


Abstract
Somatostatin receptor scintigraphy (SRS) has been shown to reveal sarcoidosis sites. The aim of this study was to prospectively compare SRS and gallium scintigraphy in the evaluation of pulmonary and extrapulmonary involvement in patients with proven sarcoidosis. Methods: Eighteen patients with biopsy-proven sarcoidosis were included. Nine were or recently had been receiving steroid therapy at the time of the examination. Planar gallium scintigraphy (head, chest, abdomen, and pelvis) and thoracic SPECT were performed at 48–72 h after injection of a mean dose of 138 ± 21 MBq 67Ga. Planar SRS and thoracic SPECT were performed at 4 and 24 h after injection of a mean dose of 148 ± 17 MBq 111In-pentetreotide. Results: Gallium scintigraphy found abnormalities in 16 of 18 patients (89%) and detected 64 of 99 clinically involved sites (65%). SRS found abnormalities in 18 of 18 patients and detected 82 of 99 clinically involved sites (83%). Of the 9 treated patients, gallium scintigraphy found abnormalities in 7 (78%), detecting 23 of 39 clinically involved sites (59%), whereas SRS found abnormalities in 9, detecting 32 of 39 clinically involved sites (82%). Conclusion: This study suggests that, compared with gallium scintigraphy, SRS appears to be accurate and contributes to a better evaluation of organ involvement in sarcoidosis patients, especially those treated with corticosteroids.
Sarcoidosis is a multisystem inflammatory disease of unknown origin, characterized by the presence of noncaseating epithelioid cell granulomas in the affected tissue. Gallium scintigraphy is a widely used method for evaluating the extent of the disease at diagnosis (1–6).
Pentetreotide is a somatostatin analog labeled with 111In. Its use was first described in the evaluation of patients with neuroendocrine tumors (7,8). Uptake of 111In-pentetreotide was also reported for granulomatous diseases, namely tuberculosis, Wegener’s granulomatosis, and sarcoidosis (8–11). In vitro autoradiography performed on biopsy specimens of sarcoidosis tissue indicated that somatostatin receptors (subtype 2) were present in epithelioid cells and giant cells and were probably the sites of in vivo 111In-pentetreotide binding (9,11). In sarcoidosis patients, uptake of 111In-pentetreotide decreased with successful corticosteroid therapy, suggesting that 111In-pentetreotide binding reflected active sites of disease (9,11).
To our knowledge, the literature includes no data on potential advantages of somatostatin receptor scintigraphy (SRS) over gallium scintigraphy in the detection of granulomatous sites in patients with proven sarcoidosis. Therefore, our aim was to compare SRS and gallium scintigraphy in the evaluation of pulmonary and extrapulmonary involvement in these patients.
MATERIALS AND METHODS
Eighteen patients (10 men, 8 women; mean age, 35 ± 7 y) with biopsy-proven sarcoidosis were prospectively and consecutively included. All gave informed consent.
The diagnosis of sarcoidosis was based on a clinical, radiographic, and biologic pattern; the presence of typical granulomatous lesions in an involved organ; and the exclusion of known causes such as mycobacterial infection and domestic or professional exposure to beryllium or aluminum. The histologic hallmark of sarcoidosis was obtained for all patients, either by bronchial biopsy (n = 13), salivary gland biopsy (n = 10), skin biopsy (n = 5), mediastinoscopy (n = 1), peripheral lymph node biopsy (n = 1), or cerebral biopsy (n = 1).
Evaluation of Disease Extent
The initial diagnostic work-up included clinical examination; plain chest radiography; chest CT; serum angiotensin-converting enzyme levels; plasma calcium levels; and, in 13 patients, bronchoscopy (with bronchoalveolar lavage) and pulmonary function tests. Thoracic involvement was confirmed in all patients on the basis of chest radiography and CT findings and was classified as stage I (6 patients), stage II (10 patients), or stage III (2 patients).
Suspected extrathoracic involvement was investigated. All instances of clinically suspected salivary gland involvement were confirmed by biopsy. Skin involvement, when clinically suspected, was confirmed by biopsy of only one lesion for each patient. Involvement of the lacrimal glands and eyes was determined on the basis of ophthalmologic examination findings. Neurologic exploration (cerebrospinal fluid analysis, cerebral CT, or MRI) was performed on 4 patients (1 with hypopituitarism, 1 with epilepsy, and 2 with headache) because nervous system involvement was suspected. Cardiac exploration (echocardiography and rest sestamibi SPECT) was performed on 1 patient with chest pain. The peripheral lymph nodes were considered involved if a palpable lesion was found on physical examination (biopsy was performed on 1 of 2 patients). The liver was considered involved if its function was altered and no other cause was apparent. Abdominal sonography or CT was performed on patients in whom an enlarged liver or spleen had been found on clinical examination or who had altered liver function (n = 5). Muscle involvement was determined on the basis of elevated blood levels of creatinine phosphokinase and aldolase (n = 3). Determination of palate involvement was based on biopsy findings (n = 1).
At the time of scintigraphic evaluation, 7 patients were receiving steroids and 2 patients had recently stopped receiving steroids (2 wk and 6 mo, respectively, before scintigraphic evaluation). The delay between the two procedures was 14 ± 4 d.
Gallium Imaging
Scintigraphic planar images were acquired with a double-head camera (DST; SMV, Brie, France) 48–72 h after injection of a mean dose of 138 ± 21 MBq 67Ga (Cis Bio International, Gif sur Yvette, France). The camera had a medium-energy parallel-hole collimator using a 256 × 256 word matrix with a preset time of 10 min. Acquisition was performed using the three 67Ga photopeaks (93, 184, and 296 keV) with a 20% window. For the chest (carefully excluding the liver and spleen), 725 ± 237 kilocounts were collected; for the abdomen, 771 ± 245 kilocounts were collected.
At 48 h, the acquisition systematically included anterior and posterior views of the head and neck, thorax, abdomen, and pelvis. Additional lateral or oblique views of the thorax or head were obtained when necessary. Delayed images at 72 h after injection were obtained in cases of negative or doubtful findings, and the time of the acquisition was increased to 15–20 min.
Thoracic 67Ga SPECT was performed at 48 h after injection (n = 13). Cerebral 67Ga SPECT was performed on one patient. The acquisition included three 67Ga photopeaks, 64 projections over a 360° rotation, 60 s per step, and a 64 × 64 matrix. Slices were reconstructed after backprojection using a Hanning filter.
Somatostatin Receptor Imaging
Scintigraphic planar images were acquired with the same double-head camera after injection of a mean dose of 148 ± 17 MBq 111In-pentetreotide (Mallinckrodt Medical, Petten, The Netherlands). The camera had a medium-energy parallel-hole collimator using a 256 × 256 word matrix with a preset time of 10 min. Acquisition was performed using both 111In photopeaks (173 and 247 keV) and a 20% window. For the chest (carefully excluding the liver and spleen), 287 ± 78 kilocounts were collected; for the abdomen, 656 ± 213 kilocounts were collected. Thoracic images were obtained 4 h after injection, in the anterior and posterior views. At 24 h, the acquisition systematically included anterior and posterior views of the head, thorax, abdomen, and pelvis. Additional lateral or oblique views of the thorax or head were obtained when necessary. Delayed images were obtained 30–48 h after injection in cases of negative or doubtful findings, and the time of the acquisition was increased to 15–20 min.
Thoracic 111In-pentetreotide SPECT was performed 24 h after injection (n = 15). Cerebral 111In-pentetreotide SPECT was performed on one patient. The acquisition included a double-indium peak, 64 projections over a 360° rotation, 60s per step, and a 64 × 64 matrix. Slices were reconstructed after backprojection using a Hanning filter.
Image Analysis
For each tracer, scintigrams were viewed separately and independently by two observers who were unaware of other findings. A decision was reached by consensus in cases of interobserver disagreement. Gallium scintigraphy and SRS results were compared with the conventional evaluation of disease extent. For the analysis of involved sites, the thorax was divided into eight regions: right and left cervical or supraclavicular, right and left hilar or mediastinal, right and left lung, and right and left axillary. Only one organ site was independently considered (even when the extent was bilateral) for the involvement of lacrimal glands, salivary glands, eyes, inguinal lymph nodes, and muscles. Different localizations of skin involvement were considered as separate sites. Other analyzed sites—all considered as separate—included the nasal sinuses, liver, spleen, heart, central nervous system, and bone.
Quantitative analysis was used to compare gallium scintigraphy and SRS findings with image quality in clinically or radiologically known involved sites. Lesion-to-background uptake ratios were determined on both 48-h 67Ga images and 24-h 111In-pentetreotide images using regions of interest over the lesion and over the ipsilateral or contralateral side of normal uptake. The mean counts over the lesions and background regions were calculated, and ratios were obtained. The results of both scintigraphic procedures were expressed according to organ involvement and image quality.
Statistical Analysis
The χ2 test was used to compare site detection by the two techniques, and the paired t test was used to compare uptake ratios. Differences between the two scintigraphic procedures were considered significant when probability values were less than 0.05.
RESULTS
Clinical, Biologic, and Radiologic Evaluation of Disease Extent
Table 1 summarizes the results. Thoracic involvement was found in all 18 patients on the basis of radiographic and CT findings, corresponding to 26 lung sites in 13 patients and 30 hilar or mediastinal sites in 16 patients.
Evaluation of Sarcoidosis Involvement in 18 Patients: Results for Both Procedures Expressed as Number of Involved Sites
Extrathoracic involvement in the salivary gland (8 patients), lacrimal glands (5 patients), and eyes (1 patient, uveitis) was found in 43 sites. Central nervous system involvement was found in 5 sites from 4 patients and included pituitary and meningeal involvement (1 patient), a pseudotumoral lesion in the left temporal lobe (1 patient), and meningeal involvement (2 patients, with negative conventional imaging findings in 1 patient). Eight skin lesions were found in 3 patients (corresponding to 3 different sites in the first patient, 4 different sites in the second, and 1 site in the third). One site in each patient was confirmed by biopsy; however, the other sites were similar to confirmed sites. Peripheral lymph node involvement was found in 2 patients (inguinal in the first patient and supraclavicular in the second). Other sites included the liver (5 patients), the spleen (4 patients), the palate (1 patient), the heart (1 patient, pericarditis), and the muscle (3 patients).
On the basis of serial clinical, biologic, and radiologic evaluations and pulmonary function tests, the 9 treated patients were considered as having active disease or as having disease relapse in spite of steroid therapy. Thirty-nine sites were found to be still involved: 24 thoracic and 15 extrathoracic.
Image Quality of the Two Scintigraphic Procedures
SRS images were consistently better than gallium images, with well-delineated lesions, especially in the hilar or mediastinal area, on either planar or SPECT images (Figs. 1 and 2). The uptake ratio was significantly higher with 111In-pentetreotide than with 67Ga when considering all sites (3.44 ± 1.35 and 2.80 ± 1.34, respectively, P < 0.0001) and when considering only thoracic sites (3.65 ± 1.28 and 2.88 ± 1.36, respectively, P < 0.0001). A moderate correlation was seen between 111In-pentetreotide uptake and 67Ga uptake (r = 0.63, P < 0.001).
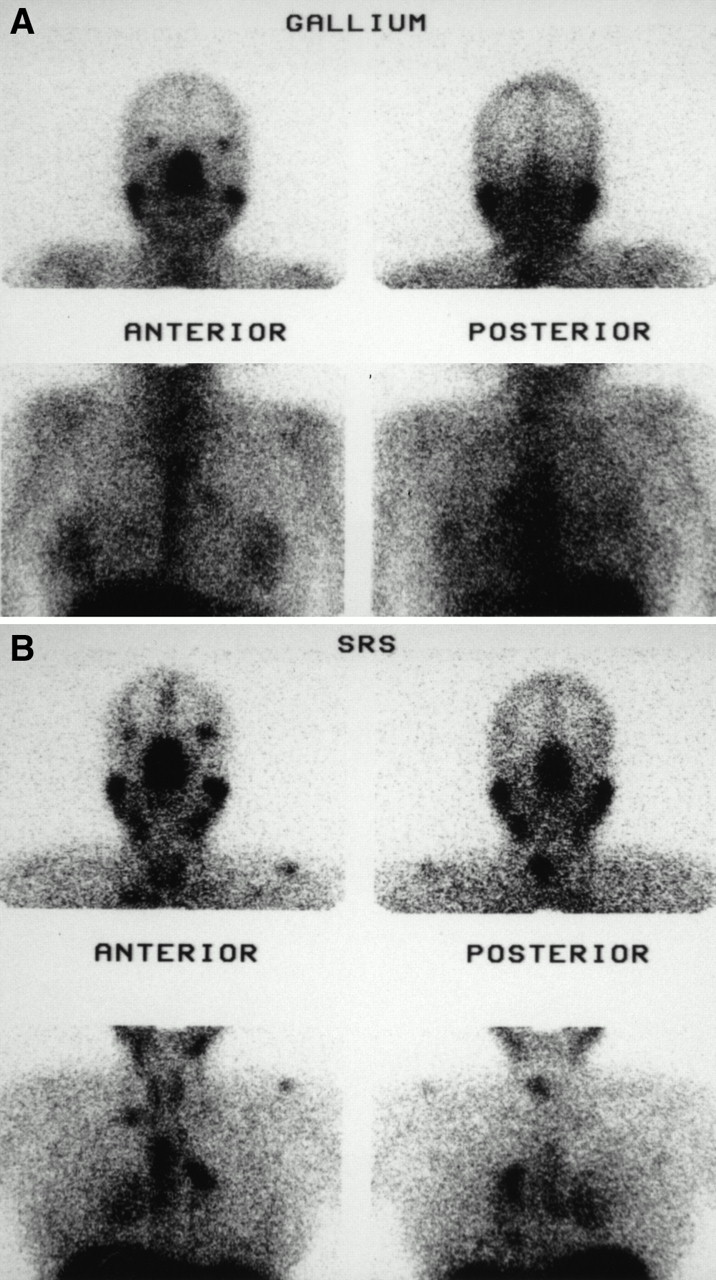
Planar images of head and chest in patient with sarcoidosis 2 wk after corticosteroid therapy was stopped. (A) Gallium scintigraphy shows high uptake in nose, lacrimal glands, and salivary glands and mild uptake in skin lesion and in hilar and mediastinal lymph nodes. (B) SRS shows high uptake in nose; meningeal, lacrimal, and salivary glands; hilum and mediastinal area; lung; and two skin lesions, one on shoulder and one on neck.
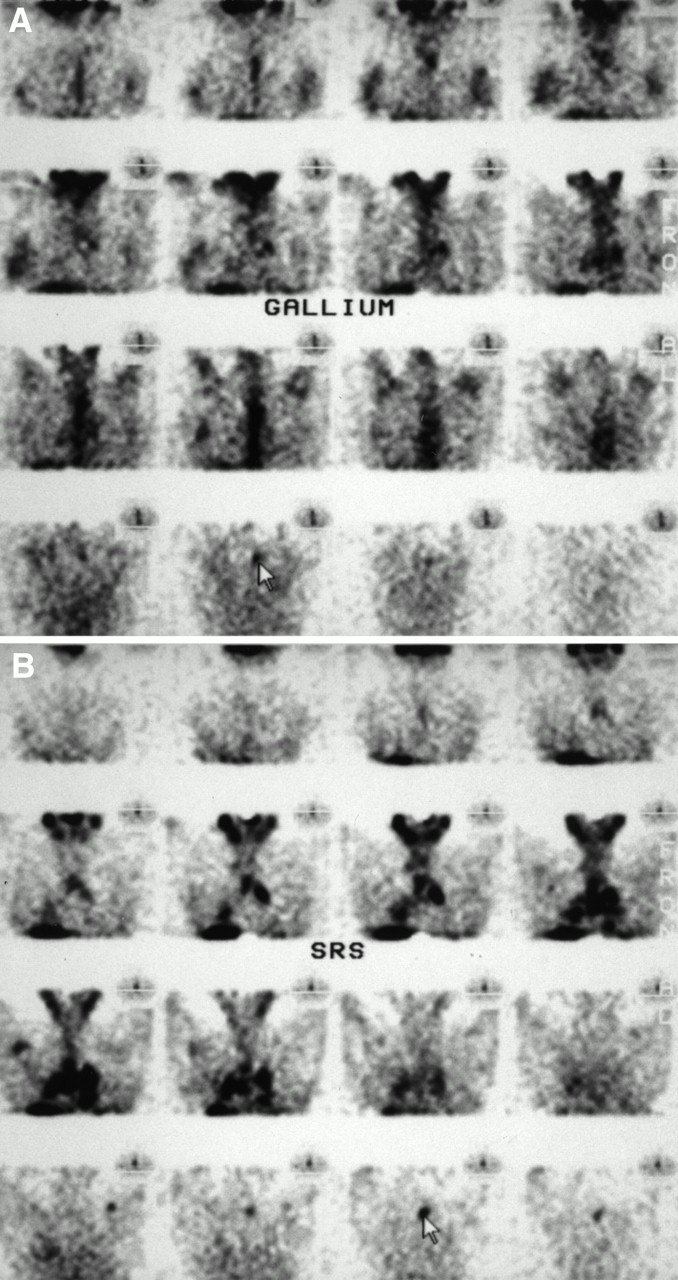
Coronal thoracic SPECT. (A) 67Ga images show mild uptake in skin lesion (arrow) and in hilar and mediastinal lymph nodes. (B) 111In-pentetreotide images show high uptake in hilar and mediastinal lymph nodes and in lung, skin lesions, and right axillary lymph node.
In the treated patients, SRS images were also consistently better than gallium images as reflected by the uptake ratio, especially for thoracic sites (3.33 ± 1. 37 and 2.41 ± 0.88 for 111In-pentetreotide and 67Ga, respectively, P < 0.002). Only in involved salivary glands did the uptake appear similar with 67Ga and 111In-pentetreotide; the uptake ratios were not significantly different (2.3 ± 0.6 and 2.3 ± 0.7, respectively, P = 0.9).
Gallium Scintigraphy
Table 1 summarizes the results. In the overall population, the results of gallium scintigraphy were abnormal in 16 of 18 patients (89%) and normal in 2 of 18 patients (11%): 64 of 99 clinically involved sites (65%) were detected (Figs. 1 and 2).
For thoracic involvement, gallium scintigraphy showed abnormal findings in 16 of 18 patients, detecting 43 of 56 sites. Gallium scintigraphy missed 13 sites (9 hilar or mediastinal lymph node sites and 4 lung sites).
For extrathoracic involvement, gallium scintigraphy showed abnormal findings in 12 of 14 patients (86%), detecting 21 of 43 sites (49%). Gallium scintigraphy missed 22 sites in 7 patients (Table 1). In 11 patients, gallium scintigraphy revealed 19 extrathoracic sites that were not suspected clinically (4 salivary gland sites, 3 lacrimal gland sites, 1 nose and sinus site, 10 peripheral lymph node sites, and 1 bone site) (Table 2).
Sites Revealed by SRS, Gallium Scintigraphy, or Both
SRS
Table 1 summarizes the results. In the overall population, SRS showed abnormal findings in all 18 patients and detected 82 of 99 clinically involved sites (83%). SRS detected significantly more sites than did gallium scintigraphy (P < 0.001), with consistently better lesion contrast, especially for the hilar or mediastinal area (Fig. 2).
For thoracic involvement, SRS showed abnormal findings in all patients, detecting all 56 involved sites (26 lung sites and 30 hilar or mediastinal lymph node sites). For extrathoracic involvement, SRS showed abnormal findings in 13 of 14 patients (93%), detecting 26 of 43 sites (60%). SRS missed 17 sites in 6 patients: 1 salivary gland site, 2 lacrimal gland sites, 1 eye site (uveitis), 1 liver site, 1 heart site (pericarditis), 3 muscle sites, 2 central nervous system sites (1 meningeal, with negative conventional imaging, and 1 pituitary), and 6 skin sites (Table 1).
In 13 patients, SRS revealed 24 extrathoracic sites that were not suspected clinically (2 salivary gland sites, 1 lacrimal gland site, 1 nose or sinus site, 16 peripheral lymph node sites, 3 bone sites, and 1 central nervous system site) (Table 2).
Comparison of Both Procedures in Corticosteroid-Treated Patients
Gallium scintigraphy showed abnormal findings in seven of nine treated patients (78%) and detected 23 of 39 clinically involved sites (59%). It failed to detect bilateral thoracic involvement and a pseudotumoral lesion in the left temporal lobe in one patient and bilateral thoracic involvement in another patient. In addition, gallium scintigraphy missed 11 extrathoracic sites in seven patients: 1 salivary gland site, 1 eye site (uveitis), 1 muscle site, and 4 skin sites. None of the 4 other central nervous system sites were shown by gallium scintigraphy.
SRS showed abnormal findings in all treated patients and detected 32 of 39 clinically involved sites (82%) (all thoracic sites [10 lung and 14 hilar or mediastinal lymph node] and 8 extrathoracic sites). In particular, SRS detected central nervous system involvement in three of four patients: meningeal involvement in two patients and a pseudotumoral lesion in the left temporal lobe in the third patient.
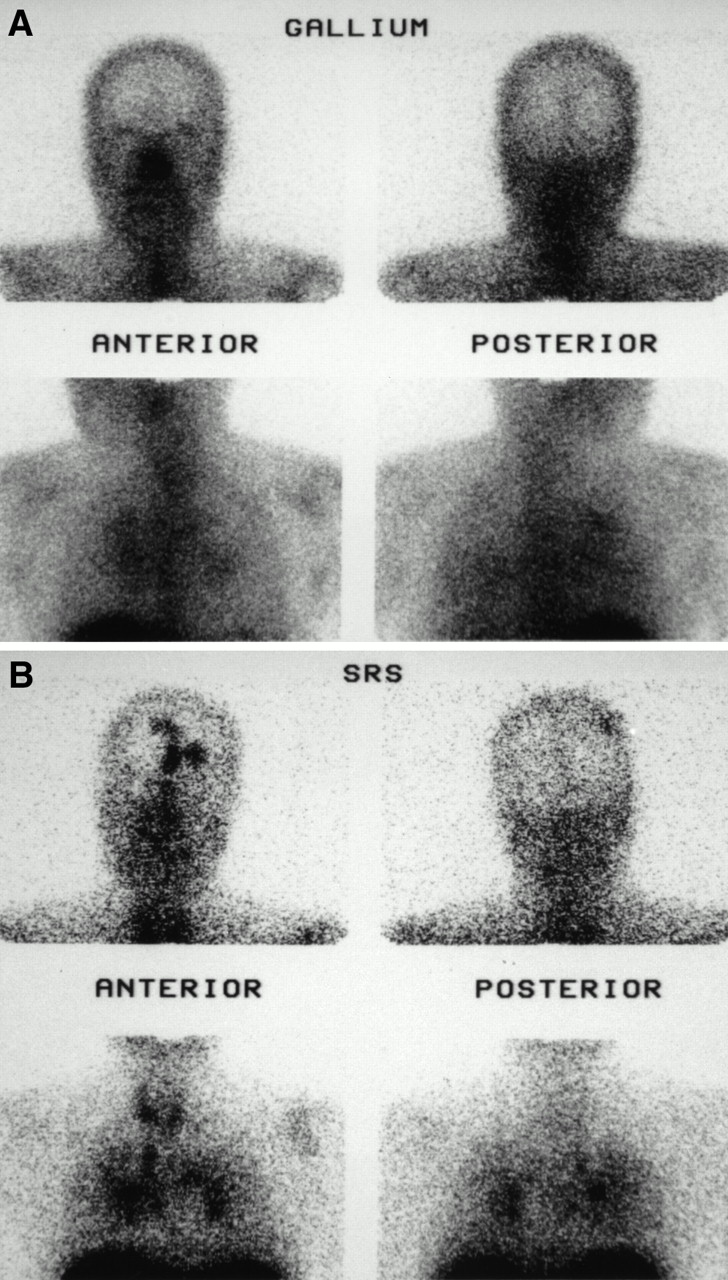
SRS missed 7 extrathoracic sites in five patients: one salivary gland site, 1 eye site (uveitis), 2 muscle sites, 2 central nervous system sites (1 pituitary and 1 meningeal), and 1 skin site. In addition, in one treated patient, SRS confirmed 3 sites of clinically suspected bone involvement for which radiography findings had been negative and revealed 1 site of cerebral involvement (meningeal and cortical) that was neither clinically suspected nor visualized by gallium but was confirmed by cerebral gadolinium-enhanced MRI performed after SRS (Fig. 3). In summary, in the treated patients, SRS detected significantly more sites than did gallium scintigraphy (P < 0.00l), especially for thoracic and central nervous system involvement, and appeared more accurate for evaluation of disease activity.
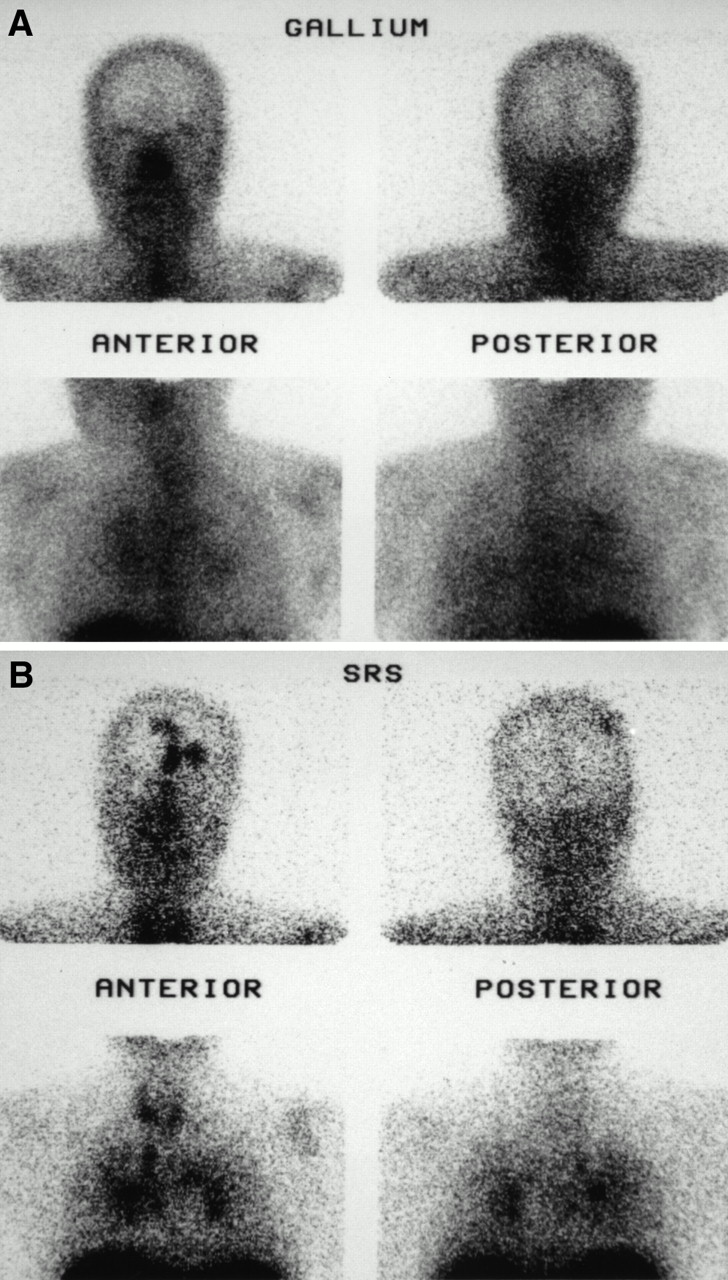
Planar images of head and chest in patient with sarcoidosis treated by steroid therapy with decreasing doses (3 mg/day at time of scintigraphic evaluation). (A) Gallium scintigraphy shows only mildly increased uptake in hilar and mediastinal lymph nodes and in lung. (B) SRS shows high uptake with well-delineated lesions in hilar and mediastinal lymph nodes and in lung and reveals corticomeningeal and skull involvement, which was confirmed after SRS by cerebral MRI.
DISCUSSION
Gallium scintigraphy has been widely used to evaluate the extent of sarcoidosis (1–6,12–16). The mechanism of uptake is related to binding to transferrin (17–19). Indeed, the sensitivity of gallium scintigraphy for the detection of granulomatous disease has varied from 60% to 90% in mediastinal or pulmonary sarcoidosis in the literature (3,6). The current recommendations for the use of gallium scintigraphy are to support the diagnosis in case of diagnostic difficulties (particularly in patients with isolated extrathoracic lesions suspected of being sarcoidosis or in patients with normal radiography findings) and to detect clinically silent extrathoracic involvement, providing extrathoracic sites for biopsy (6,19). For following up doubtful cases after steroid therapy, gallium scintigraphy may be useful; some authors have reported the results of gallium scintigraphy as a marker of sarcoidosis activity and found the technique to be accurate for evaluating therapeutic response and for detecting or excluding relapse in patients treated with steroids (12,15,19–21). However, reliability in assessing activity remains controversial. Other studies have found that gallium scintigraphy was not accurate in predicting treatment response. It shows, in patients receiving corticosteroids, decreased gallium accumulation or negative findings that do not reflect the activity of the disease and does not detect later relapses (6,22–25).
In addition, image quality with 67Ga is limited because of the presence of physiologic uptake in the liver and, to a lesser degree, in the spleen, bone marrow, lacrimal glands, salivary glands, nasopharyngeal mucosa, and breast. Slight uptake is found in normal lung as well as in bone marrow even on 48- to 72-h images, leading to high background activity and more difficult detection of lesions with low uptake.
SRS seems to be a promising alternative to gallium scintigraphy for evaluating the extent of sarcoidosis. Our study shows that SRS, compared with gallium scintigraphy, detects significantly more sites of sarcoidosis involvement. Lesion contrast was consistently and significantly higher with SRS than with gallium scintigraphy, especially for lung and mediastinal involvement. The reasons are probably the absence of physiologic uptake of 111In-pentetreotide in bone marrow or lungs, leading to better detectability, and the 111In photon energy, which better suits the gamma camera.
This good performance of SRS agrees with that reported in the literature (9–11). In a series of 46 patients with sarcoidosis, SRS detected known hilar and mediastinal lymph nodes, and interstitial lung disease in 36 of 37 patients (97%) with known sarcoidosis involvement (11). In this study, new sites were also detected by SRS in 23 of 46 patients (50%) (11). Similarly, SRS detected new granuloma sites in 9 of 13 patients (69%) in another reported study (9). However, SRS missed known granulomatous sites, including cutaneous, ocular, liver, and cerebral sites, in 23% and 28% of patients (9,11).
In these series, granulomatous sites revealed by SRS were considered to represent active disease: in vitro autoradiography and immunohistochemical studies were performed on biopsy specimens of sarcoidosis tissue and found that somatostatin receptors (subtype 2) were present in epithelioid cells and giant cells, in which octreotide uptake was detected (9,11,26). SRS was repeated in patients receiving corticosteroid therapy, and normalization or decreased pathologic uptake corresponded to clinical or radiologic improvement (9,11). In one biopsy specimen of sarcoidosis tissue from a patient successfully treated with glucocorticoids, complete sclerosis of a granulomatous lesion was shown and no somatostatin receptors were detected (9,11). The exact physiopathologic role of somatostatin receptors and the effect of octreotide are yet unknown. The use of octreotide as a possible therapeutic agent for sarcoidosis has been suggested and is under evaluation (11).
In our series, all treated patients were considered to have active disease or relapse of disease. SRS revealed a significantly greater number of abnormal sites than did gallium scintigraphy, with significantly higher lesion contrast, especially for lung and mediastinal involvement. Moreover, seven sites (four patients) were seen with SRS and not with gallium scintigraphy: one pseudotumoral lesion in the left temporal lobe, two sites of meningeal involvement, and four sites of thoracic involvement were confirmed by cerebral CT or gadolinium-enhanced MRI and chest CT. In addition, SRS revealed, in one additional patient, meningeal and cortical involvement not suspected clinically and not detected with gallium scintigraphy. The involvement was confirmed afterward with gadolinium contrast-enhanced MRI.
These results suggest that lesions found with SRS but not with gallium scintigraphy were active lesions. However, our series and other reported series included few patients, and the lack of in vitro analysis of somatostatin receptor (subtype 2) lesions limits our study. A large series is required to confirm these results.
SRS also has some limitations. It missed 40% of extrathoracic sites. These misses were sometimes related to the scanning technique. In one patient, a case of uveitis and a pituitary lesion were not detected; however, cerebral SPECT was not performed and intense uptake in the nose and sinuses led to difficulty in analyzing the pituitary area. In another patient, pericarditis was not visualized by SRS with either planar imaging or thoracic SPECT; however, diffuse and intense bilateral lung uptake was present and may have led to difficulty in detecting pericardial involvement. The other misses could be the results of receptor-negative lesions: SRS visualized only two of three skin sites in one patient and showed negative findings in the two other patients (five sites). Skin involvement was confirmed through biopsy for one site in each of the three patients. However, the other sites were similar and were not part of erythema nodosum.
CONCLUSION
This study suggests that SRS appears to be more accurate than gallium scintigraphy for evaluating the extent of sarcoidosis. In patients receiving corticotherapy, SRS contributes to a better evaluation of organ involvement. Additional studies are needed to evaluate use of SRS as an indicator of therapeutic response.
Footnotes
Received Mar. 3, 2000; revision accepted Jul. 28, 2000.
For correspondence or reprints contact: Rachida Lebtahi, MD, Service de Médecine Nucléaire, Hôpital Bichat, 46 rue Henri Huchard, 75018, Paris, France.
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Imaging the inflammatory activity of sarcoidosis
- The Utility of 18F-FDG PET/CT for Diagnosis and Adjustment of Therapy in Patients with Active Chronic Sarcoidosis
- Comparative Evaluation of 18F-FDG PET and 67Ga Scintigraphy in Patients with Sarcoidosis
- Increased Uptake of 111In-Octreotide in Idiopathic Pulmonary Fibrosis