


Abstract
2488
Introduction: Purpose: Update on the current Phase 1/2a clinical trial of 186RNL administered by convection enhanced delivery (CED) to treat recurrent glioblastoma and other cancers.
Background: Rhenium-186 (186Re) (T½ 89.2 hours) with 10% 137 KeV γ-ray has pharmacokinetics similar to radioiodine and is in the same Periodic Table column as Technetium. Liposomes of ~100 nm diameter can be radiolabeled with 186Re using a previously described BMEDA method with > 80% labeling efficiency of the radiolabeled 186RNL. 186RNL enables localized cancer therapy via direct image-guided needle insertion with convective spread within the tumor and sustained retention in the tumor post-delivery. Uptake in the thyroid, salivary gland and stomach of metabolized 186Re, chemically analogous to free 99mTc, can be efficiently blocked by oral potassium iodine [KI] saturation thereby accelerating its rapid renal urinary 186Re clearance. This novel localized radio-nanotherapeutic approach has enormous potential in a large variety of tumors as either 186RNL or generator obtained 188RNL where local tumor control is difficult or all other therapies exhausted, ineffective or toxic. Repeat RNL therapy is possible as the 186RNL radiation dose is delivered directly, locally and safely.
Methods: A dose escalation study for treatment of recurrent glioblastoma has been performed through 7 cohorts with radioactivity and volumes of 186RNL gradually increasing from 1 mCi in Cohort 1 to 22.3 mCi in the 7th cohort at a concentration of 1.5 mCi/ml to 2.54 mCi/ml delivered intratumorally by convection enhanced delivery (CED). BrainLab iPlan Flow Software and a Varioguide system were used for treatment planning and catheter placement. To improve the tumor volume coverage in escalating cohorts, the catheters were increased from 1 to 3-4 catheters starting from cohort #4. During cohort progression the rate of administration increased from 5 ml/min to 20 ml/min.
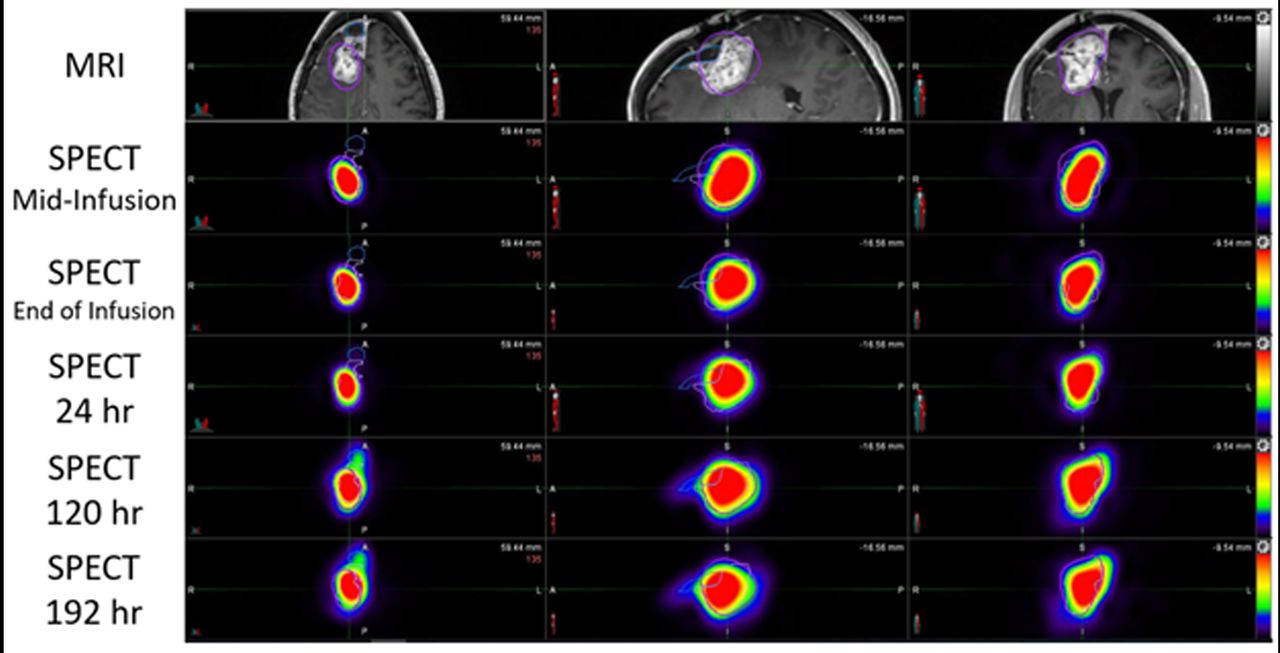
Results: SPECT/CT images fused to MRI and whole-body imaging, revealed sustained locoregional retention and distribution in the glioblastoma tumor over 8 days. The mean administered 186RNL locoregional retention in the tumor region at the end of infusion was 85.9% ± 17.1% ID (n = 18) and at 8 days post-infusion was 46.6% ± 16.7% ID (n = 17). Up to four catheters effectively enhanced locoregional drug distribution and tumor volume coverage. This increased rate of RNL administration and the use of multiple catheters decreased the average treatment time from > 8 hours to ~ 3 hours with 186RNL treated volume increasing to 54.2 ± 22.9 ml (n = 6) in cohorts 6 and 7). The cleared 186RNL was metabolized and rapidly excreted from the body via the kidneys like 131I with 186Re excretion being enhanced when saturating KI doses were pre-administered. Following 5th-7th cohorts dose escalation, the mean radiation absorbed dose delivered directly to the tumor volume increased to 354.7 ± 144.0 Gy, while whole brain was 1.32 ± 1.06 Gy, and whole body was 0.16 ± 0.04 Gy (n = 6). Initial treatment results are very encouraging with a 13-patient subset receiving a radiation dose >100 Gy with an average 487 day survival with 6 of 13 patients in this subset still alive. In contrast, in 9 patients receiving radiation doses of <100 Gy, average survival was 167 days with no patients remaining alive. Importantly, no clinically meaningful SAEs, AEs, or tolerability observations have been reported.
Conclusions: 186RNL provides local, direct therapy with high radiation absorbed doses for local tumor control with minimal brain and whole-body radiation exposure. In this preliminary Phase I/2a data, beneficial effects were observed when doses > than 100 Gy dose are delivered to >80% of a tumor without dose-limiting toxicity. Future studies are planned with 186RNL including leptomeningeal metastasis treatment (NCT05034497 at clinicaltrials.gov). 186RNL therapy is in late-stage planning for the treatment of childhood glioma.

In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.