferior apex. Endocardial wall motion was assessed visually and quantified using a 4-point scoring system as follows: 1 = normal, 2 = mild hypokinesia, 3 = severe hypokinesia, and 4 = akinesia. Viable myocardium was defined as hypokinetic areas with a ≥1 point improvement in the score.
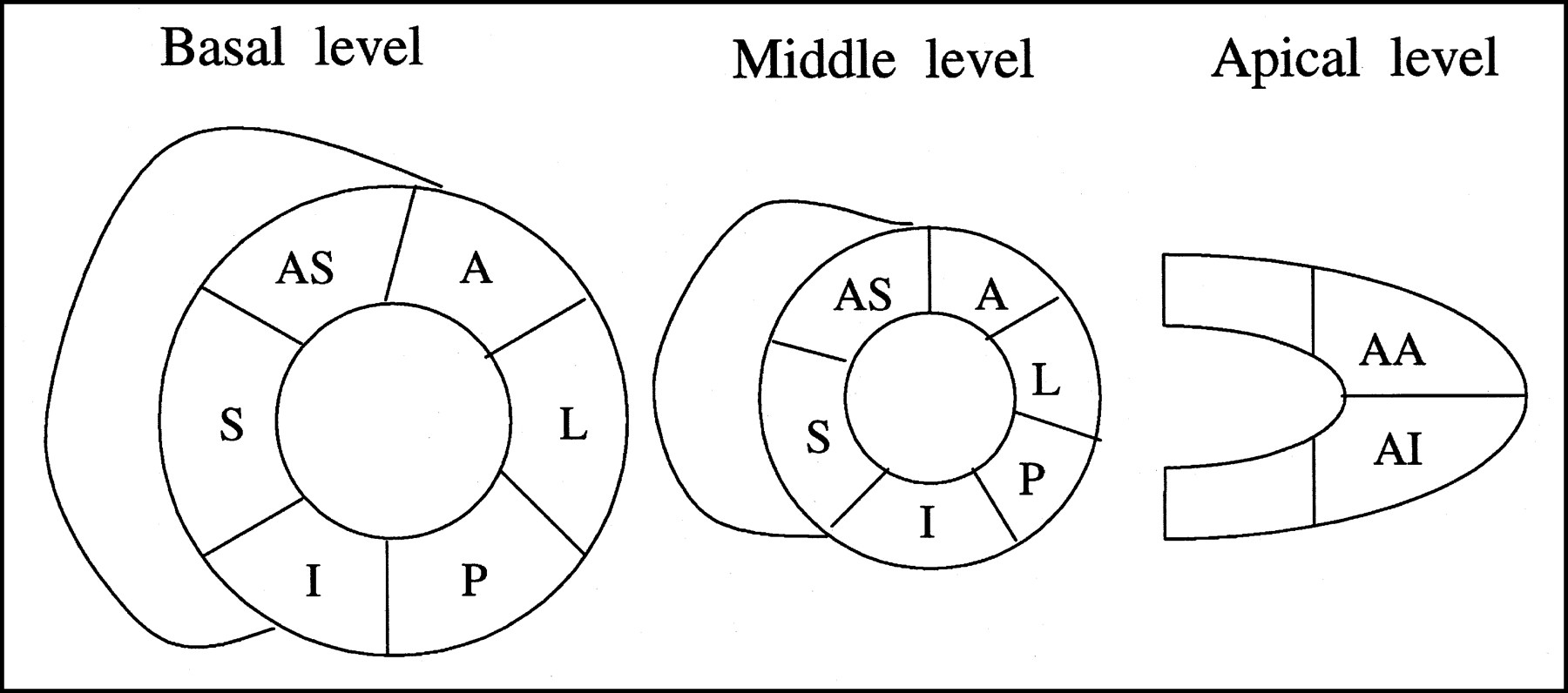
Segmental evaluation pattern for DSE, DS SPECT, and FDG positron emission tomograms. A = anterior; AA = anterior apex; AI = inferior apex; AS = anteroseptal; I = inferior; L = lateral; P = posterior; S = septal.
The gated image sets were read independently by 2 expert observers who were unaware of patient identity and the results of DSE. Interobserver concordance was 94% before discrepancies were resolved by consensus. One observer reviewed the studies twice, at least 2 wk apart, with an intraobserver concordance of 96%.
99mTc-Tetrofosmin Image Analysis
For the quantitative analysis of regional tracer uptake, the individual frames of raw projection data were summed to reconstruct nongated tomograms. Tracer uptake in the summed images was calculated using an automated circumferential profile analysis and expressed as a percentage of the maximum uptake. For resting perfusion SPECT, viable myocardium was defined as hypokinetic areas with a relative tracer uptake > 50% of the maximum uptake.
Echocardiography Protocol
Dobutamine echocardiography was performed using a standard protocol. First, resting echocardiography was performed with the patient lying in the left lateral recumbent position. Echocardiographic imaging was then performed during the intravenous infusion of dobutamine, starting at a dose of 5 μg/kg/min, which was increased every 3 min to 7.5, 10, 20, 30, and 40 μg/kg/min. Images were obtained in the standard parasternal long-axis and short-axis views, with particular attention to determining regional function. During dobutamine infusion, the 12-lead ECG and blood pressure were monitored every minute. The test was ended prematurely if the heart rate reached 85% of the predicted maximum or if any of the following developed: severe angina, a systolic blood pressure < 85 or > 220 mm Hg, ≥2 mm of ST depression, or significant arrhythmia (≥6 beats of supraventricular tachycardia or ≥3 beats of ventricular tachycardia). All studies were performed on a Sonos 1500 ultrasound system (Agilent Technologies, Palo Alto, CA) equipped with a 2.5-MHz transducer.
Echocardiographic Image Processing and Analysis
For the analysis of wall motion, the left ventricle was divided into 14 segments as described for the SPECT study. The basal and middle thirds were divided into 6 segments for the short-axis image. Apical 2-chamber views and vertical long-axis views showed the apical segments, which were divided into 2 segments (Fig. 1). Wall motion was assessed visually, using both endocardial motion and wall thickening, and was quantified using a 5-point scoring system as follows: 1 = normal, 2 = mild hypokinesia, 3 = severe hypokinesia, 4 = akinesia, and 5 = dyskinesia. Viable myocardium was defined as hypokinetic areas with ≥1 point improvement in the wall motion score.
The dobutamine echocardiographic studies were interpreted randomly using all 7 digital images for each view displayed on 2 monitors placed side by side to allow simultaneous review of all 7 stages of the test. All studies were read by a single experienced investigator who was unaware of the clinical information, the radionuclide information, and the results of resting echocardiography. A wall motion score was assigned to each of the 14 segments for every stage of the test.
FDG PET
PET was performed using a whole-body scanner (ECAT EXACT HR+; Siemens Medical Systems, Inc., Hoffman Estates, IL/CTI, Knoxville, TN) equipped with 68Ge/68Ga retractable line sources for transmission scans. Transmission images were obtained using an external ring of 68Ga so that the emission images could be corrected for photon attenuation. The intrinsic resolution was 4.5-mm full width at half maximum. For improved myocardial glucose uptake, each patient received a solution containing 50 g glucose 30 min before the injection of FDG (n = 5). If glucose intolerance was apparent, hyperinsulinemic–euglycemic clamping was performed (n = 16). Images were corrected for attenuation using coefficients received during a 20-min transmission scan. Thirty minutes after glucose loading, or 1 h after the start of insulin clamping, 555 MBq FDG were injected. Forty minutes later, exogenous myocardial glucose use was determined from a 20-min static scan.
PET Image Analysis
Segmental FDG uptake was assessed quantitatively using 2 short-axis and vertical long-axis tomograms. Viability was defined as a mean segmental FDG uptake ≥ 50% of the maximum uptake.
Statistical Analysis
Data are reported as mean ± SD. The κ statistic was used to evaluate concordance among DS SPECT, DSE, and perfusion SPECT. Frequencies were compared using χ2 analysis or the Fisher exact test. P < 0.05 was considered statistically significant.
RESULTS
No patients experienced chest pain or significant ST depression during DS SPECT or low-dose DSE.
All segments in the wall motion analysis could be assessed using DS SPECT. In contrast, 11 segments, including 5 apical segments, could not be well visualized by DSE. Of the 294 segments analyzed, 55 had severe resting dyssynergy (echocardiographic score ≥ 3). Thirty-four of these segments were identified as viable (Fig. 2) on the basis of FDG PET analysis, and 21 segments were identified as nonviable (Fig. 3). No segments with wall motion abnormality were considered nonviable at a dobutamine dose of 7.5 μg/kg/min but viable at doses > 7.5 μg/kg/min.
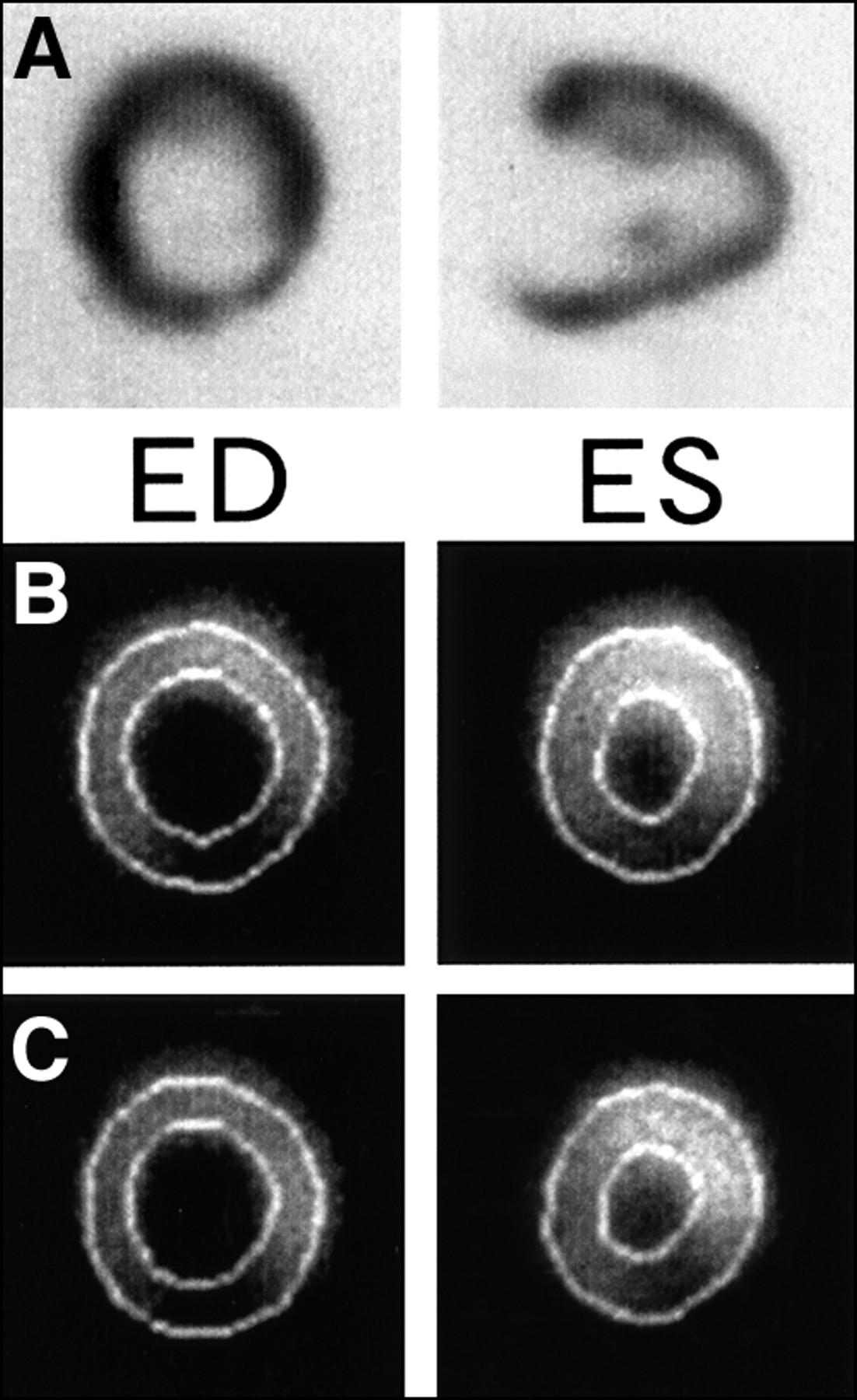
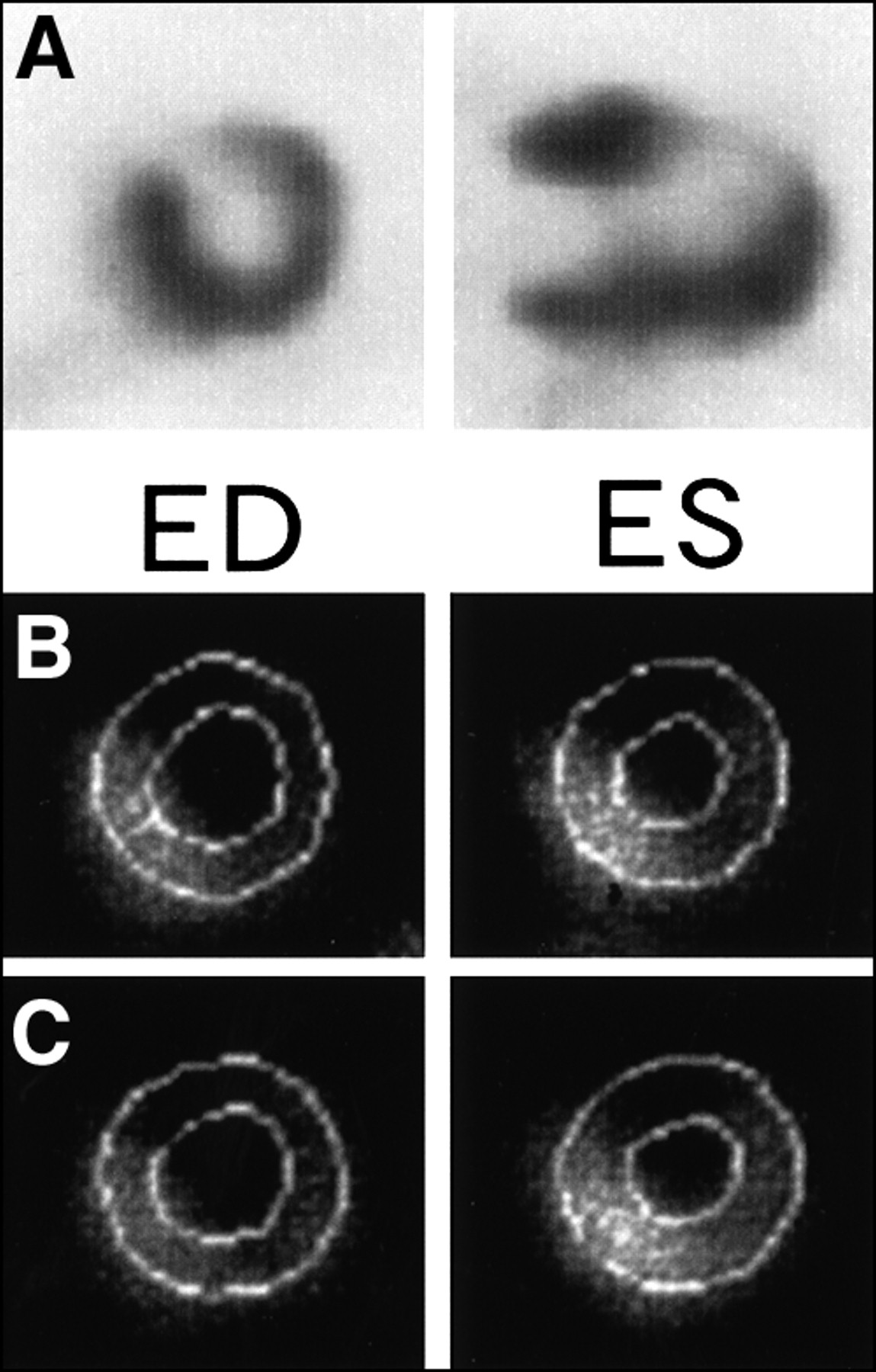
Representative images from 70-y-old man with inferior myocardial infarction. (A) Inferior segment was considered viable on basis of FDG PET findings. (B) Inferior segment had severe hypokinesis in resting gated SPECT image. (C) Dobutamine stress improved wall motion abnormality. ED = end-diastole; ES = end-systole.
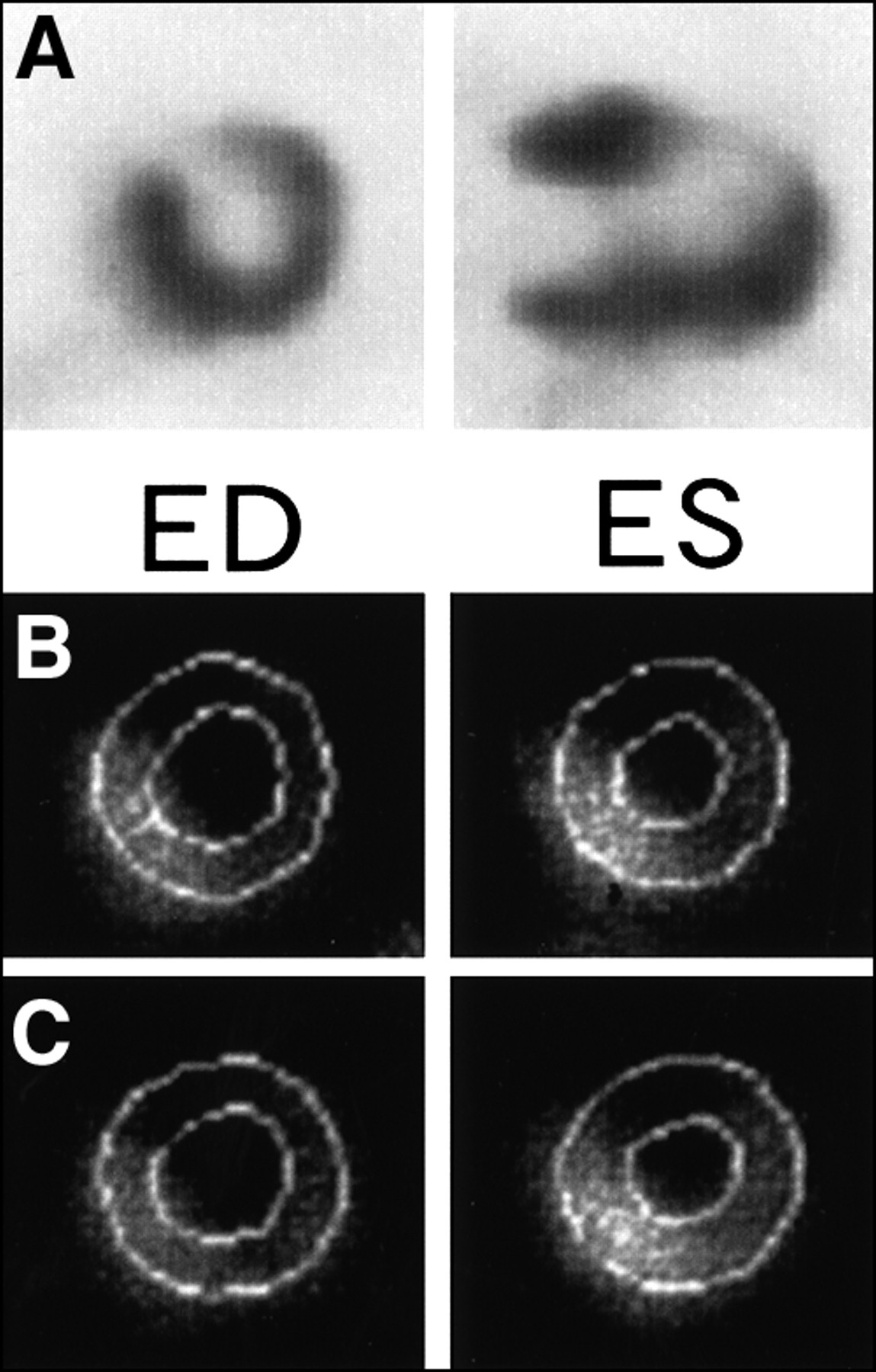
Representative images from 72-y-old woman with anteroseptal myocardial infarction. (A) Anteroseptal segment was considered not viable on basis of FDG PET findings. (B) Anteroseptal segment showed severe hypokinesis on resting gated SPECT image. (C) No improvement in wall motion was observed during dobutamine infusion. ED = end-diastole; ES = end-systole.
No significant differences were observed between DSE and DS SPECT with respect to the sensitivity, specificity, positive predictive value, and negative predictive value for the detection of dysfunctional but viable myocardium (Table 2). In the dysfunctional segments, the rate of concordance for detecting viability between DS SPECT and DSE was 86% (κ = 0.72; Table 3).
Diagnostic Accuracy of Viability Assessment by Each Method
Viability Findings Based on DS SPECT and DSE
DS SPECT and perfusion SPECT at rest did not significantly differ in sensitivity and negative predictive value for detecting dysfunctional but viable myocardium. However, DS SPECT had a significantly higher specificity (P < 0.05) and positive predictive value (P < 0.01) than did perfusion SPECT at rest (Table 3). In dysfunctional segments, the rates of concordance for detecting viability between DS SPECT and perfusion SPECT at rest was only 65% (κ = 0.32; Table 4).
Viability Findings Based on DS SPECT and Rest SPECT
DISCUSSION
The data indicate that DS SPECT correlates well with DSE in the assessment of viability. Because objective assessment of regional function is available with SPECT, gated SPECT can be used to evaluate regional wall motion, even in areas inadequately assessed by echocardiography. In addition, in the identification of viable myocardium, DS SPECT may provide information that is lacking from routine resting perfusion scans.
Gated SPECT has been used for the objective assessment of left ventricular function (13,14). We have applied gated SPECT to the assessment of regional function under low-dose dobutamine infusion. Our study showed that the results of DS SPECT correlated well with those of DSE. This finding is in keeping with the previous report showing good agreement between DS SPECT and DSE in the identification of inotropic reserve in infarcted areas (12). However, the previous study did not compare these results with other measures of viability, such as PET measurements of viability or functional recovery (10). To the best of our knowledge, our study is the first to compare the 2 methods with FDG PET.
Low-dose dobutamine echocardiography has been used as an effective method for evaluating myocardial viability. Previous studies of low-dose dobutamine echocardiography have predicted the recovery of regional function after revascularization with sensitivities ranging from 74% to 92% and specificities ranging from 74% to 96% (5,15–18). Recent studies comparing nuclear methods with DSE and regional wall motion after revascularization confirmed the high sensitivity and high negative predictive value of PET and thallium SPECT imaging. In contrast, DSE was found to be slightly less sensitive but more specific for predicting functional improvement (19).
The sensitivities determined in this study (DSE, 78%; DS SPECT, 76%) agree with previous data. The specificities determined in this study (DSE, 96%; DS SPECT, 100%) are also in keeping with previous data. Therefore, DS SPECT is relatively sensitive and highly specific in predicting functional recovery.
DS SPECT and DSE
In this study, 11 of 294 segments (3.7%) could not be adequately assessed by DSE. Five of them were in the apex. Previous studies have shown that 0%–10% of segments are inadequately assessed by DSE (5,15,19–21). Sawada et al. (22) reported that 10% of segments cannot be assessed. In our study, the percentage of segments with inadequate assessment was slightly higher, probably because of the relatively greater age of our population (mean age, 67 y). The echocardiographic analysis was complicated by the presence of chronic obstructive pulmonary disease and other factors. Therefore, in patients whose regional wall motion cannot be assessed by DSE, DS SPECT can be used to evaluate myocardial viability.
Comparison with Perfusion Imaging
Myocardial uptake of 99mTc-labeled perfusion agents can be used to identify reversible ischemic myocardium (18,19,23). Uptake and retention of 99mTc depends on cell membrane integrity and mitochondrial function and therefore reflects cellular viability. Recent studies indicated that, on the basis of a relative uptake ≥ 50% of the normal value defining viability (23), 99mTc had high sensitivity but relatively low specificity for identifying viable tissue (15,24–26). Our findings agree with these previous data. In our study, the specificity and positive predictive value of DS SPECT were significantly higher than the values for resting perfusion SPECT. Therefore, in the identification of viable myocardium, DS SPECT may provide information in addition to that provided by routine perfusion scans.
Study Limitation
Assessing regional function in patients with a large and severe perfusion defect is somewhat difficult. Manrique et al. (27) reported underestimation of left ventricular ejection fraction by gated SPECT in patients with perfusion defects. However, Germano (28) and Stollfuss et al. (29) found that large perfusion defects had no significant effect on estimation of left ventricular ejection fraction. In our study, no patients had large perfusion defects, which may cause errors in defining myocardial walls.
We used FDG PET as the gold standard for detecting myocardial viability. However, we did not assess the reversibility of regional wall motion abnormalities or global dysfunction, although this reversibility is considered an accurate indicator of myocardial viability.
Germano et al. (30) reported that quantitative gated SPECT (QGS) software (Cedars-Sinai) can be used to assess regional ventricular function quantitatively. However, evaluation of wall motion in the abnormal area is difficult. In this study, we also used automated algorithms for the assessment of changes in regional wall thickening but could not separate viable from nonviable segments. The QGS software divided left ventricular segments automatically. If the areas of asynergy are small, the automatically separated segments can include both normal and abnormal areas and thereby underestimate wall motion abnormalities.
The analytic correlation among echocardiographic segments, SPECT and PET segments, anatomy, and vascular territories is not known precisely. However, we used the same 14-segment model for 3 modalities, thereby reducing misalignment between these modalities.
In SPECT, image quality may deteriorate with gut activity; however, no overlapping gut activity occurred in this study. DS SPECT required a long acquisition time. Shortening of acquisition time is needed for further studies.
Echo data analysis used all the images from stress echocardiography (5–40 μg/kg/min), whereas DS SPECT used only the 7.5 μg/kg/min image. Afridi et al. (5) reported that the optimal dose of dobutamine in the detection of myocardial hibernation was 7.5 μg/kg/min. In our study, we evaluated wall motion on DS SPECT at a 7.5 μg/kg/min dose of dobutamine.
Some of our patients had relatively preserved global left ventricular function. However, these patients had regionally severe left ventricular dysfunction. Differentiation of viable myocardium is also relevant in these patients, who need revascularization to improve their prognosis and lower the risk of cardiac events. The current data provide useful information for clinical decision making. Larger numbers of patients with severely depressed left ventricular function are needed to further validate this method.
Clinical Implications
FDG PET, although considered the most reliable method for determining viability, is not widely available. In addition, applying FDG PET to diabetic and glucose-intolerant patients poses difficulties. These patients may require euglycemic–hyperinsulinemic clamping to assess viability using FDG PET (31).
The echocardiographic approaches are attractive from both an acquisition time and an economic point of view. However, echocardiography could not adequately assess many obese or elderly patients in this study. Image quality had a significant effect on the assessment of regional wall motion (20). Recently, the percentage of obese and elderly individuals with lung disease has increased among patients with ischemic heart disease. On the other hand, DS SPECT can be performed on almost every patient irrespective of body size or age. In addition, objective assessment of regional function is feasible in any location. Therefore, DS SPECT may be a valuable method for assessing myocardial viability.
CONCLUSION
DS SPECT correlated well with DSE in the detection of viable myocardium. In addition, gated SPECT could evaluate regional wall motion, even in areas inadequately assessed by echocardiography. In the identification of viable myocardium, dobutamine gated SPECT may provide information that is often missed by routine perfusion scans.
Footnotes
Received Sep. 20, 2000; revision accepted Feb. 14, 2001.
For correspondence or reprints contact: Nagara Tamaki, MD, Department of Nuclear Medicine, Hokkaido University School of Medicine, Kita-Ku, Kita 15 Nishi 7, Sapporo, 060-8638, Japan.
REFERENCES
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Hyperpolarised magnetic resonance for in vivo real-time metabolic imaging
- Gated Myocardial Perfusion SPECT: Basic Principles, Technical Aspects, and Clinical Applications
- Reduced Oxidative Metabolic Response in Dysfunctional Myocardium with Preserved Glucose Metabolism but with Impaired Contractile Reserve
- The Diagnostic and Prognostic Value of ECG-Gated SPECT Myocardial Perfusion Imaging
- Sequential Strategy Using Multimodality Viability Tests: Does It Work?