


Abstract
The aim of this study was to introduce a new quantification method for 153Sm-ethylenediaminetetramethylenephosphonate (EDTMP) and 186Re-(tin)1,1-hydroxyethylidene diphosphonate (HEDP) to separately measure bone uptake and soft-tissue retention of these radiopharmaceuticals. Methods: Studies were performed on 23 men and 6 women undergoing radionuclide therapy for palliation of bone pain. Whole-body images were acquired at 3 min, 3–4 h, and 24–72 h after injection of 1,295 MBq 186Re-HEDP and 37 MBq 153Sm-EDTMP per kilogram of body weight. The activities for whole body, urinary bladder, and both thighs, as representative of soft tissue, were measured by region-of-interest technique. A background region of interest adjacent to the head was used to correct for bremsstrahlung. Bone uptake was calculated as initial whole-body activity minus urinary excretion and remaining soft-tissue activity. Results: For 186Re-HEDP (n = 11) the mean bone uptake at 3 h after injection was 13.7% ± 8.6% of initial whole-body activity. The remaining soft-tissue activity was 49.4% ± 16.9%, and urinary excretion was 36.9% ± 14.4%. At 24 h after injection, bone uptake reached a value of 21.8% ± 9.0%. Urinary excretion increased to 65.3% ± 12.8% according to a decreasing soft-tissue remainder activity of 12.8% ± 5.4%. The corresponding results for 153Sm-EDTMP (n = 18) at 3 h after injection were 29.2% ± 15.5% for bone uptake, 32.3% ± 12.9% for urinary excretion, and 38.4% ± 14.5% for soft tissue. At 24 h after injection, we calculated values of 47.7% ± 11.2% for bone uptake, 39.5% ± 13.8% for urinary excretion, and 12.7% ± 4.7% for soft tissue. Conclusion: Bone uptake and soft-tissue retention for both 186Re-HEDP and 153Sm-EDTMP as obtained in this study agree well with the conventional 24-h whole-body retention measurements for these tracers. However, by this new scintigraphic quantification method, bone uptake and soft-tissue retention can be calculated separately, thus providing more detailed kinetic data and potentially improving the dosimetry of these radiopharmaceuticals in, for example, assessment of radiation dosage to bone and bone marrow.
- 186Re-(tin)1,1-hydroxyethylidene diphosphonate
- 153Sm-ethylenediaminetetramethylenephosphonate
- whole-body scintigraphy
- bone uptake
- soft-tissue retention
Treatment with 186Re-(tin)1,1-hydroxyethylidene diphosphonate (HEDP) or 153Sm-ethylenediaminetetramethylenephosphonate (EDTMP) has been proven safe and successful for palliation of bone pain in patients with widespread osseous metastases (1–6). The major side effect of this therapy is a decrease in platelets and leukocytes in the peripheral blood (3,7) caused by an irradiation of stem cells in the bone marrow by β-particles of the radiopharmaceutical affixed to the bone matrix. Thus, the extent of bone uptake is the main determinant of radiation damage to bone marrow. A sensitive and well-established method for quantification of bone uptake is to measure whole-body retention of bone-seeking tracers at 24 h after injection, as introduced by Fogelman et al. (8,9). Unfortunately, this method is of limited value because whole-body retention measurements are not routinely available in nuclear medicine departments (10). Thus, measuring urinary excretion of the activity up to 24 h after injection is commonly applied to calculate whole-body retention of the tracer (11). However, measurement of neither whole-body retention nor cumulative urinary excretion allows differentiation between bone uptake and nonskeletal tissue retention of the radiopharmaceutical. Soft-tissue retention of diphosphonates, however, is known to be as high as 30% of whole-body retention at 24 h after injection (12,13), so that using whole-body retention data instead of bone uptake data for bone marrow dosimetry of these tracers seems inappropriate. The aim of this study, therefore, was to measure net bone uptake and soft-tissue retention of 186Re-HEDP and 153Sm-EDTMP in patients undergoing therapy for bone pain palliation by modifying a recently introduced quantification method for 99mTc-hydroxymethylene diphosphonate based on whole-body bone scanning (13,14).
MATERIALS AND METHODS
Patients
Imaging was performed on 29 patients (23 men, 6 women; age range, 50–79 y; median age, 64 y). All patients underwent therapy with either 186Re-HEDP (n = 11) or 153Sm-EDTMP (n = 18) for palliation of severe pain caused by multiple bone metastases of various tumors, as proven by conventional bone scanning. Patient data are presented in Tables 1 and 2. After giving informed consent to the acquisition of three whole-body scans, patients were included in this study when serum creatinine concentrations were in the normal range (0.6–1.2 mg/dL) and when no chemotherapy, external beam radiation, or treatment with bisphosphonates had been performed during 6 wk before therapy with 186Re-HEDP or 153Sm-EDTMP.
186Re-HEDP: Patient Data and Results for Soft-Tissue Retention, Urinary Excretion, and Bone Uptake
153Sm-EDTMP: Patient Data and Results for Soft-Tissue Retention, Urinary Excretion, and Bone Uptake
Radiopharmaceuticals
For palliation of bone pain, we used 186Re-HEDP (Mallinckrodt, Petten, The Netherlands) and 153Sm-EDTMP (CIS, Gif-Sur-Yvette, France). 186Re-HEDP was applied in a standard patient dose of 1,295 MBq, whereas an activity of 37 MBq/kg of body weight was administered for 153Sm-EDTMP.
Data Acquisition
Whole-body images were acquired simultaneously from both anterior and posterior views at 3 min; at 3 h; and, in most patients, at either 24 h or 72 h after a bolus injection of the respective radiopharmaceutical. The scan speed was 40 cm/min at 3 min and 10 cm/min at the later imaging times. For each patient, images were obtained under the same conditions using a double-head gamma camera system (Bodyscan; Siemens, Erlangen, Germany) equipped with high-resolution low-energy collimators. The energy window was 137 keV ± 15% for 186Re and 103 keV ± 15% for 153Sm. Images were stored in a 1024 × 384 matrix for digital image processing.
Quantification
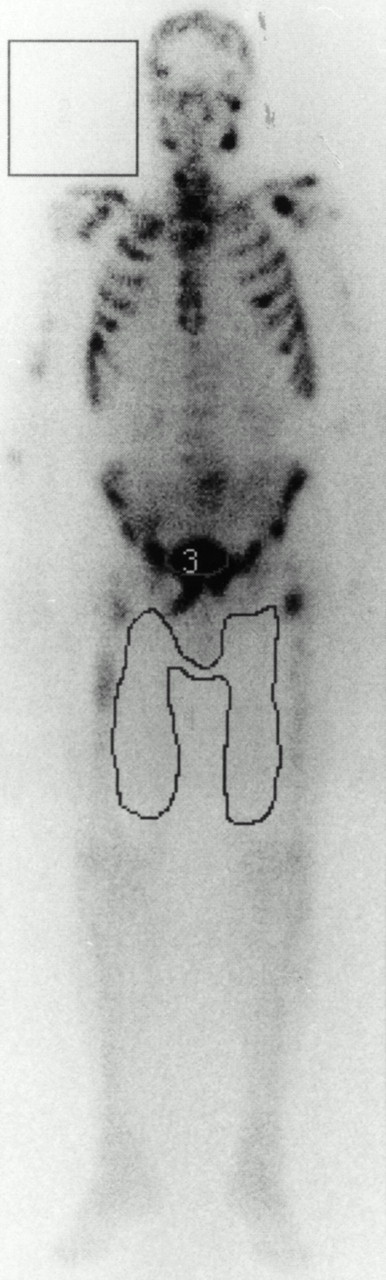
For each image the activities of the whole body, the urinary bladder, and the adductor muscles of both thighs, as representative of soft tissue, were measured by a conventional region-of-interest (ROI) technique from both anterior and posterior views. Additionally, a rectangular ROI adjacent to the head and shoulders was used to measure the bremsstrahlung of the β-particles of the radionuclides. An example for ROI positions is given in Figure 1. From these data, the geometric mean for each ROI was calculated after correction for radioactive decay, for different scan speeds, and for bremsstrahlung. After distribution of the injected tracer, total whole-body activity at 3 min after injection was defined as 100% (15). This initial total whole-body activity of each patient was used as the reference value for further calculations of activity data, which are all given as percentages of it. Furthermore, on the blood-pool image 3 min after injection, the initial whole-body activity was defined as maximum soft-tissue activity, and on the later images, the activities of the adductor muscles represent decreasing soft-tissue retention. Thus, soft-tissue activity compared with initial total whole-body activity equals the activity of the adductor muscles compared with the initial adductor activity at 3 min after injection. Urinary excretion was determined by the difference of whole-body activities between the reference image at 3 min and the image of interest plus urinary bladder activity. From these data, bone uptake was calculated for each time as 100% initial whole-body activity minus both urinary excretion and soft-tissue retention.

ROI positions on whole-body scintigram from anterior view 24 h after injection of 1,295 MBq 186Re-HEDP.
The equation used to calculate soft-tissue retention was soft (t) = total (3 min) × add (t)/add (3 min), where soft = soft-tissue retention, t = time after injection, total = total whole-body activity, and add = activity of adductor muscles. The equation used to calculate urinary excretion was urine (t) = (total (3 min) − total (t)) + bladder (t), where urine = urinary excretion and bladder = urinary bladder activity. The equation used to calculate bone uptake was bone (t) = total (3 min) − soft (t) − urine (t), where bone = bone uptake. For all three equations, the data were the geometric mean of the ROI from the anterior and posterior views, corrected for scan speed, radioactive decay, and bremsstrahlung.
According to the data measured by ROI technique, time–activity curves for soft tissue and for urinary excretion were established for each patient using monoexponential curve fitting. From these fitted curves, the time–activity curve for the bones was derived according to the bone uptake equation. For direct comparison of patient results, bone uptake, urinary excretion, and remaining soft-tissue activity were calculated from the fitted curves for 3 and 24 h after injection.
Statistics
For calculating time–activity curves from the values measured for each time, exponential curve fitting by the least squares method was used (16). The best fit proved to be a monoexponential curve asymptotically reaching a plateau according to a constant factor: an increasing curve for urinary excretion and a decreasing curve for soft-tissue retention (13). Pooled data given in the Results represent mean ± 1 SD. The two-tailed Student t test for unpaired data was used to evaluate differences, with P < 0.05 considered to be statistically significant. A linear regression analysis was performed to calculate correlation coefficients for bone uptake and soft-tissue retention relative to the number of metastases (16).
RESULTS
Fitted values for soft-tissue activities, urinary excretion rates, and bone uptake data at 3 and 24 h after injection are summarized in Tables 1 and 2 for patients treated with 186Re-HEDP and 153Sm-EDTMP, respectively.
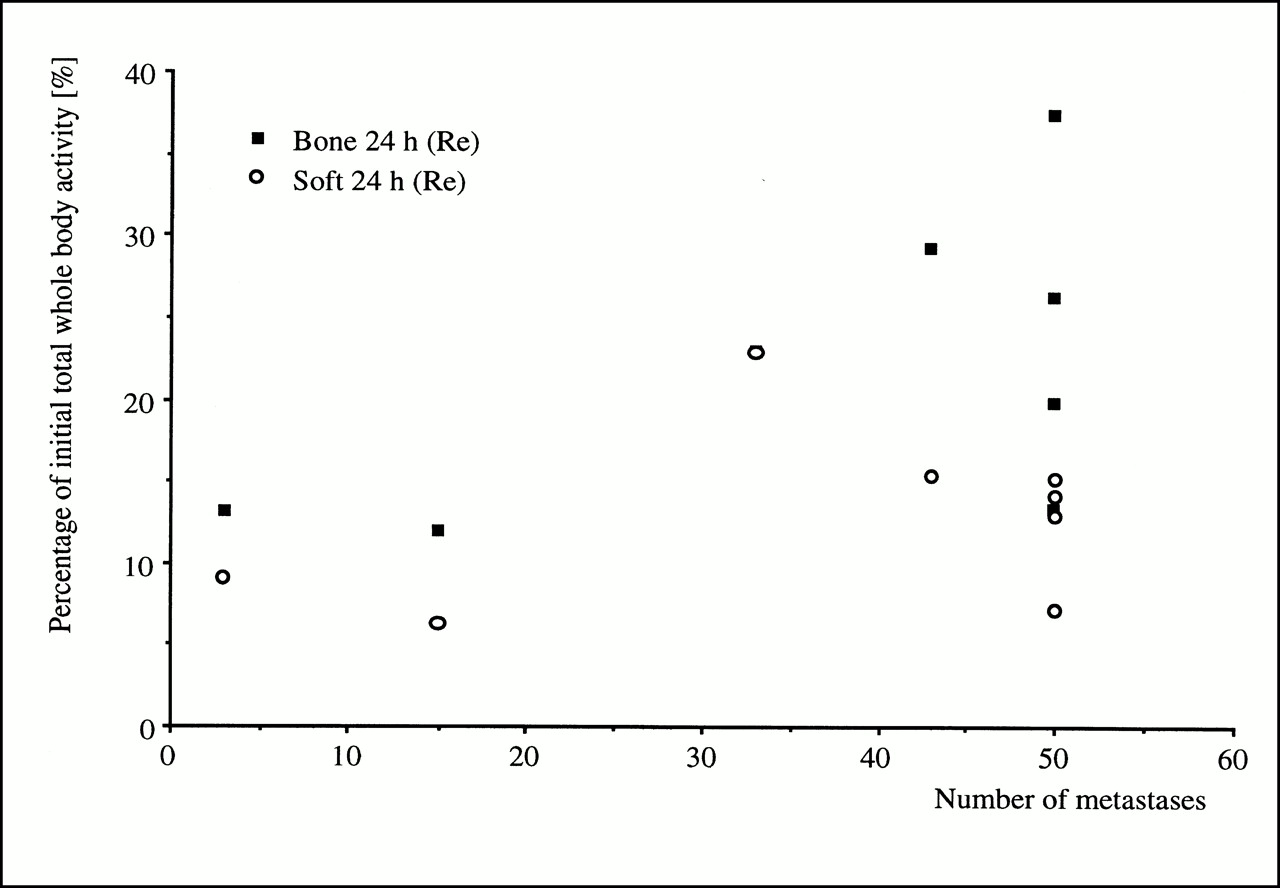
For patients receiving 186Re-HEDP (n = 11), mean bone uptake was 13.7% ± 8.6% at 3 h after injection and increased to 21.8% ± 9.0% at 24 h after injection. During this period, the remaining soft-tissue activity decreased from 49.4% ± 16.9% at 3 h after injection to 12.8% ± 5.4% at 24 h after injection according to increasing urinary excretion rates of 36.9% ± 14.4% at 3 h after injection and 65.3% ± 12.8% at 24 h after injection. Thus, after 24 h, bone activity was less than twice as high as the remaining soft-tissue activity (Fig. 2). However, bone uptake values revealed a positive linear correlation with the number of osteoblastic metastases (r = 0.58), whereas soft-tissue retention showed nearly the same values in all patients irrespective of the number of metastases (r = 0.21), as shown in Figure 3.

Mean activity data (including SE bar) for bone uptake, soft-tissue retention, and urinary excretion at 3 h and 24 h, respectively, after injection.

Relationship between number of bone metastases and both bone uptake (r = 0.58) and soft-tissue retention (r = 0.21) for 186Re-HEDP at 24 h after injection
For patients receiving 153Sm-EDTMP (n = 18), mean bone uptake was 29.2% ± 15.5% at 3 h after injection and increased to 47.7% ± 11.2% at 24 h after injection. During this period, the remaining soft-tissue activity decreased from 38.4% ± 14.5% at 3 h after injection to 12.7% ± 4.7% at 24 h after injection. Urinary excretion rates were nearly constant from 3 h after injection until 24 h after injection (32.3% ± 12.9% vs. 39.5% ± 13.8%). Thus, within 3 h approximately 80% of the activity totally excreted had been voided, as depicted in Figure 2. Bone uptake values also revealed a positive linear correlation with the number of osteoblastic metastases (r = 0.65), whereas the remaining soft-tissue activity proved to be independent of the extent of metastatic bone disease (r = 0.27), as shown in Figure 4.
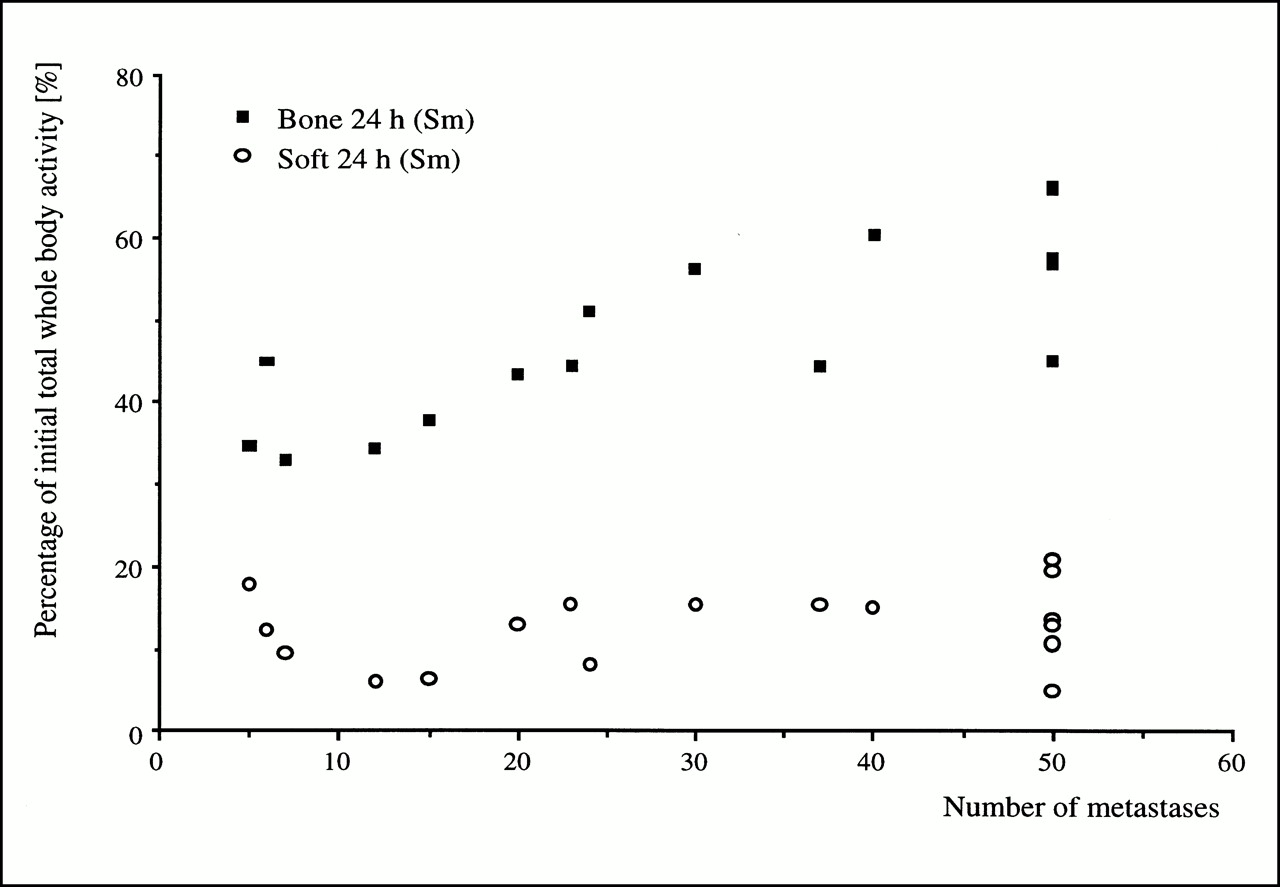
Relationship between number of bone metastases and both bone uptake (r = 0.65) and soft-tissue retention (r = 0.27) for 153Sm-EDTMP at 24 h after injection
Significantly higher bone uptake values (P < 0.05) were found for 153Sm-EDTMP than for 186Re-HEDP (Fig. 2), although the two subsets of patients had similar numbers of osteoblastic metastases and extents of metastasis (Tables 1 and 2). On the other hand, the mean tracer retention in soft tissue at 24 h after injection was the same for both radiopharmaceuticals (12.8% ± 5.4% vs. 12.7% ± 4.7%). Thus, urinary excretion was significantly higher for 186Re-HEDP than for 153Sm-EDTMP. The kinetic data for both radiopharmaceuticals are summarized in Table 3.
Mean and Range for Soft-Tissue Retention, Urinary Excretion, and Bone Uptake
DISCUSSION
In this study, a new method has been used to measure skeletal uptake, soft-tissue retention, and urinary excretion of 186Re-HEDP and 153Sm-EDTMP on the basis of whole-body bone scanning only. For this purpose, the original method, which had been developed for 99mTc-HDP (13), was modified by introducing an additional background ROI to correct bremsstrahlung caused by the β-particles of 186Re or 153Sm. Without such a correction in several cases for both 186Re-HEDP and 153Sm-EDTMP, results were obtained that did not make sense: a higher urinary excretion rate, for example, was found at 3 h than at 24 h. After correction for bremsstrahlung, these contradictory results were no longer observed. A large and rectangular ROI adjacent to the patient’s head and shoulders performed well, although we cannot prove that such an ROI is the best of all possibilities: the differences for various sizes and positions of ROI were small and thus not significant, and no gold standard was available with which to compare pure bone uptake and soft-tissue retention. However, because of this modification, scintigraphic three-phase whole-body imaging using conventional ROI techniques made possible the calculation of kinetic data for the compartments assumed in this model, that is, bone, soft tissue, and urinary excretion.
As already proven for 99mTc-HDP (13,14), the results for 186Re-HEDP and 153Sm-EDTMP are in line with data from the literature. The mean urinary excretion rate of 186Re-HEDP after 24 h was 65.3% ± 12.8% of the initial total whole-body activity. In comparison, de Klerk et al. (17) found a total urinary excretion of 69% ± 15%. For 153Sm-EDTMP, we could show rapid urinary excretion of the radiopharmaceutical: 32.3% within 3 h, increasing to 39.5% at 24 h. These data are in accordance with published results showing mean excretion rates of approximately 37% measured by cumulative urine sampling (5,18,19). However, in a few patients we observed inconsistent data. In patient 9, for example (Table 1), a bone uptake of only 3.4% was calculated at 3 h after injection. Although images of this patient were of poor quality at 3 h after injection, with a low ratio of bone to soft tissue, and improved up to 24 h after injection, we are not sure whether this uptake value reflects individual differences in tracer kinetics or methodologic problems caused by our simplified compartment model. Underestimation of bone uptake may be especially possible in patients with high soft-tissue activity and high background activity. Therefore, our future studies will include measurement of urinary excretion by simple cumulative urine sampling to prove the calculated excretion data. Nevertheless, after modification for 186Re-HEDP and 153Sm-EDTMP, the new method has, in comparison with data from the literature, proven reliable as a quantification tool.
The new aspect of this method, however, is the possibility of separately measuring bone uptake and soft-tissue retention in contrast to measuring whole-body retention. As first indicated by Smith et al. (12), the overall ratio of bone to soft tissue is approximately 2.5:1 for 99mTc-HEDP. This ratio results in a significantly lower bone uptake as measured by 24-h whole-body retention. Similar findings were obtained for 99mTc-HDP, yielding a soft-tissue retention of 13.5% ± 6.2% at 24 h after injection using our quantification method (13) and using a whole-skeleton ROI as recently published (20–22). As expected, the same pharmacokinetic pattern could be proven for the 186Re- or 153Sm-labeled phosphonates. Both compounds showed a mean soft-tissue retention of approximately 13% of the initial whole-body activity, whereas bone uptake was approximately 22% for 186Re-HEDP and 48% for 153Sm-EDTMP at 24 h after injection.
Thus, skeletal uptake of 186Re-HEDP and 153Sm-EDTMP is lower than calculated with standard whole-body retention methods applied so far. This finding may be one reason for the discrepancy between the relatively mild myelotoxicity observed in clinical studies and the estimated high bone marrow dose (18,19,23–25). Eary et al. (19), for example, calculated skeletal doses for 153Sm-EDTMP from whole-body retention assuming skeletal retention to be the inverse of urinary clearance. The overestimation of bone uptake because of this assumption (62% vs. 48% in our study) seems to be a reason for the unexpectedly mild myelotoxicity observed in that study besides the given explanation, which is based on the microscopic anatomy of bone and bone marrow.
In a comparison of the biodistribution data for both radiopharmaceuticals, the mean bone uptake for 153Sm-EDTMP was more than twice that for 186Re-HEDP, whereas the remaining nonskeletal body activities were in the same range after 24 h (Fig. 2). Although the fact that different patient populations were studied for the two radiopharmaceuticals may be one reason for the different bone uptake values for 153Sm-EDTMP and 186Re-HEDP, the patient subsets had a comparable extent of bone metastases and a similar age and sex distribution (Tables 1 and 2). Thus, the higher bone uptake values for 153Sm-EDTMP seem to be related to a different biodistribution for the two tracers. Furthermore, soft-tissue clearance was more rapid in patients treated with 153Sm-EDTMP, with a remainder activity of 38% at 3 h compared with 49% for 186Re-HEDP. From 3 to 24 h after injection, the soft-tissue activity of 186Re-HEDP decreased in accord with a steadily increasing urinary excretion rate, whereas renal clearance for 153Sm-EDTMP was less than 20% of the total activity excreted, with most of the soft-tissue activity shifting to the bones.
Thereby, no significant correlation between soft-tissue retention and the extent of bone metastases could be shown for either radiopharmaceutical, as would be expected for patients with a normal creatinine clearance. For bone uptake, however, a positive linear correlation with the number and extent of bone metastases was observed: for 153Sm-EDTMP, for example, a mean bone uptake of 38% was found at 24 h after injection in patients with fewer than 10 bone metastases, whereas the mean bone uptake value increased to 54% in patients with more than 50 metastases. A similar correlation was observed for 186Re-HEDP.
The mean bone uptake values of 186Re-HEDP and 153Sm-EDTMP may also explain, in part, the different response rates for bone pain reduction reported in the literature. In large clinical trials, significant pain reduction was observed in 54%–70% of the patients receiving 186Re-HEDP (26–28). A somewhat higher response rate, ranging from 65% to 80%, was found for patients who had undergone bone pain palliation therapy with 153Sm-EDTMP (4–6,18). Besides differences caused by radionuclide characteristics such as the energy and range of the β-particles and parameters such as the administered total activity (18,19), the more than twofold higher bone uptake of 153Sm-EDTMP may be an additional reason for the higher response rate of this radiopharmaceutical. Studies are needed that aim at a curative effect for bone therapy, as suggested by Bruland et al. (29) for primary bone tumors or for regimens combining radionuclide bone therapy with chemotherapy or stem cell transplantation (30,31). These future studies should clarify whether the higher bone uptake of 153Sm-EDTMP and, thus, a potentially higher local radiation dosage will result in higher therapeutic efficacy or whether different parameters will significantly affect patient outcome.
CONCLUSION
This article has introduced a new, easy method for quantitative measurement of bone uptake and soft-tissue retention of 186Re-HEDP and 153Sm-EDTMP based on conventional whole-body scintigraphy. The results for whole-body retention (bone uptake plus soft-tissue retention) at 24 h after injection obtained with this method agree well with published findings for conventional 24-h whole-body retention measurement, which is regarded as the standard method for assessing skeletal metabolism of these radiopharmaceuticals. However, by this new quantification method, bone uptake and soft-tissue retention can be calculated separately, thus providing more detailed kinetic data. These may improve dosimetry for 186Re-HEDP and 153Sm-EDTMP in, for example, assessment of radiation dosage to bone and bone marrow. Furthermore, significant differences in the biodistribution of both radiopharmaceuticals were shown.
Footnotes
Received Jun. 12, 2000; revision accepted Sep. 14, 2000.
For correspondence or reprints contact: Winfried Brenner, MD, Christian-Albrechts-Universität, Klinlk für Nuklearmedizin, Arnold-Heller-Strasse 9, D-24105 Kiel, Germany.
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Gemcitabine Radiosensitization after High-Dose Samarium for Osteoblastic Osteosarcoma
- A Paired-Image Radiation Transport Model for Skeletal Dosimetry
- Bone Uptake Studies in Rabbits Before and After High-Dose Treatment with 153Sm-EDTMP or 186Re-HEDP
- High-Dose Treatment with 186Re-HEDP or 153Sm-EDTMP Combined with Amifostine in a Rabbit Model