


Abstract
A radionuclide methodology and reference values have been developed for a single gastrointestinal transit study including esophageal transit, liquid and solid gastric emptying, and small- and large-bowel transit, using 111In-diethylenetriaminepentaacetic acid (DTPA) with the standardized 99mTc-labeled solid meal. Methods: Eighteen healthy subjects and 18 patients were investigated. The esophageal transit study was performed with 3.7 MBq (0.1 mCi) of 111In-DTPA in 15 mL of water. A liquid-only 30-min gastric-emptying study followed, with ingestion of 3.7 MBq (0.1 mCi) of 111In-DTPA in 300 mL of water. Then, a simultaneous solid–liquid emptying study was acquired after ingestion of a solid 99mTc-sulfur colloid–labeled meal and 7.4 MBq (0.2 mCi) of 111In-DTPA in 120 mL of water. Images were acquired intermittently for 4 h. Additional 111In images were acquired at 5 and 6 h to measure small-bowel transit, and at 24, 48, and 72 h for large-bowel transit. Results: Reference values were determined for esophageal transit (transit time, percentage emptying at 10 s), liquid-only gastric emptying (emptying half-time), liquid and solid emptying in a dual-phase solid–liquid study (emptying half-time and percentage emptying at 1, 2, 3, and 4 h), small-bowel transit index (percentage transit to ileocecal valve at 6 h), and colonic transit (geometric center and percentage colonic emptying) at 24, 48, and 72 h. Results from the first 18 patients found abnormal transit in 72% (13/18); clinical management changed in 61% (11/18). Conclusion: We have developed a radionuclide methodology and derived reference values for a comprehensive gastrointestinal transit study using 111In-DTPA with the standardized 99mTc-labeled solid meal. Our initial clinical experience suggests clinical value.
Patients with symptoms of early satiety, postprandial abdominal discomfort, bloating, fullness, and nausea are referred for radionuclide gastric-emptying studies for suspected gastroparesis (delayed gastric emptying), a functional disorder usually without anatomic correlation. However, until recently, gastroparesis was diagnosed by the study in only 20%–40% of patients (1).
Recent progress has been made in improving the diagnostic yield of the test. Extending the study from 2 to 4 h has increased the diagnosis of gastroparesis by a third (2–4). Liquid gastric-emptying studies can further increase detection of gastroparesis by another third (5–7). Still, in many patients the cause of their symptoms goes undiagnosed.
Gastrointestinal symptoms are often nonspecific as to the organ of origin. Dyspeptic symptoms are common in both gastric and small-bowel dysmotility and are reported with esophageal dysmotility. Although constipation and diarrhea predominate in large-bowel transit disease, these patients often have symptoms that overlap with those of the upper gastrointestinal tract. Transit abnormalities may occur in more than one gastrointestinal organ. If we could routinely investigate patients for small- and large-bowel dysmotility in addition to gastric emptying, we might be able diagnose additional patients with functional gastrointestinal disease.
Conventional intestinal transit studies such as the hydrogen breath test, radiopaque markers, and wireless motility capsules can be invasive, costly, have a high radiation dose, or be of limited reliability and nonphysiologic (8,9). Radionuclide methods studying intestinal transit have been published, but few centers offer them and there is no standard methodology or generally applicable reference values, although a practice guideline was recently published (10).
The purpose of this investigation was to develop a physiologic radionuclide methodology and establish reference values for a comprehensive gastrointestinal transit clinical study, including esophageal transit, liquid and solid gastric emptying, and small- and large-bowel transit, using 111In-diethylenetriaminepentaacetic acid (DTPA) in conjunction with the consensus-recommended standardized 99mTc-labeled solid meal (11–13) and to present our initial clinical experience.
MATERIALS AND METHODS
Study Population
Eighteen healthy subjects (10 men, 8 women; age range, 20–57 y; mean ± SD, 33.6 ± 11.9 y) were enrolled. The Mayo Clinic Research Questionnaire was used to interview and screen them. The subjects had no history of gastrointestinal disorders or prior surgery, were on no medications, and did not smoke or abuse alcohol. The investigational protocol was approved by the Johns Hopkins University Institutional Review Board. Written informed consent was obtained. The initial 18 consecutive patients (5 men, 13 women; age range, 20–72 y; mean, 52.6 ± 16.4) were referred because of a variety of gastrointestinal symptoms (Table 1).
Clinical Patient Results
Methodology
All subjects and patients were instructed to fast overnight before the study. Patients took medications prescribed by their referring physicians.
A dual-head large-field-of-view γ camera with medium-energy collimators was used. Images were acquired with a 20% window around the photopeaks of 99mTc (140 keV) and 111In (171, 245 keV).
Esophageal Transit
Two practice swallows (15 mL of water) with a 15-s delay between swallows were followed by a third (111In-DTPA, 3.7 MBq [0.1 mCi] in 15 mL of water). Data acquisition began before the third swallow, and 60 frames of 0.5 s each (64 × 64) were acquired posteriorly with the subject standing. The field of view included the mouth through the upper stomach.
To process, a region of interest (ROI) was drawn around the esophagus from the level of the cricoid to the lower esophageal sphincter using Xeleris esophageal swallow software (GE Healthcare). Both esophageal transit time (time for activity to decrease to 10% of peak) and percentage esophageal emptying (% activity decrease from peak over 10 s) were calculated.
Liquid-Only Gastric Emptying
A 30-min liquid-only study was acquired (1-min frames, 64 × 64) after ingestion of 300 mL of water with 111In-DTPA (3.7 MBq [0.1 mCi]). Patients were imaged while semiupright (45%), lying supine on a hospital gurney, with the γ camera placed in the left anterior oblique position. To process, a ROI was drawn for the stomach. The half-time of emptying and a fitted exponential half-time were determined.
Combined Liquid–Solid Gastric Emptying
Subjects ingested the standardized 99mTc-sulfur colloid (7.4 MBq [0.2 mCi]) egg-substitute solid meal (113 g [4 oz] of Optimum Choice; Sysco Corp.), 2 slices of toast, 30 g of strawberry jam (11–13), and 120 mL of water mixed with 111In-DTPA (7.4 MBq [0.2 mCi]). Anterior and posterior simultaneous dual-isotope images were acquired at 0.0, 0.5, 1.0, 1.5, 2, 3, and 4 h. Processing used gastric-emptying software (GE Healthcare) with decay and geometric mean attenuation correction.
To process the liquid portion of the study, the half-emptying time, fitted exponential half-time, and percentage gastric emptying were calculated at each time point. The solid meal was processed similarly, except using a fitted linear half-time.
Patients were instructed not to eat until imaging was concluded on day 1 of the study, but they were allowed to go about normal activities in the clinic vicinity.
Small-Bowel Transit
At 5 and 6 h after meal ingestion, static anterior and posterior 1-min images (128 × 128) were acquired. A small-bowel transit index (SBTI) was determined. To establish counts in the small bowel available to fill the terminal ileum, an ROI was drawn to include the entire abdomen to calculate a decay-corrected geometric mean average of total abdominal counts between 2 and 5 h, corrected for gastric counts. On the 6-h image, an ROI was drawn around the ileocecal valve or cecum and around any colonic activity. The terminal ileum or cecum was located by observing progressive focal accumulation in the right lower quadrant during the first 6 h of imaging.
To test interobserver bias, 3 residents independently drew the ROI, confirming their choice by observing subsequent transit in the expected large-bowel pattern in the 24-, 48-, and 72-h anterior and posterior images.
SBTI was calculated by dividing the geometric mean (decay-corrected) percentage 111In activity that had passed into the area at 6 h by the mean 2- to 5-h abdominal activity. Calculations were facilitated by the use of an Excel worksheet (Microsoft) with decay correction factors.
Large-Bowel Transit
At 24, 48, and 72 h, 5-min images (128 × 128) were acquired in the anterior and posterior views. Geometric mean attenuation and decay correction was performed. Two quantitative methods were performed with the healthy subjects.
First, the geometric center (GC) was determined. The large intestine was manually divided into 7 ROIs (ascending, hepatic flexure, transverse, splenic flexure, descending, rectosigmoid, and excreted activity). The count in each of the 7 segments was multiplied by its corresponding factor (1–7) and then summed. The percentage activity for each segment was calculated as the count in that segment divided by the initial count (average of total abdominal counts between hours 2 and 5). The GC represented a number between 1 and 7.
Second, percentage colonic emptying at 24, 48, and 72 h was determined. A ROI was drawn around the entire abdomen at each period. The percentage emptying was calculated using gastric-emptying software by dividing the geometric mean counts at each time point by the amount of initial activity in the colon using the 2- to 5-h average counts, including any gastric counts, and in a separate calculation using the 6-h total counts. The results of the 2 calculations were compared.
Jaszczak Phantom Study
The percentage spillover of one isotope into the window setting of the other was investigated using 42.2 MBq (1.14 mCi) of 111In and 41.8 MBq (1.13 mCi) of 99mTc. 99mTc spillover into the 111In window was 2.5% of total 111In counts, whereas 111In spillover into the 99mTc window was 33.1% of total 99mTc counts. The 5:1 ratio of 99mTc to 111In in our experimental study would result in a maximum 99mTc spillover of 12.5% and a minimum 111In spillover of 6.6%. As 99mTc decays more quickly than 111In, the percentage of spillover from either isotope is expected to range between 6.6% and 12.5% during the gastric-emptying and small-bowel transit portions of the study.
Statistical Analysis
Data are presented as mean ± SD for central tendencies, as median and range when data were skewed, and as frequency and percentage for categoric variables. Between groups, analyses were performed using independent-sample t tests. Statistical significance was set at a 2-tailed P value of 0.05 for all tests. The Shapiro–Wilk test of normality was used. Interobserver analysis was performed using Bland–Altman plots and the Pittman test of difference in variance. All statistical analysis was performed with the JMP statistical package (version 11.0; SAS Institute, Inc.).
The decision on how to best determine reference values was based on the test for normality. Normal was defined as the mean ± 2 SDs in a parametric sample and as the 95% confidence interval in a nonparametric sample.
RESULTS
All 18 subjects completed the study. Table 2 displays the transit results of the healthy subjects; Table 3 the calculated reference values.
Transit Parameters
Reference Values
Esophageal Transit
A good swallowed bolus was uniformly observed, and interpretable time–activity curves generated.
Liquid-Only Gastric Emptying
The time–activity curves usually demonstrated a single-exponential emptying pattern in healthy subjects. Occasionally, overlapping small bowel delayed apparent emptying.
Combined Liquid–Solid Gastric Emptying
Liquid Emptying
Time–activity curves demonstrated a multiexponential emptying pattern. Normal liquid emptying was slower in the combined study than in the liquid-only study (mean half-time, 38.8 vs.14.3 min) (P < 0.0001). Liquid half-time emptying was significantly different without the 0.5- and 1.5-h data points (P = 0.0003). For clinical patients, we now image only at 0, 1, 2, 3, and 4 h, using the half-time derived from these time points. Because of the rapid emptying of liquids, the best estimate of liquid emptying was at 1 h.
Solid Emptying
The percentage emptying and half-emptying time at each time point were similar and not significantly different from the published standardized meal data. Thus, for clinical purposes we use the references values of Tougas et al. (11). Unlike liquid emptying, for solid emptying the half-time was not affected by the selection of fewer time points (P = 0.57).
Small-Bowel Transit
An interobserver study (3 residents) showed good correlation for drawing ROIs, with a mean bias of 7.3%–14.8% (Pittman test, P = 0.4–0.9). With some experience, our technologists usually accurately draw the ROIs.
Large-Bowel Transit
For large-bowel transit, interobserver agreement for the GC was not significantly different for 24- and 48-h measurements (mean bias, 0.06–0.6) but was significantly different for 72 h (mean bias, 0.03–0.19; Pittman P = 0.03–0.21). There was good correlation between the GC determination and the percentage colonic emptying at 24, 48, and 72 h (24-h R2 = 0.70; 48-h R2 = 0.90; 72-h R2 = 0.95; all P < 0.0001).
Using the 2- to 5-h and 6-h input, the counts to calculate percentage emptying were not significantly different (P = 0.7820). The 6-h counts are now routinely used for clinical studies. Reference intestinal transit values are shown in Figures 1 and 2.
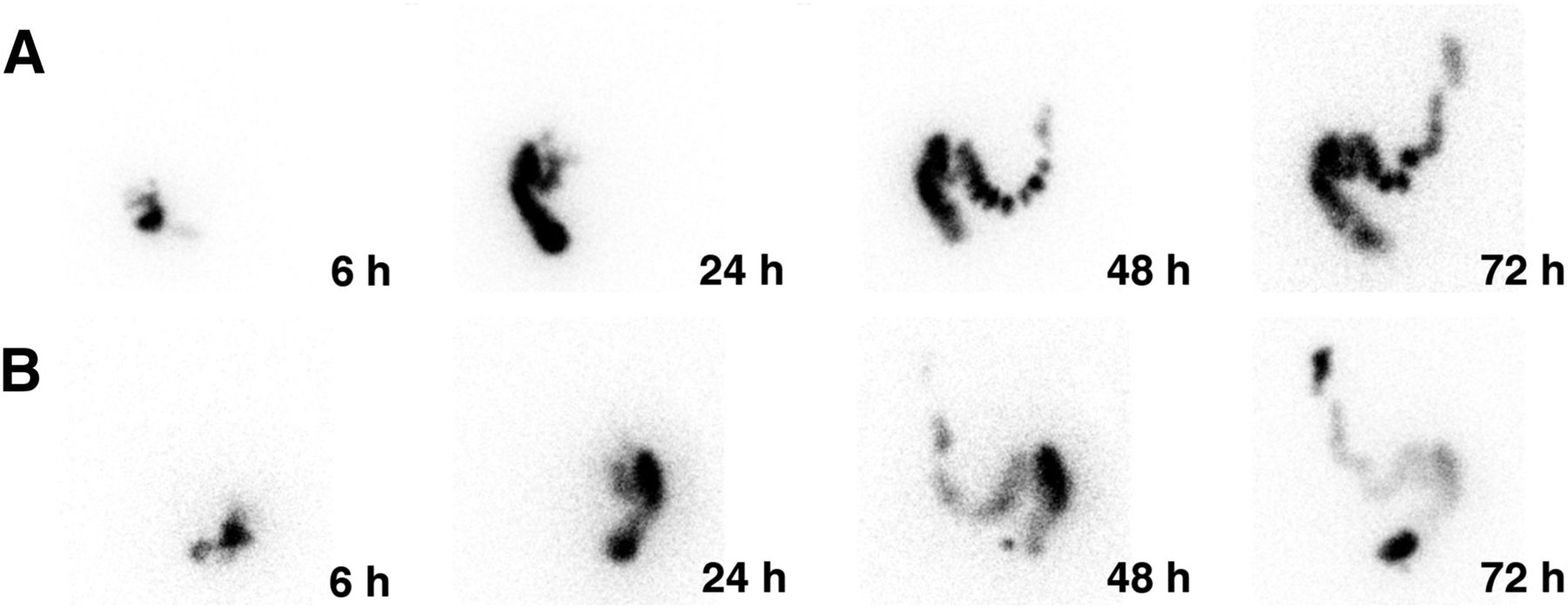
Normal small-bowel transit. Anterior (A) and posterior (B) views are shown, with ROI drawn around ileocecal value and cecum to calculate SBTI.

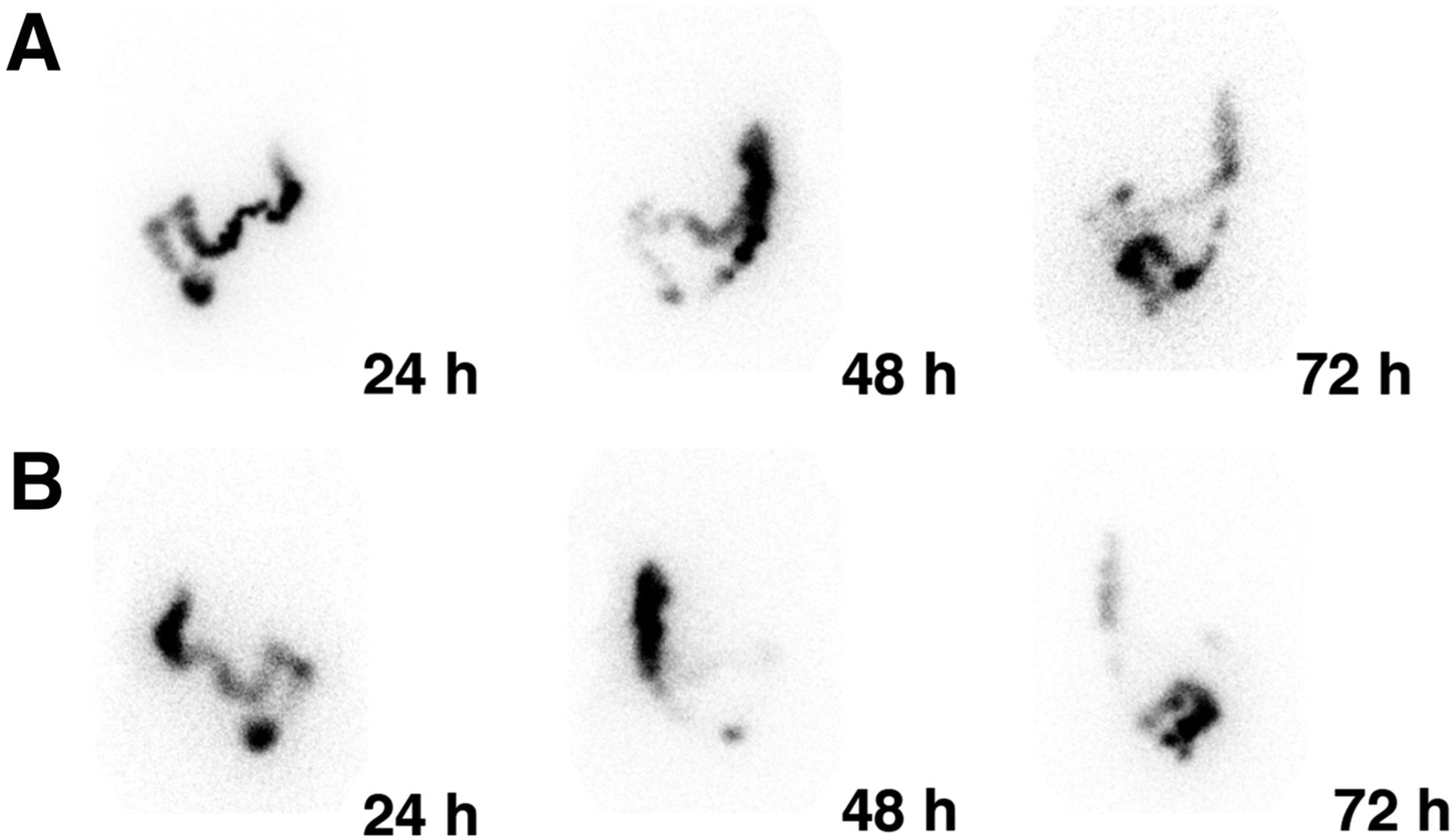
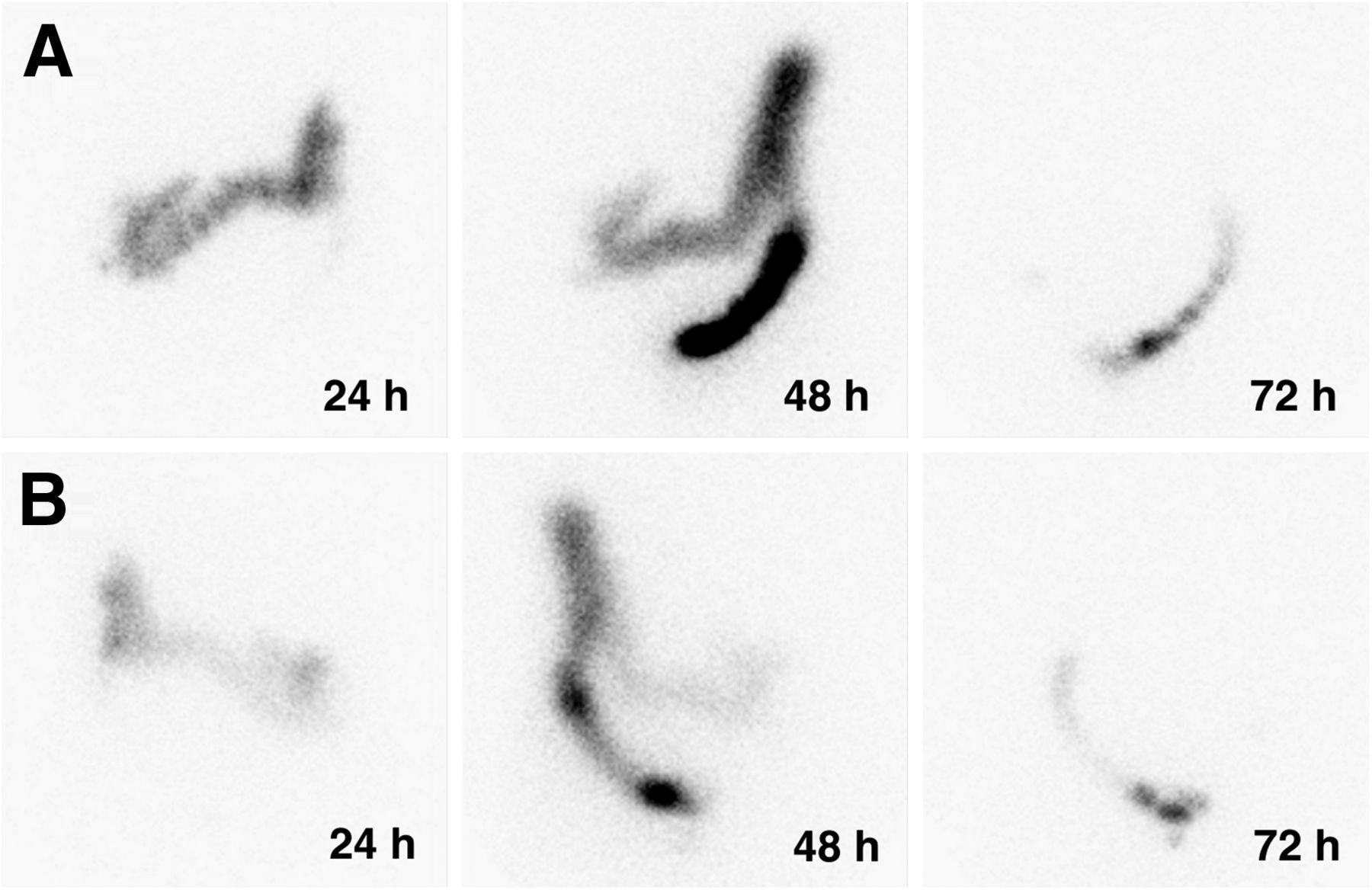
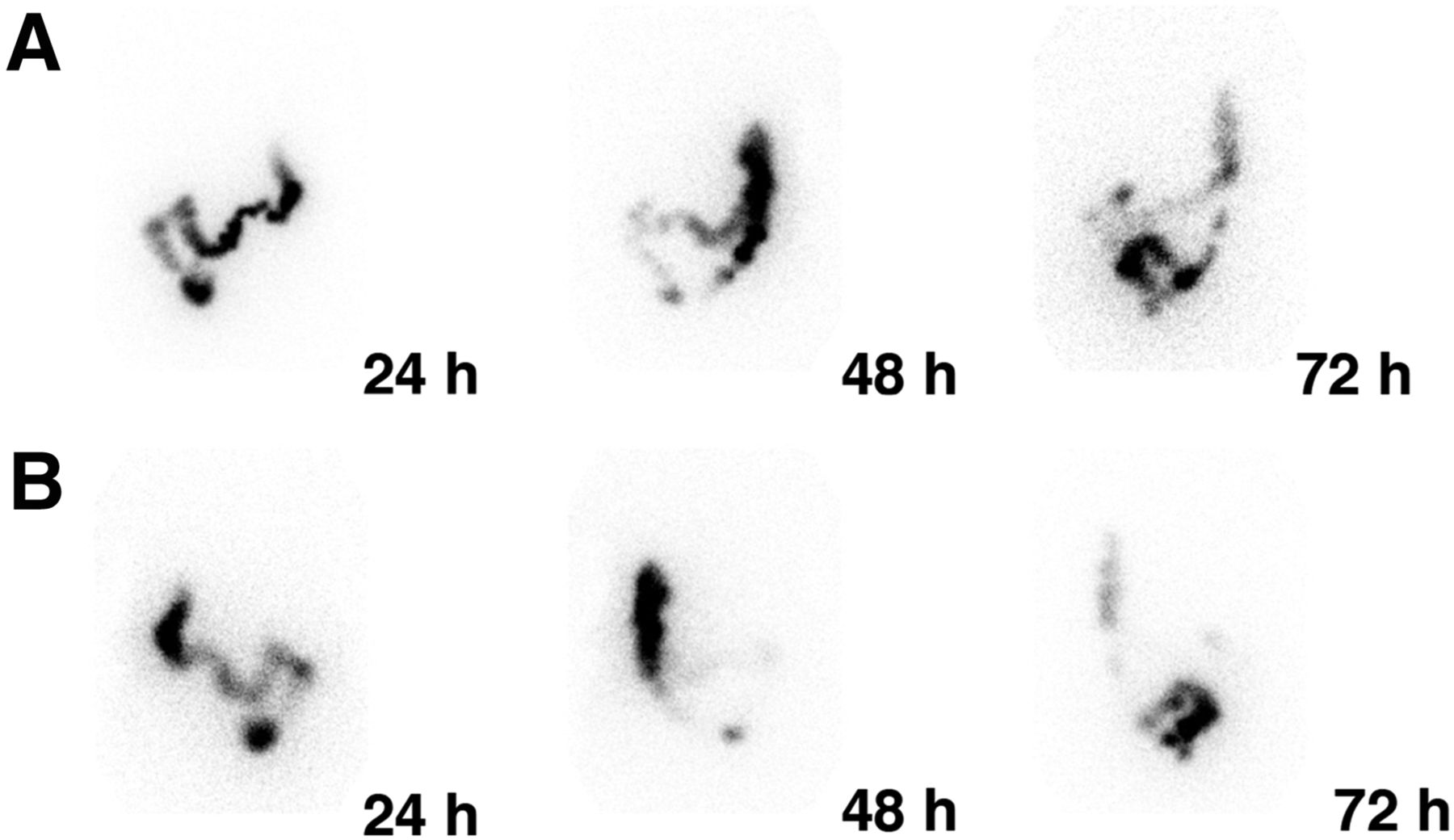
Normal large-bowel transit. Anterior (A) and posterior (B) views at 24, 48, and 72 h are shown. Most activity is in transverse colon by 24 h, in descending colon by 48 h, and in rectosigmoid colon or excreted by 72 h.
Clinical Results
Of the first 18 patients, 72% (13/18) had abnormal transit in at least one gastrointestinal organ; 33% (6/18) had abnormal transit in more than one organ, 28% (5/18) had normal transit (Table 1). Examples of abnormal transit are shown in Figures 3–7. As a result, there was a subsequent change in diagnosis in 67% of patients (12/18) and a change in management in 61% (11/18).

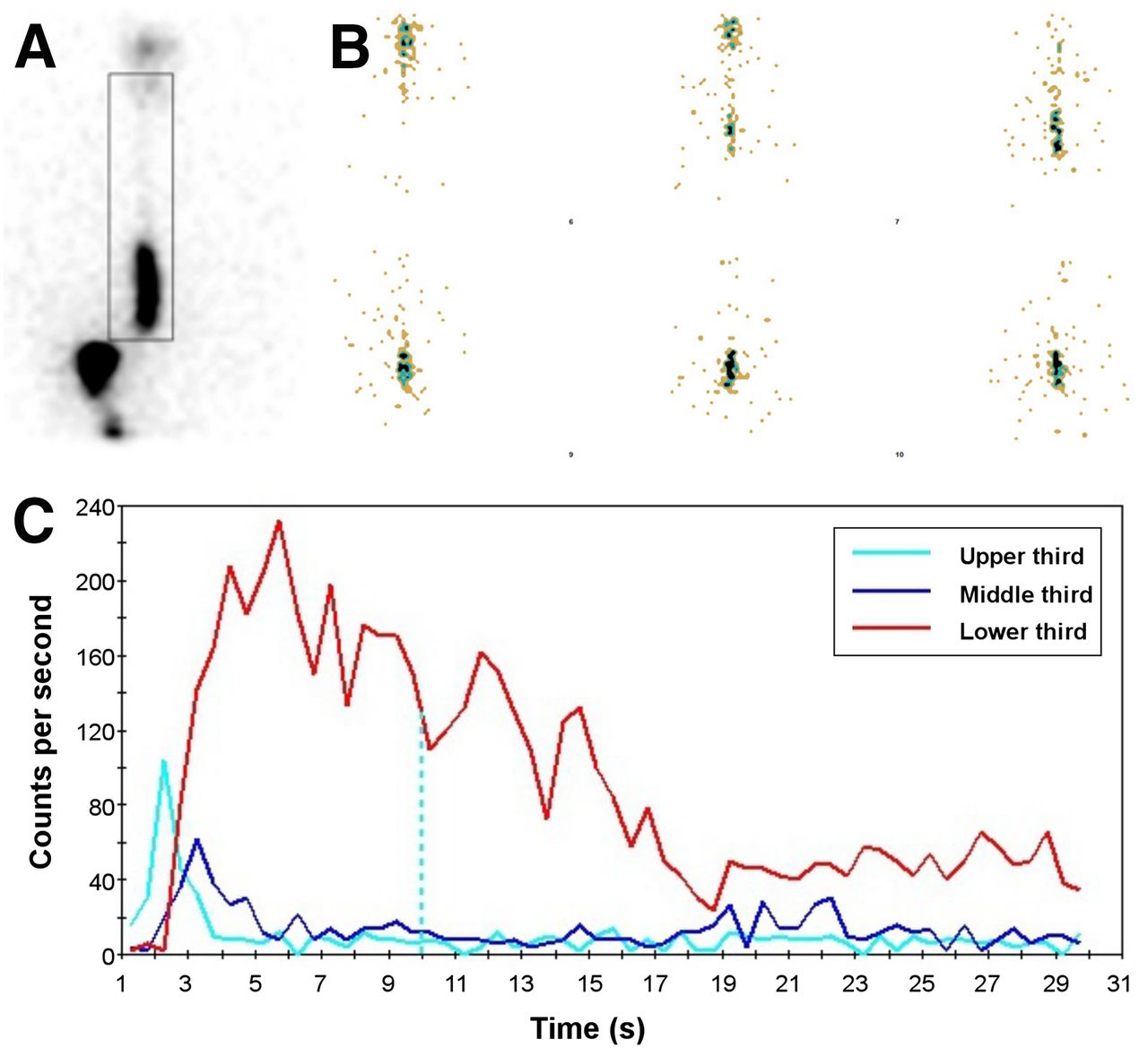
Delayed esophageal transit. (A) Summed image demonstrates delayed transit through lower third of esophagus. (B and C) Dynamic 0.5-s frames show rapid transit through first two thirds of esophagus in 1–2 s but slow transit in distal third (B), confirmed by time–activity curve (red) (C). Esophageal transit time (ETT) was not reached by 30 s. Percent esophageal emptying (%EE) at 10 s was 54% (normal > 83%).
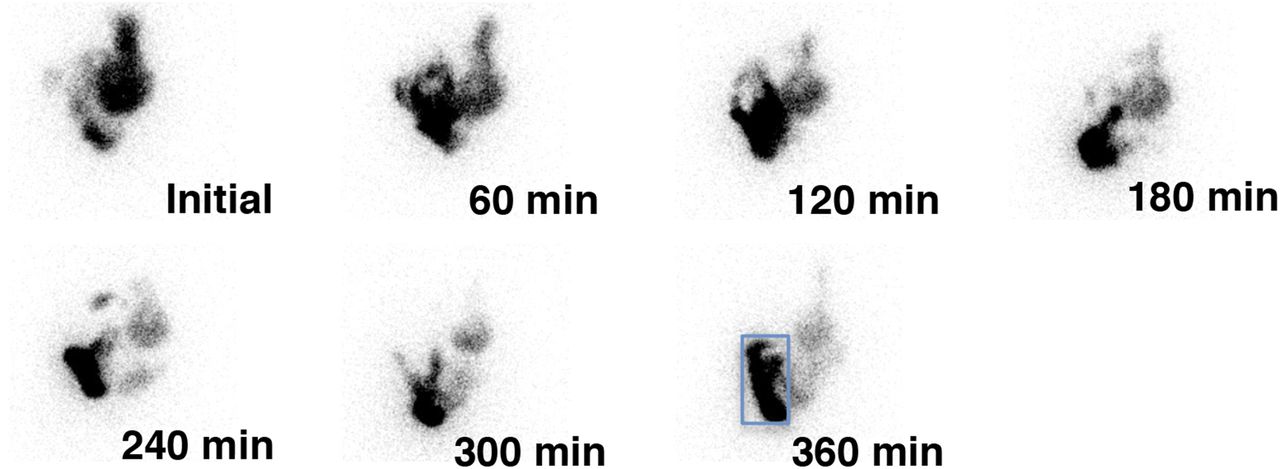
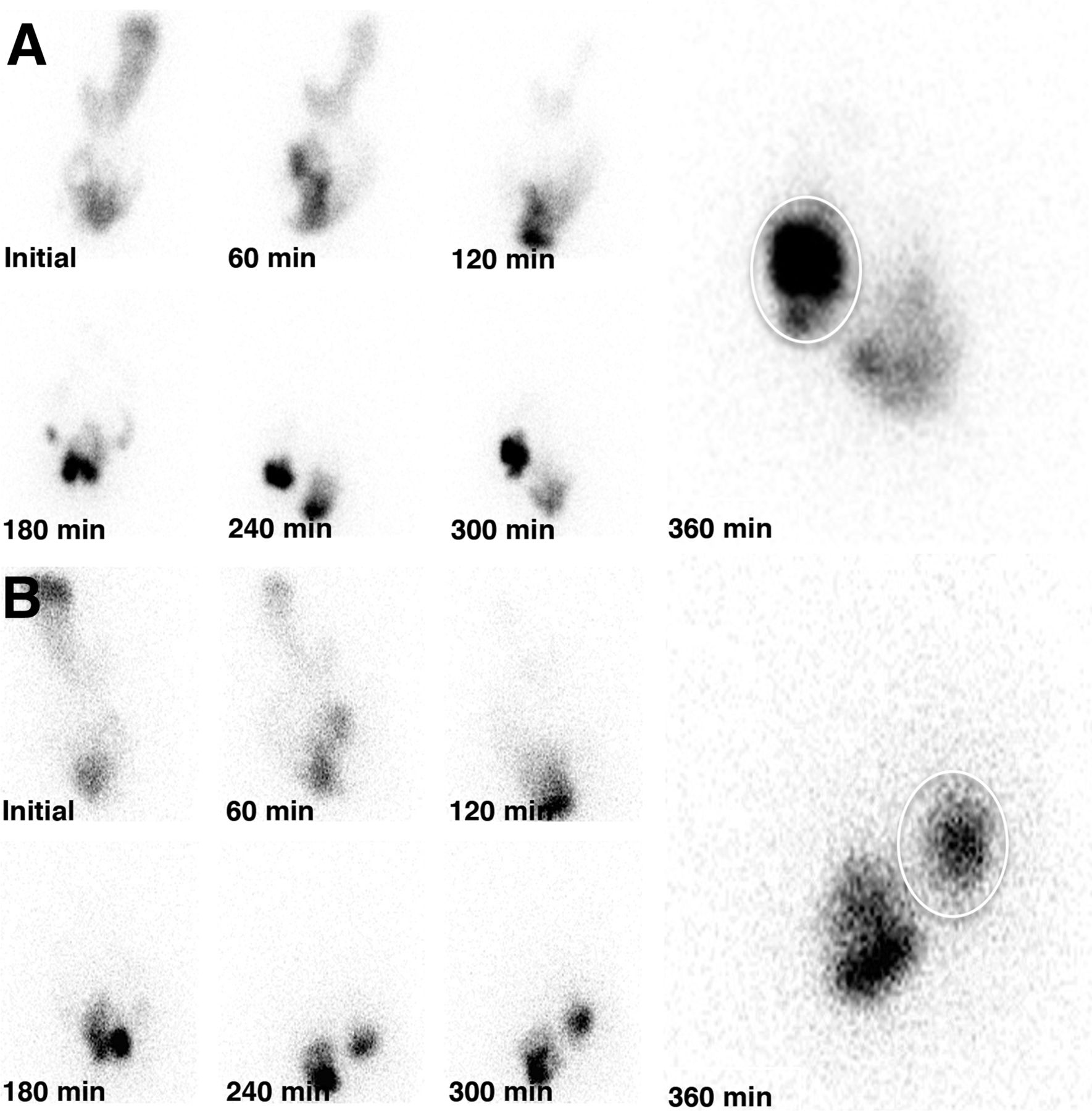
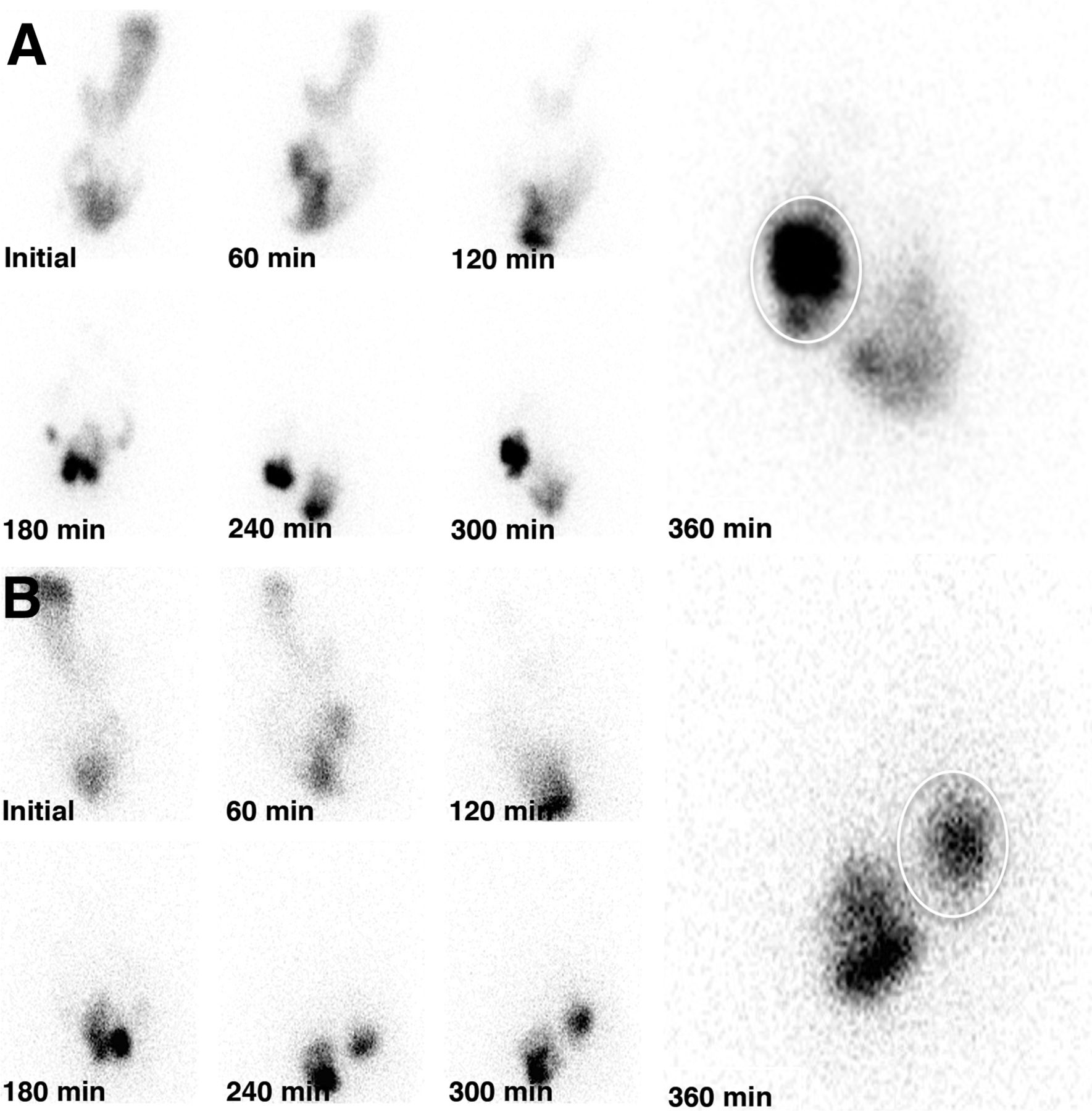
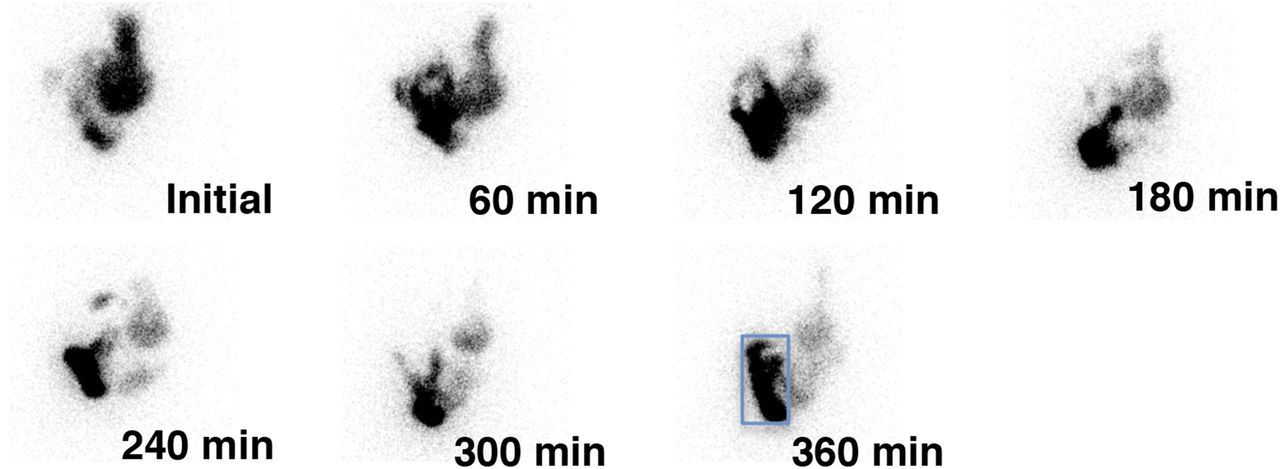
Small-bowel transit study corrected for delayed gastric transit. Patient had delayed gastric emptying in liquid-only study, liquid portion of combined liquid–solid study, and solid study. 111In counts in stomach are subtracted from total average counts between hours 2 and 5, correcting small-bowel transit for gastric emptying. This patient had normal SBTI of 82% (normal > 50%). Blue rectangle denotes ileocecal/ascending colon ROI for calculation of SBTI.
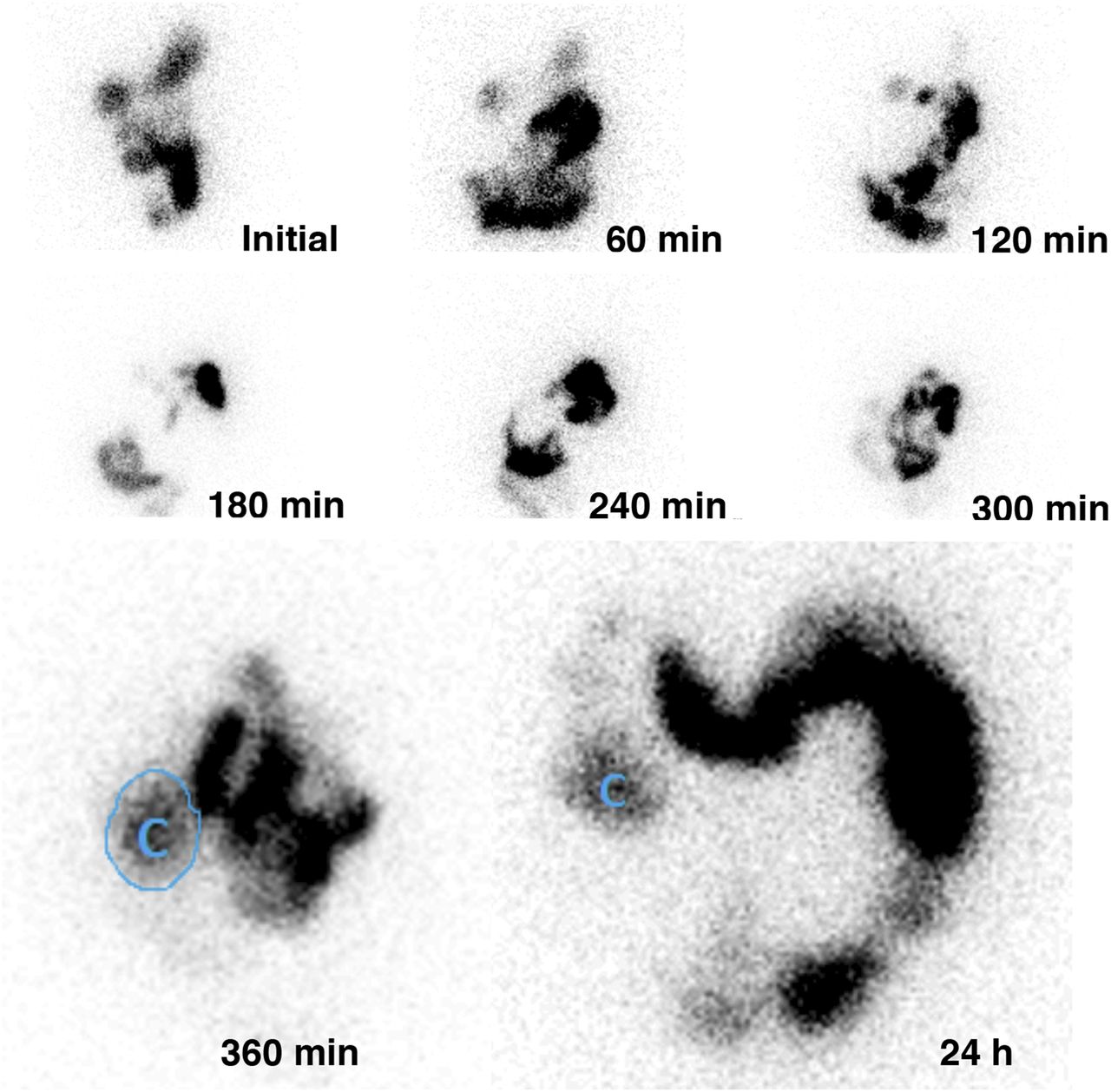
Delayed small-bowel transit. Anterior views are shown of patient with delayed SBTI (28%). At 360 min, ROI shows activity reaching cecum (C). Large-bowel emptying (84%) is normal.

Delayed large-bowel transit. Anterior (A) and posterior (B) projection images show delayed ascending and transverse colonic transit. Little to no activity has transited into descending colon by 72 h.
Delayed rectosigmoid transit. Anterior (A) and posterior (B) images show only 5% large-bowel transit by 72 h, with most activity seen just proximal to mid-to-distal rectosigmoid colon.
DISCUSSION
In this paper, we have described our methodology for a scintigraphic comprehensive gastrointestinal transit study, reported reference values we determined from 18 healthy subjects, and related our initial clinical experience in 18 patients.
The methodology is unique in that it evaluates transit from esophagus to rectum, using 111In-DTPA for esophageal, liquid gastric, and small- and large-bowel transit, in conjunction with the standardized 99mTc-sulfur colloid–labeled solid meal and methodology recommended by the American Neurogastroenterology and Motility Society and the Society of Nuclear Medicine and Molecular Imaging, based on Tougas et al. (11–13).
Clinical indications for a comprehensive gastrointestinal transit study include suspected pandysmotility with overlapping regional symptoms, small-bowel dysmotility and therapy response for bacterial overgrowth, dysmotility in autoimmune (scleroderma) or other disorders (Ehlers-Danlos syndrome), and preoperative evaluation (achalasia, colonic inertia).
The first published study combining radionuclide gastric emptying and a small- and large-bowel transit study was in 1975 (14). Various methodologies and reference values have been described since (15,16). To date, there is no standard methodology. Only a few institutions routinely perform “whole gut transit scintigraphy” (17,18). Our methodology differs from others previously described in several ways.
First, an esophageal transit study is performed. This initial 30-s study serves as a rapid screening test for delayed transit. It is a well-validated simple, short add-on to the comprehensive study. Numerous publications have shown it to have a high sensitivity as a stand-alone test for detecting esophageal transit disorders (19,20). The method used is similar to methods previously described, and the reference values are consistent with previous literature (21–24).
The radionuclide methodology has been the gold standard for gastric-emptying evaluation for decades (25,26). Before the published consensus recommendations, imaging clinics used various meals with different food content, often considerably higher in fat. In this comprehensive protocol, we have used the recommended standardized methodology and meal for the solid portion of the study, which is low in fat. The specific solid meal matters because it determines the rate of both solid and liquid emptying. The larger the meal, the greater the calories, carbohydrate, and fat consumed, and the slower the solid and liquid gastric emptying, and vice versa (27). To our knowledge, our comprehensive transit study is the first to publish and document reference values for liquid gastric emptying and small- and large-bowel transit using 111In-DTPA in conjunction with the standardized solid meal.
Two different dual-isotope dual-phase approaches to liquid gastric emptying have been described using 111In-DTPA in water and a 99mTc-labeled solid meal. One method begins with a 30-min liquid-only study followed by the solid study (5,6). The other approach is to simultaneously administer the dual-isotope solid and liquid meal (7). Liquid-only studies have been shown to be more sensitive for detection of gastroparesis than the solid study using the sequential method (5–6), and both methods detect gastroparesis in 28%–32% of patients with normal solid emptying (5–7). The prior teaching was that liquid emptying is not delayed until after solid emptying becomes abnormal (28,29).
In this comprehensive protocol, both methods were performed sequentially. We found that the liquid-only study emptied normally in a monoexponential pattern, whereas the combined liquid–solid study had a multiexponential clearance pattern. Liquid-only emptying had a shorter mean half-emptying time (14 vs. 39 min, P < 0.0001) than the liquid in the combined liquid–solid meal, raising the question of whether the two different methods measure the same physiology.
The reference liquid-emptying values for this liquid–solid study are different from those previously reported. The lower limit of normal was 40% emptying at 1 h versus 50% published previously (7). One explanation may be that our reference values were determined using the consensus standardized solid meal (18).
Reference values for the standardized solid meal were not significantly different from those published by Tougas et al. (11). Even though our patients ingested a larger volume of water, 345 mL (esophageal, liquid only, and liquid–solid) compared with the 120 mL of water recommended, there was no effect on our solid-emptying results, consistent with previous reports that solid transit is not affected by the addition of liquid (30).
To quantify small-bowel transit, various methods have been used. One approach has been to calculate orocecal transit time, that is, the time for radionuclide to accumulate in the cecum or the cumulative percentage entry into the colon over time (18,31). This method has shown a generally good correlation with the hydrogen breath test (32). Another method has used SBTI, that is, the percentage activity that reaches the ileocecal value by 6 h (33). The latter method was chosen for this investigation. Our results differ from those that have been reported. We found normal small-bowel transit to be more than 50% at 6 h; others using similar 111In methodology, but administering a whole-egg meal, reported reference values of more than 40% (28).
To investigate large-bowel transit, 111In-DTPA has been instilled directly into the proximal large bowel via cecal intubation (34). Although this is likely an accurate method, it is invasive and not practical clinically. Two different oral ingestion methodologies using different radiopharmaceuticals have been described. One has patients ingest a pH-sensitive methacrylate-coated capsule containing 111In-labeled activated charcoal particles (17). The capsule dissolves at the pH of the large bowel (7.4), and the 111In is released into the cecum.
An alternative method has been to administer the 111In-DTPA in water with a solid meal and follow its transit with imaging at various time points (18,34). For colonic transit, the GC of activity has been used (28). We found this methodology demanding and time-consuming for technologists and physicians. Drawing multiple ROIs was not always reproducible.
Therefore, percentage colonic emptying at 24, 48, and 72 h was chosen. The 6-h counts were used as the initial counts. The entire field-of-view ROI measured percentage large-bowel emptying using commercially available gastric-emptying software. For interpretation, we first determine whether there is a quantitative delay in percentage emptying at any of 3 time points. We then provide additional qualitative visual assessment to distinguish between diffuse colonic delay and a regional abnormality, for example, the rectosigmoid colon. On the basis of the lower 95% confidence interval of calculated GC, our data show that healthy patients have most activity in or distal to the transverse colon by 24 h, descending colon by 48 h, and rectosigmoid colon by 72 h. The percentage colonic-emptying method correlated well with the GC method.
The results in 18 patients suggest clinical value for our methodology for diagnosing various esophagogastrointestinal dysmotility disorders (Table 1).
CONCLUSION
A radionuclide methodology and reference values have been described for a comprehensive clinical gastrointestinal transit study that includes esophageal transit, liquid and solid gastric emptying, small-bowel transit, and large-bowel transit, using 111In-DTPA in conjunction with the consensus-recommended standardized 99mTc-labeled solid meal. Our preliminary experience suggests its clinical value.
DISCLOSURE
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734. No potential conflict of interest relevant to this article was reported.
Acknowledgments
We acknowledge the hard work and dedication of the Johns Hopkins nuclear medicine technologists as we translated this project from research into clinical use.
Footnotes
Published online Mar. 12, 2015.
- © 2015 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication November 25, 2014.
- Accepted for publication January 14, 2015.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Abnormal gastrointestinal motility is a major factor in explaining symptoms and a potential therapeutic target in patients with disorders of gut-brain interaction
- A Syndrome of Joint Hypermobility, Autonomic Dysfunction, Gastrointestinal Dysfunction and Autoimmune markers (JAG-A): Clinical Associations and Response to Intravenous Immunoglobulin Therapy
- Experience with Esophagogastrointestinal Transit Scintigraphy in the Initial 229 Patients: Multiple Regions of Dysmotility Are Common
- Gastrointestinal Motility, Part 1: Esophageal Transit and Gastric Emptying
- Gastrointestinal Motility, Part 1: Esophageal Transit and Gastric Emptying
- Will Comprehensive Assessment from Esophagus to Large Bowel Revive the Momentum for Radionuclide Gastrointestinal Transit Studies?