


Abstract
In patients with acute myocardial infarction (AMI) before primary coronary stenting with adjunct glycoprotein IIb/IIIa receptor blockade, whether residual blood flow in the infarct-related artery (IRA) affects infarct size or myocardial salvage is not known. Methods: This study included 118 patients with ST-segment elevation AMI who received coronary stenting plus abciximab. SPECT studies were performed before and 7–14 d after stenting. Results: Patients were divided into a group with initial Thrombolysis in Myocardial Infarction (TIMI) flow grade ≤ 1 (77 patients) and a group with initial TIMI flow grade > 1 (41 patients). The initial median perfusion defect and (in brackets) the 25th and 75th percentiles were 29.1% [21.0%; 52.0%] of the left ventricle in patients with TIMI flow grade ≤ 1, versus 16.5% [8.0%; 33.1%] of the left ventricle in patients with TIMI flow grade > 1 (P < 0.001). Baseline left ventricular ejection fraction (54.0% [45.0; 63.0] vs. 57.0% [40.0; 62.0], P = 0.623) or extension of hypokinetic region (28.0 [14.0; 41.0] hypokinetic chords vs. 24.0 [13.0; 39.0] hypokinetic chords, P = 0.643) did not differ significantly between the group with TIMI flow grade ≤ 1 and the group with TIMI flow grade > 1. Final infarct size was 11.0% [6.1%; 23.5%] of the left ventricle in the group with TIMI flow grade ≤ 1, versus 6.0% [2.0%; 12.8%] of the left ventricle in the group with TIMI flow > 1 (P = 0.008). Salvage index was 0.58 [0.38; 0.76] in the group with TIMI flow grade ≤ 1, versus 0.61 [0.36; 0.74] in the group with TIMI flow grade > 1 (P = 0.952). At the day 14 angiography, patients with TIMI flow grade > 1 had better left ventricular ejection fraction (61.0% [54.0%; 68.0%] vs. 56.5% [42.9%; 65.0%]; P = 0.03) and a smaller hypokinetic region (7 chords [0; 22.0] vs. 16 chords [2.5; 30.0]; P = 0.024) than did patients with TIMI flow grade ≤ 1. Conclusion: Preserved blood flow in the IRA in patients with AMI is associated with a smaller area at risk, a smaller infarct, and better recovery of regional and global left ventricular function. The proportion of initial area at risk salvaged by coronary stenting does not seem to depend on residual blood flow in the IRA.
Earlier studies demonstrated that in the infarct-related artery (IRA) at the time of percutaneous coronary interventions, the presence of residual blood flow, either spontaneously occurring or facilitated by pharmacologic agents, is associated with better clinical outcomes (1–3). The exact mechanisms that mediate these benefits, however, are still unclear. Two previous studies of patients with acute myocardial infarction (AMI) used SPECT to assess the influence on infarct size and myocardial salvage of residual blood flow in the IRA before mechanical revascularization with balloon angioplasty (4,5). Those studies included a limited number of patients with AMI (60 and 36 patients, respectively), and their results were partly discordant. Clements at al. demonstrated that patients with preserved blood flow (those with Thrombolysis in Myocardial Infarction [TIMI] flow grade > 1) had a smaller area at risk and greater myocardial salvage than did patients with TIMI flow grade 0 or 1 (4). Compared with the date at which that study was performed (early 1990s), today major advances in the field of mechanical reperfusion have occurred, particularly coronary stenting and modern antithrombotic therapy. Recently, Leoncini et al. used 99mTc-sestamibi gated SPECT to assess the influence of persistent blood flow before primary angioplasty on myocardial salvage and functional recovery in 36 patients with AMI (5). Those authors did not find significant differences in the initial perfusion defect (area at risk) among patients with initial TIMI flow grade ≤ 1 and those with TIMI flow grade > 1 (5). However, both studies reported greater myocardial salvage in patients with preserved blood flow in the IRA. Because predischarge coronary angiography was not performed, those studies provided no information on the predischarge TIMI flow grade or on how many patients underwent silent reocclusion. To our knowledge, no studies have used 99mTc-sestamibi SPECT to assess the impact on infarct size or myocardial salvage of residual blood flow in the IRA of AMI patients before coronary stenting with glycoprotein IIb/IIIa receptor blockade (abciximab). The aim of this study was to assess this impact and the impact on left ventricular functional recovery.
MATERIALS AND METHODS
Patients
This study included 118 AMI patients with ST-segment elevation who presented within 12 h of symptom onset and underwent coronary stenting as part of a trial (i.e., either Stent versus Thrombolysis for Occluded Coronary Arteries in Patients with Acute Myocardial Infarction [STOPAMI] 1 or STOPAMI 2 (6,7)). The stenting arms in STOPAMI 1 and 2 included 152 patients. The present study did not include patients with previous myocardial infarction (15 patients) or with incomplete scintigraphy (initial scintigraphy, 8 patients; follow-up scintigraphy, 7 patients) or angiography (initial angiography, 1 patient; follow-up angiography, 3 patients). The diagnosis of AMI was established by chest pain lasting at least 20 min and associated with ST-segment elevation (at least 1 mm in 2 or more extremity leads or 2 mm in 2 or more contiguous precordial derivations) or new-onset left bundle branch block. The protocols of the original studies had been approved by institutional ethics committees.
Details of stent implantation have been published in the reports of the respective trials (6,7). Briefly, all patients received 500 mg of aspirin and 5,000 U of heparin intravenously in the emergency room. During the intervention, an additional dose of 2,500 U of heparin was applied intraarterially. Abciximab (ReoPro; Lilly Deutschland) was given as a bolus of 0.25 mg/kg, followed by continuous infusion at a rate of 10 μg/min for 12 h. Postinterventional antithrombotic therapy consisted of ticlopidine, 250 mg twice a day for 4 wk (in the patients of STOPAMI 1), or clopidogrel, 75 mg/d for 4 wk (in the patients of STOPAMI 2), and aspirin, 100 mg twice a day, indefinitely.
Scintigraphic Study
Before stenting, patients received an intravenous injection of 1,000 MBq (27 mCi) of 99mTc-sestamibi. SPECT was performed within 6–8 h after injection of the radioactive agent. Follow-up myocardial scintigraphy was scheduled 7–14 d after the stenting procedure. A multihead camera system, equipped with low-energy, high-resolution collimators, was used for myocardial imaging. Images were acquired in a 64 × 64 matrix at an acquisition time of 40 s per image. With dedicated software (ICON version 6.0.2; Siemens Medical Systems), transaxial slices were reconstructed. A volumetric sampling tool was applied to create polar maps of relative distribution throughout the entire left ventricle. Each polar map was normalized to its individual maximum. A defect was defined as an area with <50% uptake. The 50% threshold was based on phantom studies performed at the Klinik und Poliklinik für Nuklearmedizin rechts der Isar Technische Universität using previously described methods (8,9). Four parameters were obtained using paired scintigraphic examinations: initial perfusion defect (perfusion defect on initial scintigraphy), final infarct size (perfusion defect on follow-up scintigraphy), absolute salvage (initial perfusion defect minus final infarct size), and salvage index (initial perfusion defect minus final infarct size divided by initial perfusion defect). The first 3 parameters were expressed as percentage of the left ventricle. All measurements were performed in the scintigraphic core laboratory by investigators unaware of the TIMI flow grade.
Angiographic Evaluation
Coronary angiography was performed according to standard criteria and was scheduled to be repeated 14 d after the stenting procedure. Offline analysis of digital angiograms was performed in the core laboratory using an automated edge detection system (CMS; Medis Medical Imaging Systems) by personnel unaware of the scintigraphic data. Identical projections were used for initial and follow-up angiographic examinations. Blood flow in the IRA was graded according to the TIMI classification (10). Collateral circulation was quantified according to Rentrop et al. (11). Global left ventricular ejection fraction was determined by using the area–length method (12). Regional wall motion was assessed by determining the number of chords within the region of interest showing hypokinesia (≥ −1 SD) (13).
Statistical Analysis
Data are presented as medians and (in brackets) 25th and 75th percentiles, as counts, or as proportions. The normality of distribution was assessed with the 1-sample Kolmogorov–Smirnov test. Continuous data were compared with the Wilcoxon rank-sum test. Categoric data were compared with the χ2 test or Fisher exact test when expected cell values were <5. Multiple linear regression modeling was used to identify independent predictors of initial perfusion defect, infarct size, and myocardial salvage. P < 0.05 was considered to indicate statistical significance.
RESULTS
Baseline Characteristics
Patients were divided into 2 groups depending on TIMI flow grade: a group with TIMI flow grade ≤ 1 (77 patients) and a group with TIMI flow grade > 1 (41 patients). Baseline characteristics of the patients are shown in Table 1. Patients in the group with TIMI flow grade > 1 were older and had lower values of peak creatine kinase and its MB izoenzyme activities than did the group with TIMI flow grade ≤ 1. The remaining characteristics did not differ significantly between the patients in the 2 groups.
Baseline Data
Angiographic Data
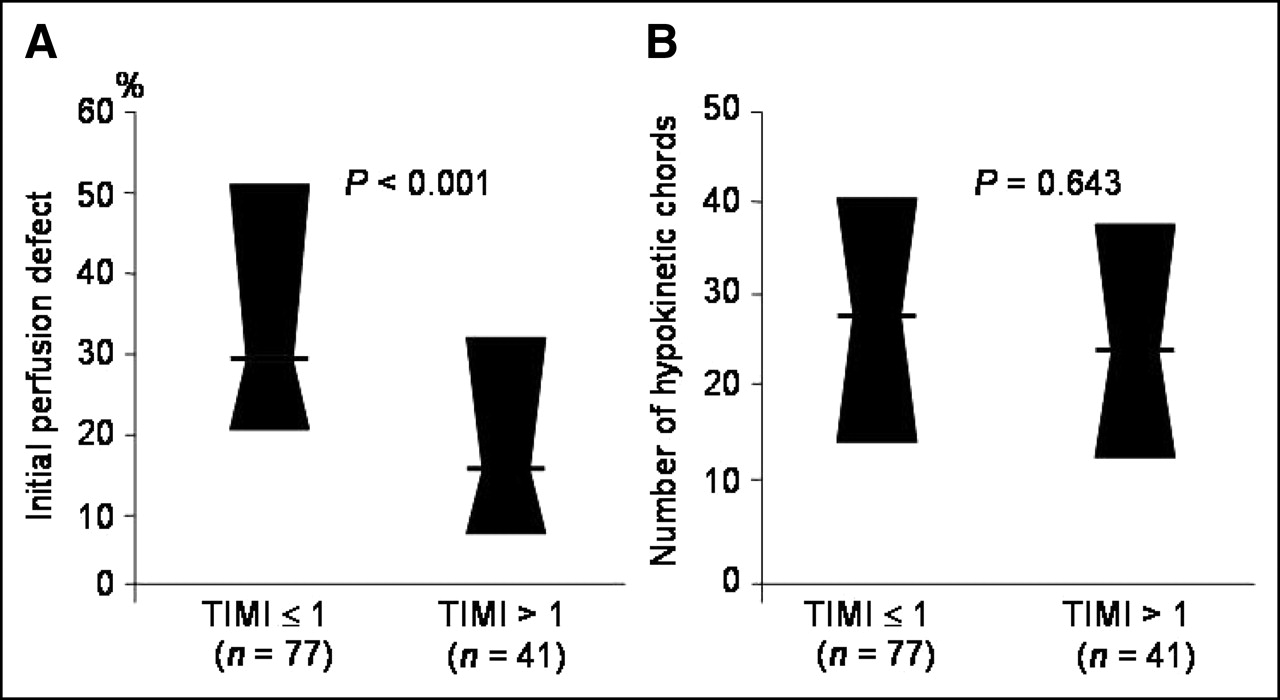
Initial angiographic data are shown in Table 2. Initial TIMI flow grades 0, 1, 2, and 3 were observed in 64 patients (54.2%), 13 patients (11.0%), 25 patients (21.2%), and 16 patients (13.9%) of the whole population. The groups did not significantly differ in the number of hypokinetic chords in the region of interest (Fig. 1) or postinterventional TIMI flow grade (Table 2).

Initial perfusion defect (A) and extension of hypokinetic area expressed as number of hypokinetic chords (B). Data are medians and 25th and 75th percentiles.
Angiographic Data
At the day 14 coronary angiography, the TIMI flow grades 0, 1, 2, and 3 were observed in 3.8% (3 patients), 3.8% (3 patients), 10.4% (8 patients), and 81.8% (63 patients), respectively, of the patients with initial TIMI flow grade ≤ 1. In the group with initial TIMI flow grade > 1, TIMI flow grades 0 and 1 were not observed, whereas TIMI flow grades 2 and 3 were observed in 1 patient (2.4%) and 40 patients (97.6%), respectively (P = 0.07, compared with TIMI flow grade distribution in the group with TIMI flow grade ≤ 1). When the rates of TIMI flow grade 3 at 14-d coronary angiography were analyzed separately, fewer of the patients with that grade had had an initial grade ≤ 1 than an initial grade > 1 (63 patients, 81.8%, vs. 40 patients, 97.6%; P = 0.01). A larger number of hypokinetic chords was found in the group with TIMI flow grade ≤ 1 than in the group with TIMI flow grade > 1 (16 chords [2.5; 30.0] vs. 7 chords [0; 22.0], P = 0.024; Fig. 2). Left ventricular ejection fraction was 56.5% [42.9%; 65.0%] in the group with TIMI flow grade ≤ 1, versus 61.0% [54.0%; 68.0%] in the group with TIMI flow grade > 1 (P = 0.03).
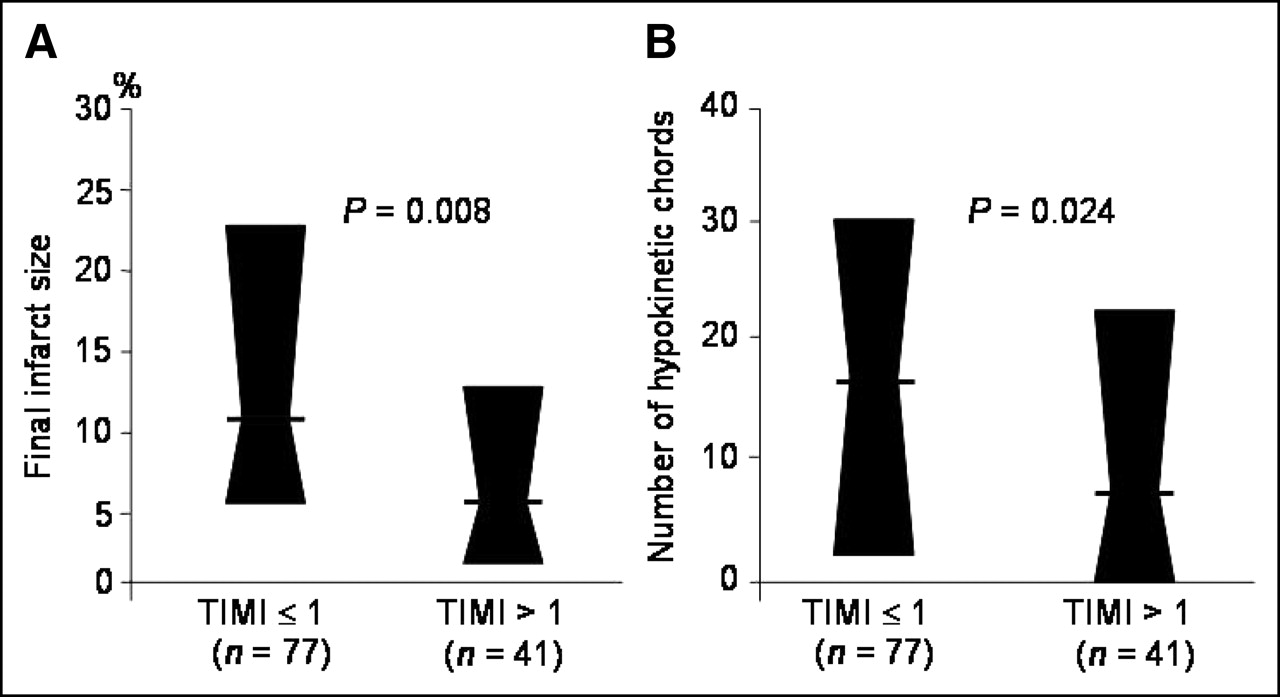
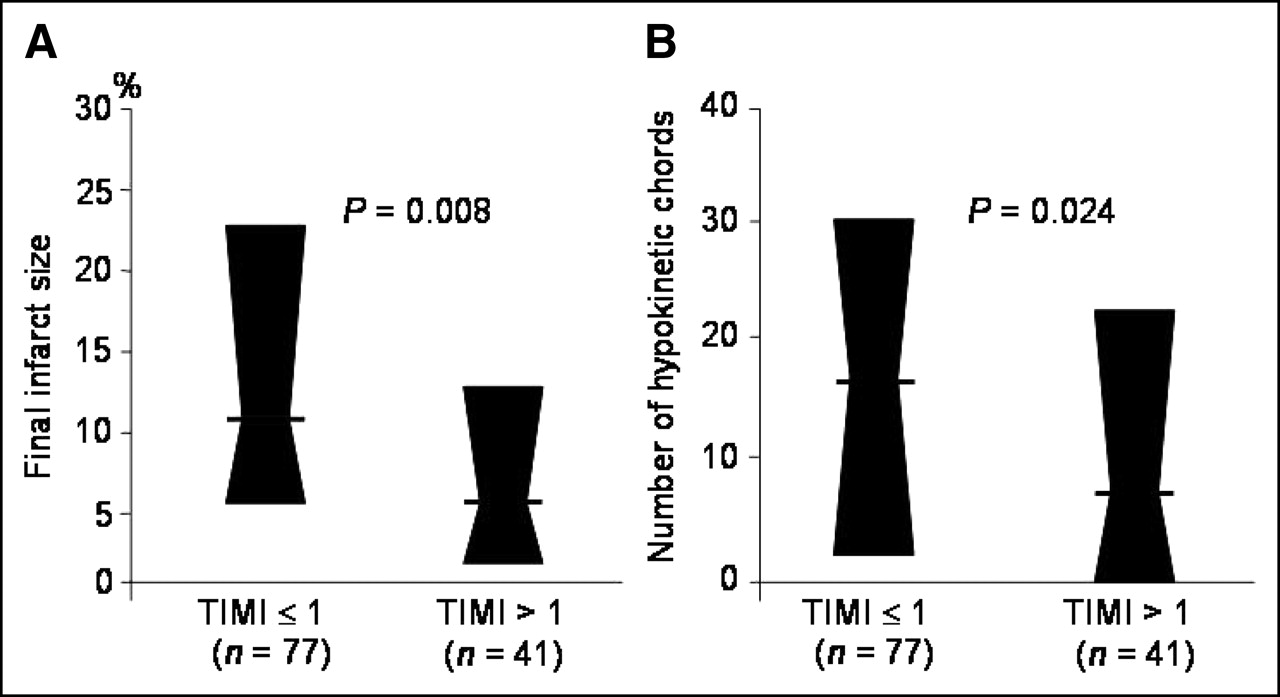
Final infarct size on scintigraphy performed 7–14 d after coronary stenting (A) and number of hypokinetic chords on day 14 angiography (B). Data are medians and 25th and 75th percentiles.
Scintigraphic Data
The initial perfusion defect was 29.1% [21.0%; 52.0%] of the left ventricle in the group with TIMI flow grade ≤ 1, versus 16.5% [8.0%; 33.1%] in the group with TIMI flow grade > 1 (P < 0.001; Fig. 1). Follow-up scintigraphy was performed after 10.4 d [8.0; 11.9 d] in the group with initial TIMI flow grade ≤ 1 and 10.2 d [8.4; 12.0 d] in the group with initial TIMI flow grade > 1 (P = 0.859). Final infarct size was 11.0% [6.1%; 23.5%] of the left ventricle in the group with TIMI flow grade ≤ 1, versus 6.0% [2.0%; 12.8%] in the group with TIMI flow > 1 (P = 0.008; Fig. 2). The absolute amount of at-risk myocardium salvaged was 17.8% [8.5%; 27.0%] of the left ventricle in the group with TIMI flow grade ≤ 1, versus 9.0% [4.8%; 19.0%] in the group with TIMI flow grade > 1 (P = 0.002). Salvage index showed no significant differences between patients with TIMI flow grade ≤ 1 and patients with TIMI flow grade > 1 (0.58 [0.38; 0.76] vs. 0.61 [0.36; 0.74]; P = 0.952). Scintigraphic data were further compared in subgroups with TIMI flow grade 0 vs. 1 in the group with TIMI flow grade ≤ 1 and in subgroups with TIMI flow grade 2 vs. 3 in the group with TIMI flow grade > 1. Results are shown in Table 3.
Scintigraphic Data According to TIMI Flow Grade
Multiple linear regression analysis was used to define the independent correlates of initial perfusion defect, final infarct size, and relative salvage (salvage index). The following variables were entered into the model: age, sex, diabetes, arterial hypertension, smoking, hypercholesterolemia, previous myocardial infarction, previous coronary bypass graft surgery, Killip class, time to admission, IRA, multivessel disease, initial TIMI flow grade, and collateral grade. All 3 dependent variables were entered into the models as continuous variables. The models showed that initial TIMI flow grade ≤ 1 (P < 0.001) and the left anterior descending coronary artery as the IRA (P = 0.039) were the only independent predictors of greater initial perfusion defect. The overall R2 of the model was 0.46. When the model was applied for final infarct size or salvage index, postprocedural TIMI flow was added to the variables entered into the model. The model showed that initial TIMI flow grade ≤ 1 was the only independent correlate of final infarct size (P = 0.05). None of the abovementioned variables, including initial TIMI flow grade (P = 0.26), were associated independently with the salvage index or the proportion of initial perfusion defect salvaged by coronary intervention.
DISCUSSION
The major findings of this study are as follows: First, persistence of residual blood flow in the IRA before coronary stenting is associated with a smaller initial area at risk (initial perfusion defect), and although the area at risk was smaller in patients with initial TIMI flow grade > 1, regional and global left ventricular function did not differ significantly between patients with and patients without preserved blood flow in the IRA. Second, the proportion of the initial perfusion defect (salvage index) that is salvaged by stenting with adjunct use of abciximab did not seem to depend on the presence of residual blood flow in the IRA. Third, patients with AMI and TIMI flow grade ≤ 1 before mechanical reperfusion with coronary stenting had a larger final infarct, a less favorable TIMI flow grade, and worse regional and global left ventricular function at the day 14 angiography than did patients with initial TIMI flow grade > 1.
Initial TIMI Flow Grade and Infarct Size
Our data showed that persistence of residual blood flow in the IRA is associated with a significant reduction in the initial perfusion defect. Even after adjustment in the multivariable model, the initial TIMI flow grade before coronary stenting was a strong independent correlate of initial area at risk and infarct size. With regard to the relationship between initial TIMI flow grade and the area at risk (initial perfusion defect), our results coincide with those of Clements et al. (4). However, our results are at variance with a recent study that did not show significant differences between patients with TIMI flow grade ≤ 1 and those with TIMI flow grade > 1 (5). We do not know the exact reason for this discrepancy; however, the inability to detect significant differences in the initial area at risk between patients with different grades of initial TIMI flow in the study by Leoncini et al. (5) might have been conditioned by the limited number of patients.
Another finding of the present study with potential practical implications concerns the differences in the amount of absolute myocardium salvaged by percutaneous mechanical reperfusion. Because the amount of myocardium salvaged by mechanical reperfusion was greatest in patients with initial TIMI flow grade ≤ 1, data from this study suggest that these patients benefit from percutaneous coronary intervention mostly in terms of reduction of the infarct size.
Earlier IRA blood-flow restoration, either spontaneously occurring or facilitated by aspirin and heparin, may explain differences in the initial area at risk. Previous angiographic studies have indicated that, at the time of angiography, IRA was not totally occluded in up to a third of patients (14,15). Reimer et al. have shown that extension of the amount of myocardial ischemia or necrosis critically depends on the time of coronary occlusion (16). Contrary to the significant differences in the initial area at risk, analysis of regional kinetics (number of hypokinetic chords) showed no differences in the extension of hypokinetic zone between the group with TIMI flow grade ≤ 1 and the group with TIMI flow grade > 1. The obvious perfusion–contraction mismatch in the group with TIMI flow grade > 1 indicates that earlier recanalization of the occluded IRA may have restored perfusion to large parts of the initial area at risk that subsequently undergo myocardial stunning. Because uptake and retention of 99mTc-sestamibi do not appear to be affected by stunning (17,18), the early-reperfused parts of the initial area at risk are accounted for as viable tissue by 99mTc-sestamibi scintigraphy, limiting the territory of the area at risk.
Initial TIMI Flow Grade and Procedure-Related Myocardial Salvage
There is no doubt that overall salvage (i.e., salvage obtained by early spontaneous recanalization and by mechanical reperfusion) should be greater in the group with preserved blood flow in the IRA. However, the proportion of initial perfusion defect salvaged by coronary intervention differed little between the group with TIMI flow grade ≤ 1 and the group with flow grade > 1. Restoration of blood flow in the IRA by coronary intervention is the main mechanism by which ischemic myocardium is salvaged in the group with TIMI flow grade ≤ 1. In the group with preserved blood flow in the IRA (TIMI flow grade 2 or 3), however, the benefits of mechanical reperfusion may be more difficult to explain. We postulate 3 mechanisms that may explain the observed benefits of mechanical reperfusion in patients with preserved blood flow in the IRA. First, because in nearly all patients with TIMI flow grade 2, optimal epicardial blood flow (TIMI flow grade 3) was restored by mechanical reperfusion, the perfusion of the residual ischemic tissue may further improve. Second, recanalization of the IRA does not afford a substantial clinical benefit if coronary flow continues to be compromised at the microcirculation level (19). Abciximab, by its actions at the microcirculation level (13), may further improve tissue reperfusion, leading to further myocardial salvage. Third, restoration of blood flow to previously ischemic myocardial tissue is not associated with an immediate full recovery of cellular energetic supply or mitondondrial ability to retain 99mTc-sestamibi. MR spectroscopy has shown that the ratio of phosphocreatine to β-adenosine triphosphate did not return to the control value with reperfusion (20). Myocellular uptake of 99mTc-sestamibi involves passive distribution across plasma and mitochondrial membranes and sequestration within mitochondria because of a large negative transmembrane potential (21). We may speculate that because of time-dependent restoration of the functional integrity of the inner mitochondrial membrane after prolonged myocardial ischemia, myocardial cells that survived ischemia may have a reduced capacity to take up enough radionuclide tracer to reach the detection threshold immediately on restoration of coronary blood flow. Because of restoration of the functional integrity of the inner mitochondrial membrane, in follow-up scintigraphy these myocardial cells may retain more tracer and thus may be considered viable. If so, the detected amount of salvaged myocardium is increased. However, these mechanisms also facilitate myocardial salvage in patients without effective coronary blood flow before mechanical reperfusion.
Initial TIMI Flow Grade and Regional and Functional Recovery
Angiographic examination performed at 14 d after primary coronary stenting showed that patients with initial TIMI flow grade > 1 before the procedure had better regional and global left ventricular function. Regional and global left ventricular function improved in both groups; however, differences at 14 d reached statistical significance because of the greater improvement in the group with TIMI flow grade > 1. These data are in line with a recent gated-SPECT study that assessed left ventricular function after AMI (5). Better regional recovery in the group with TIMI flow grade > 1, including anatomic factors (smaller infarcts) and functional recovery (fewer hypokinetic chords) may explain the differences in left ventricular function. Of note, our data showed that patients with TIMI flow grade ≤ 1 had a worse TIMI flow status at the day 14 angiography than did those with TIMI flow grade > 1. The exact reasons for worsening of blood flow in patients without anterograde residual flow are unclear. Nevertheless, one can speculate that a greater thrombus burden, more distal microvascular obstruction related to larger infarct size, and more prolonged ischemia are contributing factors. Whether worsening of blood flow in patients with initial TIMI flow grade ≤ 1 did have a role in the less favorable functional recovery remains purely conjectural. However, maintenance of an optimal postprocedural TIMI flow is crucial for a better clinical outcome (22). We accept as a limitation of this study the lack of information on the exact timing of blood flow obstruction after procedural success. Furthermore, we do not know whether the blood flow obstruction is progressive and will continue to worsen beyond 14 d, particularly in patients with preprocedural TIMI flow ≤ 1.
CONCLUSION
Preserved blood flow in the IRA (TIMI flow grade > 1) in patients with AMI is associated with a smaller area at risk and infarct, better recovery of regional and global left ventricular function, and maintenance of an optimal postprocedural blood flow. The proportion of initial area at risk salvaged by coronary stenting does not seem to depend on residual blood flow in the IRA.
Footnotes
Received Apr. 27, 2005; revision accepted Aug. 3, 2005.
For correspondence or reprints contact: Gjin Ndrepepa, MD, Deutsches Herzzentrum, Lazarettstrasse 36, 80636 München, Germany.
E-mail: ndrepepa{at}dhm.mhn.de





{kind=link}
{kind=link}