


Abstract
99mTc-macroaggregated albumin (99mTc-MAA) scanning precedes radioembolization of the liver to detect extrahepatic shunting to the lung or gastrointestinal tract. Despite strict preventive measures in the production of 99mTc-MAA and in scanning protocols, the images frequently show a gastric concentration of free 99mTc-pertechnetate, hindering accurate evaluation of the gastroduodenal region. Our aim was to evaluate whether oral administration of sodium perchlorate (NaClO4) before 99mTc-MAA scanning will improve its accuracy by blocking free 99mTc-pertechnetate gastric uptake. Methods: In 144 patients, 171 diagnostic hepatic angiograms combined with a 99mTc-MAA scan were performed; 86 angiograms were performed after oral administration of NaClO4, and 85 were performed without this premedication. Clinical follow-up, esophagogastroduodenoscopy, and angiography served as reference standards. Results: 99mTc-MAA studies showed tracer uptake in the gastric region of 25 patients who did not receive NaClO4. The uptake was interpreted as a free 99mTc-pertechnetate concentration in 21 studies and as a 99mTc-MAA accumulation in 4 studies. In 5 patients with a free 99mTc-pertechnetate concentration, aberrant vessels were detected in angiographic reexamination, and 3 patients developed gastrointestinal ulcer. In 7 studies, gastric findings viewed pretherapeutically as free 99mTc-pertechnetate were retrospectively classified as equivocal. Of the patients receiving NaClO4, 2 showed gastric accumulation of 99mTc-MAA but no equivocal or free 99mTc-pertechnetate. Oral administration of NaClO4 increased the negative predictive value and accuracy of the test concerning the detection of gastric perfusion from 68% and 69%, respectively, to 93% and 94%, respectively. Conclusion: Oral administration of NaClO4 before the test angiogram with 99mTc-MAA resulted in effective avoidance of free 99mTc-pertechnetate concentration and, consequently, of equivocal findings in the gastroduodenal region. This technique increased test accuracy and reporter confidence, saved time in reviewing the angiograms, and can improve treatment planning and reduce therapeutic side effects.
Scanning with 99mTc-macroaggregated albumin (99mTc-MAA) generally precedes radioembolization of the liver to detect extrahepatic shunting to the lung or gastrointestinal tract (1). To avoid dissociated 99mTc-pertechnetate, 99mTc-MAA should be prepared under strict quality control assessments (2–4) and scintigraphy should be performed within 1 h of the radiopharmaceutical injection. Despite the preventive measures, a gastric concentration of free 99mTc-pertechnetate is frequently seen in 99mTc-MAA images and can hinder the accurate evaluation of the gastroduodenal region. Sodium perchlorate (NaClO4) has a great affinity for the sodium–iodine symporter and is safely used for prophylaxis of iodine-induced hyperthyroidism due to iodinated contrast agents (5–7). Our aim was to evaluate whether oral administration of NaClO4 before 99mTc-MAA scanning will improve its accuracy and diagnostic confidence by facilitating the detection of gastric shunting.
MATERIALS AND METHODS
Patients
In 144 patients with primary and secondary hepatic malignancies, 171 diagnostic hepatic angiograms with 99mTc-MAA were performed. The mean and median ages of the patients were 63 y and 65 y, respectively (range, 34–86 y; 50 women [34.7%] and 94 men [65.3%]). The patients were categorized into 2 subgroups. The first subgroup consisted of the chronologic first 72 patients, who did not receive NaClO4 before 99mTc-MAA assessment, undergoing a total of 85 diagnostic hepatic angiograms combined with administration of 99mTc-MAA (test angiogram). The second subgroup consisted of the next 72 patients (86 angiograms), who did receive NaClO4 before the test angiogram. Written informed consent was given by each participant before 99mTc-MAA assessment.
Procedures
A preparation kit (GE Healthcare Buchler) was used for the labeling of 99mTc-pertechnetate with macroaggregated human albumin. Quality control was performed according to the instructions of the manufacturer to assess particle size (10–100 μm), radiochemical purity (>95%), and aggregate stability (≤5 h). To avoid a gastric concentration of free 99mTc-pertechnetate, the test angiograms of subgroup 2 were performed after oral administration of 600 mg of NaClO4. Prophylactic embolization of all visible extrahepatic arteries, including the gastroduodenal and right gastric arteries, was performed as close as possible to the intended time of radioembolization to avoid the revascularization of these vessels (maximum interval, 10 d). During the angiograms, under blood flow control and depending on the anatomy of the liver, about 185 MBq (5 mCi) of 99mTc-MAA were administered intraarterially into the common hepatic artery in 3 tests (1.8%), into the proper hepatic artery in 70 tests (41%), into the right and left hepatic arteries separately in a single session in 57 tests (33%), only into the right hepatic artery in 24 tests (14%), only into the left hepatic artery in 15 tests (9%), and superselectively into segmental arteries in 2 tests (1.2%). Whole-body anterior and posterior scanning were performed within 1 h of 99mTc-MAA injection with a dual-head γ-camera (E.Cam; Siemens) to calculate the percentage of liver-to-lung shunting and was followed by planar scintigraphy and SPECT of the upper abdomen to rule out extrahepatic gastrointestinal shunting. Additionally, SPECT/CT using a dual-detector γ-camera with a mounted 2-row CT scanner (Symbia T2; Siemens) was performed in the last 90 studies to allow better evaluation of intra- and extrahepatic tracer accumulations. Apart from the introduction of SPECT/CT, during the study no changes occurred in our angiographic and imaging protocols (including the time from injection of 99mTc-MAA); in the preparation of 99mTc-MAA; or in the respective quality control measures.
Image Interpretation
All images were reviewed retrospectively by 2 experienced nuclear medicine physicians. Gastric tracer uptake was interpreted visually as a free 99mTc-pertechnetate concentration or as a 99mTc-MAA accumulation. Diffuse gastric mucosal uptake, considerably less intense than hepatic tracer uptake and usually accompanied by thyroid uptake, suggested a free 99mTc-pertechnetate accumulation. Focally increased activity in the gastric region was considered a 99mTc-MAA accumulation, indicating true gastric shunting. Gastric uptake that was initially (in the clinic) viewed as free 99mTc-pertechnetate was retrospectively classified as equivocal if definitive indicators for free 99mTc-pertechnetate etiology—thyroid uptake and homogeneity of gastric uptake (Fig. 1)—were absent.
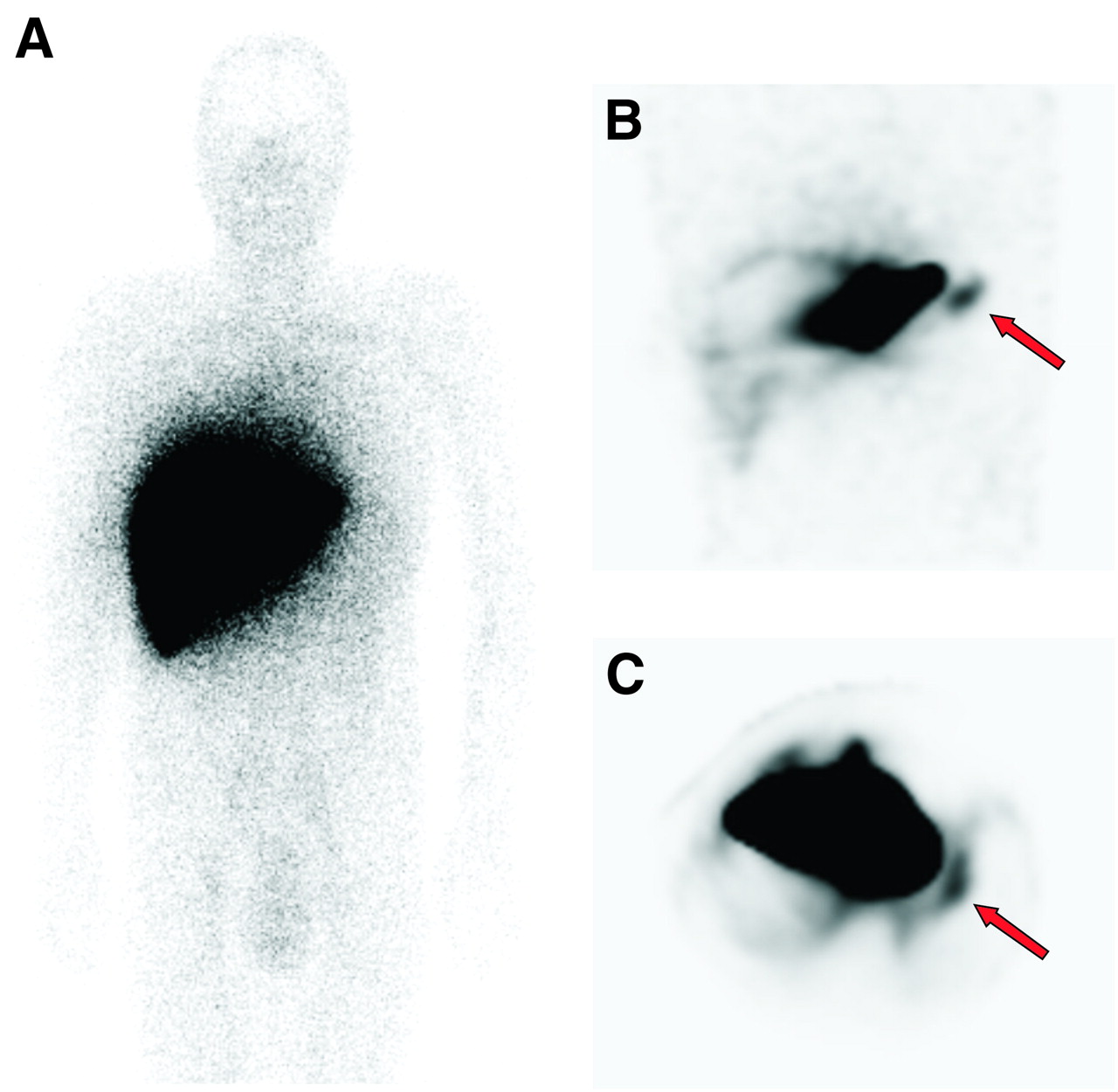
Whole-body image (A) and coronal (B) and transaxial (C) SPECT images of subgroup 1 patient with colorectal cancer and hepatic metastases whose gastric uptake was viewed pretherapeutically as free 99mTc-pertechnetate (arrows). Finding was retrospectively classified as equivocal because of absence of thyroid uptake. Patient developed posttherapeutic gastrointestinal ulcer.
Reference Standard and Data Analysis
Angiographic scans of patients showing extrahepatic accumulation in their 99mTc-MAA images were reviewed to find aberrant vessels. Possible underlying arteries were reassessed for coil embolization in a repeated angiography followed by a repeated 99mTc-MAA scan to rule out any remaining extrahepatic shunting. Moreover, a routine angiographic reassessment was performed for all patients just before the start of treatment with 90Y microspheres. For all patients receiving radioembolization, postintervention follow-up consisting of physical examination and laboratory testing was performed on days 2, 14, 30, 60, 90, and up to 1 y (if the patients were alive). Additionally, esophagogastroduodenoscopy was performed for all patients with gastrointestinal complaints. The results of follow-up and esophagogastroduodenoscopy examinations, along with angiographic findings, served as the reference standard for gastric shunting. To make the results of the 2 subgroups comparable, SPECT/CT findings served as only a part of the reference standard and were not considered for data analysis. For both subgroups, the reference standard was used in calculations of the sensitivity, specificity, positive predictive value, negative predictive value, and accuracy of 99mTc-MAA scanning in the detection of gastric shunting. For statistical analysis, equivocal findings were considered to indicate a gastric concentration of free 99mTc-pertechnetate. Finally, the possible significance of NaClO4 in this regard was investigated applying the Fisher exact test.
RESULTS
First Subgroup
99mTc-MAA images of the first subgroup demonstrated extrahepatic tracer uptake in the gastric region in 25 studies (29%). The uptake was interpreted pretherapeutically as a free 99mTc-pertechnetate gastric concentration in 21 studies, 7 of which were rated retrospectively as equivocal and 4 as a 99mTc-MAA gastric accumulation (Table 1). Thyroid uptake was present in all but 5 studies, 2 of which showed gastric tracer uptake rated as a free 99mTc-pertechnetate gastric concentration.
Retrospective Interpretation of Gastric Uptake in 99mTc-MAA Images
Review of the angiograms revealed a possible aberrant vessel in 1 of the 4 patients with 99mTc-MAA deposition in the gastric region. However, because of technical problems, the suspected artery could not be embolized and 90Y microspheres were injected from a more distal catheter position without embolization of the aberrant artery. But the treatment had to be stopped because of reflux of the microspheres, and the patient developed a gastrointestinal ulcer 1 wk later. In another patient with an apparent 99mTc-MAA accumulation in the gastric region, review of the angiographic scans proved him to have an intrahepatic accumulation in only the second segment of his very large liver, not distinguishable from the stomach in 99mTc-MAA images. The remaining 2 patients with a 99mTc-MAA gastric accumulation were not treated because no underlying arteries were found on review of the test angiograms or on repeated angiographies.
Of 21 patients with gastric uptake interpreted as a free 99mTc-pertechnetate accumulation, aberrant vessels to the gastric region were detected and coiled in the routine angiographic reexamination just before the start of therapy in 5 patients, whereas 3 patients developed a gastrointestinal ulcer during follow-up. 99mTc-MAA images were retrospectively classified as equivocal in 4 of these 8 patients, 1 of which was due to the absence of concordant thyroid uptake (Table 1).
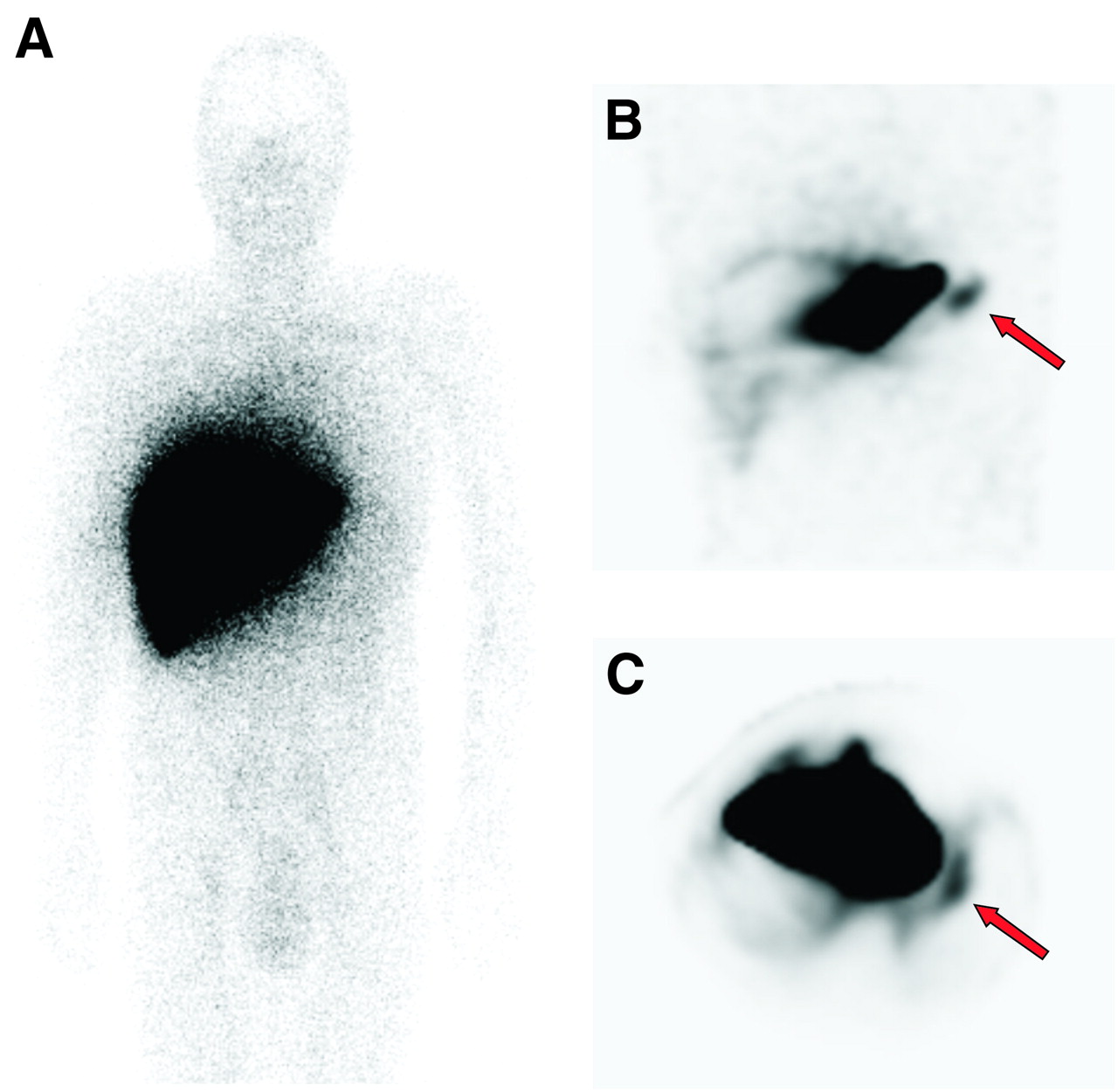
Three patients with a free 99mTc-pertechnetate gastric concentration were excluded from radioembolization because of contraindications, and the remaining patients (10/21) underwent treatment without experiencing any relevant side effects (Fig. 2).

Whole-body image (A) and coronal (B) and transaxial (C) SPECT images of subgroup 1 patient with hepatocellular carcinoma who experienced no side effects after treatment. Gastric finding was interpreted as free 99mTc-pertechnetate (arrows).
In 11 patients, angiographic reexaminations revealed gastric shunting despite an unremarkable 99mTc-MAA scan, whereas 2 patients developed gastrointestinal ulcer and 9 patients were excluded from treatment.
Four patients of the first subgroup underwent SPECT/CT in the first week of its use in our institution. All 4 of these patients showed gastric uptake on SPECT/CT images, and the uptake was interpreted at the time as a free 99mTc-pertechnetate concentration. However, 1 of these patients was among those who developed a posttherapeutic gastrointestinal ulcer, and surgical detection of microspheres in the ulcer strongly disputed the interpretation of the gastric finding as a free 99mTc-pertechnetate concentration.
Altogether, 14 patients of the first subgroup were excluded from treatment with 90Y microspheres because of undetected aberrant arteries despite an extrahepatic 99mTc-MAA accumulation in the stomach (2/14) or other parts of the gastrointestinal system (2/14), liver-to-lung shunting higher than 20% (5/14), deteriorated liver function (2/14), or lack of tumoral 99mTc-MAA accumulation (3/14).
Second Subgroup
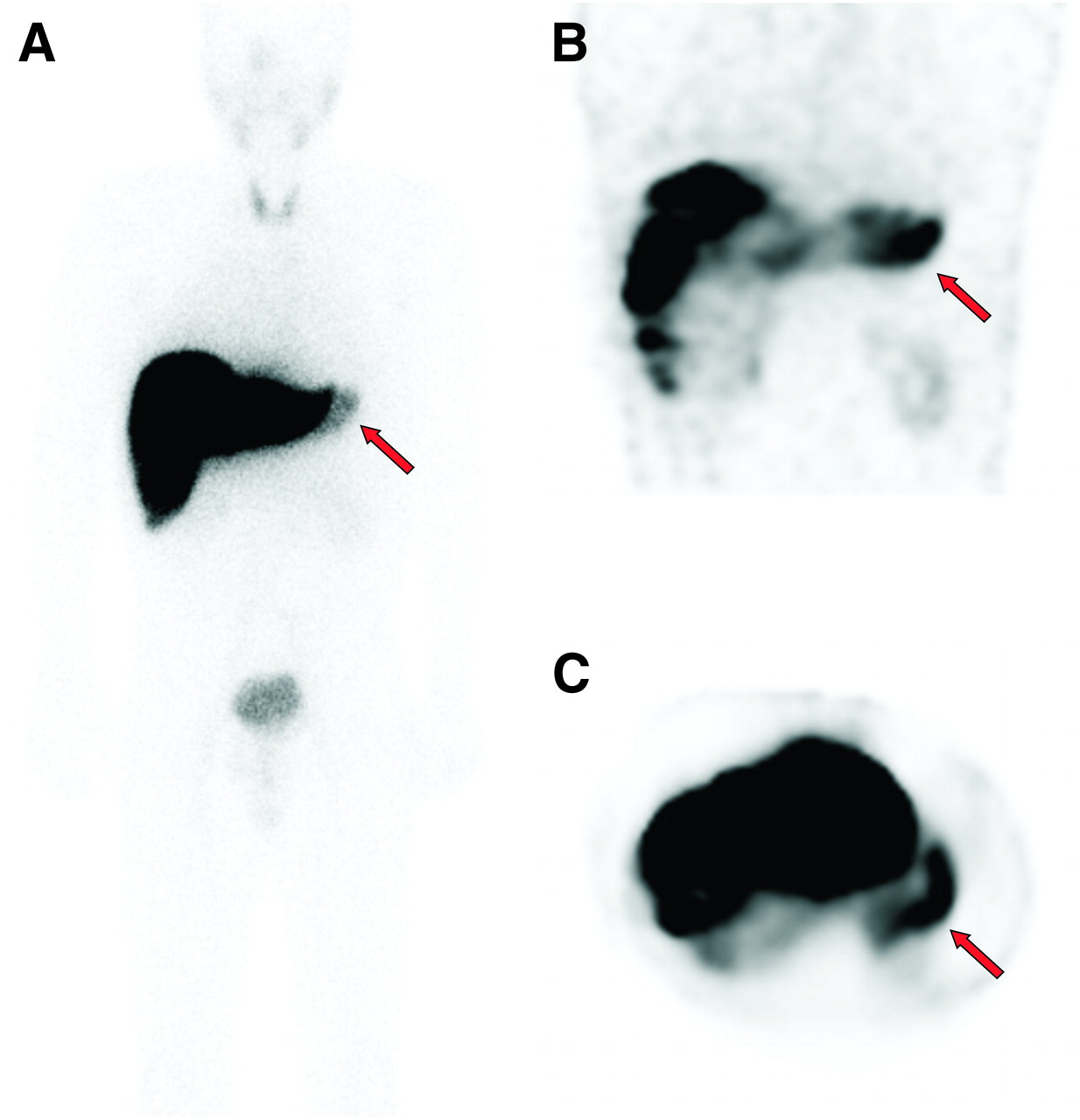
In the second subgroup, an extrahepatic accumulation in the gastric region was observed in only 2 SPECT studies, whereas SPECT/CT images revealed a gastric accumulation in another 5 studies (Fig. 3). The angiographic scans of the second subgroup were reviewed in the same manner as for the first subgroup. Radioembolization was performed on 3 of these 7 patients after an unremarkable 99mTc-MAA test after the embolization of possible aberrant vessels, whereas in 2 patients with evident underlying vessels on test angiograms, the vessels were coiled without any further 99mTc-MAA examination. None of these 5 patients developed gastrointestinal side effects during follow-up. In the other 2 patients with a 99mTc-MAA gastric accumulation, underlying arteries were found neither on review of the test angiograms nor on repeated angiography despite a persistent accumulation seen on SPECT/CT images. These patients were not treated. In the second subgroup, no gastric finding was interpreted as free 99mTc-pertechnetate concentration or as equivocal (8).
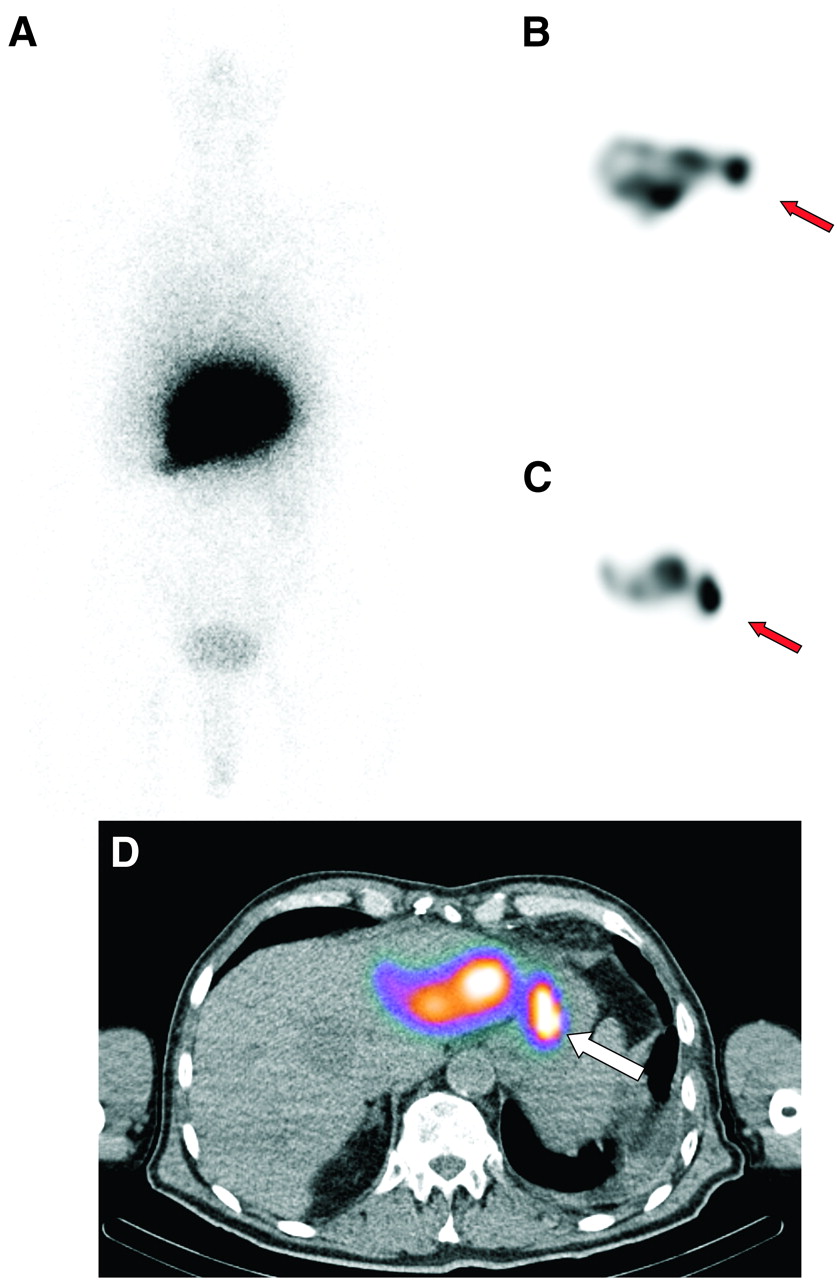
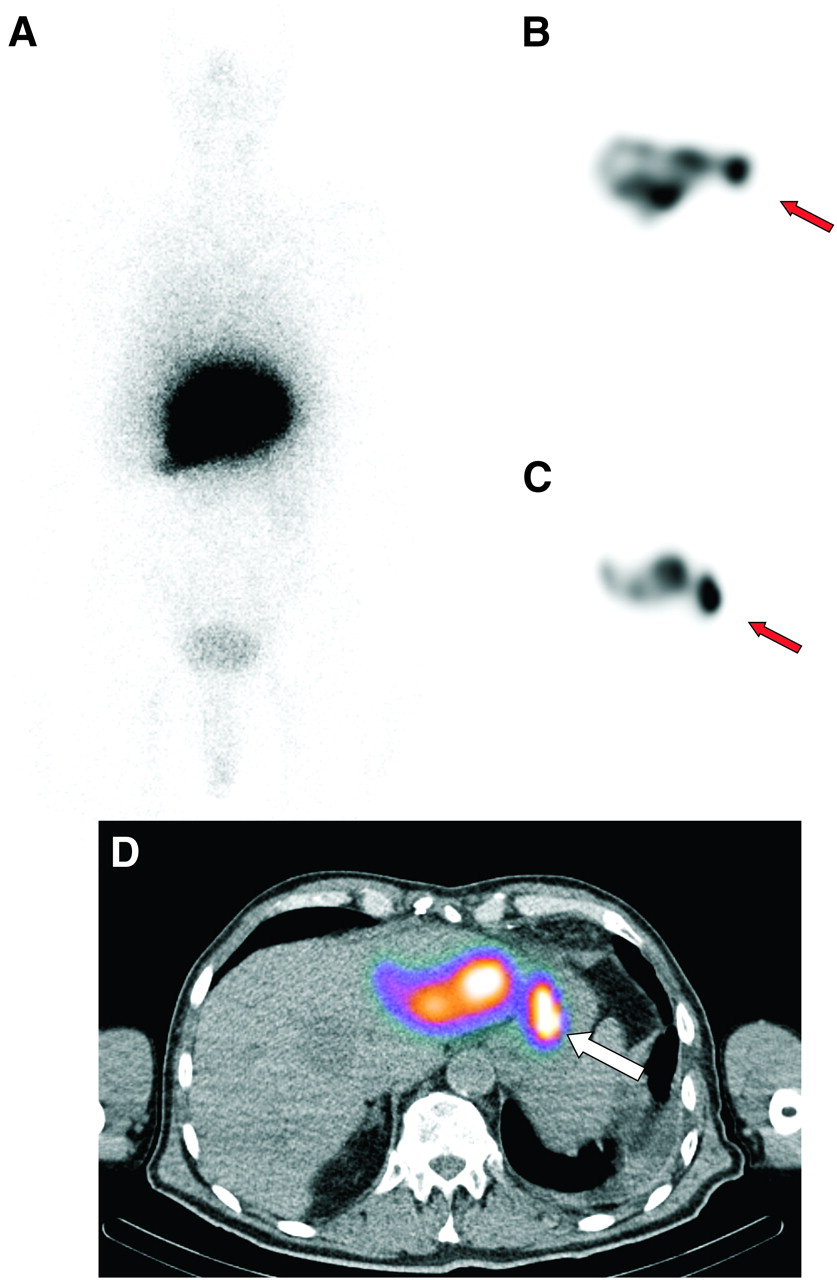
Whole-body image (A), coronal (B) and transaxial (C) SPECT images, and SPECT/CT image (D) of subgroup 2 patient with hepatocellular carcinoma who showed gastric accumulation of 99mTc-MAA. Radioembolization was performed after embolization of aberrant vessels, without any relevant side effects. Extrahepatic uptake (arrows) was optimally localized using SPECT/CT.
Subgroup Comparison
The sensitivity of 99mTc-MAA scanning in detection of gastric shunting was only 12% in the first subgroup but was raised to 28% in the second subgroup as a result of complete elimination of any free 99mTc-pertechnetate gastric concentration. Oral administration of NaClO4 before 99mTc-MAA assessment significantly increased the negative predictive value and accuracy of the test concerning the detection of gastric perfusion from 68% and 69%, respectively, to 93% and 94%, respectively (P < 0.001). The results of the 2 subgroups are summarized in Table 2.
99mTc-MAA in Diagnosis of Gastric Shunting
DISCUSSION
Radioembolization of the liver with 90Y-microspheres is a novel catheter-based liver-directed modality for treating primary and metastatic liver cancers. An angiographic evaluation combined with 99mTc-MAA scanning generally precedes treatment to define the vascular anatomy of the liver, to assess the vascularity of the hepatic tumors or metastases, and to detect extrahepatic shunting to the lung or gastrointestinal tract (1). Prophylactic embolization of all extrahepatic vessels is also performed to avoid extrahepatic deposition of 90Y-microspheres (9). These procedures should be performed as close as possible to the intended time of radioembolization, considering the quick revascularization of these vessels (9). A reassessment arteriogram is also required just before the treatment to ensure that such revascularization has not occurred (6). However, in nearly 4% of radioembolization cases, microspheres can be transported into the vascular territory of the gastrointestinal organs, resulting in severe damage (10). This occurs when the microspheres are inadvertently injected into small arteries supplying the gut, are misinterpreted as suppliers of the left lobe of the liver, or remain undetected in pretherapeutic tests. Reported complications include gastrointestinal ulceration or bleeding, gastritis or duodenitis, cholecystitis, pancreatitis, and radiation pneumonitis (10–18).
99mTc-pertechnetate concentrates in the brain, thyroid, salivary glands, and gastric mucosa, mediated by plasma membrane glycoprotein sodium–iodine symporter (19,20). To avoid dissociated 99mTc-pertechnetate, 99mTc-MAA should be prepared under strict quality control assessments and scintigraphy should be performed within 1 h of 99mTc-MAA injection. However, 99mTc-MAA scans frequently show accumulation of free 99mTc-pertechnetate in radioembolization candidates, hindering accurate evaluation of the gastric region. In such cases, a visual distinction between a free 99mTc-pertechnetate concentration and true gastric 99mTc-MAA shunting may be difficult, as seen in the 7 of our patients who had to be retrospectively classified as equivocal (Table 1). This limitation considerably reduces diagnostic confidence. Furthermore, gastric accumulation of 99mTc-MAA can remain unrecognized in the presence of gastric free 99mTc-pertechnetate, as seen in the 4 patients of our cohort with a free 99mTc-pertechnetate concentration, 3 of whom had aberrant vessels found on routine angiographic reexamination whereas 1 developed a posttherapeutic gastrointestinal ulcer.
Perchlorate anion can inhibit sodium–iodine and has been successfully and safely used for prophylaxis of iodine-induced hyperthyroidism before administration of iodinated contrast agents (5–7).
As demonstrated by our second subgroup, without a single equivocal finding, a gastric free 99mTc-pertechnetate concentration can effectively be avoided by oral administration of NaClO4 before the test angiogram. This step considerably facilitates the detection of a gastric accumulation of 99mTc-MAA and could significantly increase the negative predictive value and accuracy of the test.
The low overall sensitivity of 99mTc-MAA scintigraphy in detecting extrahepatic uptake may be increased to up to 100% using SPECT/CT methodology (8,21). However, the sensitivity of SPECT/CT is completely dependent on the absence of gastric free 99mTc-pertechnetate. Ruling out 99mTc-MAA gastric shunting will be impossible in the presence of a free 99mTc-pertechnetate accumulation even when SPECT/CT is applied, as observed in 1 of our 4 patients in the first subgroup who developed posttherapeutic gastrointestinal ulcer.
This study had some limitations. Because a SPECT/CT system was not available at the time of the 99mTc-MAA assessments of nearly half our patients, and in order to make the results of the 2 subgroups comparable, we did not consider the SPECT/CT findings in the data analysis. These data could have dramatically enhanced the 99mTc-MAA test sensitivity, as has already been shown by other studies (8,21). However, the use of SPECT/CT is not expected to replace the need for NaClO4 administration to achieve a confident evaluation of the gastric region. In addition, the chronologic division of our 2 subgroups may also be statistically influential because of the improvement in angiographic techniques over time. The other principal limitation of this study was its retrospective nature and the absence of paired comparisons, which will inevitably affect the strength of conclusions.
CONCLUSION
The administration of oral sodium perchlorate before 99mTc-MAA assessment results in effective avoidance of a gastric concentration of free 99mTc-pertechnetate and, consequently, of equivocal extrahepatic findings in the gastric region. These benefits increase test sensitivity and accuracy and save time in reviewing the angiograms. Hence, the oral administration of NaClO4 should be an integral part of patient preparation directly before angiography in order to improve treatment planning and reduce therapeutic side effects.
DISCLOSURE STATEMENT
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734.
Acknowledgments
No potential conflict of interest relevant to this article was reported.
Footnotes
↵* Contributed equally to this work.
- © 2011 by Society of Nuclear Medicine
REFERENCES
- Received for publication September 27, 2010.
- Accepted for publication April 13, 2011.





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- A Prospective Study of Quantitative SPECT/CT for Evaluation of Lung Shunt Fraction Before SIRT of Liver Tumors
- Predictive Value of 99mTc-MAA SPECT for 90Y-Labeled Resin Microsphere Distribution in Radioembolization of Primary and Secondary Hepatic Tumors
- Safety of a Scout Dose Preceding Hepatic Radioembolization with 166Ho Microspheres
- Systematic Evaluation of Tumoral 99mTc-MAA Uptake Using SPECT and SPECT/CT in 502 Patients Before 90Y Radioembolization