


Abstract
Gated blood-pool SPECT (GBPS), inherently 3-dimensional (3D), has the potential to replace planar equilibrium radionuclide angiography (ERNA) for computation of left ventricular ejection fraction (LVEF), analysis of regional wall motion (RWM), and analysis of right heart function. The purpose of this study was to compare GBPS and ERNA for the assessment of ventricular function in a large, multicenter cohort of patients. Methods: One hundred seventy-eight patients referred in the usual manner for nuclear medicine studies underwent ERNA followed by GBPS. Each clinical site followed a GBPS acquisition protocol that included 180° rotation, a 64 by 64 matrix, and 64 or 32 views using single- or double-head cameras. Transverse GBPS images were reconstructed with a Butterworth filter (cutoff frequency, 0.45–0.55 Nyquist; order, 7), and short-axis images were created. All GBPS studies were processed with a new GBPS program, and LVEF was computed from the isolated left ventricular chamber and compared with standard ERNA LVEF. Reproducibility of GBPS LVEF was evaluated, and right ventricular ejection fraction (RVEF) was computed in a subset of patients (n = 33). Using GBPS, RWM and image quality from 3D surface-shaded and volume-rendered cine displays were evaluated qualitatively in a subset of patients (n = 30). Results: The correlation between GBPS LVEF and planar LVEF was excellent (r = 0.92). Mean LVEF was 62.2% for GBPS and 54.1% for ERNA. The line of linear regression was GBPS LVEF = (1.04 × ERNA LVEF) + 6.1. Bland–Altman plotting revealed an increasing bias in GBPS LVEF with increasing LVEF (Y = 0.13x + 0.61; r = 0.30; mean difference = 8.1% ± 7.0%). Interoperator reproducibility of GBPS LVEF was good (r = 0.92). RVEF values averaged 59.8%. RWM assessment using 3D cine display was enhanced in 27% of the studies, equivalent in 67%, and inferior in 7%. Conclusion: GBPS LVEF was reproducible and correlated well with planar ERNA. GBPS LVEF values were somewhat higher than planar ERNA, likely because of the exclusion of the left atrium.
Planar equilibrium radionuclide angiography (ERNA) is well established and provides a relatively simple and noninvasive method to assess ventricular function and, in particular, left ventricular ejection fraction (LVEF) (1,2). In any planar projection imaging study, anatomic structures overlap. In planar equilibrium blood-pool imaging, the inferior wall of the left ventricle is obscured by the right ventricle in anterior and right anterior oblique (RAO) projections, and the left atrium may partially overlap, posteriorly, the left ventricle in left anterior oblique (LAO) or best septal views. The partial inclusion of the left atrium in a left ventricular region of interest (ROI) has been shown to decrease LVEF, because left atrial counts from the filled left atrium may be present in the left ventricular ROI at ventricular end-systole (3).
Tomography has been extensively used in myocardial perfusion imaging, and recently, calculation of LVEF from gated myocardial perfusion SPECT studies has been widely reported (4–6). These methods are adjunctive to the assessment of coronary artery disease by perfusion imaging using 99mTc agents and 201Tl, providing assessment of ventricular function and wall thickening. However, these methods (using only 8 gated frames, precluding the computation of ejection and filling parameters) have poor temporal resolution and, by and large, use geometric methods to compute LVEF. These methods do not fare well in the presence of high extracardiac activity or low counting statistics and in patients with severe perfusion defects or small hearts (7–9). Moreover, errors in the assessment of myocardial wall thickening because of the partial-volume effect have been reported (9).
For analysis of ventricular function, gated blood-pool SPECT (GBPS) has the benefit of the tomographic perspective to isolate the left and right ventricles without overlap of other cardiac chambers and to improve the assessment of regional wall motion (RWM) (10–16). Further, most reported GBPS methods are truly volumetric in their computation of LVEF and ventricular volumes. GBPS images can be acquired in less time than is needed for a 3-view planar ERNA series using multihead gamma cameras (approximately 15 min), improving patient throughput. Using GBPS has an added advantage, because the best septal view, unlike planar imaging, need not be found for computation of LVEF. The search for the best septal view is frequently tedious and sometimes unproductive.
The computation of right ventricular ejection fraction (RVEF) with planar ERNA techniques is unreliable at best. First-pass techniques have become the standard for computation of RVEF but are tedious to perform and can lack adequate statistics (16). Using GBPS, not only can the effect on LVEF from left atrial activity contamination be removed, but also, potentially, RVEF may be accurately quantified. With improved gamma cameras and faster computers, GBPS may become a practical tool for assessment of ventricular performance. However, the calculation of global LVEF from GBPS has not been evaluated in a large-scale study. The purpose of this investigation was to compare GBPS assessment of ventricular performance and, in particular, global LVEF with planar ERNA assessment in a multicenter environment and to establish reference limits for RVEF from a cohort of patients with normal right ventricular function. Additionally, the reproducibility of manually determined GBPS LVEF computation was assessed, and visual assessment of RWM from 3-dimensional (3D) surface-shaded displays was compared with planar ERNA cine assessment in a subset of patients.
MATERIALS AND METHODS
Planar and GBPS Studies
Planar and GBPS studies were successfully acquired for 178 patients from the 5 participating clinical sites, who were referred in the usual manner for nuclear medicine assessment of ventricular function. Both the planar and the GBPS studies were acquired on the same day—the SPECT study immediately after the planar views. The population was largely composed of chemotherapy patients (124 patients) and also included some coronary artery or heart disease patients and 8 heart failure patients. A dose of 925–1110 MBq 99mTc was administered as a blood-pool tag, with each site using its own tagging protocol. Standard ERNA imaging used a low-energy, all-purpose or high-resolution collimator, and the protocol included standard electrocardiography (ECG) peak R-wave gating with on-the-fly arrhythmia rejection, acquiring 16–24 forward-gated or forward- and backward-gated frames. The planar acquisition time was 25–35 min and included 3 or 4 views (e.g., RAO, anterior, best septal, 70° LAO, or left lateral), according to the individual standards of each institution. SPECT was performed after the planar acquisitions. Each institution used its own standard protocol to compute global LVEF. In general, planar LVEF processing included either manual definition of the left ventricle in the end-diastolic and end-systolic frames from the best septal view or automatic determination of the left ventricular boundary with opportunity for operator approval or modification of the borders. RWM was visually assessed from the simultaneously displayed cines of the 3 acquired planar views.
GBPS
Acquisition.
GBPS was performed using either a single-head gamma camera (42 patients) or a double-head gamma camera in the 90° configuration (136 patients). All patient studies were acquired using a 180° arc, starting at −45° (RAO), using either a low-energy, all-purpose collimator (single-head systems) or a high-resolution collimator. Single-head systems used a circular orbit, whereas double-head systems used either circular or noncircular orbits, depending on the institutional protocol. Images were acquired in a 64 by 64 matrix with a zoom of 1.23 or 1.45 (depending on heart size), using either 32 views at 1 min per projection for single-head systems or 64 views (32 per head) at 30 s per projection for double-head systems, in step-and-shoot mode. Conventional ECG gating was used with a wide R-R acceptance window (60%), and 16 forward-gated frames were acquired over the cardiac cycle, using standard on-the-fly arrhythmia rejection. With this protocol, double-head gamma camera acquisitions typically contained approximately 30–40 million total counts (2–2.5 million counts per time bin). GBPS was successfully performed for all patients.
Reconstruction.
Transverse 64 by 64 images were reconstructed with a ramp filter using a seventh order, 2-dimensional Butterworth filter and a cutoff frequency of 0.45–0.55 Nyquist for each of the 16 time bins. The default cutoff was 0.55 Nyquist. However, if the projection data appeared noisy on the cine display because of arrhythmias or irregular rhythms, the cutoff was adjusted downward to between 0.50 and 0.45 Nyquist. Flood and center-of-rotation corrections were applied, but not attenuation or decay correction. Short- and long (sagittal or coronal)-axis oblique slices were formed by reorienting the transverse image data using standard, partly manual methods. The total reconstruction and processing time was <10 min.
Analysis of Ventricular Performance
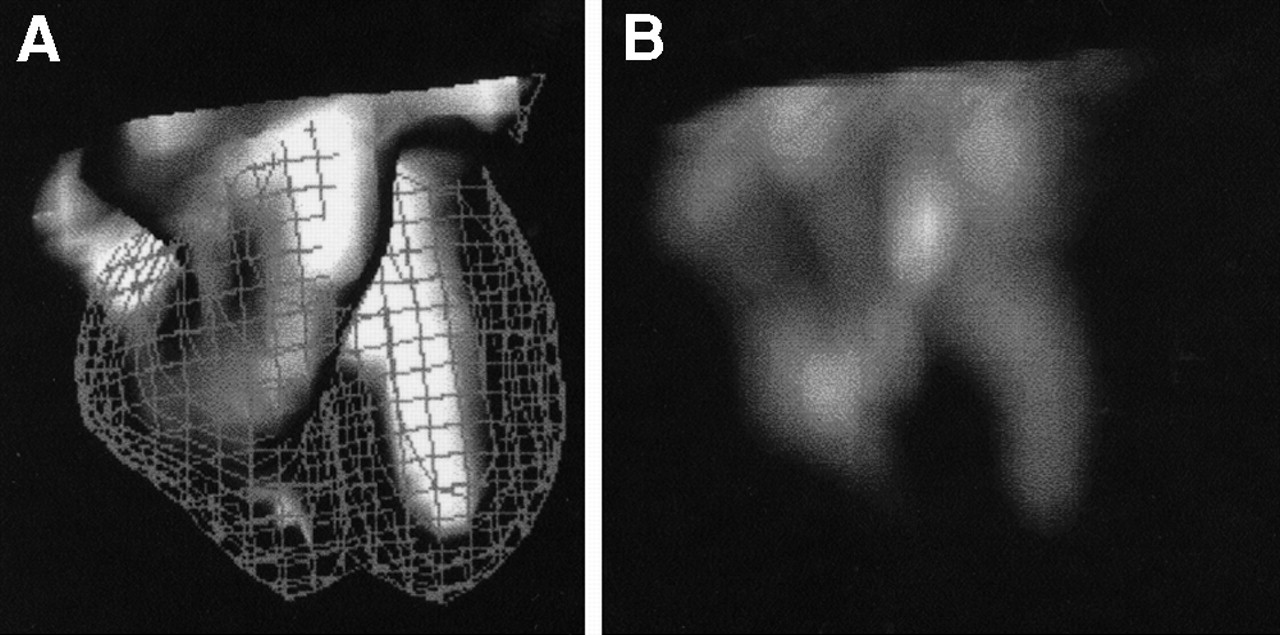
A quantitative GBPS program (NUMUGAS; Northwestern University, Chicago, IL) was coded using the IDL language (Research Systems Inc., Boulder, CO) on an ICON computer (Siemens Medical Systems, Hoffman Estates, IL). The GBPS program creates a 3D, rotatable, cine display of volume renderings (maximum intensity projection [MIP]) and surface-shaded renderings from the short-axis oblique dataset. Figure 1 illustrates a typical surface-shaded and volume-rendered display in 1 long-axis orientation. The program quantifies ejection fraction, volumetrically, using maximal or minimal (diastole to systole) count change from all 16 gated frames. For GBPS, no background correction is required (3). Also available, but not used for this study, are regional ejection fraction, maximum and average emptying and filling rates, and ejection and filling periods.

Three-dimensional surface-shaded (A) and volume-rendered (B) images at selected long-axis projection. End-diastolic birdcage (A) is used as reference for assessment of RWM.
LVEF
Global LVEF was computed for all patients by manual definition of boundaries on all 16 gated frames of the left ventricular blood pool (which included the left ventricle and excluded the left atrium and right heart), using the short-axis oblique slices. The beating cine display of the short-axis slices was used to help the operator separate the left ventricle from the left atrium, and the slices were summed to include the most apical slice through the basal slice that contained the left ventricle but excluded the left atrium. Computation of ejection fraction took, on average, 5–8 min of technologist time. The trained operators were unaware of the results of the planar ERNA analysis. The images of all patients were successfully processed by both SPECT and planar methods. GBPS LVEF was computed by 2 trained users for a subset of 33 patients to assess operator dependencies, if any, in computation of global LVEF using SPECT studies. These patients were chosen at random from the entire cohort, and the GBPS SPECT and planar studies were reprocessed at the core laboratory site by 2 operators.
RVEF
Global RVEF was computed for a 33-patient subset with no clinical or planar scintigraphic evidence of right ventricular dysfunction. The right ventricular boundary was manually defined on each of the 16 gated frames over the right ventricular blood pool, as had been done for the LVEF determination. Because of the lack of a gold standard for RVEF (no first-pass imaging was performed on this patient cohort), GBPS RVEF was computed for the subset but was not compared with any other methods.
RWM
Three-dimensional renderings included a volume-rendered display using the MIP method, in which the cardiac silhouette appears translucent. The 3D surface-shaded rendering was created using a modified threshold method for surface detection, as previously described (17), with polygon tiling and Gouraud shading (lighting algorithm) for the blood-pool surface. An end-diastolic (or any other of the 16 frames) “birdcage” was available and was used as a fixed reference for wall motion assessment (Fig. 1). The 3D displays, which the user could rotate to any orientation in space, allowed assessment of RWM from all aspects of the right and left ventricles. For 30 patients from 1 site, RWM determined from 3-view planar imaging was compared with visual interpretation of RWM using the 3D surface-shaded display at operator-controlled viewing angles. The 2 methods were compared subjectively by 2 experienced readers who reached a consensus and who knew in detail each patient’s clinical history, ECG findings, and other diagnostic findings. Assessment of RWM using the GBPS surface-shaded display was rated as superior, equivalent, or inferior to assessment of RWM from simultaneous cine display of the 3-view planar ERNA studies.
Statistical Analysis
Global LVEF, as determined by GBPS, was compared with planar ERNA LVEF using linear regression analysis. The correlation coefficient, line of linear regression, SEE, and probability value were computed. The average values of GBPS and planar ERNA LVEF were determined, and Bland–Altman plotting was used to evaluate systematic differences, if any, between LVEFs from the 2 methods. Linear regression analysis was also applied to assess interoperator variability. For visual assessment of RWM, a subjective comparison was used.
RESULTS
Global LVEF
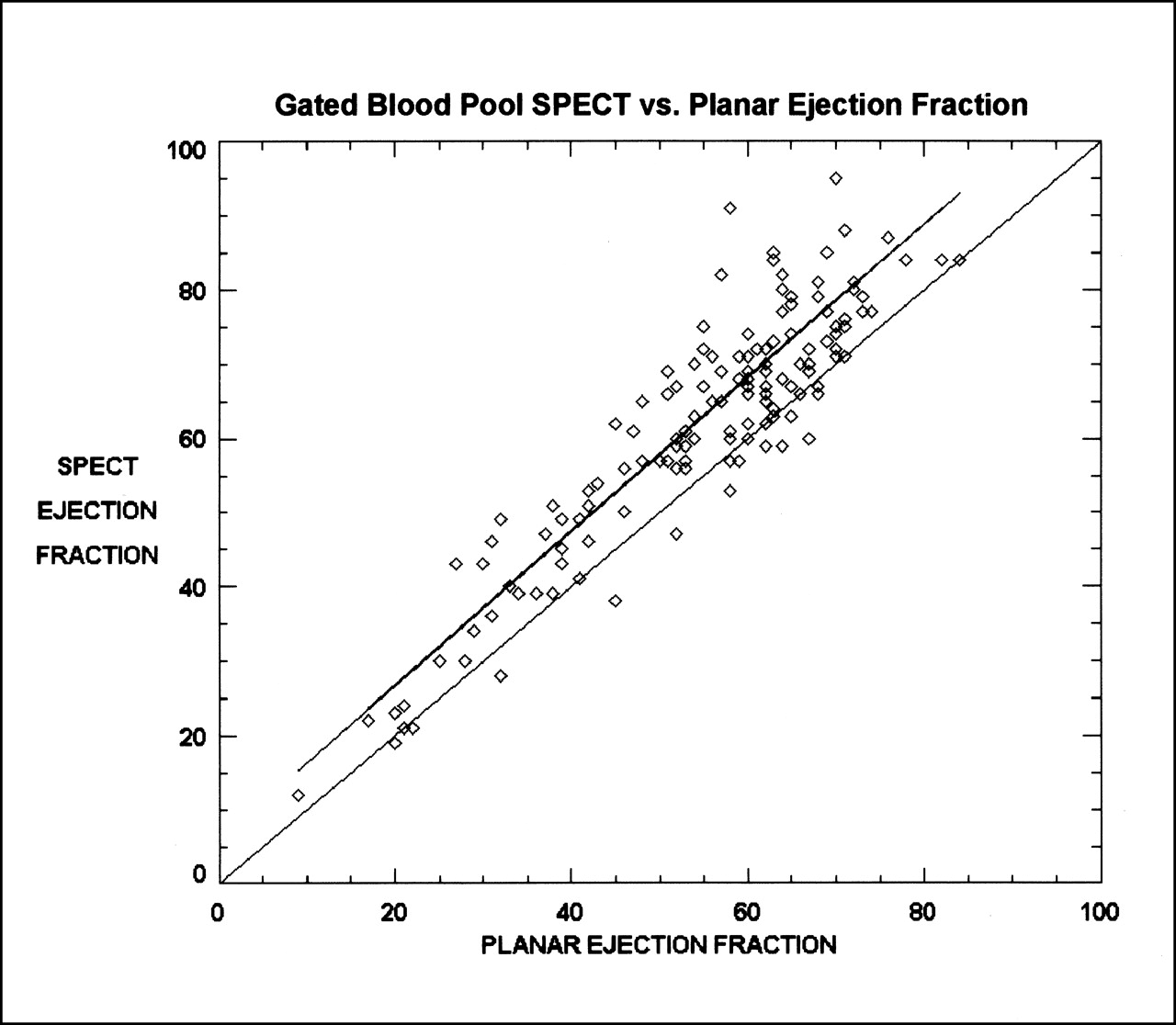
Global LVEF assessed by GBPS correlated well with that assessed by conventional planar methods (r = 0.92; SEE = 5.4; P < 0.001) for the 178 patients, as illustrated in Figure 2. The line of linear regression was GBPS LVEF = (1.04 × ERNA LVEF) + 6.1. The average value of planar LVEF was 54.1% ± 15.3%, whereas the average value for GBPS LVEF was 62.2% ± 17.2%.

LVEF determined by GBPS (ordinate) vs. LVEF determined by planar ERNA (abscissa). Line of linear regression (top) and line of identity (bottom) are shown.
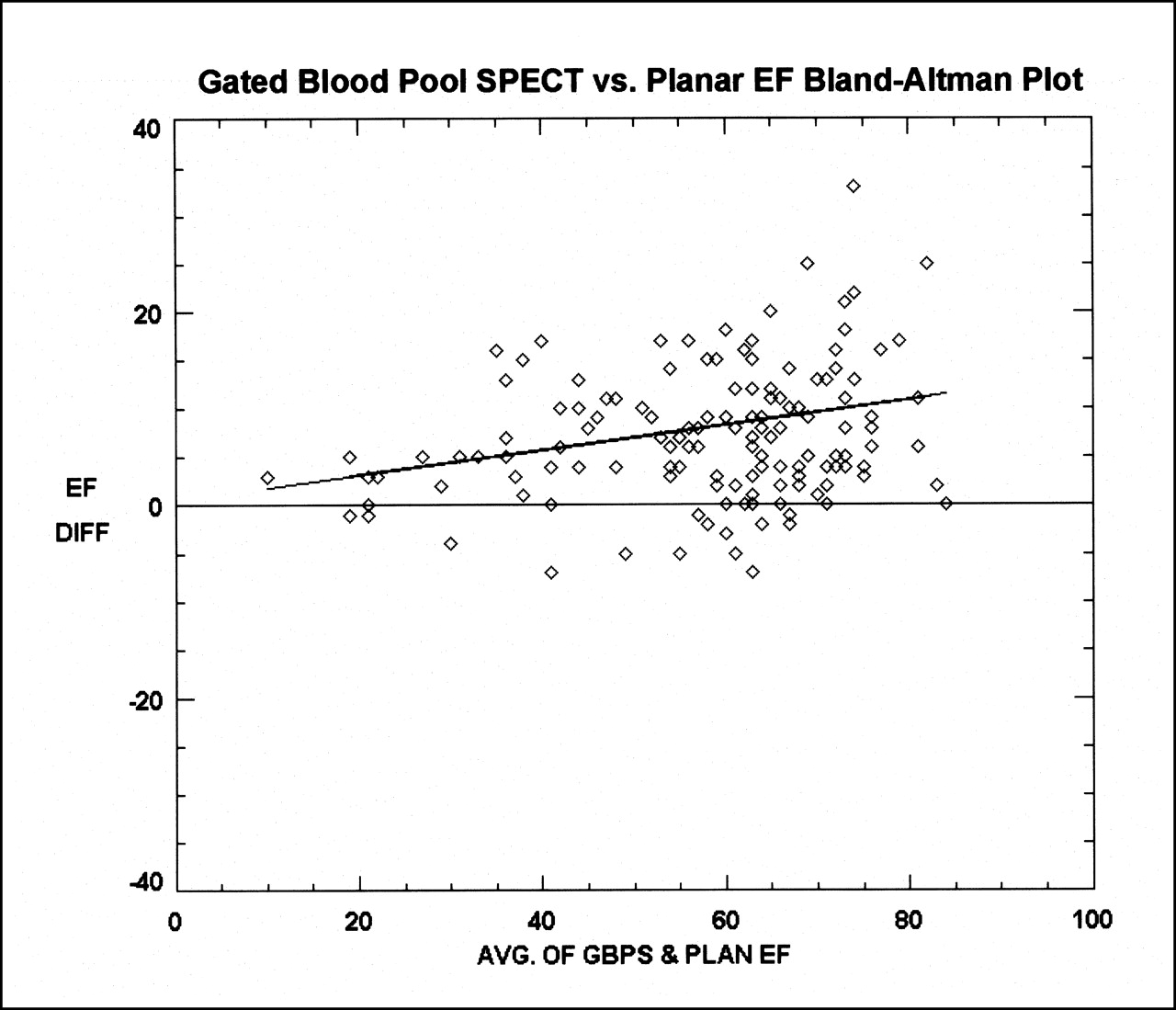
Bland–Altman plotting (Fig. 3) revealed a systematic bias toward higher LVEF values when using GBPS. Also, a trend toward higher GBPS LVEF than planar LVEF with increasing magnitude of LVEF was noted on the Bland–Altman plot Y = 0.13x + 0.61 (r = 0.30; P < 0.01). The mean difference in LVEF value was 8.1% ± 7.0% in ejection fraction units.
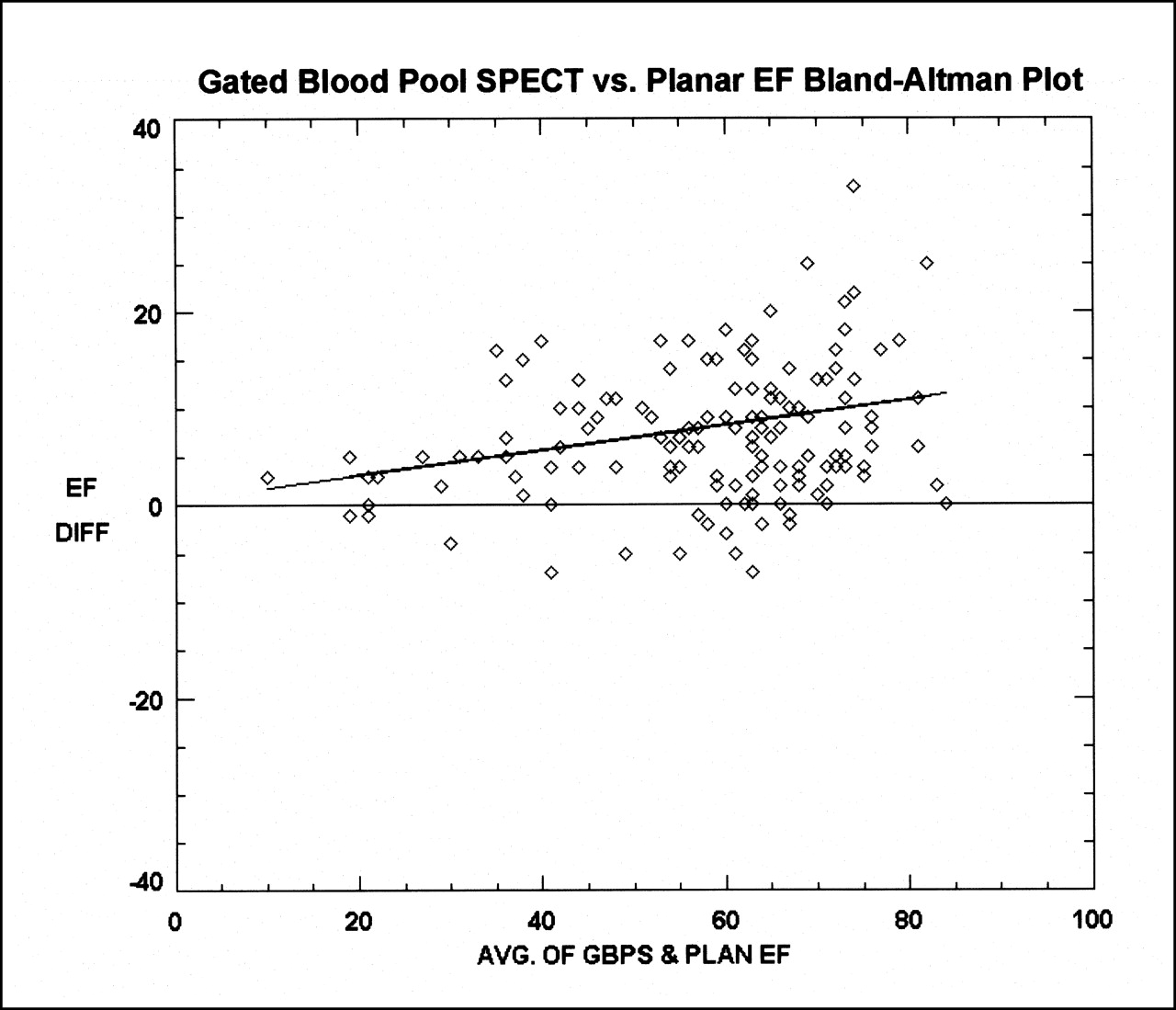
Bland–Altman plot of GBPS LVEF vs. planar ERNA LVEF, along with fit (Y = 0.13x + 0.61) of data. AVG. = average; DIFF = difference; EF = ejection fraction; PLAN = planar.
For the subset of 33 patients, interoperator agreement in the calculation of global GBPS LVEF was good (r = 0.92; P < 0.01), with interoperator variability of ±4.1%. The interoperator LVEF values are plotted in Figure 4. The interoperator variability for conventional planar ERNA LVEF determination was ±3.2%.

GBPS LVEF determined by operator 1 (ordinate) vs. GBPS LVEF determined by operator 2 (abscissa). Line of identity is shown.
RVEF
The mean value of global RVEF was 59.8% ± 12.9% in the subset of patients without right ventricular dysfunction. Definition proved to be much more difficult for the right ventricular border than for the left ventricular border because of the tortuous geometries of the right ventricle. The average RVEF values in these patients without right ventricular dysfunction were lower than the average GBPS LVEF but somewhat higher than RVEF values determined using first-pass or planar techniques, perhaps again because of the isolation of the right ventricle.
RWM
Three cardinal views of the variable, user-controlled, surface-shaded display are shown in Figure 5 as long-axis, anterior, and left lateral equivalent views. The long-axis view shows the apex, septum, and lateral wall of the left ventricle and the septum and apex of the right ventricle. The anterior equivalent view shows the right ventricular long axis and the basal septum of the left ventricle. The left lateral equivalent view shows the inferior wall of the left ventricle and the anterior wall of the right ventricle. For the RWM study, the user was allowed to rotate the beating cine 3D display into any angle for best assessment of a particular cardiac region.

Three possible views (long-axis [A], anterior [B], and left lateral [C] equivalents), at end-diastole, of 3D Gouraud surface-shaded display showing left and right ventricles and pulmonary trunk.
Of the 30 patients evaluated by both 3-view planar cine and GBPS surface-shaded display, 24 (80%) of whom had a normal LVEF, the GBPS RWM was qualitatively assessed as superior in 8 (27%) by an experienced nuclear cardiologist. Planar cine assessments of RWM and GBPS surface-shaded cine displays were judged to be equivalent in 20 patients (67%), whereas the planar display was judged to be superior in only 2 patients (7%). In these 2 patients, septal wall motion was believed to be better assessed by the LAO or best septal view than by the 3D surface-shaded display. Of the 6 patients with decreased LVEF, evaluation of RWM abnormalities using GBPS was rated superior to 3-view planar cine visual assessment in 4 and equivalent in 2.
DISCUSSION
The global LVEF computed from GBPS was, on average, 8% higher than that computed using conventional ERNA methods. This finding is consistent with the findings of Bartlett et al. (3). They computed LVEF using GBPS by reprojecting the blood pool back to a conventional LAO planar view with and without the presence of the left atrium. They found that the presence of the left atrium reduced LVEF because, relative to diastole, additional systolic counts were present in the left ventricular ROI from the left atrium. Our results confirm that finding. Bland–Altman plotting revealed a trend toward a higher GBPS LVEF than planar LVEF at higher LVEF values. This finding is understandable, because better left ventricular pump function at higher LVEF values would produce a smaller end-systolic volume and the relative contribution from the left atrium would be more significant. As the left ventricle dilates and LVEF lessens, the large end-systolic volume would likely be less affected by the presence of left atrial counts. At lower LVEF values and in dilated ventricles, GBPS and planar LVEF values should be closer, as was observed in our data at LVEF values < 30%. Using GBPS LVEF in chemotherapy patients requires care. Although GBPS LVEF is likely to be an accurate reflection of ejection fraction, use of ERNA studies by SPECT methods to assess chemotoxicity in cancer patients may require reassessment of the conventional lower limit of normal LVEF (50%). The results of this multicenter study show that the lower limit of normal LVEF may lie in the 58%–60% range. The variability of GBPS LVEF for any single LVEF value is approximately the same as the planar LVEF variability. Thus, the precision of both methods is similar.
Attenuation correction was not applied. Attenuation defects in the center of the left ventricle were noted in some but not all patients with severely dilated left ventricles. If the relative effect of photon attenuation was higher at end-diastole than at end-systole, attenuation may have had some impact on the calculated LVEF. These patients were likely to have poor left ventricular function, and the effect might be minimal. However, the use of attenuation correction in GBPS studies should be evaluated.
Assessment of RWM either quantitatively, using SPECT (15), or qualitatively, using visual analysis of 3D surface displays, may prove superior to planar methods, although additional rigorous studies are required. Appropriate methodology to view and ascertain abnormalities using 3D analysis have yet to be fully developed. In this study, a volume-rendered display using MIP did not add to the analysis of RWM, and this MIP algorithm may not be a good model for visualization of the 3D motion of the heart. The Gouraud surface-shaded display did, however, appear to have merit in assessing RWM, although more study is required. RWM was judged equivalent between planar multicine assessment and 3D surface-shaded renderings in 66% of the patients. However, in most (80%) of the 30 patients who were evaluated by both methods, RWM motion was normal, and thus, the 30-patient cohort was likely not a good test of the ability of 3D renderings to detect subtle defects in wall motion. In the 6 patients with depressed LVEF, GBPS RWM fared well, rating better than planar cine display in two thirds of these patients. The Gouraud surface-shaded display did appear to provide a reasonable representation of cardiac motion, but whether this display accurately represents wall motion, or creates or masks wall motion defects in portions of the right and left heart, needs to be determined by a larger-scale study.
GBPS assessment of ventricular function provides efficiency when performed using multihead cameras. Reduced patient acquisition time will increase throughput. Perhaps the greatest challenge for the nuclear technologist in performing ERNA studies is finding the best septal view for a particular patient. At a minimum, the SPECT study can be reprojected into a best septal view retrospectively (and altered again, if necessary, by the evaluating physician) and conventional LVEF calculation performed.
Right ventricular function is important for the assessment of patients with congenital abnormalities, patients with heart failure, and patients for whom anesthesia poses a risk. Planar equilibrium methods have not been widely used to assess right ventricular function, and first-pass techniques, which do compute RVEF, are technically more difficult to perform because of the required bolus injection. Moreover, first-pass gamma cameras and adequate first-pass processing software are not as widely available as are planar and gated SPECT systems. The natural separation of right from left heart provided by tomographic techniques may be used for accurate assessment of the right heart. However, the geometry of the right ventricle is much more complex than that of the left ventricle, and manual definition of the right ventricle is tedious. A limitation of this study was that RVEF values were computed for a subset of patients with normal right ventricular function but were not compared with other methods. Perhaps automated, intelligent methods may optimize the assessment of right ventricular function (18).
CONCLUSION
GBPS was compared with conventional planar ERNA methods in a large, multicenter patient population. LVEF computed from GBPS correlated well with planar ERNA methods over a wide range of LVEF values. GBPS LVEF values were higher than planar values, particularly at higher LVEF values, likely because of the removal of the left atrium from the left ventricular ROI. In 93% of the studies from a small subset of patients, 3D analysis of RWM was superior or equal to 3-view planar analysis. The utility of 3D displays for assessment of RWM requires further study, as does the computation of RVEF using GBPS techniques.
Acknowledgments
The authors acknowledge Antonella DeRango, Michael A. Roman, Lisa Wall, Judith Cain, Scott M. Leonard, and Paul J. Groch for technical assistance and Marla C. Kiess, MD (University of British Columbia); H. William Strauss, MD (Stanford University, Stanford, CA); and Edwin M. Leidholdt, PhD (University of California-Davis), for helpful comments. This study was supported in part by a grant from Siemens Medical Systems and was presented in part at the 47th annual meeting of the Society of Nuclear Medicine, St. Louis, MO, June 2000, and at the 82nd annual scientific meeting of the American Heart Association, New Orleans, LA, November 2000.
Footnotes
Received May 18, 2001; revision accepted Aug. 7, 2001.
For correspondence or reprints contact: Mark W. Groch, PhD, Department of Nuclear Medicine, Northwestern Memorial Hospital, 251 E. Huron St., Chicago, IL 60611.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}