


Abstract
The purpose of this study was to evaluate the feasibility of using 18F-FDG and PET for the detection of infection associated with lower limb arthroplasty. Methods: Seventy-four prostheses in 62 patients in whom infection was suspected after artificial hip or knee placement were studied with this technique. Images were obtained 60 min after an intravenous injection of FDG. The images were interpreted as positive for infection if tracer uptake was increased at the bone–prosthesis interface. A final diagnosis was made by surgical exploration or clinical follow-up for 1 y. PET results were compared with the follow-up outcome in all patients. Results: The sensitivity, specificity, and accuracy of PET for detecting infection associated with knee prostheses were 90.9%, 72.0%, and 77.8%, respectively. The sensitivity, specificity, and accuracy of PET for detecting infection associated with hip prostheses were 90%, 89.3%, and 89.5%, respectively. Overall, the sensitivity was 90.5% and the specificity was 81.1% for detection of lower limb infections. Conclusion: FDG PET is a useful imaging modality for detecting infections associated with lower limb arthroplasty and is more accurate for detecting infections associated with hip prostheses than for detecting infections associated with knee prostheses.
In the past few years, lower limb arthroplasty has become common. The number of patients who are appropriate candidates for this type of surgery is increasing rapidly. The widespread use and dramatic success of prosthetic joint implant surgery has greatly improved the quality of life for many individuals with degenerative, arthritic, or injured joints. In a significant number of cases, however, the patients experience pain at the site of arthroplasty at some point after surgery. The pain can signal biomechanical failure, periprosthetic infection of the joint, or both. Approximately 10% of lower limb arthroplasties need surgical revision because of the pain. Although infection occurs in 1%–4% of original lower limb arthroplasties (1,2), the infection rate can reach more than 30% after revision arthroplasty (2,3). One of the most difficult diagnostic dilemmas in this setting is to distinguish an aseptic from a septic process. Existing preoperative tests for the diagnosis of periprosthetic infection are disappointing because of the relatively high frequency of false-negative results. The cause of a painful prosthesis often remains unclear until after intraoperative culturing and histopathologic examination. In only 25% of patients are infected prostheses accurately diagnosed on the basis of clinical history and physical examination (4). In most patients, multiple tests are required to establish the diagnosis before revision surgery (4). These tests include routine radiography, joint aspiration followed by bacterial culturing, and conventional nuclear medicine studies such as bone scanning, gallium scanning, and indium-labeled white blood cell scanning.
18F-FDG PET has been extensively used in oncology (5). In contrast, reports about the usefulness of FDG PET in detecting infections are still few (6). Because of elevated glycolytic activity, inflammatory cells such as neutrophils and activated macrophages also have increased FDG uptake at the site of inflammation and infection (7–9) and therefore allow visualization of these sites. In this preliminary study, we evaluated the feasibility of the FDG PET approach in 74 lower extremity prostheses with suspected infection. PET results were compared with the final clinical diagnosis, which was based on all available clinical and laboratory data, including all outcome information.
MATERIALS AND METHODS
Patient Population
Sixty-two patients (age range, 27–81 y) with painful lower limb prostheses were studied with FDG PET. All had undergone routine clinical and laboratory studies for the evaluation of painful prostheses, but no clear diagnosis had been established before PET scanning. Three patients underwent PET 3, 7, and 9 mo, respectively, after arthroplasty. For all other patients, the interval between arthroplasty and PET was 1–8 y. A total of 74 prostheses (36 knee prostheses and 38 hip prostheses) were examined with this technique. All patients gave written informed consent for the study.
FDG PET Study
PET scans were acquired using either a PENN PET 240H scanner (UGM ADAC Medical Systems, Inc., Philadelphia, PA) (n = 53) or an EACT HR+ PET camera (Siemens Medical Systems, Iselin, NJ) (n = 21). The patients fasted for at least 4 h before receiving the injection. The images were obtained 60 min after intravenous administration of 4.22–4.56 MBq FDG per kilogram body weight. The areas of interest were imaged with sequential scans of 4–5 min each. The imaging bed moved 6.4 cm axially to provide uniform sensitivity in the entire image set generated. The images were reconstructed using ordered-subset expectation maximization (10), and most images were not corrected for attenuation.
Image Interpretation
Two observers who were unaware of clinical and radiologic information read the studies jointly, and a consensus was reached on the basis of a discussion of each case. When an area of increased uptake was detected in the bone–prosthesis interface for either hip or knee arthroplasty compared with adjacent soft tissue, a diagnosis of infected prosthesis was suggested. If no such increased tracer uptake was noted, infection was considered unlikely. For a hip prosthesis, if the increased tracer uptake was limited to an area around the femoral head or neck portion of the prosthesis but did not extend to the femoral shaft, loosening was considered a likely diagnosis.
Follow-Up
The final diagnosis was made by surgical exploration (43 patients) or clinical follow-up (19 patients) for 1 y. Arthroplasties were considered infected if aspiration cultures grew organisms or if infection was verified at surgery. Arthroplasties were considered uninfected if an operative smear revealed no leukocytes and if intraoperative cultures obtained from suspected sites during surgery revealed no growth. Arthroplasties that did not require surgical exploration during the follow-up period were considered uninfected. Most patients with painful prostheses responded to conservative anti-inflammatory (but not antibiotic) therapy during the follow-up period.
RESULTS
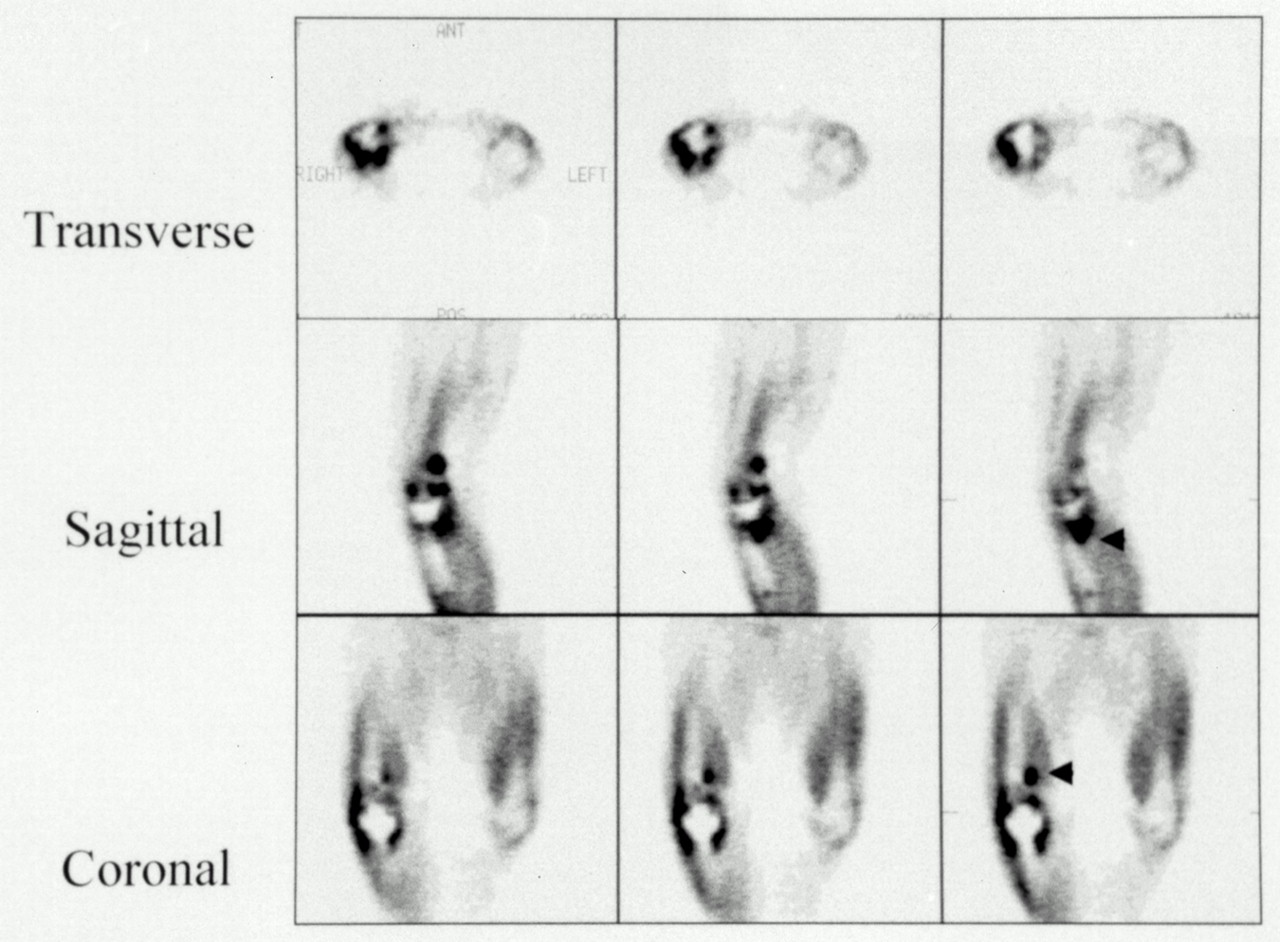
The FDG PET scan correctly revealed 10 of 11 knee prosthesis infections (Fig. 1). However, 7 positive results in 25 knees eventually proved not to be infections. For hip prostheses, the PET scan successfully revealed 9 of 10 hip infections associated with prostheses (Figs. 2A–C) and excluded infection in 25 of 28 without infection (Fig. 3). The sensitivity, specificity, and accuracy of PET for detecting infection associated with knee prostheses were 90.9%, 72.0%, and 77.8%, respectively. The sensitivity, specificity, and accuracy of PET for detecting infection associated with hip prostheses were 90.0%, 89.3%, and 89.5%, respectively. Overall, the sensitivity for the entire population studied was 90.5% and the specificity was 81.1% for detecting infections of lower limb arthroplasties.
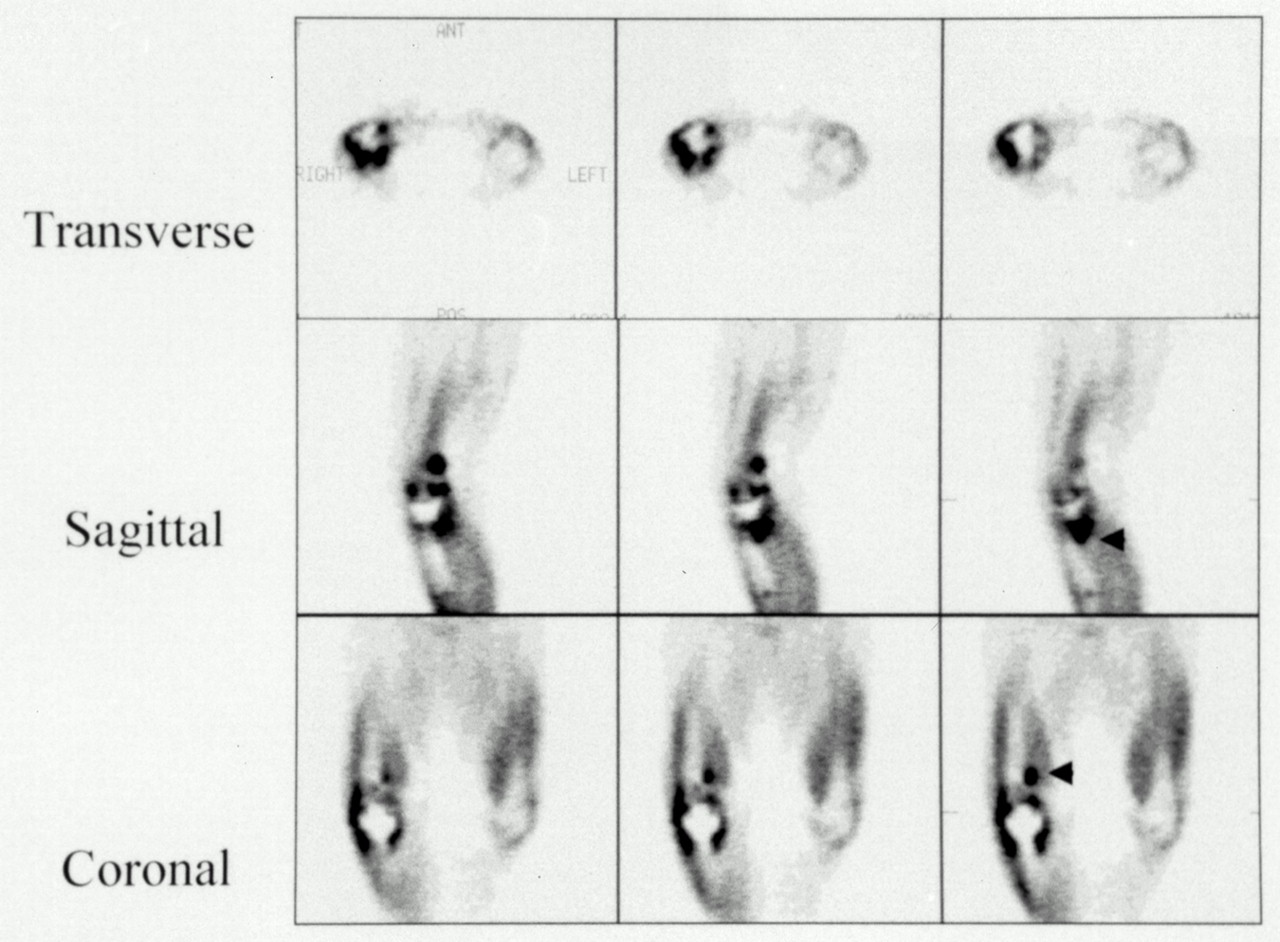
PET images of 60-y-old woman with painful right knee prosthesis proven infected by revision arthroplasty. Bone–prosthesis interface shows areas of intense uptake in both femoral and tibial component of prosthesis (arrowheads).
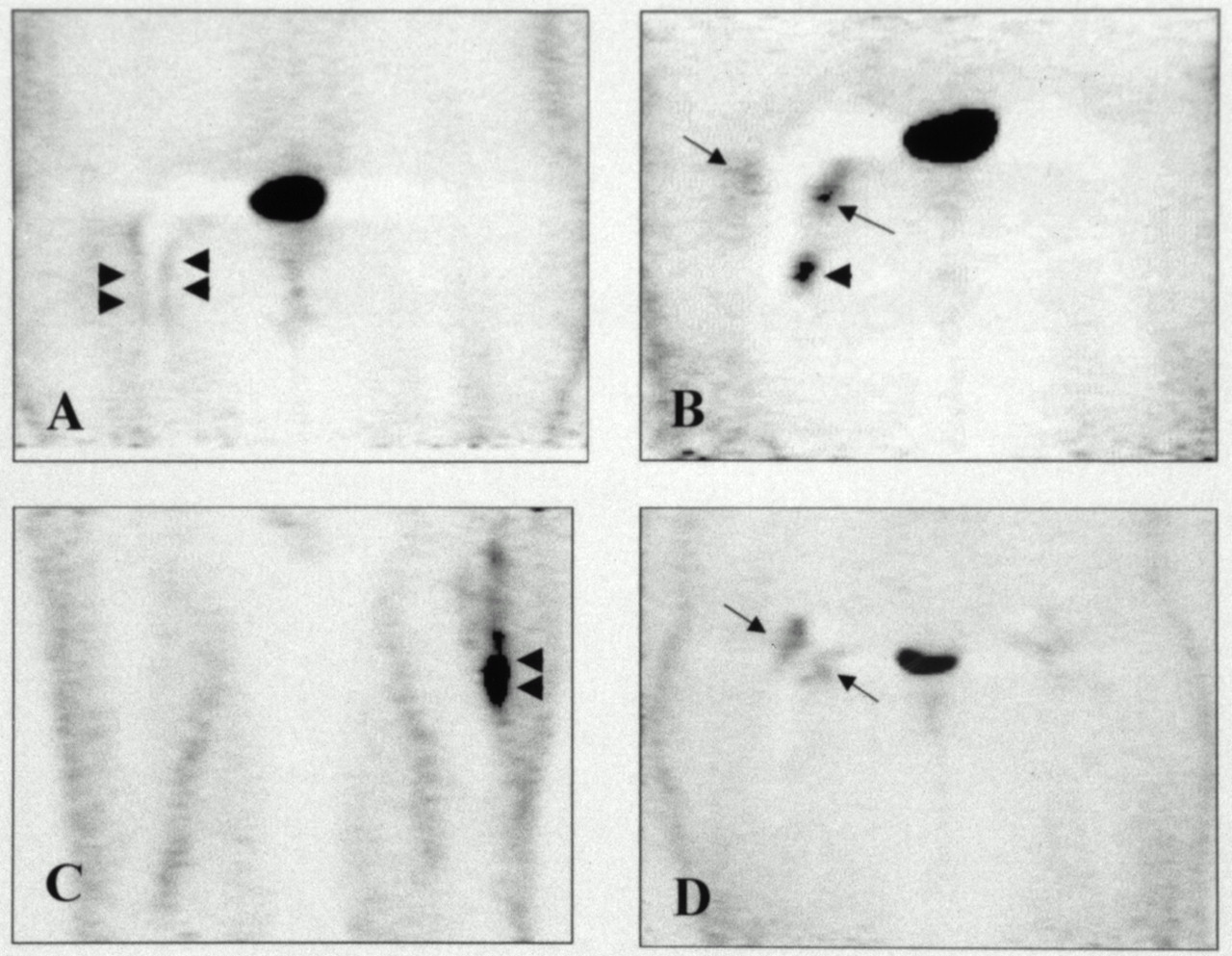
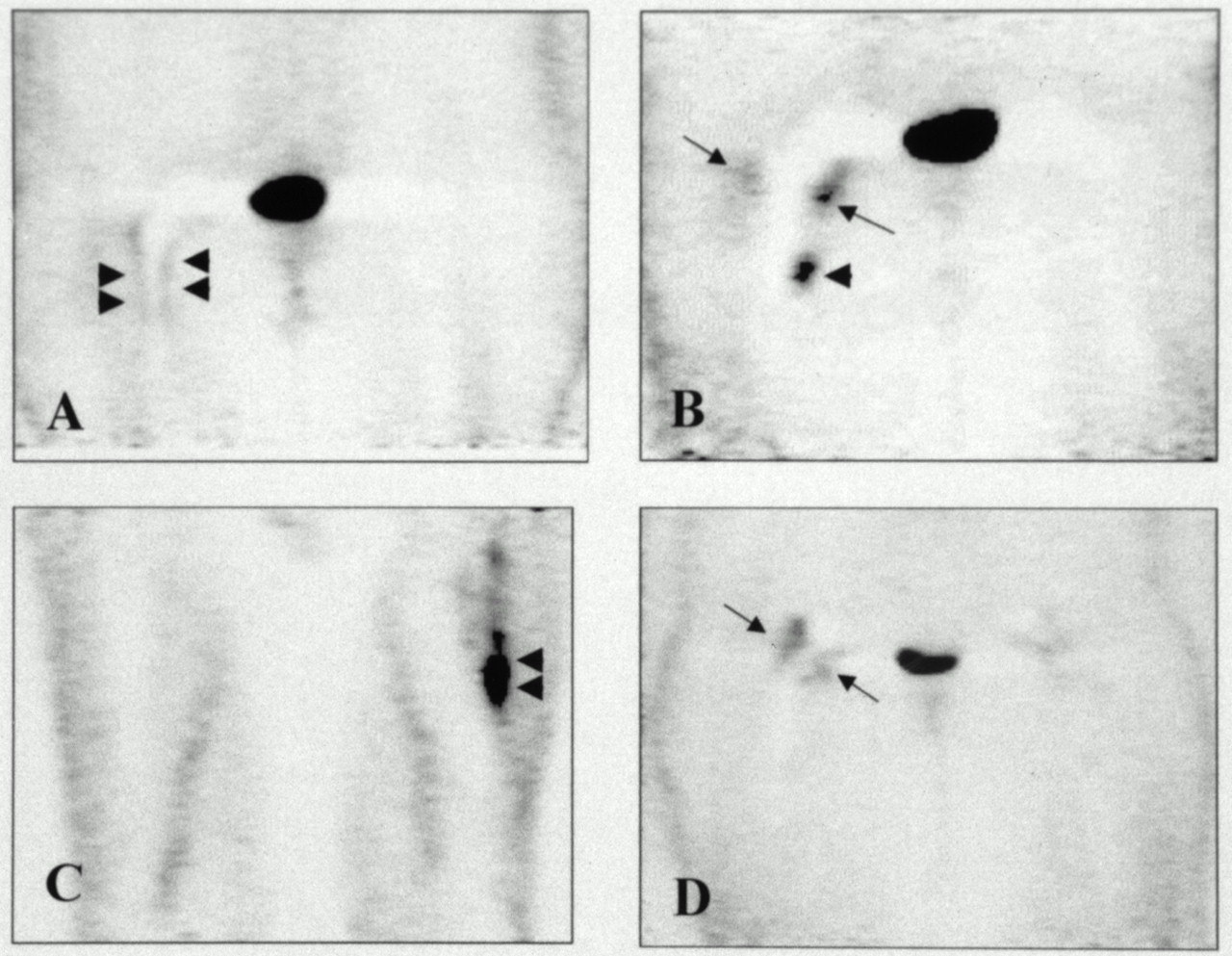
(A) Coronal image of 72-y-old woman with hip prosthesis. Periprosthetic infection on right side was identified (arrowheads). (B) Coronal image of 76-y-old woman with bilateral hip prostheses. Both infection (arrowhead) and loosening (arrows) were shown. (C) Coronal image of 78-y-old man with painful left hip prosthesis. Arrowheads indicate periprosthetic infection and osteomyelitis. (D) Coronal image of 76-y-old woman with bilateral hip prostheses. FDG uptake is noted only around neck of prosthesis (arrows). FDG PET diagnosis of loosening was confirmed after revision arthroplasty.
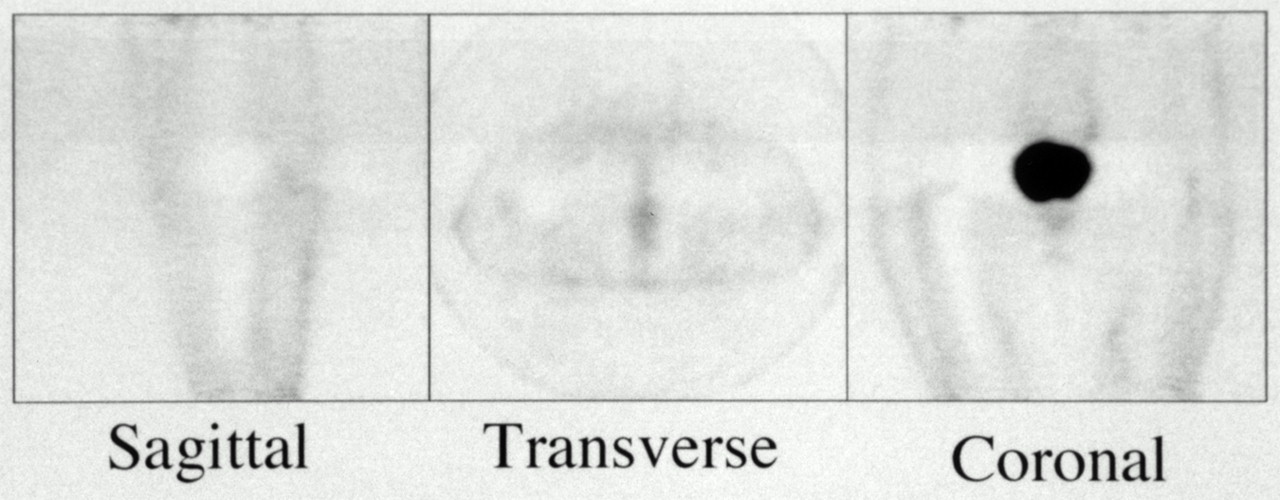
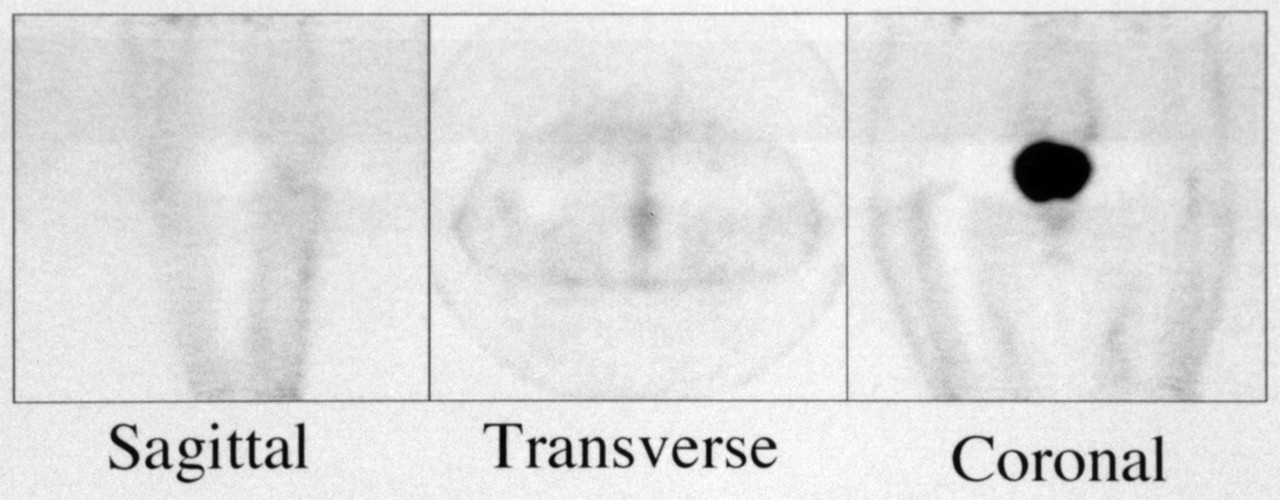
A 76-year-old woman with right hip prosthesis who presented with right hip pain. No focally increased FDG accumulation is seen around any portion of prosthesis on PET scan. Therefore, both infection and loosening were ruled out. Patient responded to conservative therapy during 16 mo of follow-up.
DISCUSSION
FDG PET has been used extensively for the detection of malignancy. However, on the basis of a large body of data in the literature, FDG uptake is not specific for a malignant process and is the source of low specificity when used in such settings. FDG accumulation has been reported in a variety of infectious or inflammatory sites, including abdominal infection (11), brain abscesses (12), inflammatory pancreatic disease (13), lobar pneumonia (14), sarcoidosis (15), osteomyelitis (16,17), tuberculosis (18), colitis (19), asthma (20), sinusitis (21), myositis (22), mastitis (23), and thyroiditis (24). On the other hand, in a proper setting, increased FDG accumulation may suggest the presence of infection or inflammation. This study clearly shows the feasibility of using FDG PET for discriminating infection as a complication of prosthesis from noninfectious processes in patients who have undergone lower limb arthroplasty.
Differentiation of an infected from a uninfected prosthesis (such as loosening) is essential for optimal and cost-effective management of these patients. Accurate confirmation or exclusion of infection before revision surgery can substantially simplify plans in these circumstances. In addition, the outcome can be significantly influenced by an accurate initial diagnosis. Current tests do not provide a sensitivity or specificity adequate for accomplishing these goals (25). Plain radiography has a limited role for the diagnosis of infection associated with prostheses because findings are common to both septic and aseptic failure. Also, infection and loosening commonly show no finding. Therefore, aspiration biopsy of the hip or knee of the patient is perhaps the most useful investigative tool for preoperative confirmation of infection, with sensitivity and specificity ranging from 50% to 93% and from 82% to 97%, respectively (25–27). However, the sensitivity of even preoperative joint aspiration is not high enough to exclude infection with an acceptable certainty (28). Moreover, the administration of antibiotics before aspiration biopsy can further reduce the sensitivity of this approach (26,27).
Radionuclide imaging has been extensively used for the diagnosis of infection after joint replacement. However, conventional nuclear medicine modalities, in addition to having limited sensitivity and specificity, suffer from two other shortcomings: the time required to complete the procedures and the cost of the examinations. Bone and gallium scans were first used in patients with a painful lower limb prosthesis in the 1970s (29). The sensitivity of combined bone and gallium scans is relatively poor (38%) (30). In only about one fourth to one third of patients with proven prostheses infections was the infection detected with these modalities (31,32). According to most reports, 111In-labeled white blood cell scanning, when combined with 99mTc-sulfur colloid bone marrow imaging (33), may provide superior sensitivity and specificity for detecting infection in this setting compared with other conventional nuclear medicine modalities. The sensitivity, specificity, and accuracy of this dual-tracer modality have been reported to be 86%–100%, 89%–94%, and 89%–96%, respectively (34–36).
A major concern about indium-labeled leukocyte imaging is the separating, labeling, and reinjection of the white blood cells, which offer several significant opportunities for iatrogenic errors (37) and significantly affect the function and viability of the final product. 111In- and 99mTc-labeled antibodies are emerging as a new approach to detect prosthesis infections without the necessity of labeling the cells outside the body and have had some success (38,39). However, other disadvantages of indium-labeled leukocyte imaging, such as the necessity for delayed imaging (24 h or longer), relatively high radiation exposure, and additional bone marrow imaging, remain major shortcomings.
To our knowledge, no major reports have appeared in the literature about the usefulness of FDG PET in the setting of chronic infection of orthopedic implants. FDG PET is often misperceived as an expensive, complicated imaging modality and, as such, requiring limited use. However, compared with traditional nuclear medicine methods, FDG PET may prove to be a single and cost-effective modality for accurately diagnosing infection associated with lower limb arthroplasty, especially in the hips. Based on routine practice in most institutions, the expense of FDG PET is substantially lower than the combined costs of 111In-labeled white blood cell scanning, bone marrow studies, and bone imaging, which are performed as a combination in most patients. In addition, tomographic images with FDG PET provide better spatial resolution than do conventional nuclear medicine modalities, significantly improving the performance of the test. Therefore, PET can better detect small and subtle changes in disease activity, which may be missed by other techniques. Figure 4 shows the value of this modality in providing information about a complex process. In the patient illustrated, who had clear clinical evidence of infection, FDG PET revealed the presence of infection in the bone–prosthesis interface, fistulous drainage of pus in the area, and a suggestion of loosening with superimposed infection around the neck. The details shown were unique and exemplified the unusual capability of this modality. Furthermore, FDG PET can be completed within a few hours, compared with 2 d for other nuclear medicine methods. Considering that the average cost of treating an arthroplasty patient with infection ranges from $50,000 to $60,000 (40) and that the success of treating infection associated with a prosthesis largely depends on early, accurate diagnosis, FDG PET may prove useful and cost-effective for optimal patient management of painful lower limb prostheses.
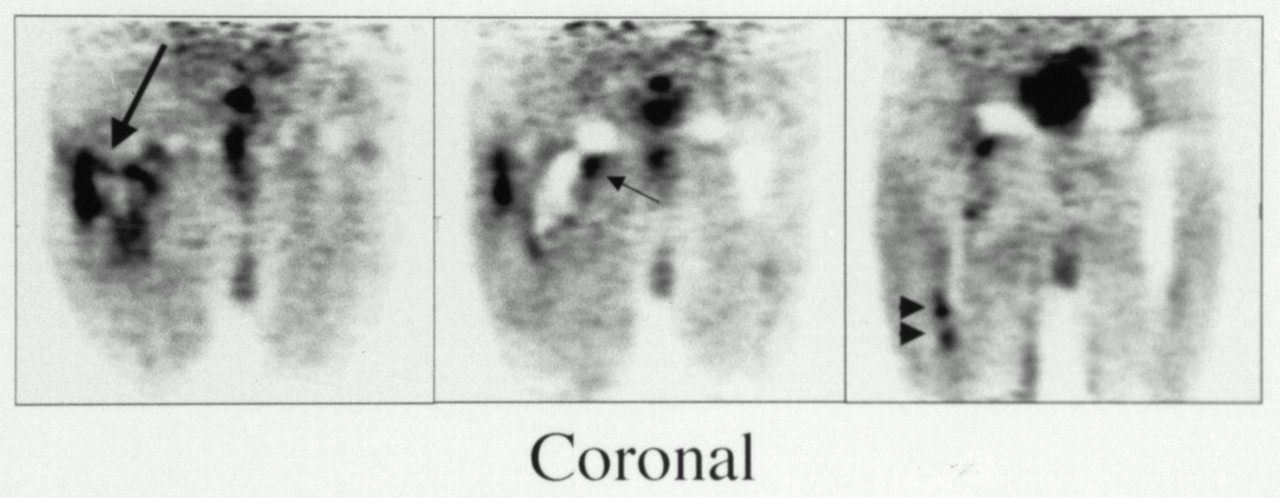
Coronal images of 63-y-old man with painful right hip prosthesis. Loosening (short arrow), infection (arrowheads), and fistula (long arrow) are shown.
Interestingly, the intensity of uptake at the bone–prosthesis interface was not important when making the diagnosis, and only the presence of uptake was an indication of infection. Therefore, increased tracer uptake at the bone–prosthesis interface should be considered suggestive of infection. In the hip, increased tracer uptake around the femoral head portion of the prosthesis was a reliable sign of loosening. If the accumulated FDG was limited around the femoral head or neck and did not extend to the bone–prosthesis interface, the probability of infection was low (Fig. 2D; compare with Figs. 2A and B). The simplicity of the diagnostic criteria proposed should reduce potential interobserver variation and increase the accuracy of the scan.
As a result of the high sensitivity of FDG PET, only two false-negative results were reported in this study. In contrast, 10 false-positive results, mostly among patients with knee prostheses, were reported. Incorrect interpretation of postsurgical changes as positive findings in FDG PET is well known. However, the interval between surgery and FDG PET was more than 1 y in all patients with false-positive results in this study. Therefore, in addition to postsurgical changes, other factors must have contributed to inaccurate results. Further research is required to clearly define the factors that contribute to false-positive results, especially in knee prostheses.
Our data clearly show that the performance of this technique is optimal for diagnosing and excluding the presence of infection in hip and knee prostheses. We have shown that using appropriate criteria for uptake of FDG in uninfected, infected, and loose prostheses achieves high accuracy, particularly for FDG PET of complicated hip prostheses. For reasons unknown, the FDG PET results for knee prostheses are somewhat inferior to those for hip prostheses. The major advantage of FDG PET over conventional nuclear medicine procedures is the simplicity of the approach and the timely availability of results (within 2–3 h).
CONCLUSION
These preliminary data show that the use of FDG PET for detecting infection associated with lower limb prosthesis is feasible but has some limitations. FDG PET is more useful for detecting infections in painful hip prostheses than in painful knee prosthesis.
Acknowledgments
This study was supported in part by a Department of Energy grant and by training grant CA-65442–04 from the National Institutes of Health, Bethesda, MD.
Footnotes
Received May 8, 2000; revision accepted Jul. 6, 2000.
For correspondence or reprints contact: Abass Alavi, MD, Division of Nuclear Medicine, Hospital of the University of Pennsylvania, 110 Donner Bldg., 3400 Spruce St., Philadelphia, PA 19104.
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- The Accuracy of Imaging Techniques in the Assessment of Periprosthetic Hip Infection: A Systematic Review and Meta-Analysis
- Radionuclide Imaging of Musculoskeletal Infection: A Review
- Failed Total Knee Arthroplasty
- Diagnosis and Management of Periprosthetic Shoulder Infections
- The assessment of total hip arthroplasty
- EANM/SNMMI Guideline for 18F-FDG Use in Inflammation and Infection
- Usefulness of Fluorine-18 Positron Emission Tomography/Computed Tomography for Identification of Cardiovascular Implantable Electronic Device Infections
- Role of Modern Imaging Techniques for Diagnosis of Infection in the Era of 18F-Fluorodeoxyglucose Positron Emission Tomography
- Imaging of prosthetic joints
- Diagnosis of Vascular Prosthesis Infection: PET or SPECT?
- Prosthetic Vascular Graft Infection: The Role of 18F-FDG PET/CT
- Diagnosis of Periprosthetic Infection
- Radionuclide imaging of the painful hip arthroplasty: POSITRON-EMISSION TOMOGRAPHY VERSUS TRIPLE-PHASE BONE SCANNING
- The Diabetic Foot: Initial Experience with 18F-FDG PET/CT
- Diagnosing Infection in the Failed Joint Replacement: A Comparison of Coincidence Detection 18F-FDG and 111In-Labeled Leukocyte/99mTc-Sulfur Colloid Marrow Imaging
- Radionuclide Imaging of Infection
- Detection of Musculoskeletal Infection with 18F-FDG PET: Review of the Current Literature
- Imaging of prosthetic joints
- Nuclear Medicine, the Painful Prosthetic Joint, and Orthopedic Infection