


The term metabolic trapping means intracellular enzymatic conversion of a radiotracer into a metabolic product that is trapped and concentrated in key tissues. In a classic paper selected by the editors of JNM for the 60th anniversary edition, Brian Gallagher et al. reported on the dominant biochemical features of 18F-FDG metabolism in vivo and linked 18F-FDG uptake unequivocally to hexokinase-based metabolic trapping as a prime example of the general concept of the metabolic trap as a principle of radiopharmaceutical design (1).
In the last 20 years, there has been a revolution in the practice of clinical nuclear medicine, based on the implementation and acceptance of two developments that are now part of modern medical practice. The first was the widespread availability of 18F-FDG for reimbursed clinical studies. The second was the development of commercially supported PET units, which can be used in fusion with CT for practical whole-body imaging. Approximately 2.2 million 18F-FDG PET/CT studies were performed in the United States in 2019, of which 90% were oncology studies (Fig. 1) (2).
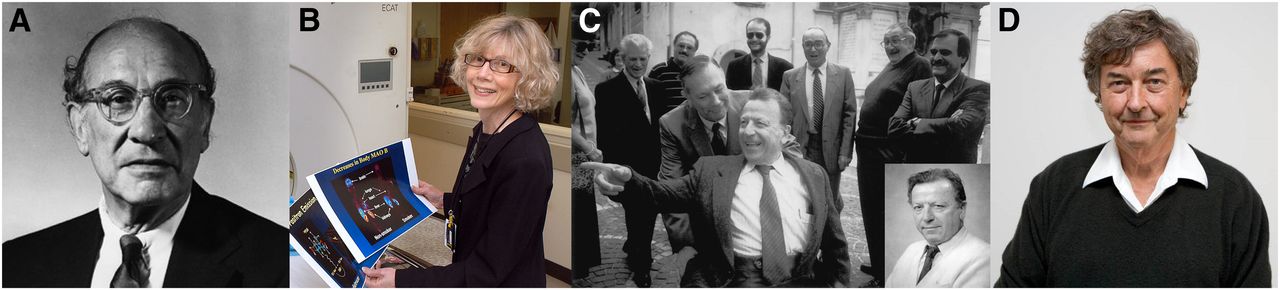
18F-FDG PET/CT is a revolutionary approach in oncology, as well as other fields. These 4 revolutionaries are arguably the individuals most responsible for benefits we see today from modern PET imaging in oncology: Louis Sokoloff, for the 2 deoxyglucose method for regional tissue glucose metabolism (A); Joanna Fowler, for 18F-FDG radiochemistry (B); Giovanni Di Chiro, for metabolic imaging of tumor metabolism in human tumors (C); and Michael Phelps, for PET imaging and development (D).
Sokoloff introduced the concept of metabolic trapping for regional brain metabolism using 2-deoxyglucose, a glucose analog (3). Sokoloff realized that postmortem use of the radiotracer 14C-2-deoxyglucose and quantitative radiographic methods would provide high-resolution tomographic information about rat brain glucose metabolism, including critical brain subregions. Following quickly from this seminal study, the team of Joanna Fowler and Alfred Wolf at Brookhaven National Laboratory developed 18F-fluorinated deoxyglucose, that is, 18F-FDG, as a metabolically trapped PET imaging radiotracer suitable for use in patients (4). 18F-FDG was first used clinically in 1977 to image the brain (5).
The value of Gallagher’s work lies in the holistic approach he used for the in vivo pharmacology of 18F-FDG. For 18F-FDG, it was known that the basis of tissue trapping was enzymatic phosphorylation by the hexokinase enzyme at an early stage in glycolysis (the conversion of glucose to pyruvate/lactate, with the production of metabolites for use as building blocks for important structural cell components, that is, DNA and RNA, and energy, in the form of adenosine triphosphate).
18F-FDG accumulates in tissues as the FDG-6 phosphate because the lack of an oxygen molecule at position 2 of the 18F-FDG structure makes the product of hexokinase phosphorylation, FDG-6 PO4, a poor substrate for subsequent metabolism in the glycolytic chain. Thus, there is progressive, time-dependent accumulation of 18F-FDG in the tissue, which correlates with glucose tissue metabolism. Gallagher observed that the brain and heart had the greatest uptake and prolonged retention in comparison to other tissue such as liver, lungs, and kidney. He documented that 18F-FDG uptake was proportional to the expression of hexokinase enzyme in these tissues, associated with low dephosphorylation (low glucose-6 phosphatase) in tissues with high uptake (Fig. 2). Gallagher also noted a second highly favorable pharmacokinetic property: unlike glucose, 18F-FDG is rapidly excreted by the kidneys, improving image contrast. 18F-FDG is secreted mostly intact into the urine.
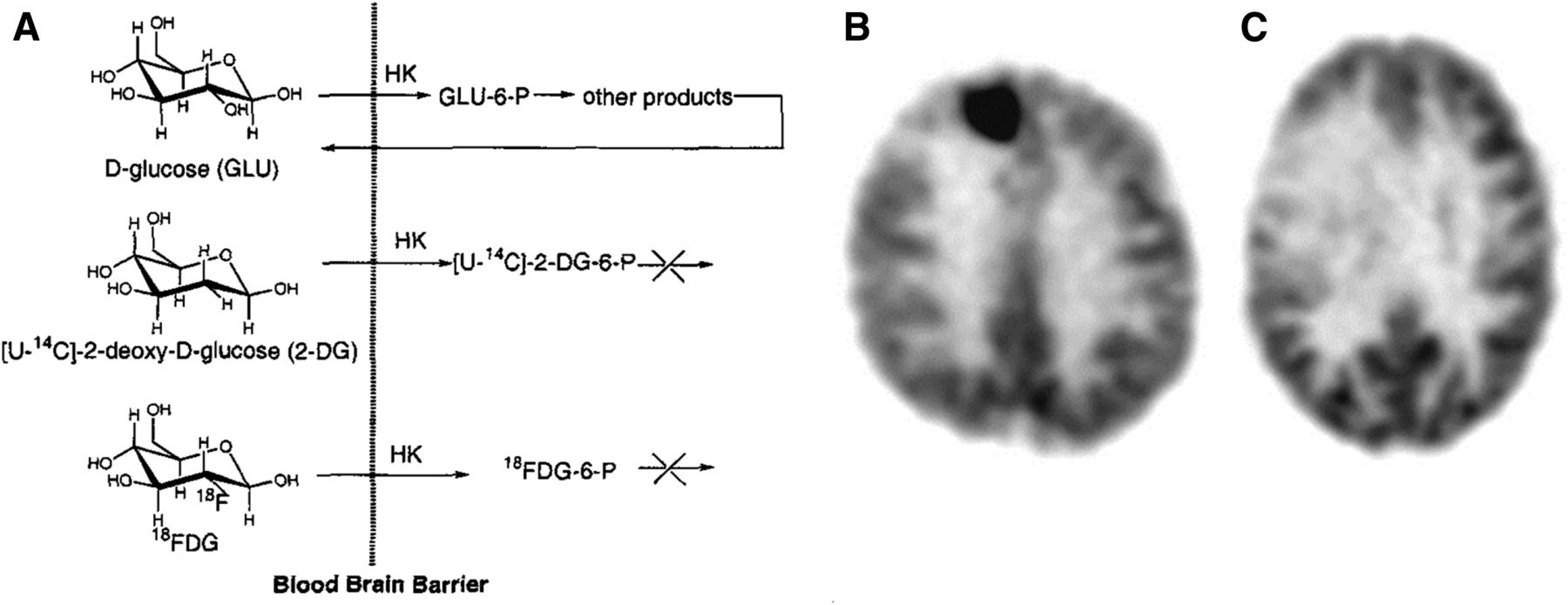
(A) Comparison of transport of 18F-FDG, 2-deoxyglucose (DG), and glucose, showing metabolic trap (7). Hexokinase (HK) phosphorylates both glucose and 18F-FDG at position 6. Both 2-DG and 18F-FDG lack oxygen (as OH) at position 2 and, consequently, are metabolically trapped. (B and C) In 18F-FDG PET imaging of brain tumors, 18F-FDG uptake is predictive of tumor grade: glioblastoma multiforme (B) and grade II oligodendroglioma (C).
In 1927, Otto Warburg reported that cancer cells, unlike normal tissues, had strong reliance on glycolysis—the metabolism of glucose to lactate to produce energy, even in the presence of abundant oxygen. This aerobic glycolysis, or the Warburg effect, was energetically very inefficient. But cancer cells’ specialized metabolism manages particular problems created by the rapidly proliferating cell. Aerobic glycolysis not only satisfies a macromolecular requirement for rapidly proliferating tissues, but also provides metabolites that detoxify waste products that would otherwise disrupt redox state and damage the growing cancer cell.
The first person to pioneer the clinical use of 18F-FDG systematically in human tumors was Giovanni Di Chiro, a neuroradiologist who studied 18F-FDG imaging of human glioblastoma. Early PET images using 18F-FDG are shown in Figure 2. Di Chiro was the first to show that 18F-FDG uptake is increased in higher-grade, poor-prognosis tumors and that metabolic tumor response is an effective predictor of treatment response, tumor recurrence, and tumor transformation (6). These features form the foundation of metabolic imaging of human tumors.
18F-FDG discovery and development is a fascinating story of the fortuitous match between medical need and in vivo radiopharmacology that forms the foundation for Gallagher’s remarkably prescient paper on 18F-FDG and the metabolic trap. Driven primarily by clinical benefit for oncology, 18F-FDG is the single most valuable radiopharmaceutical drug in modern nuclear medicine practice.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
- © 2020 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication June 18, 2020.
- Accepted for publication June 26, 2020.




{kind=link}
{kind=link}