


Abstract
Idiopathic pulmonary fibrosis (IPF) is characterized by an uncontrolled accumulation and activation of lung fibroblasts. A modulation of fibroblast activation has been observed in various systems with octreotide, a synthetic somatostatin analog with strong affinity for the somatostatin receptor subtype 2 (sst2). One aim of our study was to evaluate the expression of somatostatin receptors in the lungs of patients with IPF. A second aim was to evaluate the relationship between 111In-octreotide uptake and the effect of pulmonary fibrosis as assessed by lung function tests and parameters and by radiologic findings. Methods: We investigated 11 patients with IPF, 6 patients with pulmonary fibrosis associated with systemic sclerosis (SSc), and 19 patients with disease not of the lung (control patients). The expression of somatostatin receptors was evaluated in vivo using 111In-octreotide scintigraphy. We evaluated the relationship between 111In-octreotide uptake and the activity of pulmonary fibrosis as assessed by lung function tests, bronchoalveolar lavage (BAL) cellularity, and high-resolution CT (HRCT) of the chest. Planar images and thoracic SPECT (24 h) were performed after injection of 222 MBq of 111In-octreotide. Lung uptake was quantified using the lung-to-background ratio (L/B). In addition, the expression of sst2 was evaluated in vitro, in frozen lung-tissue samples using autoradiography, and in human cultures of lung fibroblasts using a ligand-binding assay. Results: Compared with lung uptake in control patients (median L/B, 1.25; range, 1.14–1.49), lung uptake was increased in all 11 IPF patients (median L/B, 2.63; range, 1.59–3.13; P < 0.001) and in 4 of 6 SSc patients (median L/B, 1.68; range, 1.42–2.16). The L/B was lower in SSc patients than in IPF patients (P = 0.011). Increased uptake correlated with the alteration of lung function (carbon monoxide diffusing capacity [ρ = −0.655; P = 0.038], diffusing capacity for carbon monoxide and alveolar volume ratio [ρ = −0.627; P = 0.047], vital capacity [ρ = −0.609; P = 0.054], and total lung capacity [ρ = −0.598; P = 0.058]) and with the intensity of alveolitis (total BAL cellularity [ρ = 0.756; P = 0.045], neutrophil counts [ρ = 0.738; P = 0.05]), and HRCT fibrosis score (ρ = 0.673; P = 0.007). Autoradiography suggested that vascular structures were a prominent binding site. Lung fibroblasts expressed somatostatin receptors in vitro as measured by binding assay. Conclusion: Our preliminary results identified an increased expression of sst2 in (mainly idiopathic) pulmonary fibrosis. Lung uptake correlates with the alteration of lung function and with the intensity of alveolitis.
Idiopathic pulmonary fibrosis (IPF) is a relentlessly progressive disease of unknown cause that usually leads to death within 5 y of diagnosis and has the worst prognosis of all interstitial lung diseases (1). Although the therapeutic strategy is based on the use of low-dose corticosteroids combined with immunosuppressants (azathioprine or cyclophosphamide), according to the American Thoracic Society/European Respiratory Society (ATS/ERS) consensus statement (1), the available data suggest that this therapy may have a limited effect, if any, on clinical outcome (2). New therapeutic approaches for IPF are mandatory.
Current understanding of the pathophysiology of IPF suggests that the disease results from uncontrolled accumulation and activation of lung fibroblasts (3). Some alternative therapies that were developed to inhibit specifically fibroblast activation or proliferation have proved useful in animal models of pulmonary fibrosis and are undergoing evaluation in human IPF (4–6).
Octreotide, a synthetic somatostatin analog with strong affinity for the somatostatin receptor subtypes 2 (sst2), 3, and 5 (7–9), has been shown to modulate fibroblast activation in vitro (10,11); to exert antifibrotic properties in vivo in rat models of hepatic, esophageal, or digestive fibrosis (12–16); and to decrease the accumulation of connective tissue in mice (17). The mechanisms of the antifibrotic action of octreotide remain unclear. In vitro, octreotide inhibits the proliferation of skin fibroblasts cultured from pretibial myxedema human tissues and of orbital fibroblasts from retroorbital tissues in Grave's disease (10,11). Some data also indicate that octreotide inhibits the in vivo expression of transforming growth factor-β, a key fibrogenic mediator in rat models of intestinal and peritoneal fibrosis (16,18).
Therefore, the first aim of our study was to evaluate the expression of somatostatin receptors in the lungs of patients with IPF. We compared the expression in these patients with that in patients who had pulmonary fibrosis associated with systemic sclerosis (SSc) and in control patients. The comparison was done in vivo using 111In-octreotide scintigraphy. The second aim of our study was to evaluate the relationship between 111In-octreotide uptake and the effect of pulmonary fibrosis as measured by lung function tests and parameters and by radiologic findings.
In addition, the expression of sst2 was evaluated in vitro using receptor autoradiography in frozen lung-tissue samples and using a ligand-binding assay in human cultures of lung fibroblasts (derived from patients with IPF).
MATERIALS AND METHODS
Seventeen consecutive patients (11 men and 6 women) were evaluated: 11 with IPF (median age, 67 y; range, 46–76 y) and 6 with pulmonary fibrosis associated with SSc (median age, 45 y; range, 23–74 y). All the patients were informed of the rationale of the study and gave their consent. The study was approved by the local ethics committee.
A population of 19 patients (12 men and 7 women; median age, 69 y; range, 45–78 y) without lung disease who were evaluated with 111In-octreotide scintigraphy for the diagnostic workup of digestive neuroendocrine tumors were included as control patients for 111In-octreotide uptake in the lungs.
IPF was diagnosed according to the criteria given in the ATS/ERS consensus statement (1). For the IPF patients, the median delay between diagnosis and evaluation was 9 mo. Lung biopsy results were available for 2 of 11 patients with IPF and showed a usual pattern of interstitial pneumonia. One patient was an active smoker, 8 patients were former smokers, and 2 patients had never been smokers. Two patients received treatment for IPF at the time of the examination: prednisone (25 mg/d) and azathioprine (125 mg/d) in one patient, and prednisone (20 mg/d) in the other patient. For the SSc patients, the median delay between SSc diagnosis and evaluation was 48 mo. Lung biopsy had not been performed on SSc patients. One patient was a former smoker, and 5 patients had never been smokers. Two patients received prednisone (20 and 35 mg/d) at the time of the examination.
Scintigraphic planar images were acquired using a double-head camera (DST XL; GE Healthcare) after injection of 222 MBq of [111In-(diethylenetriaminepentaacetic acid)-d-phenylalanine]octreotide (111In-octreotide; Mallinckrodt Medical). Acquisitions were performed with a medium-resolution parallel-hole collimator centered on both 111In peaks (171 and 245 keV), using a 256 × 256 word matrix with a preset time of 15 min, as previously described (19). Thoracic SPECT was performed 24 h after injection in all patients (64 × 64 matrix, 64 projections, 60 s per step). Slices were reconstructed iteratively.
111In-Octreotide uptake in the lungs was assessed visually and was quantified using the lung-to-background ratio (L/B) (19). Regions of interest were manually drawn over the 2 lungs on the anterior planar image and on a region considered the background, the ipsilateral shoulder. The average counts per pixel in each region of interest were computed, the L/B was generated for each lung, and the lung uptake was expressed as the mean L/B.
We evaluated the relationship between 111In-octreotide uptake and the activity of pulmonary fibrosis as assessed by pulmonary function tests (vital capacity, total lung capacity, carbon monoxide diffusing capacity, arterial blood gas analysis), bronchoalveolar lavage (BAL) cytology, and high-resolution CT (HRCT) of the lung performed within 3 mo. The extent of the fibrosis and of the ground-glass opacities was evaluated on HRCT in a masked fashion according to the criteria of Kazerooni et al. (20) and was scored by 2 independent observers. A fibrosis score, a ground-glass score, and a total HRCT score were calculated for each patient. We correlated the mean L/B with pulmonary function test results, BAL results, and HRCT scores obtained within 3 mo of the scintigraphy.
In addition, the expression of sst2 was evaluated “in vitro,” using autoradiography of lung samples from 2 control patients and from 4 IPF patients. Only 1 of these 4 IPF samples was obtained from a patient previously studied by 111In-octreotide scintigraphy. Evaluation of the sst2 expressed in frozen pulmonary-tissue samples was performed with in vitro receptor autoradiography on 20-μm-thick sections using [125I-Tyr3]octreotide as the radioligand, according to a previous report (21). Briefly, frozen tissue sections were incubated for 2 h at room temperature with the sst2-preferring radioligand [125I-Tyr3]octreotide. Nonspecific binding was determined in serial tissue sections incubated with the radioligand in the presence of a 10−6 mol/L concentration of unlabeled octreotide. The slides were exposed to BioMax MR film (Kodak) for 7 d at 4°C.
Lung fibroblasts derived from IPF patients and from control patients (not included in the scintigraphic study) were cultured in vitro for 6 d in Dulbecco's modified Eagle medium with 10% fetal bovine serum according to previously described methods (22). Lung fibroblasts from IPF or control patients were grown in 24-well plates and incubated for 1 h at 37°C with [125I-Tyr11]somatostatin-14 (0.2 nmol/L final concentration; Amersham Bioscience) in 250 μL of Dulbecco's modified Eagle medium containing 0.5% bovine serum albumin and a protease inhibitor cocktail (Sigma). The fibroblasts were then washed 3 times with ice-cold Dulbecco's modified Eagle medium and 0.5% bovine serum albumin and lysed with 0.1N NaOH, and the radioactivity was counted. The amount of somatostatin-14–sensitive and octreotide-sensitive [125I-Tyr11]somatostatin-14 binding sites was evaluated in the presence of 10−6 mol/L concentrations of somatostatin-14 (Neosystem) or octreotide, respectively. Binding results (disintegrations per minute) from 4–6 wells were normalized to 106 cells.
Data are expressed as median followed by range, in parentheses, except for L/B and for the analysis of radioligand-binding experiments. Comparisons between control patients, IPF patients, and SSc patients were performed using the nonparametric Mann–Whitney U test. The Spearman rank test was used for correlations. Binding assays were analyzed using the Kruskal–Wallis ANOVA test, followed by the Mann–Whitney U test. A P value of 0.05 or less was considered significant.
RESULTS
111In-Octreotide scintigraphy in the 19 control patients showed no significant uptake in the lungs. The L/B was 1.25 (1.14–1.49). All 11 IPF patients demonstrated a strong increase in 111In-octreotide uptake in the lungs, compared with the uptake seen in control patients (Fig. 1). The L/B in IPF patients was 2.63 (1.59–3.13) and was always higher than in control patients (P < 0.001).
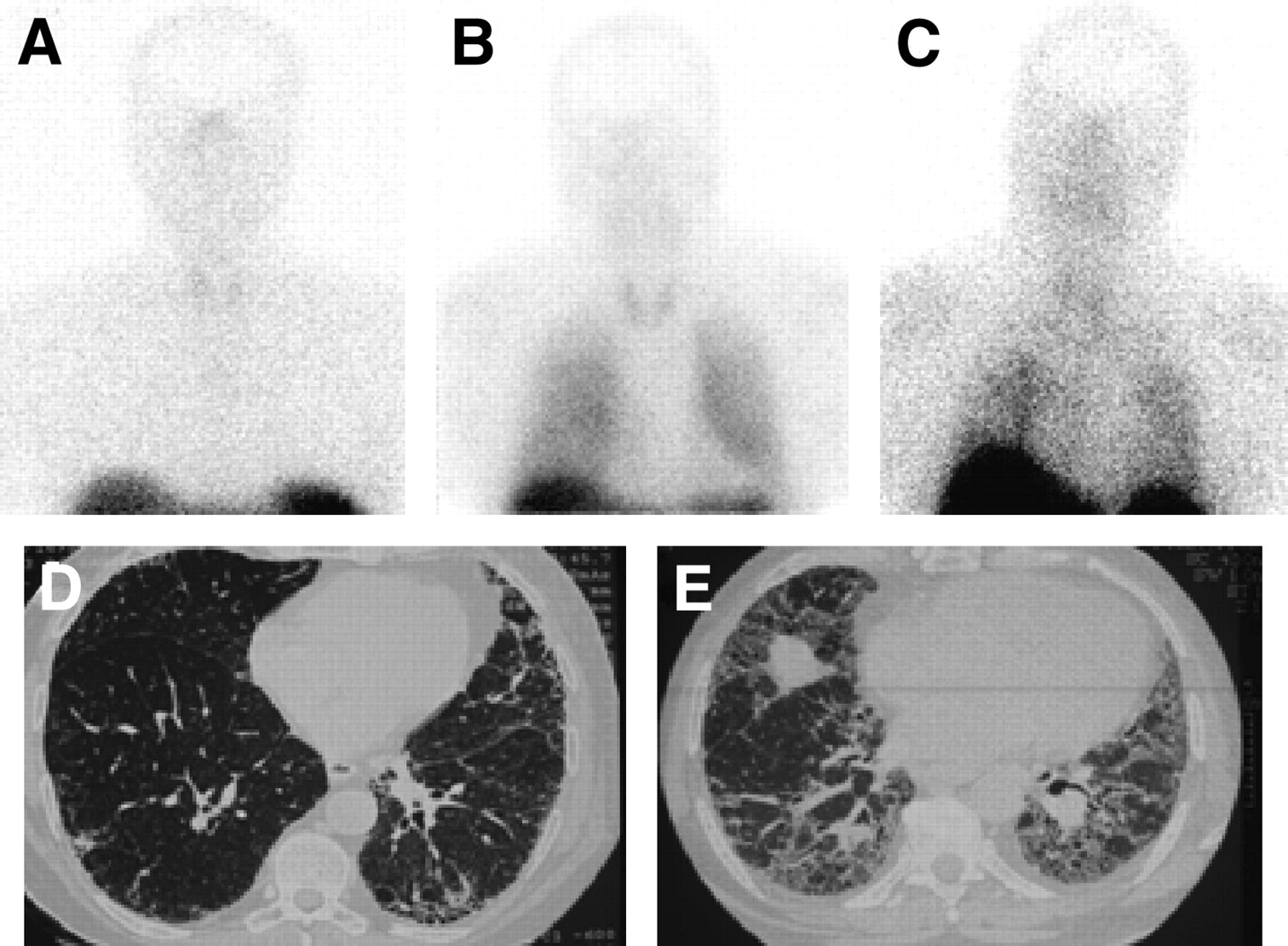
Octreotide scintigraphy. (A) In patient with carcinoid tumor of digestive tract without lung involvement, no octreotide uptake is seen in lung. (B–E) In 2 patients with IPF, diffuse uptake of 111In-octreotide is seen in both lungs, but extent of CT abnormalities differs (L/B of 2.82 and 2.63 and total CT score of 2.8 and 3 for patient in B and D and patient in C and E, respectively).
Pulmonary function test results, BAL results, and HRCT results in IPF and SSc patients are shown in Table 1. The 111In-octreotide uptake in the lungs did not correlate with age, cumulative tobacco smoking, or disease duration. The 111In-octreotide uptake in the lungs correlated with the intensity of alveolitis as assessed by total BAL cellularity (ρ = 0.756; P = 0.045) and neutrophil counts (ρ = 0.738; P = 0.05) and tended to correlate with BAL macrophages (ρ = 0.667; P = 0.078) and BAL lymphocytes (ρ = 0.643; P = 0.089). The 111In-octreotide uptake was higher in the patients with the more deteriorated lung function as assessed by a low diffusing capacity for carbon monoxide (ρ = −0.655; P = 0.038), a low diffusing capacity for carbon monoxide and alveolar volume ratio (ρ = −0.627; P = 0.047), a low volume capacity (ρ = −0.609; P = 0.054), and low total lung capacity (ρ = −0.598; P = 0.058). The arterial partial pressures of oxygen and carbon dioxide did not correlate with the lung octreotide uptake.
Pulmonary Function Tests, BAL, and HRCT Results in IPF and SSc Patients
Four of 6 patients with SSc demonstrated an increase in 111In-octreotide uptake in the lungs, compared with the uptake seen in control patients. The L/B was 1.68 (1.42–2.16). We observed that the median L/B was lower in patients with SSc than in patients with IPF (P = 0.011). No correlation between 111In-octreotide uptake and HRCT scores was found in SSc patients. However, when IPF and SSc patients were analyzed together, we found a positive correlation between 111In-octreotide uptake and the HRCT fibrosis score (ρ = 0.673; P = 0.007).
Autoradiography evidenced moderate binding of [125I-Tyr3]octreotide on vascular structures (large vessels) of lung samples in 3 patients with IPF (Fig. 2). However, not all vessels were labeled; medium-sized vessels were preferentially labeled. No specific binding was detected in 1 IPF sample and in the 2 control lung samples. In some areas, we observed a weak labeling of lymphoid aggregates—almost at the limit of the sensitivity of the methods.
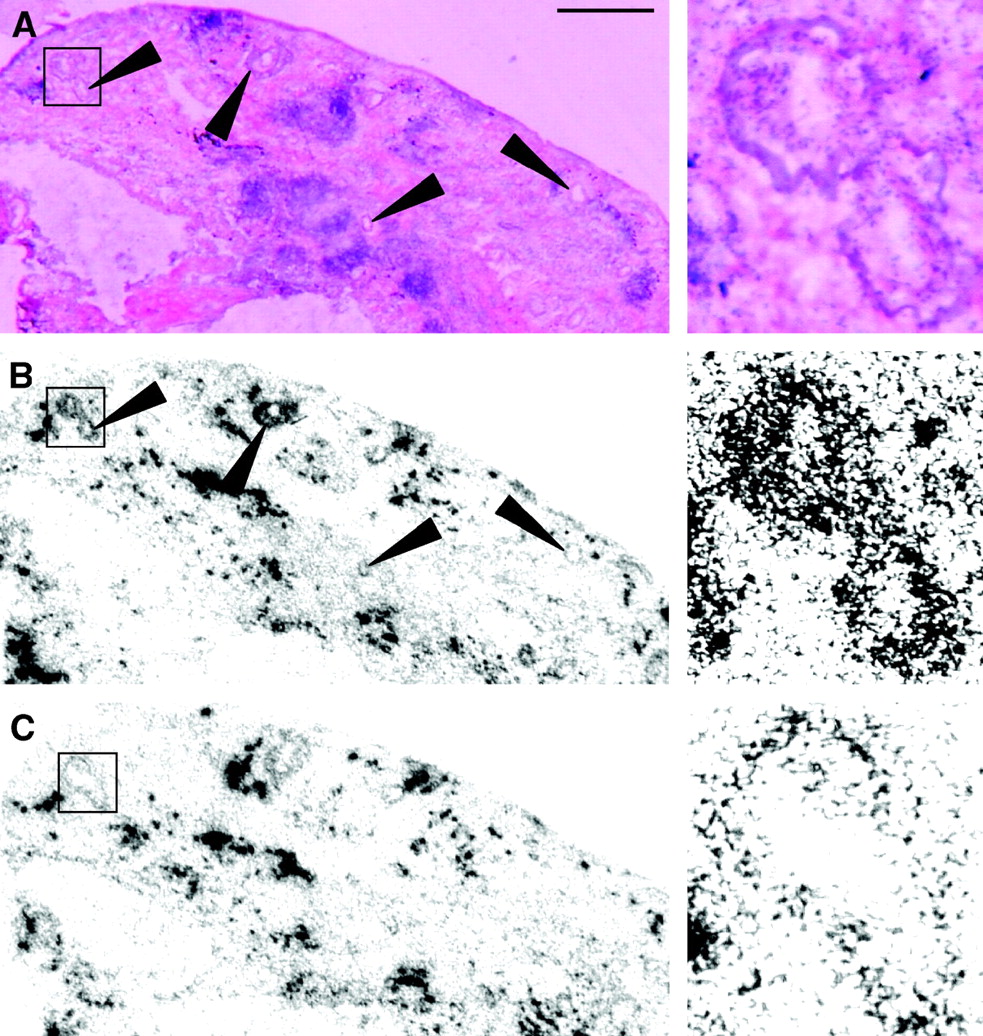
Autoradiography from fibrotic lung sample, with enlarged views of boxed areas shown on right. (A) Hematoxylin- and eosin-stained section showing blood vessels (arrowheads). (B) Autoradiogram showing total binding of [125I-Tyr3]octreotide. Medium-sized vessels are clearly labeled (arrowheads). Weak labeling may also be seen in some lymphoid aggregates. (C) Autoradiogram showing strong, nonspecific binding that remains in presence of octreotide (1 μmol/L) in several elements of lung. Bar = 1 mm.
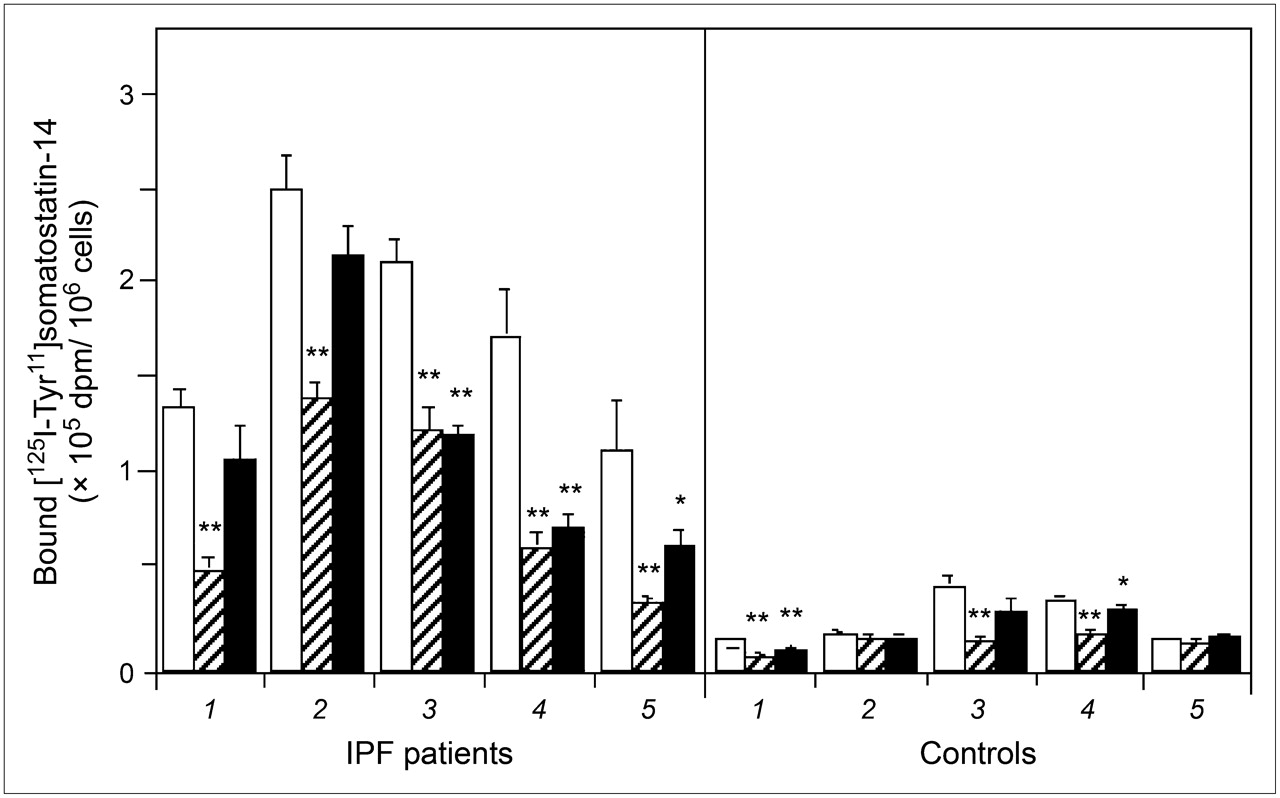
On cultures of lung fibroblasts, the in vitro [125I-Tyr11]somatostatin-14 binding assay found that fibroblasts from every IPF patient exhibited both somatostatin-sensitive and octreotide-sensitive binding sites but that the amount of somatostatin-14–sensitive sites was 5-fold higher, and the amount of octreotide-sensitive sites 10-fold higher, on IPF fibroblasts than on control fibroblasts (Fig. 3). Somatostatin-14–sensitive and octreotide-sensitive [125I-Tyr11]somatostatin-14 binding sites were observed on fibroblasts from 3 and 2 control patients, respectively.

Inhibition of [125I-Tyr11]somatostatin-14 binding to cultured lung fibroblasts from IPF and control patients by somatostatin-14 and octreotide. Fibroblasts were incubated for 1 h at 37°C with [125I-Tyr11]somatostatin-14 alone (0.2 nmol/L, white bars) or in presence of somatostatin-14 (10−6 mol/L, hatched bars) or octreotide (10−6 mol/L, black bars). For each patient, results are expressed as mean ± SEM of 4–6 determinations of bound disintegrations per minute (dpm) normalized to 106 cells. *P < 0.05 vs. [125I-Tyr11]somatostatin alone. **P < 0.01 vs. [125I-Tyr11]somatostatin alone.
DISCUSSION
The normal human lung expresses low levels of somatostatin receptors (19) and, in vivo, shows no increased uptake of 111In-octreotide on scintigraphy (21–23). The in vivo uptake of 111In-octreotide is determined predominantly by sst2 (24).
The present data indicate that increased sst2 binding sites are present in the lung in patients with pulmonary fibrosis (IPF and SSc), as evidenced by in vivo increased uptake of 111In-octreotide. The data also indicate that lung uptake correlates with altered findings on lung function tests, with the intensity of alveolitis, and with the HRCT fibrosis score. The receptor autoradiography findings suggest that vascular structure receptors are prominent sites of binding, and the in vitro results indicate that lung fibroblasts express somatostatin receptors.
Increased uptake of 111In-octreotide in the lung has been demonstrated in vivo in patients with distinctly different lung diseases, either inflammatory (e.g., sarcoidosis (22) or Langerhans cell granulomatosis (23)), tumoral (e.g., cancer) (25), or fibrotic (e.g., fibrotic pleural plaques (26) or radiation-induced fibrosis (27)). Interestingly, other studies have reported that uptake of 111In-octreotide in sarcoidosis lesions and rheumatoid arthritis lesions was related to the activity of the disease, with lower uptake of 111In-octreotide after successful therapy in accordance with clinical and radiologic findings (24,28,29).
Although the exact mechanisms of increased 111In-octreotide uptake remain undetermined for many conditions, 3 different mechanisms may be involved: lung infiltration with inflammatory cells, increased expression of somatostatin receptors by fibroblasts and other cells resident in the lung, and increased expression of somatostatin receptors by blood vessels. The present data suggest that all 3 mechanisms participate in the constant increase in 111In-octreotide uptake measured in all patients with IPF and in the 4 of 6 patients with SSc. Indeed, the intensity of 111In-octreotide uptake in vivo correlated positively with the total number of macrophages and neutrophils measured in BAL fluid, an index of inflammatory cell infiltration in the lung. Previous data have indicated that macrophages and lymphocytes express a somatostatin receptor (30,31). The present data indicate, in addition, that isolated lung fibroblasts cultured from IPF patients specifically bind somatostatin in vitro and that this binding is both somatostatin and octreotide sensitive.
In addition, the present autoradiographic data point out that blood vessels are a prominent site of [125I-Tyr3]octreotide binding, although increased vascularity is recognized in pulmonary fibrosis (32) and may have significantly contributed to the observed increase in 111In-octreotide uptake in patients. Reubi et al. (29,33) previously reported increased expression of somatostatin receptors in intestinal vessels of patients with inflammatory bowel disease and in the whole vessel wall of patients with active rheumatoid arthritis. The increased expression of somatostatin receptors in vessels suggests an active involvement of this peptide and a possible influence on the pathophysiology of the inflammatory process and neovascularization.
The finding that 111In-octreotide uptake in the lung was lower in patients with SSc than in patients with IPF could be related to a lesser proportion of fibrosis and a greater proportion of ground-glass attenuation in SSc lung patients than in IPF patients, as previously shown by Desai et al. (34). This hypothesis is supported by the observation that octreotide uptake in the lung correlated with the fibrosis HRCT score but not with the ground-glass score in the present IPF patients. Whether this difference is explained by the different histopathologic patterns usually observed in the 2 conditions, namely “usual interstitial pneumonia” in IPF and “nonspecific interstitial pneumonia” in SSc, remains to be elucidated.
Our preliminary study had some limitations: relatively few patients were included. Because surgical lung biopsy is not systematically indicated to make a diagnosis of IPF, in vitro and in vivo studies were not both performed on the same patient. In our series, IPF was diagnosed according to the criteria in the ATS/ERS consensus statement (1). Autoradiography was performed on lung samples from patients who were not imaged with octreotide, except one. However, these patients had IPF of the typical histopathologic pattern and were fully representative of IPF patients.
CONCLUSION
The present preliminary results confirmed the increased uptake of 111In-octreotide in (mainly idiopathic) pulmonary fibrosis. Lung uptake correlates with alterations in lung function and with the intensity of alveolitis and seems to be related to the severity of lung fibrosis. Our study suggests, in addition, that blood vessels are prominent sites of [125I-Tyr3]octreotide binding in pulmonary fibrosis and that isolated lung fibroblasts obtained from IPF patients express somatostatin receptors.
Whether the antifibrotic properties of octreotide might represent a therapeutic option in patients with lung fibrosis remains to be evaluated. Ongoing preclinical studies of lung fibrosis will soon provide us with further information.
Acknowledgments
We gratefully acknowledge Prof. Pascal Merlet for expert discussions and helpful comments and Dr. François Rouzet for assistance.
Footnotes
-
COPYRIGHT © 2006 by the Society of Nuclear Medicine, Inc.
References
- Received for publication December 20, 2005.
- Accepted for publication April 21, 2006.





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Visualisation of interstitial lung disease by molecular imaging of integrin {alpha}v{beta}3 and somatostatin receptor 2
- Type I collagen-targeted PET probe for pulmonary fibrosis detection and staging in preclinical models
- Imaging Pulmonary Inflammation
- Idiopathic pulmonary fibrosis
- Octreotide treatment of idiopathic pulmonary fibrosis: a proof-of-concept study
- A View on Imaging in Drug Research and Development for Respiratory Diseases
- 68Ga-DOTANOC PET/CT Allows Somatostatin Receptor Imaging in Idiopathic Pulmonary Fibrosis: Preliminary Results
- Activation of somatostatin receptors attenuates pulmonary fibrosis