

Abstract
Cancer patients frequently have anemia or an altered coagulation state that may affect their risk stratification for perioperative cardiac events. We performed this study to investigate the incidence of perioperative cardiac events in cancer patients who had abnormal stress myocardial perfusion imaging (MPI) results versus cancer patients with normal MPI results. Methods: We included 394 consecutive cancer patients with normal (n = 201) or abnormal (n = 193) results on MPI studies performed for preoperative risk stratification. MPI was performed within 6 mo before each patient's scheduled operation. All the patients had surgical procedures requiring general anesthesia, except for 18 who had endoscopic or colonoscopic procedures. We retrospectively reviewed their data for the incidence of major cardiac events intraoperatively and for 1 mo postoperatively. We collected data on their cancer type, risk factors for coronary artery disease, MPI findings, risk of operation, and intraoperative or postoperative major cardiac events, which included death, myocardial infarction (MI), and congestive heart failure (CHF). Results: The patients with abnormal MPI results included 97 with ischemia, 80 with scarring, and 16 with mixed scarring and ischemia. The mean left ventricular ejection fraction and end-diastolic volume were 63.8% ± 9.8% and 82.0 ± 53.5 mL in the normal MPI group versus 52.1% ± 13.1% and 118.1 ± 53.4 mL in the abnormal-MPI group (P < 0.001). There were 9 major intraoperative or postoperative cardiac events (4.7%) in the patients with abnormal MPI results and none in the patients with normal MPI results (P = 0.001). These major events consisted of 3 deaths, 2 acute MIs, 1 non–Q-wave MI, and 3 cases of CHF. Four of these patients had only scarring on their MPI studies, 3 had ischemia, and 2 had scarring and ischemia. Conclusion: Normal MPI results have a high negative predictive value for perioperative cardiac events in cancer patients. Abnormal MPI results, whether demonstrating scarring or ischemia, should prompt appropriate perioperative management in patients with cancer to minimize major cardiac events.
- risk stratification
- cancer
- myocardial perfusion imaging
Multiple studies have established the value and prognostic impact of gated myocardial perfusion imaging (MPI) in predicting perioperative cardiac events (1–5). The concern for perioperative cardiac events is usually higher with major surgical procedures when significant blood loss, prolonged anesthesia, surgical trauma, hypothermia, or pain is anticipated (6). Because patients with peripheral vascular disease are expected to have significant coronary artery disease (CAD) and to undergo major surgeries, many of the previous studies for perioperative risk stratification were performed on patients who underwent vascular operations (7–11). Patients with cancer also frequently undergo major surgical procedures for tumor or metastasis resections or for reconstruction. These patients often have anemia, hypercoagulability, or pain in relation to their underlying malignancies (12). These factors are expected to add stress to the heart during major operative procedures. Additionally, many of these patients have received chemotherapy or radiation therapy before their surgery in an attempt to shrink their tumors or for adjuvant systemic or local control of their disease. Some chemotherapeutic agents, such as the anthracyclines, have deleterious cardiac effects (13–15). The effects of other chemotherapeutic agents on the coronaries are debatable. In addition, patients with tumors near the heart who receive radiation before their surgery may already have subclinical radiation-induced CAD (16–20).
Awareness of all these additional risks in cancer patients has necessitated evaluation of the usefulness and yield (21,22) of stress MPI for risk stratification in this special cancer population. Therefore, we performed this study to evaluate the usefulness and reliability of stress MPI in risk stratification and in the prediction of major perioperative and postoperative cardiac events in patients with cancer.
MATERIALS AND METHODS
Upon approval of the study by the Institutional Review Board, we retrospectively reviewed a database containing prospectively collected information on MPI results. The records of 193 consecutive patients with abnormal stress MPI results and 201 consecutive patients with normal MPI results on studies performed during the interval from March to December 2003 were reviewed. The MPI studies were performed within the 6 mo before an operation that required general anesthesia or, in 18 patients, before endoscopic or colonoscopic procedures. All MPI studies were performed using a dual-isotope, resting 201Tl and gated stress 99mTc-tetrofosmin standard protocol. They were ordered for the purpose of risk stratification for patients who had one or more risk factors for CAD or who had known CAD. Results were reported for a 14-segment cardiac model. The patients had different cancer types and were proceeding to surgical or diagnostic procedures related to their cancer. The risk of the operation or procedure was graded as low, intermediate, or high according to the guidelines of the American College of Cardiology/American Heart Association (Table 1) (22). The patients' records were reviewed for the incidence of major intraoperative and postoperative cardiac events. The patients were followed up for 1 mo after their operation. Major cardiac events were identified as death, nonfatal myocardial infarction (MI), malignant arrhythmia, or congestive heart failure (CHF). The clinicians were aware of the results of MPI in these patients and managed the patients accordingly during the perioperative period. Data on the perfusion and functional findings of the MPI studies; the patients' risk factors for CAD; and previous MI, CHF, or revascularization procedures were accumulated and compared between the 2 study groups.
Cardiac Risk Stratification for Noncardiac Surgical Procedures According to the 2002 Guidelines of the American College of Cardiology/American Heart Association (22)
Patients who underwent local anesthesia for their procedures were excluded from the study. Similarly, patients with an interval of greater than 6 mo between the MPI study and their operation were excluded. Patients who had cardiac events in the interval between the MPI study and the operation were also excluded.
The statistical analysis consisted of descriptive statistics comparing patients with normal MPI results and patients with abnormal MPI results. The difference in cardiac events between the 2 study groups was evaluated using the Mann–Whitney test. Statistical significance was indicated by P values of less than or equal to 0.05.
RESULTS
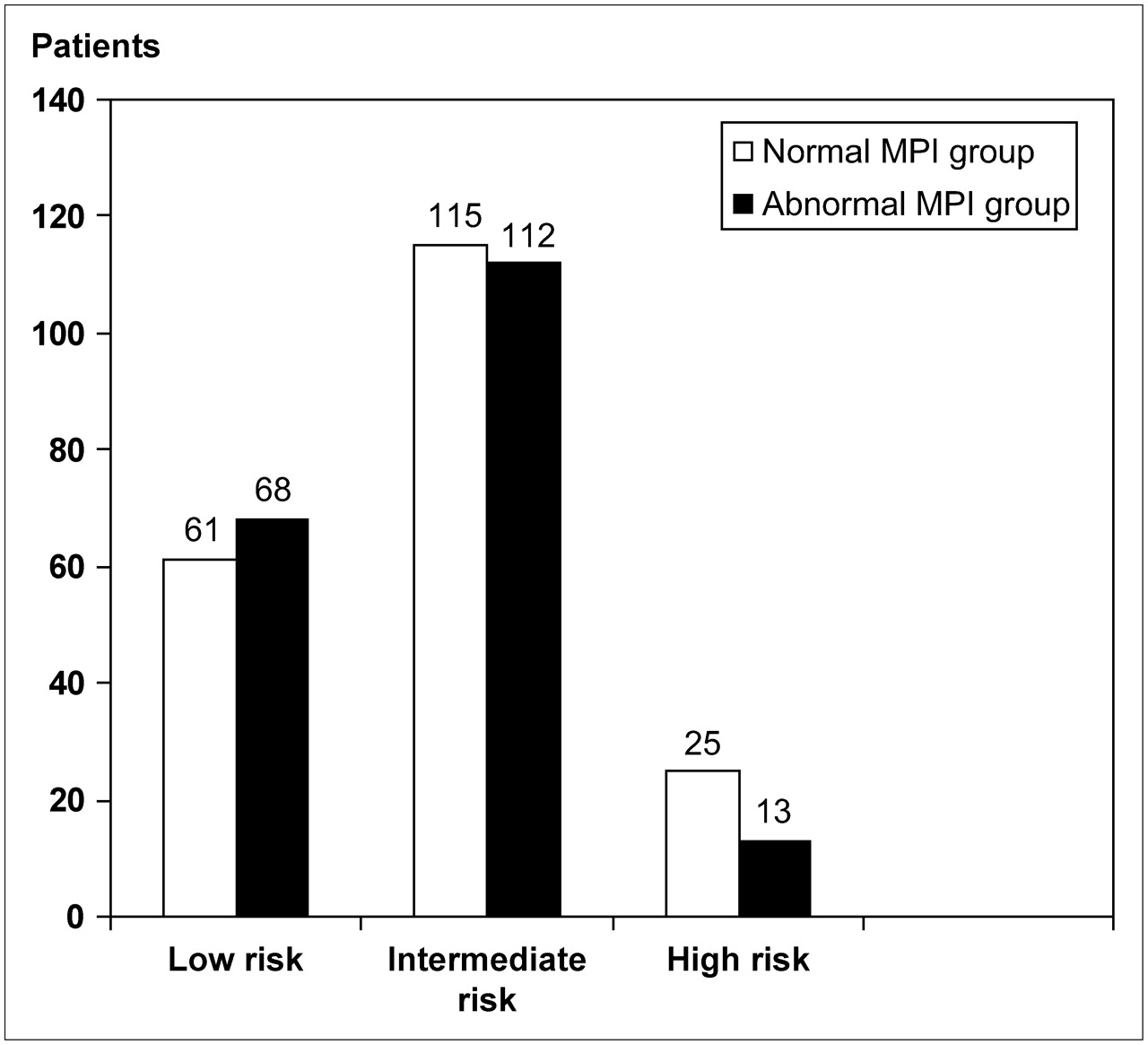
The total number of patients included was 394: 193 patients with abnormal preoperative MPI results and 201 patients with normal results. Their demographic characteristics and risk factors for CAD are summarized in Table 2. Significantly more patients in the group with abnormal MPI results had hypercholesterolemia (P = 0.003), a family history of CAD (P = 0.005), a history of CAD (P < 0.001), or revascularization procedures (P <0.001) before the MPI studies. Additionally, significantly more patients in the group with abnormal MPI results had a prior history of CHF and pacemaker placement. The number of patients with the remaining risk factors for CAD was comparable in the 2 groups. Twenty-one patients in the normal-MPI group had a history of chest pain within 3 mo before the operation, and 20 patients had dyspnea on exertion, whereas in the abnormal-MPI group 26 patients had a history of chest pain, 36 patients had dyspnea on exertion, and 5 patients had both chest pain and dyspnea on exertion. The mean and median intervals between the MPI studies and the operative procedure were 26.7 d and 13 d, respectively, in the patients with normal MPI results and 28.2 d and 17.5 d, respectively, in the patients with abnormal MPI results. Operations for tumors of the lung, breast, gastrointestinal and genitourinary tracts or for melanoma were the most common procedures (Table 3). Statistical analysis of the differences in common tumors between the 2 groups demonstrated significantly more operations for cervical or uterine tumors in the normal MPI group (P = 0.015). On the other hand, significantly more operations were performed for renal cancer (P = 0.04) and melanoma (P = 0.02) in the abnormal MPI group. There was no statistically significant difference in the operations for lung, breast, colorectum, bladder, or head and neck cancers between the 2 groups. The risk of operations or procedures in the normal- and abnormal-MPI groups is summarized in Figure 1.

{kind=link}
Operative or procedure risk in patients with normal and abnormal myocardial perfusion results.
Patient Characteristics and Risk Factors for CAD in the Normal and Abnormal MPI Groups
Types of Cancer in Patients with Normal and Abnormal Myocardial Perfusion Results
The abnormal MPI results included ischemia in 97 patients, scarring in 80 patients, and mixed scarring and ischemia in 16 patients. The mean left ventricular ejection fraction and end-diastolic volume were 63.8% ± 9.8% and 82.0 ± 53.5 mL in patients with normal MPI results and 52.1% ± 13.1% and 118.1 ± 53.4 mL in patients with abnormal MPI results (P < 0.001). Seventy-seven patients had already been receiving β-blockers before the operation, and 53 patients were newly started on β-blockers before the operation in the group with abnormal MPI results. These patients were maintained on β-blockers during the perioperative period. Only 7 patients underwent revascularization procedures based on abnormal MPI results before their cancer-related operation. One of these patients had a coronary bypass operation 25 d before a hemicolectomy for colon cancer and took clopidogrel bisulfate (Plavix; Sanofi-Synthelabo) and aspirin for only 2 wk after the coronary bypass. The remaining 6 patients had stent placement in one of the coronary arteries before their cancer operation. The mean interval between stent placement and their cancer operation was 55 d. These patients were taking clopidogrel bisulfate and aspirin before their cancer operation. The medications were discontinued 1–7 d before the operation and were restarted 1–3 d postoperatively.
There were 9 major cardiac events (4.7%) in the patients with abnormal MPI results intraoperatively or postoperatively and no major cardiac events in the patients with normal MPI results (P = 0.001). The 9 major events included 3 deaths, 2 acute MIs, 1 non–Q-wave MI, and 3 cases of CHF. All deaths and MIs occurred either intraoperatively or within the first 6 d postoperatively. The causes of death were cardiac arrest in 2 patients and progressive CHF and respiratory failure in the third patient. Of the 3 cases of CHF, 2 of them were new episodes and 1 was in a patient who had a prior history of CHF. The mean interval between the operation and death or acute MI was 1.7 d and between the operation and CHF was 21.3 d. Four of these patients had only scarring on their MPI, 3 had ischemia, and 2 had scarring and ischemia. The cancer type, blood loss and transfusions, and MPI abnormalities of the patients who had major cardiac events are summarized in Table 4. Nonmalignant arrhythmias occurred in 12 patients with normal MPI results and 16 patients with abnormal MPI results (P = 0.37). In all patients, these arrhythmias occurred within the first week after the operation, except for 1 patient who had atrial fibrillation on day 23 after the operation.
Operative Data and MPI Results in Patients Who Had Major Perioperative Cardiac Events
DISCUSSION
In this study, we evaluated the incidence of perioperative and postoperative complications in cancer patients with normal versus abnormal MPI results. Despite the major procedures that many of these patients underwent, our overall incidence of major cardiac events was low, at 4.7%. All of these events occurred in patients who had abnormal MPI results during the preoperative risk stratification assessment. None of the patients with normal MPI results had major cardiac events, indicating a 100% negative predictive value for MPI in patients with cancer. This finding is contrary to our expectation of unpredictable cardiac events by MPI in cancer patients because of their multiple comorbidities, altered coagulability, paraneoplastic syndromes, or adjunctive anticancer therapies, which can be deleterious to the heart. We have anticipated major cardiac events in cancer patients with normal myocardial perfusion results on account of their hypercoagulable status and possible vulnerability to thrombosis (23–25), in an area of vulnerable but insignificantly stenotic coronary plaques. In other words, we expected a higher incidence of false-negative MPI results in this special cancer population than that in noncancer patients. The rate of false-negative MPI results in noncancer patients has previously been reported to range from 0% to 3.5% (26). Our lack of false-negative MPI results in this study population indicated that MPI is a strong predictor of intraoperative or postoperative major cardiac events even in cancer patients.
The incidence of major cardiac events in patients with abnormal MPI results in this study could have been low because the clinicians and anesthesiologists knew of the results before the operative procedure and were thus directed toward appropriate perioperative patient management. Knowledge of the MPI findings resulted in additional medical therapy or revascularization in 32% of patients before their operation. In contrast, the study of Mangano et al., in which clinicians did not know the results of MPI before the operation, had a major cardiac event rate of 58% (27). Alternatively, the low incidence of major cardiac events could be related to the fact that many of the operations in our patient population were of low risk (61 and 65 in the normal and abnormal MPI groups, respectively). However, 8 of the major cardiac events occurred with operations of intermediate risk and 1 occurred after an operation of low risk. Additionally, all major cardiac events occurred in the abnormal MPI group, for which the number of high-risk operation was almost half that in the normal MPI group (13 vs. 25). Thus, necessary precautions should be taken on the basis of the preoperative patient evaluation, including MPI findings, rather than on the risk of the operation. In other words, the patient risk of having CAD is more important than the risk of the operation.
The finding of scarring without ischemia in 4 of the 9 patients with major cardiac events and in 1 of the 3 who died might have lowered the precaution level preoperatively, suggesting that both reversible and irreversible perfusion defects may warrant additional intraoperative and postoperative precaution. Our results differ from those of multiple previous studies indicating that adverse outcomes occurred mostly in patients in whom MPI studies found reversible defects (28–31).
Two of the patients who died had lung cancer, and the third had squamous cell cancer of the head and neck. Patients who had CHF postoperatively had a prior history of MI and had a low left ventricular ejection fraction (25%, 28%, and 34%). The additional value of functional information has previously been established (32,33) and was further demonstrated in our study by the significant difference found in mean left ventricular ejection fraction and end-diastolic volume in the abnormal and normal MPI groups.
One limitation of our study was that it did not evaluate the additive value of MPI over clinical risk stratification alone or other noninvasive cardiac tests in patients with cancer. However, these issues were previously investigated by studies that agreed on the additive value of noninvasive testing over clinical scoring systems alone (1,3,34) but differed on which noninvasive test—stress echocardiography, MPI, or 24-h Holter monitoring—best predicted outcome (26,35). We chose to focus on the value of preoperative MPI as the sole test for preoperative risk stratification. A second limitation was the inherent inaccuracy of retrospective data collection, with possible deficiencies in the documenting of patient risk factors for CAD. However, this limitation did not affect our results on the prognostic value of MPI in the preoperative risk stratification of cancer patients. Because our initial hypothesis was a higher incidence of major cardiac events in cancer patients with normal preoperative MPI results, conveying MPI results to clinicians before the operation was not considered a limitation of our study because a normal MPI result did not change patient management perioperatively.
In summary, MPI results have accurately identified cancer patients undergoing major surgical procedures who might experience serious cardiac events intraoperatively or postoperatively. Although surgery is rarely delayed in cancer patients because of abnormalities seen on MPI, additional perioperative precautions and care measures can be prompted by the MPI results. MPI also helped in identifying patients with previously undetected CAD, allowing proper management to be initiated before the operation.
CONCLUSION
Normal findings on stress MPI have a high negative predictive value for perioperative major cardiac events in cancer patients. The incidence of perioperative major cardiac events is low in cancer patients having major surgical procedures when necessary medical and anesthesia precautions are taken on the basis of MPI results. Patients who had major cardiac events perioperatively had preoperatively abnormal MPI results demonstrating scarring or ischemia.
Footnotes
-
COPYRIGHT © 2007 by the Society of Nuclear Medicine, Inc.
References
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.
- 21.
- 22.
- 23.
- 24.
- 25.
- 26.
- 27.
- 28.
- 29.
- 30.
- 31.
- 32.
- 33.
- 34.
- 35.
- Received for publication July 17, 2006.
- Accepted for publication November 21, 2006.