


Abstract
447
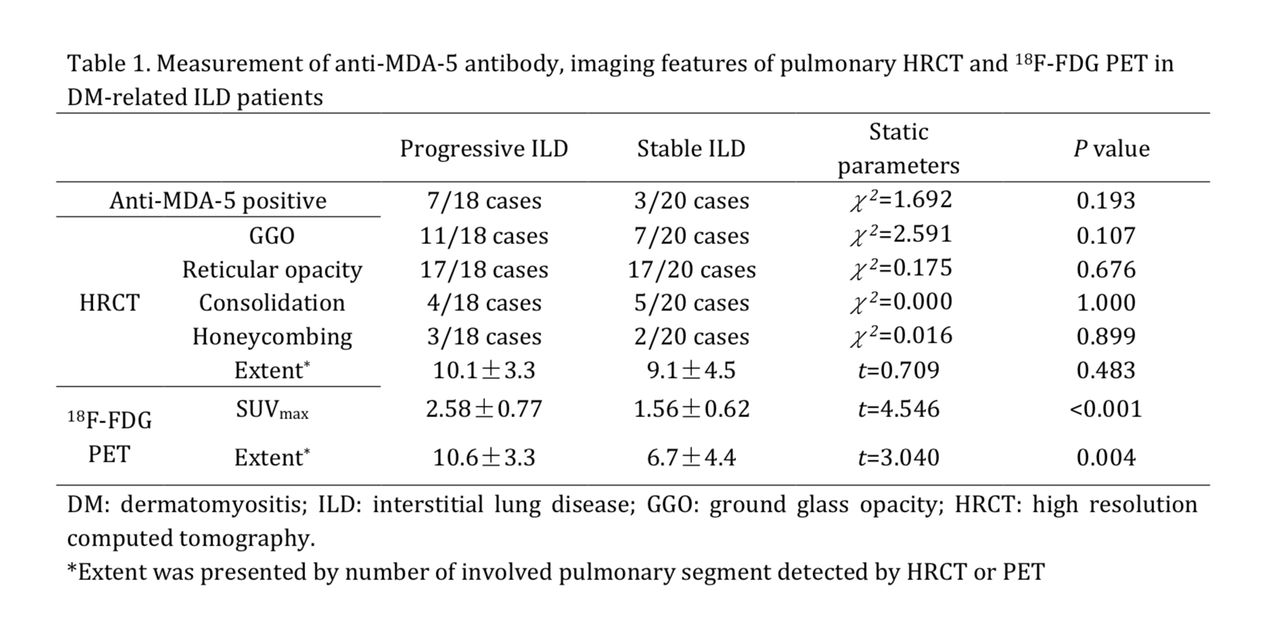
Background: Compared to other connective tissue diseases, pulmonary involvement was more likely to occur in dermatomyositis(DM). Interstitial lung disease (ILD) is the most common cause of disability and mortality that affects the prognosis of DM. Previous studies shows that anti-MDA-5 antibody was associated with severe progressive ILD and poor prognosis. FDG PET and pulmonary high resolution computed tomography (HRCT) was proved to be useful in the evaluation of ILD. However, the relationship between anti-MDA-5 antibody, imaging features of FDG PET and HRCT with long-term outcome of DM-related ILD remains unclear. This study retrospectively reviewed consecutive cases of DM to clarify the prognosis factor of DM-related ILD. Methods: We retrospectively analyzed the data of consecutive 47 cases of DM, including 17 male and 30 female with average age 55.7±11.6 years. All patients underwent regular 18F-FDG PET/CT imaging and pulmonary HRCT simultaneously. Serum anti-MDA-5 antibody was measured for all cases. Imaging analysis including the absence of ILD and its imaging features in HRCT, SUVmax of ILD in PET imaging, as well as the number of segments involved in HRCT and PET. All patients were followed-up by HRCT for at least 6 month. Progressive ILD was defined when the extent of ILD was enlarged during follow-up. Measurement of serum anti-MDA-5 antibody, FDG PET and HRCT findings were correlated with the clinical outcome. Results: Among 47 cases, 38 cases (80.9%) were diagnosed of ILD associated with DM. Ten of 38 cases (26.3%) were anti-MDA-5 positive. On HRCT images, ILD was manifested as patchy ground glass opacity, reticular opacity, consolidation and honeycombing in 18/38(47.3%), 34/38(89.5%), 9/38(23.7%) and 5/38(13.2%) cases, respectively. Average number of pulmonary segment involved was 9.6±4.1 on HRCT. In PET images, average SUVmax of ILD was 2.04±0.86 (ranged from 0.6 to 4.7) and the average number of pulmonary segment involved was 8.5±4.4. According to the follow-up HRCT, 18 cases showed a progressive ILD. Compare to the stable ILD, the SUVmax(2.58±0.77 vs 1.56±0.62, t=4.546,P<0.001) and ILD extent on PET imaging(10.6±3.3 vs 6.7±4.4, t=3.040, P=0.004) was significantly different in progressive ILD. However, the imaging feature and ILD extent on HRCT, as well as anti-MDA-5 positive, showed no significant difference between two groups (table 1). To predict progressive ILD by FDG uptake, ROC curve analysis showed that the area under the curve was 0.856. When SUVmax≥2.2 was employed as the threshold, the diagnostic sensitivity, specificity and accuracy was 83.3% (15/18), 85.0% (17/20), and 84.2% (32/38), respectively. Cox proportional hazards regression model suggested that SUVmax of ILD was the independent risk factor for predicting the progressive ILD (HR=13.839, P=0.001, 95% CI 3.084-62.113).
Conclusions: To evaluate the outcome of DM-related ILD, 18F-FDG PET was more valuable than pulmonary HRCT and serum anti-MDA-5 antibody measurement. The prognosis of DM-related ILD was poor when its SUVmax is higher than 2.2.

In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.