


Abstract
The aim of this experimental study was to investigate the myeloprotective potential of amifostine in rabbits receiving high-dose treatment with either 153Sm-ethylenediaminetetramethylene phosphonate (EDTMP) or 186Re-hydroxyethylidene diphosphonate (HEDP) and to check for drug interactions impairing the skeletal uptake of these radiopharmaceuticals by amifostine. Methods: To a total of 24 rabbits, we administered 1,000 MBq of either 153Sm-EDTMP (n = 12) or 186Re-HEDP (n = 12). Six animals of each group received 500 mg amifostine intravenously 10–15 min before injection of the radiopharmaceutical, whereas the other 6 animals served as controls. Up to 8 wk after treatment, blood samples were collected every 3–5 d to measure platelet and leukocyte counts. Furthermore, whole-body images were acquired at 3 min, 3 h, and 24 h after injection of the radiopharmaceutical to quantify the skeletal uptake. Results: For 186Re-HEDP, the mean decrease in platelets was significantly less in the amifostine group (35.5% ± 2.4%) than in the control group (61.3% ± 5.4%, P < 0.001). Similar results were found for 153Sm-EDTMP (36.5% ± 8.3% vs. 52.3% ± 14.0%, P < 0.05). No significant differences in leukocyte counts were found for 186Re-HEDP (75.3% ± 12.3% in the amifostine group and 72.5% ± 4.1% in the control group, P > 0.05), whereas rabbits treated with 153Sm-EDTMP plus amifostine showed a significantly greater decrease in leukocytes (69.2% ± 10.8%) than did the control group (56.6% ± 4.0%, P < 0.05). Bone uptake in percentage of initial total whole-body activity was significantly decreased in animals treated with amifostine compared with the control groups for both 186Re-HEDP (15.8% ± 3.1% vs. 30.9% ± 1.9%, P < 0.001) and 153Sm-EDTMP (31.7% ± 8.9% vs. 44.0% ± 6.5%, P < 0.05). Conclusion: For amifostine, we found a highly significant cytoprotective effect on platelets but no leukoprotective effect. The latter probably relies on the intrinsic myelotoxicity of high-dose amifostine, which seemed to potentiate the leukodepression of the radiopharmaceuticals. The lower bone uptake in amifostine-treated animals may be caused by the chemical structure of amifostine, which is a potentially complex-forming compound that may be able to displace bisphosphonates from the rhenium– and samarium–bisphosphonate complexes, resulting in altered biodistribution patterns.
- amifostine
- myeloprotection
- 186Re-hydroxyethylidene diphosphonate
- 153Sm-ethylenediaminetetramethylene phosphonate
- skeletal uptake
Treatment with 186Re-hydroxyethylidene diphosphonate (HEDP) or 153Sm-ethylenediaminetetramethylene phosphonate (EDTMP) has been proven safe and successful for palliation of bone pain in patients with widespread osseous metastases (1–6). The major side effect of this therapy is a drop in the number of platelets and leukocytes in the peripheral blood (3,7) caused by irradiation of stem cells in the bone marrow by the β-particles of the bone-seeking radiopharmaceutical. Myelotoxicity is therefore a therapy-limiting factor in patients with extended osseous disease: these patients are often affected a priori by disease-associated myelodepression, and increased skeletal uptake because of widespread bone metastases (8) is a main determinant of radiation damage to bone marrow. Thus, improvement of radionuclide therapy of bone pain through minimization of myelotoxic side effects seems essential.
For the radical scavenger amifostine, an organic thiophosphonate, cytoprotection of the salivary glands against radiation damage has been reported for patients with head and neck cancer undergoing external radiation therapy (9,10) and patients with differentiated thyroid cancer receiving high-dose radioiodine treatment (11,12). Furthermore, amifostine has been approved in Europe for myeloprotection of patients with ovarian cancer scheduled for chemotherapy with cyclophosphamide and cisplatin (13). Because both the therapeutic effects and the side effects of external radiotherapy, chemotherapy with alkylating agents, and radionuclide therapy are produced through generation of free radicals, an evaluation of the cytoprotective effect of amifostine on bone marrow cells during radionuclide bone pain therapy with β-emitter–labeled bisphosphonates such as 153Sm-EDTMP and 186Re-HEDP seemed worthwhile. However, apart from evaluation of the myeloprotective effects of amifostine, documentation of any drug interactions between amifostine and radiolabeled bisphosphonates that might impair bone uptake of these radiopharmaceuticals would be of particular interest because of the possibility that amifostine may alter renal drug clearance (14) and bone metabolism (15,16).
The aim of this experimental study, therefore, was to investigate the myeloprotective potential of amifostine in rabbits receiving high-dose treatment with either 153Sm-EDTMP or 186Re-HEDP and to determine whether any drug interactions with amifostine were impairing skeletal uptake of the radiopharmaceuticals.
MATERIALS AND METHODS
Animals and Study Design
The studies were performed on 24 female New Zealand White rabbits (age range, 10–12 wk; mean weight ± SD, 2.5 ± 0.2 kg; Charles River, Kissleg, Germany). For radionuclide bone therapy, we used 186Re-HEDP (Mallinckrodt, Petten, The Netherlands) and 153Sm-EDTMP (CIS, Gif-Sur-Yvette, France). A standard activity of 1,000 MBq of either 153Sm-EDTMP (n = 12) or 186Re-HEDP (n = 12) was administered intravenously according to a dose of 400 MBq/kg of body weight. As suggested from patient studies with amifostine, all animals received 4 mg dexamethasone (Fortecortin; Merck, Darmstadt, Germany) as an antiemetic treatment 20–30 min before the administration of the radiopharmaceutical. In both animal groups, 153Sm-EDTMP and 186Re-HEDP, the rabbits were divided into 2 subgroups: 6 animals from each group received 500 mg (200 mg/kg of body weight) of amifostine (i.e., ethanethiol, or 2-[(3-aminopropyl)amino]-, dihydrogen phosphate [ester]) (Ethyol; Essex, Munich, Germany) as a 5-min intravenous infusion 10–15 min before injection of the radiopharmaceutical, and 6 rabbits from each group served as controls. This administration procedure was found effective, with no major side effects, for radioprotection in rabbits (17). Furthermore, the standard dose of 500 mg amifostine with 4 mg dexamethasone was administered without any further treatment to 4 additional animals, which served as negative controls with regard to the radiopharmaceuticals. The animal studies were approved by Ministerium für Umwelt, Natur und Forsten des Landes Schleswig-Holstein (X 252-72241.121-17 56-8/98).
The myeloprotective effects of amifostine were investigated by collecting blood samples before therapy and then every 3–5 d until ≤8 wk after radionuclide treatment to measure platelet and leukocyte counts. Furthermore, quantitative bone scanning was performed to assess whether amifostine was interfering with 153Sm-EDTMP or 186Re-HEDP.
Scintigraphic Skeletal Uptake Measurement
Whole-body images from anterior and posterior views were acquired simultaneously at 3 min, 3 h, and 24 h after a bolus injection of the respective radiopharmaceutical. The acquisition time was 1 min during the blood-pool phase and 10 min for the later images. Images were obtained under the same conditions for each rabbit, using a double-head gamma camera (Bodyscan; Siemens, Erlangen, Germany) equipped with high-resolution low-energy collimators. The energy window used was 137 keV ± 15% for 186Re and 103 keV ± 15% for 153Sm.
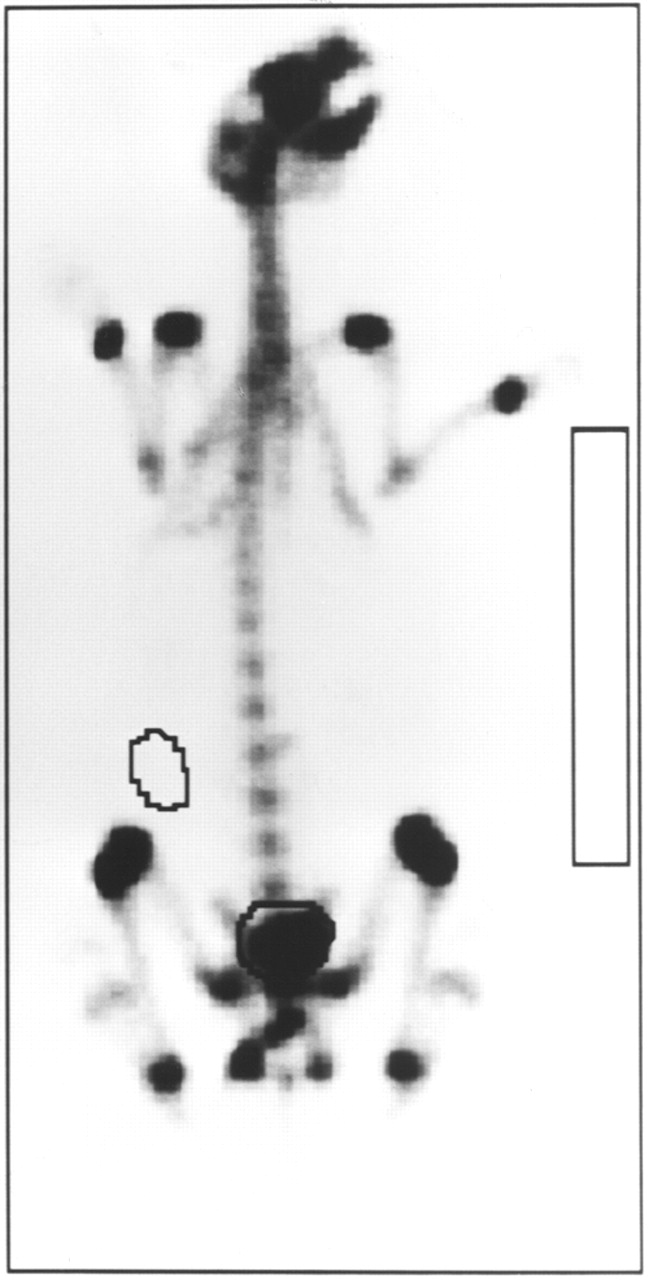
For each image, activity in the whole body, urinary bladder, and soft tissue of the flank was measured by region-of-interest (ROI) technique using both anterior and posterior views. Additionally, a rectangular ROI adjacent to the body was used to measure the bremsstrahlung of the β-particles of the radionuclide. An example of ROI positions is shown in Figure 1. From these data, the geometric mean for each ROI was calculated after correction for different acquisition times, radioactive decay, and bremsstrahlung. The initial whole-body activity of each rabbit was used as the reference value for further calculations of activity data, which are all given as a percentage of the whole-body activity. According to a simplified 3-compartment model, soft-tissue activity compared with initial whole-body activity equals activity in muscles compared with initial muscle activity at 3 min after injection. Urinary excretion was determined by the difference in whole-body activity between the reference image at 3 min and the image of interest plus urinary bladder activity. From these data, bone uptake at 24 h after injection was calculated as 100% of initial whole-body activity minus both urinary excretion and soft-tissue retention, as has been described in detail elsewhere (8).
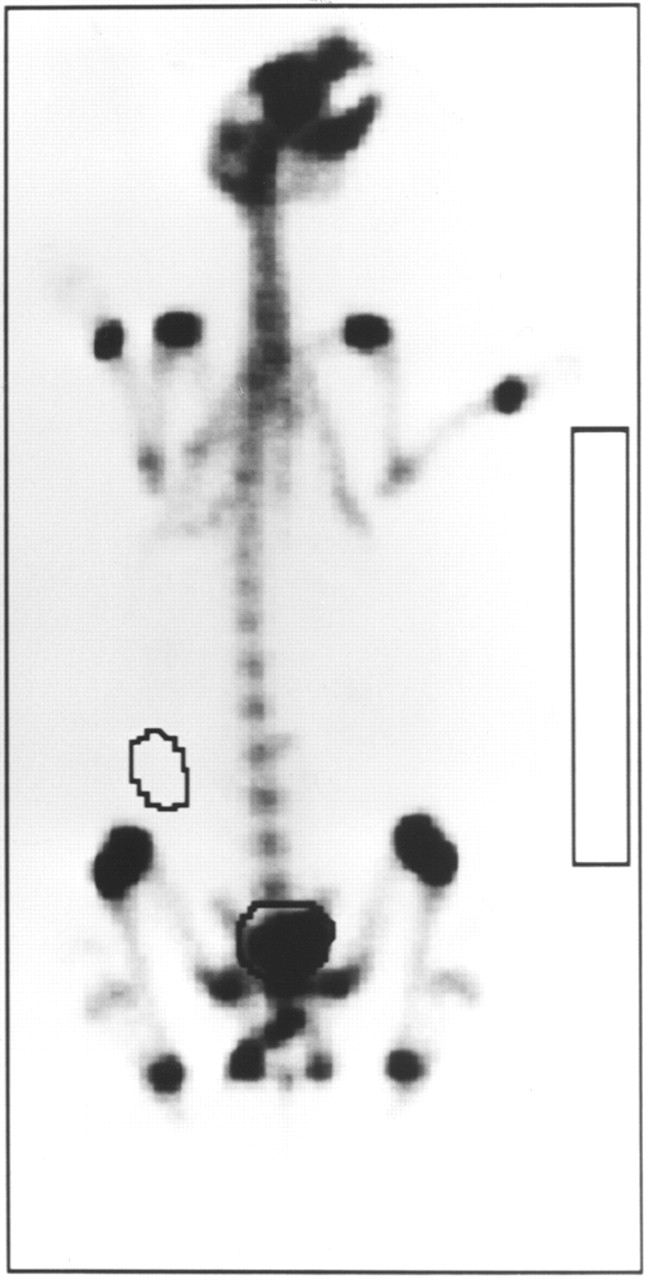
ROI positions on whole-body scintigram of rabbit from posterior view 3 h after injection of 1,000 MBq 153Sm-EDTMP.
Statistics
Data are given as mean ± 1 SD. A 2-tailed Student t test for unpaired data (including both the F test and the test of David, Pearson, and Stephens to prove normal distribution of the data) was used to evaluate the significance of differences between rabbit subgroups, with P < 0.05 considered to be statistically significant (18).
RESULTS
Platelets and Leukocytes
In rabbits treated with 1,000 MBq 186Re-HEDP plus amifostine (ReA; n = 6), the mean pretherapeutic platelet counts were 316 ± 14/nL. Platelet counts reached a mean nadir of 201 ± 11/nL after 11 ± 3 d, corresponding to a mean decrease of 35.5% ± 2.4%. In the control group, which was treated with 1,000 MBq 186Re-HEDP alone (ReC; n = 6), pretherapeutic platelet counts of 342 ± 28/nL decreased to 134 ± 29/nL after 13 ± 2 d, corresponding to a decrease of 61.3% ± 5.4% (Table 1). Thus, the mean decrease in platelets was significantly greater in ReC than in ReA (P < 0.001), whereas the intervals of the nadir were not different (P > 0.05). The corresponding data for the pretherapeutic leukocyte counts were 5.2 ± 1.4/nL for ReA and 5.4 ± 1.4/nL for ReC (Table 1). The respective nadirs were reached after 7 ± 1 d and 6 ± 0 d (P > 0.05), with a mean decrease in leukocytes to 1.3 ± 0.6/nL for ReA (75.3% ± 12.3%) and 1.5 ± 0.2/nL for ReC (72.5% ± 4.1%). Thus, the decrease in leukocytes did not significantly differ between the 2 subgroups (P > 0.05).
Decrease in Platelet and Leukocyte Counts After Treatment with 186Re-HEDP
In rabbits treated with 1,000 MBq 153Sm-EDTMP plus amifostine (SmA; n = 6), the mean pretherapeutic platelet counts were 269 ± 33/nL. A mean nadir of 169 ± 17/nL was reached after 24 ± 2 d, corresponding to a mean decrease of 36.5% ± 8.3%. In the control group, which was treated with 1,000 MBq 153Sm-EDTMP alone (SmC; n = 6), pretherapeutic platelet counts of 270 ± 36/nL decreased to 125 ± 21/nL after 27 ± 3 d, corresponding to a decrease of 52.3% ± 14.0%, which was significantly greater than the decrease for the SmA group (P < 0.05) (Table 2), with no difference between the intervals of the nadir. The corresponding data for the pretherapeutic leukocyte counts were 5.4 ± 1.0/nL for SmA and 6.1 ± 1.3/nL for SmC (Table 2). The respective nadirs were reached after 7 ± 3 d and 10 ± 4 d (P > 0.05): 1.6 ± 0.3/nL for SmA (69.2% ± 10.8%) and 2.6 ± 0.6/nL for SmC (56.6% ± 4.0%). Thus, the decrease was significantly greater (P < 0.05) for the amifostine group.
Decrease in Platelet and Leukocyte Counts After Treatment with 153Sm-EDTMP
Comparing the intervals between administration of the radiopharmaceutical and the nadir, we found no significant differences in leukocyte counts between 186Re-HEDP and 153Sm-EDTMP (6 ± 0 d for ReC and 10 ± 4 d for SmC, P > 0.05), whereas the nadir of the platelet counts was reached significantly earlier in rabbits treated with 186Re-HEDP (13 ± 2 d for ReC and 27 ± 3 d for SmC, P < 0.001). However, both the leukocyte counts and the platelet counts recovered completely, reaching the initial values 6 wk after treatment with 186Re-HEDP either with or without amifostine. The same recovery time, 6 wk, was observed for both the leukocyte counts and the platelet counts of SmA and SmC after treatment with 153Sm-EDTMP. Thus, for both radiopharmaceuticals, the recovery times of rabbits treated with amifostine did not differ from those of rabbits treated without it.
In 4 animals that served as negative controls with regard to radiopharmaceuticals, that is, animals treated with amifostine and dexamethasone only, both the leukocyte counts and the platelet counts showed no changes up to 5 wk after injection. Thus, no myelotoxic effects from use of amifostine in combination with dexamethasone were found by simple blood cell counting.
Skeletal Uptake of 186Re-HEDP and 153Sm-EDTMP
In rabbits receiving ReA (n = 6), the mean bone uptake at 24 h after injection was 15.8% ± 3.1%. For the control group (ReC; n = 6), uptake of 30.9% ± 1.9% was obtained at 24 h after injection, and this value was significantly higher (P < 0.001) than that for the amifostine group. Although the remainder soft-tissue activity at 24 h after injection was not significantly different between the groups (ReA, 14.8% ± 3.2%; ReC, 14.0% ± 2.7%), urinary excretion was significantly increased in rabbits treated with amifostine (ReA, 69.4% ± 2.5%; ReC, 55.1% ± 3.8%; P < 0.001).
For 153Sm-EDTMP in combination with amifostine (SmA; n = 6), the mean bone uptake at 24 h after injection was 31.7% ± 8.9%, whereas in the control group a mean uptake value of 44.0% ± 6.5% at 24 h after injection was found, showing a significant difference from the amifostine group (P < 0.05). On the other hand, the 18.4% ± 7.0% remainder soft-tissue activity found in animals treated with amifostine was significantly higher (P < 0.05) than the 9.8% ± 4.4% found in control animals. The mean urinary excretion rate was similar for both groups: 49.9% ± 11.8% and 46.3% ± 7.5% in rabbits treated with amifostine and without amifostine, respectively.
Significantly higher bone uptake at 24 h after injection was found for 153Sm-EDTMP than for 186Re-HEDP for both the animals treated with amifostine (P < 0.01) and the control animals (P < 0.001), whereas the remainder soft-tissue activity was in the same range for SmA and ReA and for SmC and ReC (P > 0.05 for each).
DISCUSSION
The cytoprotective potential of thiol-containing compounds against radiation damage has been known for many years (19). Amifostine was selected from >4,000 of such compounds as the agent with the best clinical profile. In animal studies, amifostine protected normal tissues such as bone marrow, salivary glands, skin, and oral mucosa from the toxic effects of lethal doses of ionizing radiation, with no impact on malignant transformed cells (20,21). The mechanism of this selective radioprotection of amifostine has been shown to be related to its preferential rapid uptake into normal tissues and no or only slow uptake into tumor cells. This selectivity results mainly from differences in the presence of alkaline phosphatase at capillary endothelial cells and the pH of normal tissues compared with the pH of tumor tissue. These conditions favor the dephosphorylation of amifostine by the membrane-bound alkaline phosphatase to its active metabolite, the free thiol WR-1065 (Fig. 2), which immediately enters normal tissues (22). Once inside the cell, WR-1065 acts as a scavenger of oxygen free radicals by detoxifying these radicals before they can damage the DNA or RNA (23). After intravenous injection, amifostine is rapidly cleared from the plasma, with half-lives of <1 min and <8 min (23). In contrast to the brief systemic half-life, retention of amifostine and its metabolites in normal tissue is prolonged. During the first 30 min after administration, uptake into normal tissues such as salivary glands, kidneys, liver, and bone marrow has been shown to be >100-fold higher than uptake into tumor tissue, with intracellular retention up to 24 h after injection (24). As a result of these experimental findings, numerous clinical studies have been performed and have shown amifostine to be a potent cyto- and myeloprotective agent in patients undergoing chemotherapy or radiation therapy (16,25,26). Consequently, amifostine has gained drug approval in the United States and in Europe (13,27).
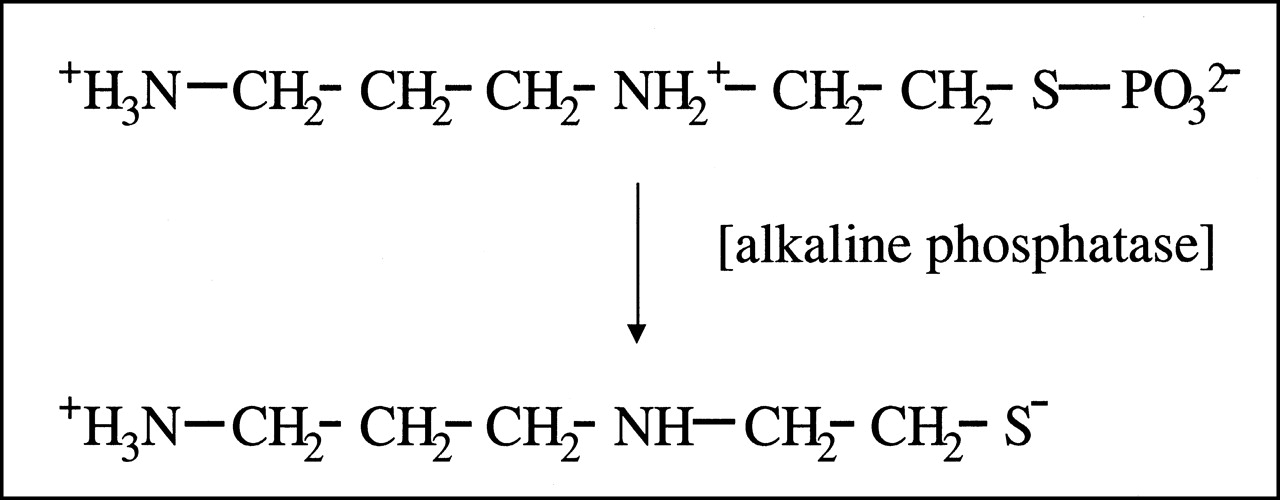
Chemical structure of amifostine and its active metabolite, the free thiol WR-1065.
In this rabbit animal model, amifostine was found to have a significant cytoprotective effect on platelets both in rabbits treated with 186Re-HEDP and in rabbits treated with 153Sm-EDTMP, and this finding is in line with the well-documented myeloprotective effects in radiation therapy (10,16,20,25,27). Of special interest is the finding that a single administration of amifostine 10–15 min before the radionuclide treatment could clearly reduce cytotoxic effects on platelets despite the somewhat long radiation exposure of bone marrow cells caused by the radiopharmaceuticals affixed to the bone matrix, with physical half-lives of 90.6 and 46.7 h for 186Re-HEDP and 153Sm-EDTMP, respectively. This observation, however, is in line with reports that single amifostine administrations have a cytoprotective effect on salivary glands during high-dose radioiodine treatment (12,28).
Completely different findings were obtained for leukocytes: Whereas for 186Re-HEDP no significant differences could be found between amifostine-treated animals and control animals, the rabbits treated with SmA showed a significantly greater decrease in leukocytes than did animals treated with 153Sm-EDTMP only. On the other hand, treatment with amifostine alone, without any radionuclide administration, showed no changes in leukocyte counts. These data indicate increased cytotoxic effects on leukocytes for the combination of 153Sm-EDTMP and amifostine compared with the other subgroups in this study. Klutmann et al. (29) found similar leukotoxic effects in 9 rabbits after administration of 200 mg amifostine per kilogram of body weight in combination with 400 MBq 186Re-HEDP: in amifostine-treated animals, leukocyte counts decreased from 5.7 ± 2.1/nL to 3.4 ± 0.9/nL, corresponding to a mean decrease of approximately 40%, whereas the control animals showed somewhat constant values. The difference between the 2 groups was reported to be highly significant, with P < 0.002. The authors therefore concluded that a selective cytotoxic effect on leukocytes has to be discussed for amifostine in combination with 186Re-HEDP. Although we could not document a significant effect for amifostine in combination with 186Re-HEDP, we did show similar results for amifostine in combination with 153Sm-EDTMP. The myelotoxicity of high-dose amifostine is known, and lymphopenia and a corresponding decrease in total white blood cells caused by amifostine in both rats and dogs has been reported for the dosage administered in this study, that is, 200 mg/kg of body weight (30). For platelets, only a moderate decrease has been observed (30). Nevertheless, in this study we found neither leukotoxic nor platelet-toxic effects in rabbits when we administered amifostine alone in a dosage of 200 mg/kg of body weight. The same dosage had been used successfully in rabbits undergoing high-dose radioiodine therapy in previous studies (17,28). Thus, the myelotoxic effects of high-dose amifostine, although not detectable through measurement of platelet and leukocyte counts in blood, seemed to potentiate the myelotoxic effects of β-emitter–labeled bisphosphonates. However, in contrast to Klutmann et al., we found such an additive leukotoxic effect only for 153Sm-EDTMP, not for 186Re-HEDP, possibly because of a statistical problem caused by the small number of animals. Summarizing all these observations, we conclude that in rabbits, a dosage of 200 mg amifostine per kilogram of body weight is close to but below the threshold of measurable leukotoxic effects, which may become detectable during combined treatment with amifostine and myelotoxic drugs such as 153Sm-EDTMP or 186Re-HEDP. Therefore, for further studies in rabbits, the dosage of amifostine should be reduced if white blood cell counts are part of the study design. To our knowledge, however, there are no other reports on the use of amifostine in radionuclide bone therapy that might support our conclusions or explain the underlying mechanisms in more detail.
Our study used a recently introduced quantification method based on whole-body bone scanning to measure skeletal uptake, soft-tissue retention, and urinary excretion of radiolabeled bisphosphonates (8,31) and, thus, document drug interactions with amifostine. This step seemed necessary because of the known possibility that amifostine may alter renal drug clearance (14) and bone metabolism (15,16). For 186Re-HEDP, bone uptake at 24 h after injection was significantly lower in animals treated with amifostine than in control animals. The remainder soft-tissue activity at 24 h after injection was the same in amifostine-treated rabbits as in control animals, suggesting that the higher amount of nonskeletal bound activity was completely excreted by the kidneys. For 153Sm-EDTMP also, significantly reduced bone uptake was found in amifostine-treated animals. However, in these rabbits the main observation was a shift in activity toward the soft-tissue compartment, whereas urinary excretion was nearly the same for both amifostine-treated animals and untreated animals. Because amifostine can alter bone metabolism through both parathyroid hormone–independent and parathyroid hormone–dependent mechanisms, resulting in hypocalcemia and an inhibition of osteoclastic bone resorption (15,16,32), the reduced bone uptake of 186Re-HEDP and 153Sm-EDTMP after administration of amifostine might be explained by subsequent reduction of osteoblastic activity in response to transient osteoclastic inhibition. However, this hypothesis would not explain the increased remainder soft-tissue activity of 153Sm-EDTMP, because excretion of nonskeletal-bound 153Sm-EDTMP by the kidneys is expected, as shown in patients with bone metastases: the lower the number and extent of bone metastases, the lower was bone uptake and the higher was urinary excretion, whereas constant soft-tissue retention values proved to be independent of the number of metastases (8,33). However, because of the chemical structure of amifostine, it is a potentially chelating agent that presents thiol moieties containing electron-rich coordinating atoms for rhenium or samarium. Thus, amifostine might be able to displace bisphosphonates from their rhenium– and samarium–bisphosphonate complexes, building up new rhenium–amifostine or samarium–amifostine complexes. This hypothesis would explain both the reduced bone uptake of 153Sm and the reduced bone uptake of 186Re, because rhenium– or samarium–amifostine complexes are not expected to have bone affinity, and different biodistribution pattern are caused by the different biochemical characteristics of amifostine–samarium and amifostine–rhenium complexes. Because the plasma half-life of amifostine is only about 8 min, administration of the radiolabeled bisphosphonates as late as 30 min after the infusion of amifostine might be helpful to ensure almost complete intracellular uptake of amifostine and its metabolites and to reduce the possible formation of rhenium– or samarium–amifostine complexes. Furthermore, amifostine cannot, at this point in its investigation, be recommended for general use in patients undergoing radionuclide therapy of painful bony metastases, because the lower uptake in the skeleton may reduce the efficacy of this treatment modality.
CONCLUSION
In rabbits undergoing high-dose treatment with 1,000 MBq of either 186Re-HEDP or 153Sm-EDTMP, we found amifostine to have a highly significant cytoprotective effect on platelets. However, no leukoprotection was found, and even leukotoxicity was shown for the combination of amifostine and 153Sm-EDTMP. This effect most probably relies on the intrinsic myelotoxicity of high-dose amifostine, which seemed to potentiate radiopharmaceutical-induced myelodepression. These findings suggest the use of lower doses of amifostine in rabbits. Furthermore, significantly reduced bone uptake of 186Re-HEDP and 153Sm-EDTMP was found in amifostine-treated animals. Amifostine, because of its potential to form complexes, may be able to displace bisphosphonates from the rhenium– and samarium–bisphosphonate complexes, resulting in reduced bone uptake and an altered biodistribution pattern.
Acknowledgments
The authors thank Dr. Hans-Ulrich Wottge and his team for providing perfect animal care service. This study was supported by Mallinckrodt GmbH, Hennef, Germany, and was presented in part at the annual meeting of the Society of Nuclear Medicine, St. Louis, MO, June 3–7, 2000. To express their great esteem, the authors dedicate this study to Prof. Dr. Willi Ernst Adam.
Footnotes
Received Jan. 29, 2001; revision accepted May 29, 2001.
For correspondence or reprints contact: Winfried Brenner, MD, Christian-Albrechts-Universität, Arnold-Heller-Strasse 9, D-24105 Kiel, Germany.
REFERENCES
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.